
A Rapid Systematic Review on the Experiences of Cancer Survivors Residing in Rural Areas during the COVID-19 Pandemic

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Protocol Registration
2.2. Study Design
2.3. Search Strategy
Eligibility Criteria
- (1)
- Inclusion Criteria
- (2)
- Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Analysis

{kind=link}
| Authors and Title | Setting | Participants | Methods/Design | Findings in Relation to Rurality |
|---|---|---|---|---|
| Baffert et al. (2021) [46] Quality of life in patients with cancer during the COVID-19 pandemic (France) | Patients managed in a day hospital of the Medical Oncology Department at Limoges Dupuytren Hospital which is located in a rural area. | n = 189 Patients mostly aged 61–70, female (n = 113) and male (n = 64) who presented with lung, breast or colorectal cancer. | Quantitative study design A prospective observational study on patient-reported outcomes, quality of life and satisfaction in patients with cancer with their care management in a day hospital during May–June 2020. | Rural n not reported but the authors refer to the hospital being in a rural setting in the French countryside and that many of the patients that go there reside in rural areas. Overall, patients’ anxiety scores remained low post-lockdown in rural regions where the rate of infection was limited and where patients had preserved quality of life which the authors infer could be by having a nice home in a rural area and where the organisation of care was globally maintained. Identified risk factors for post-lockdown anxiety were female gender and living in a city apartment. |
| Davis et al. (2021) [47] Exploring the challenges in accessing care and support for cancer survivors in Australia during COVID-19 (Australia) | Cancer community wellness center in rural/regional Australia. The center cares for cancer survivors and caregivers at all stages of the care trajectory. | n = 66 Cancer survivors with a range of diagnoses, 71% female and 29% male (n = 19), 6% 40 and under (n = 4), 42% 41–64 (n = 28) and 52% 65+ (n = 34). | Qualitative and quantitative study design Completed an online survey via Qualtrics regarding the impact of COVID-19 on their access to medical and support services. Data were collected July-October 2020. | Authors refer to total n as rural/regional cancer survivors (n = 66). Quantitative data Reduced their social support from family and friends (59%) Reduced ability to see their health care providers (46%) Impacted their access to supportive services (44%) Increased their distress over their cancer and health (40%) Negatively impacted their emotional wellbeing including depression and/or anxiety (35%) caused major worry in their life (33%) Delayed their testing or checkups for their cancer (20%), and delayed their access to cancer treatment (15%) Older adults reporting that COVID-19 had a significantly greater impact in their ability to access supportive services, their ability to obtain social support from family and friends, feeling distressed over cancer and health and their overall quality of life. Qualitative data Participants indicated social concerns including isolation from friends and family. Other concerns related to purchasing of groceries and social distancing. Some also reported concerns with access to treatment and the government’s ability to cope with the pandemic Most helpful during the pandemic was access to friends and family via online services or telephone. Access to online activities such as yoga, support services and cancer communities were also identified as helpful. Also extra time to engage in physical activity was helpful. |
| Galica et al. (2021) [48] Coping during COVID-19: a mixed methods study of older cancer survivors. (Canada) | Patients discharged from care of their cancer team at the Cancer Centre of South-eastern Ontario, Kingston, Ontario, Canada | n = 30 Older adults (>60 years) who were recently (<12 months) discharged from care of their cancer team | Mixed methods study design Quantitative data were collected using the Brief-COPE questionnaire. Qualitative data were collected using telephone interviews to explore experiences and strategies for coping with cancer-related concerns. No dates for data collection are given but the authors do report that this took place during the pandemic. The article was published in Jan 2021 so we can assume that data collection took place post March in 2020. | 37% of participants resided in rural area (n = 11). Participants appreciated how the privileges of financial planning for retirement, downsizing/renovating their living space, preparing living wills/funeral, and their living circumstances (e.g., not in long term care, in a rural area, an independent retirement community) provided ‘insulation’ from the negative effects of COVID-19. However, for one disabled participant living in a rural area, her in-home supportive services ceased due to the pandemic, which she said: “made me very confined because everything in this country is based on driving a car. …I have to arrange for somebody to do the groceries… it has affected me in a big way. |
| Himbert et al. (2022) [49] Factors associated with changes in exercise behavuours during the COVID-19 pandemic. (USA) | Cancer patients enrolled in the Total Cancer Care study, Huntsman Cancer Institute, Utah, USA | n= 1210 Adult cancer patients (>18 years) | Quantitative study design COVID-19 questionnaire (demographics and changes in exercise habits, health behaviours and psychosocial factors) Zip codes were categorised as urban or rural using the Rural-urban commuting Area Codes (RUCA) classification system. Data were collected from August–September 2020. | 27% of participants resided in rural areas (n = 328) Patients living in rural areas appeared not to change their exercise habits as compared to exercising less or more (32% vs. 21% or 19%; p < 0.0003). Higher percentage of urban patients reported changes in their exercise habits. |
| Howden et al. (2021) [50] A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults (Canada) | Participants were recruited across Canadian through an online survey link via cancer support group websites. | n = 805 Adolescents and young adults (18–39 years old) Diagnosed with any types of cancer | Quantitative and qualitative study design Data obtained through prior national cross-sectional survey. Survey created and administered online using REDCap. Data collected between January–February 2021. | 22% of participants resided in rural areas (n = 179) and 2% in remote areas (n = 17). Province/territory of residence was associated with experiencing at least one negative impact on cancer care (p < 0.03). The odds of having a negative impact on cancer care were higher for participants living in Central Canada, the Prairies and British Columbia compared to those living in the Territories of Canada. |
| Howden et al. (2022) [51] Loneliness among adolescents and young adults with cancer during the COVID-19 pandemic: a cross-sectional study (Canada) | Participants were recruited across Canadian through an online survey link via cancer support group websites. | n = 805 Adolescents and young adults (18–39 years old) Diagnosed with any types of cancer | Quantitative study design. Data obtained through prior national cross-sectional survey. Survey created and administered online using REDCap. Loneliness was measured using the 3-item UCLA Loneliness Scale. Data collected between January–February 2021. | 22% of participants were from rural (n = 179) and 2% from remote areas (n = 17). Participants who lived in rural or remote locations were less likely to experience loneliness (AOR 0.59, 95% CI 0.40–0.87, p = 0.008) than those living in urban settings. Authors comment that regional differences in the burden of COVID-19 cases, duration of lockdowns and degree of public health restrictions may have resulted in different social isolation restrictions in different locations in Canada. Also, sense of community and belonging can be more strongly developed in rural areas due to smaller population sizes. |
| Krok-Schoen et al. (2021) [52] Experiences of healthcare providers of older adults with cancer during the COVID-19 pandemic (Australia, Canada, Denmark, France, Germany, Hong Kong, Italy, Japan, Mexico, Netherlands, South Africa, Spain, UK, USA) | Respondents worked in academic/NCI comprehensive care program, hospitals, integrated network cancer programs, and other settings | n = 274 Healthcare providers of older adults with cancer. Social workers (43%), oncologists, geriatricians, advanced practice providers (28%), administrators (8.1%), navigators (5.1%), multiple professions or positions (6.3%), other professions (9.2%). | Qualitative study design Questionnaire survey data obtained from a larger study. Focus on analysing the qualitative findings. The survey was live from April–May 2020. | 17% of respondents were located at a cancer programmes/institutes in a rural area (n = 47). A prominent theme identified included telehealth challenges. Telehealth challenges included access and support issues as well as communication difficulty due to sensory impairment, rurality, and inadequate equipment. Disparities in access was another reported telehealth challenge. One healthcare provider noted, “patient’s tech ability, no internet, no computer, or smart phone availability” while another stated, “rural settings lack internet service.” |
| Peoples et al. (2022) [53] Impact of the COVID-19 pandemic on rural and urban cancer patients’ experiences, health behaviors, and perceptions. (USA) | Across 3 Cancer Centers: University of Utah Huntsman Cancer Institute, University of Miami Sylvester Comprehensive Cancer Center and Moffit Cancer Center | n= 1472 Adult cancer patients with a range of different tumour sites. | Quantitative study design COVID-19 survey between August–September 2020 either electronically, in-person/via mail or over the phone. Assessed the impact of the pandemic on medical appointments, prevention/health behaviours and psychosocial factors. | 27% were from rural areas (n = 397) Rural versus urban patients were more like to be older, not employed, uninsured, former/current smokers, consume alcohol and have pandemic-related changes/cancellations in surgery appointments. Urban versus rural patients were more likely to socially distance, use masks and hand sanitizer and experience changes in exercise habits and in their daily lives. |
| Podubinski et al. (2021) [54] Experience of Healthcare Access in Australia during the First Year of the COVID-19 Pandemic. (Australia) | Individuals living within Australia | n = 59 Individuals living within Australia who raised issues related to healthcare access in a wider COVID-19 study. | Qualitative study design Semi-structured interviews conducted between August–December 2020 via phone or video conference. Participants were selected from a larger pool of respondents who had completed an online, nationally distributed survey on transmission and compliance with isolation, hygiene and social distancing measures. | Delay in access to specialist care was a major issue raised by people who lived away from major metropolitan areas, and the effect was cumulative across multiple types of care, particularly for older people. “We’ve put off going to specialists… its two and a half hours away from us. Both my husband and I have skin cancers that have to be removed, which we haven’t had done… and optometrists and dental appointments. Yeah. So those sorts of appointments have had to be cancelled. Because we can’t travel.” |
| Rajan et al. (2021) [55] Impact of COVID-19 pandemic on cancer surgery: Patient’s perspective (India) | The study was conducted in the Department of Surgical Oncology, at a tertiary care referral centre. | n = 310 Cancer patients (>18 years), male (n = 187, 60%) and female (n = 123, 40%) | Quantitative study design A cross-sectional survey that collected data on finances, access to healthcare, anxiety, stress and depression. Data were collected between June–August 2020. | 73% of participants resided in rural areas (n = 227) Patients who belonged to rural areas were impacted significantly more than those living in urban areas in terms of healthcare access (mean difference, 35 vs. 31, p = 0.015). The hospital is located in an urban area and as urban people had better access to transport, they were less impacted in accessing healthcare. Higher odds of COVID-19 related impact in patients from rural areas. Difficulty in reaching the hospital and arranging accommodation due to the majority of the sample coming from rural areas. |
| Ratnapradipa et al. (2022) [56] Qualitative analysis of cancer care experiences among rural cancer survivors and caregivers (USA) | Rural Cancer Centers located in central and western Nebraska | n = 20 Cancer survivors/patients (n = 16) and caregivers (n = 5). Female (n = 16) and Male (n = 4). Breast (n = 2), Bladder (n = 1), Multiple myeloma (n = 2), Lymphoma (n = 2), Prostate (n = 1) | Qualitative study design. Three 75–90 min. focus groups were conducted between Feb–May 2021 with 6–8 participants per group. Focus group questions were based on a community health needs assessment and the extant literature. Questions were asked in relation to community health status, cancer experiences (diagnosis and treatment, sources of cancer-related information). | The authors refer to the total n as being in a rural setting (n = 20) Participants identified barriers to care, including finances (treatment costs/insurance), transportation and lack of support groups and social support, as well as, more general cultural barriers. Participants noted the challenges with rural cancer centres retaining specialists referring to the turnover as “radiation oncologist of the month” |
| Singh et al. (2021) [57] Impact of COVID-19 lockdown on patients with cancer in North Bihar, India: A phone-based survey. (India) | Preventive oncology clinic in the Muzaffarpur district of North Bihar, India | n = 210 Cancer patients, majority were women (63%) and aged more than 40 years (77%). | Quantitative study design Descriptive, cross-sectional telephone survey. Data were collected between April–May 2020. Questions related to the patients characteristics, type of cancer, their current and past treatment status, impact of the lockdown on their follow-up appointments, treatment, and surgery, or any other problems they may have faced during the lockdown that affected their treatment. | 60% of participants resided in rural areas (n = 125) Most patients who missed their scheduled appointments were aged more than 60 years, women, inhabitants of rural areas, with multiple comorbidities, or belonged to the lower middle-income economic strata. About 70% of the patients faced transportation issues, and 55% experienced financial problems during the lockdown. |
| Spencer-Bowdage et al. (2021) [58] The experience of UK patients with bladder cancer during the COVID-19 pandemic: a survey-based snapshot (UK) | Action Bladder Cancer UK website, Patient Support Groups and Social Media Platforms. Geographical reach included from all the UK | n = 156 Patients with bladder cancer | Quantitative study design Online questionnaire survey. Data were collected between April–July 2020. | 34% of participants were from rural areas (n = 53). Our survey appears to demonstrate that both MIBC and NMIBC patients have been equally affected by delays, postponements and cancellations during the COVID-19 pandemic. There was no association between area type (rural/urban) and disruption to cancer treatment during the COVID-19 pandemic. |
| Zomerdijk et al. (2021) [59] Prevalence and correlates of psychological distress, unmet supportive care needs, and fear of cancer recurrence among haematological cancer patients during the COVID-19 pandemic. (Australia) | Online advertisement distributed via haematology groups. Geographic reach included from all of Australia. | n = 394 Patients with haematological cancer diagnosis | Quantitative study design An online cross-sectional survey was conducted that explored wellbeing, psychological distress, unmet supportive care needs and fear of cancer recurrence. Data were collected between July–August 2020. | 50% of participants lived in regional areas (n = 196). Living in a ‘regional’ area were associated with greater psychological distress during the pandemic. |
3. Results
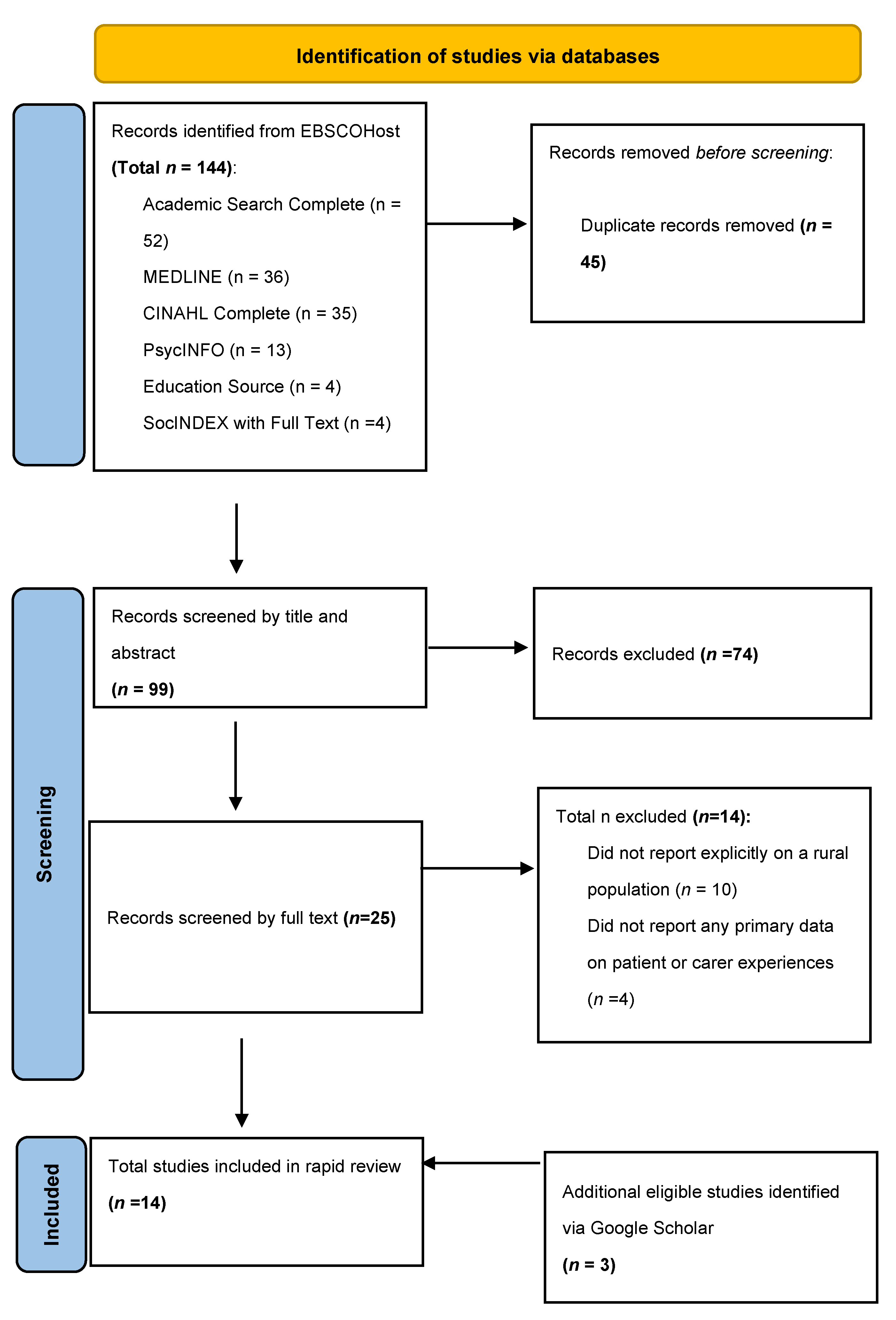
3.1. Search Results
3.2. Study Characteristics
3.3. Narrative Overview
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddams, J.; Utley, M.; Møller, H. Projections of cancer prevalence in the United Kingdom, 2010–2040. Br. J. Cancer 2012, 107, 1195–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lorenzo, F.; Apostolidis, K.; Florindi, F.; Makaroff, L.E. Improving European policy to support cancer survivors. J. Cancer Policy 2018, 15, 72–75. [Google Scholar] [CrossRef]
- Bakouny, Z.; Hawley, J.E.; Choueiri, T.K.; Peters, S.; Rini, B.I.; Warner, J.L.; Painter, C.A. COVID-19 and Cancer: Current Challenges and Perspectives. Cancer Cell 2020, 38, 629–646. [Google Scholar] [CrossRef]
- Alkatout, I.; Biebl, M.; Momenimovahed, Z.; Giovannucci, E.; Hadavandsiri, F.; Salehiniya, H.; Allahqoli, L. Has COVID-19 Affected Cancer Screening Programs? A Systematic Review. Front. Oncol. 2021, 11, 675038. [Google Scholar] [CrossRef]
- Riera, R.; Bagattini, Â.M.; Pacheco, R.L.; Pachito, D.V.; Roitberg, F.; Ilbawi, A. Delays and Disruptions in Cancer Health Care Due to COVID-19 Pandemic: Systematic Review. JCO Glob. Oncol. 2021, 7, 311–323. [Google Scholar] [CrossRef]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef]
- Jones, J.M.; Saeed, H.; Katz, M.S.; Lustberg, M.B.; Forster, V.J.; Nekhlyudov, L. Readdressing the Needs of Cancer Survivors During COVID-19: A Path Forward. JNCI J. Natl. Cancer Inst. 2021, 113, 955–961. [Google Scholar] [CrossRef]
- Nekhlyudov, L.; Duijts, S.; Hudson, S.V.; Jones, J.M.; Keogh, J.; Love, B.; Lustberg, M.; Smith, K.C.; Tevaarwerk, A.; Yu, X.; et al. Addressing the needs of cancer survivors during the COVID-19 pandemic. J. Cancer Surviv. 2020, 14, 601–606. [Google Scholar] [CrossRef] [Green Version]
- Moss, J.L.; Pinto, C.N.; Mama, S.K.; Rincon, M.; Kent, E.E.; Yu, M.; Cronin, K.A. Rural–urban differences in health-related quality of life: Patterns for cancer survivors compared to other older adults. Qual. Life Res. 2021, 30, 1131–1143. [Google Scholar] [CrossRef]
- Weaver, K.E.; Geiger, A.M.; Lu, L.; Case, L.D. Rural-urban disparities in health status among US cancer survivors. Cancer 2013, 119, 1050–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, K.E.; Palmer, N.; Lu, L.; Case, L.D.; Geiger, A.M. Rural–urban differences in health behaviors and implications for health status among US cancer survivors. Cancer Causes Control 2013, 24, 1481–1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahnd, W.E.; Davis, M.M.; Rotter, J.S.; Vanderpool, R.C.; Perry, C.K.; Shannon, J.; Ko, L.K.; Wheeler, S.B.; Odahowski, C.L.; Farris, P.E.; et al. Rural-urban differences in financial burden among cancer survivors: An analysis of a nationally representative survey. Support. Care Cancer 2019, 27, 4779–4786. [Google Scholar] [CrossRef]
- Burris, J.L.; Andrykowski, M. Disparities in mental health between rural and nonrural cancer survivors: A preliminary study. Psycho-Oncology 2010, 19, 637–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNulty, J.A.; Nail, L. Cancer Survivorship in Rural and Urban Adults: A Descriptive and Mixed Methods Study. J. Rural. Health 2015, 31, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Afshar, N.; English, D.R.; Milne, R.L. Rural–urban residence and cancer survival in high-income countries: A systematic review. Cancer 2019, 125, 2172–2184. [Google Scholar] [CrossRef] [Green Version]
- van der Kruk, S.R.; Butow, P.; Mesters, I.; Boyle, T.; Olver, I.; White, K.; Sabesan, S.; Zielinski, R.; Chan, B.A.; Spronk, K.; et al. Psychosocial well-being and supportive care needs of cancer patients and survivors living in rural or regional areas: A systematic review from 2010 to 2021. Support. Care Cancer 2022, 30, 1021–1064. [Google Scholar] [CrossRef]
- Carriere, R.; Adam, R.; Fielding, S.; Barlas, R.; Ong, Y.; Murchie, P. Rural dwellers are less likely to survive cancer—An international review and meta-analysis. Health Place 2018, 53, 219–227. [Google Scholar] [CrossRef]
- Stolzenbach, L.F.; Deuker, M.; Collà-Ruvolo, C.; Nocera, L.; Tian, Z.; Maurer, T.; Tilki, D.; Briganti, A.; Saad, F.; Mirone, V.; et al. Differences between rural and urban prostate cancer patients. World J. Urol. 2021, 39, 2507–2514. [Google Scholar] [CrossRef]
- Deuker, M.; Stolzenbach, L.F.; Collà Ruvolo, C.; Nocera, L.; Tian, Z.; Roos, F.C.; Becker, A.; Kluth, L.A.; Tilki, D.; Shariat, S.F.; et al. Bladder cancer stage and mortality: Urban vs. rural residency. Cancer Causes Control 2021, 32, 139–145. [Google Scholar] [CrossRef]
- Ruvolo, C.C.; Stolzenbach, L.F.; Nocera, L.; Deuker, M.; Wenzel, M.; Tian, Z.; La Rocca, R.; Creta, M.; Capece, M.; Saad, F.; et al. Higher Cancer Mortality in Rural Upper Urinary Tract Urothelial Carcinoma Patients. Urol. Int. 2021, 105, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Butow, P.N.; Phillips, F.; Schweder, J.; White, K.; Underhill, C.; Goldstein, D. Psychosocial well-being and supportive care needs of cancer patients living in urban and rural/regional areas: A systematic review. Support. Care Cancer 2012, 20, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Reid-Arndt, S.A.; Cox, C.R. Does Rurality Affect Quality of Life Following Treatment for Breast Cancer? J. Rural. Health 2010, 26, 402–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noonan, D.; LeBlanc, M.; Conley, C.; Benecha, H.; Leak-Bryant, A.; Peter, K.; Zimmerman, S.; Mayer, D.; Smith, S. Quality of Life and Impact of Cancer: Differences in Rural and Nonrural Non-Hodgkin’s Lymphoma Survivors. J. Rural. Health 2020, 36, 536–542. [Google Scholar] [CrossRef]
- Nelson, D.; McGonagle, I.; Jackson, C.; Kane, R. What is known about the role of rural-urban residency in relation to self-management in people affected by cancer who have completed primary treatment? A scoping review. Support. Care Cancer 2021, 29, 67–78. [Google Scholar] [CrossRef]
- Loughery, J.; Woodgate, R. Supportive care needs of rural individuals living with cancer: A literature review. Can. Oncol. Nurs. J. 2015, 25, 10. [Google Scholar] [CrossRef] [Green Version]
- Graham, F.; Kane, R.; Gussy, M.; Nelson, D. Recovery of Health and Wellbeing in Rural Cancer Survivors Following Primary Treatment: Analysis of UK Qualitative Interview Data. Nurs. Rep. 2022, 12, 482–497. [Google Scholar] [CrossRef]
- Levit, L.A.; Byatt, L.; Lyss, A.P.; Paskett, E.D.; Levit, K.; Kirkwood, K.; Schenkel, C.; Schilsky, R.L. Closing the Rural Cancer Care Gap: Three Institutional Approaches. JCO Oncol. Pract. 2020, 16, 422–430. [Google Scholar] [CrossRef]
- Sugiyama, T.; Carver, A.; Koohsari, M.J.; Veitch, J. Advantages of public green spaces in enhancing population health. Landsc. Urban Plan. 2018, 178, 12–17. [Google Scholar] [CrossRef]
- Nelson, D.; McGonagle, I.; Jackson, C.; Gussy, M.; Kane, R. A rural-urban comparison of self-management in people living with cancer following primary treatment: A mixed methods study. Psycho-Oncology 2022, 31, 1660–1670. [Google Scholar] [CrossRef]
- Gunn, K.M.; Olver, I.; Skrabal Ross, X.; Harrison, N.; Livingston, P.M.; Wilson, C. Improving Survivors’ Quality of Life Post-Treatment: The Perspectives of Rural Australian Cancer Survivors and Their Carers. Cancers 2021, 13, 1600. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.; Law, G.R.; McGonagle, I.; Turner, P.; Jackson, C.; Kane, R. The Effect of Rural Residence on Cancer-Related Self-Efficacy With UK Cancer Survivors Following Treatment. J. Rural. Health 2022, 38, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.; McGonagle, I.; Jackson, C.; Kane, R. An Exploration of Rural-Urban Residence on Self-Reported Health Status with UK Cancer Survivors Following Treatment: A Brief Report. Nurs. Rep. 2022, 12, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Gunn, K.M.; Berry, N.M.; Meng, X.; Wilson, C.J.; Dollman, J.; Woodman, R.J.; Clark, R.A.; Koczwara, B. Differences in the health, mental health and health-promoting behaviours of rural versus urban cancer survivors in Australia. Support. Care Cancer 2020, 28, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Jammu, A.S.; Chasen, M.R.; Lofters, A.K.; Bhargava, R. Systematic rapid living review of the impact of the COVID-19 pandemic on cancer survivors: Update to August 27, 2020. Support. Care Cancer 2021, 29, 2841–2850. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pose, A.; Burlina, C. Institutions and the uneven geography of the first wave of the COVID-19 pandemic. J. Reg. Sci. 2021, 61, 728–752. [Google Scholar] [CrossRef] [PubMed]
- Asongu, S.A.; Diop, S.; Nnanna, J. The geography of the effectiveness and consequences of COVID-19 measures: Global evidence. J. Public Aff. 2021, 21, e2483. [Google Scholar] [CrossRef]
- McLeod, B.; Cooke, S.; Kane, R.; Gussy, M.; Nelson, D. A Protocol for a Rapid Systematic Review on the Experiences of Cancer Survivors Who Reside in Rural Areas during the COVID-19 Pandemic. Open Sci. Framew. 2022. [Google Scholar] [CrossRef]
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J. Clin. Epidemiol. 2021, 130, 13–22. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Moher, D.; Stewart, L.; Shekelle, P. All in the Family: Systematic reviews, rapid reviews, scoping reviews, realist reviews, and more. Syst. Rev. 2015, 4, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E. A scoping review of rapid review methods. BMC Med. 2015, 13, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khangura, S.; Konnyu, K.; Cushman, R.; Grimshaw, J.; Moher, D. Evidence summaries: The evolution of a rapid review approach. Syst. Rev. 2012, 1, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Haby, M.M.; Chapman, E.; Clark, R.; Barreto, J.; Reveiz, L.; Lavis, J.N. What are the best methodologies for rapid reviews of the research evidence for evidence-informed decision making in health policy and practice: A rapid review. Health Res. Policy Syst. 2016, 14, 83. [Google Scholar] [CrossRef] [Green Version]
- Baffert, K.-A.; Darbas, T.; Lebrun-Ly, V.; Pestre-Munier, J.; Peyramaure, C.; Descours, C.; Mondoly, M.; Latrouite, S.; Bignon, E.; Nicouleau, S.; et al. Quality of Life of Patients with Cancer during the COVID-19 Pandemic. In Vivo 2021, 35, 663. [Google Scholar] [CrossRef]
- Davis, C.; Cadet, T.; Rune, K.; Wilson, P.; Banks, J. Exploring the Challenges in Accessing Care and Support for Cancer Survivors in Australia during COVID-19; Taylor & Francis Ltd.: Philadelphia, PA, USA, 2021; Report No.: 0734-7332. [Google Scholar]
- Galica, J.; Liu, Z.; Kain, D.; Merchant, S.; Booth, C.; Koven, R.; Brundage, M.; Haase, K.R. Coping during COVID-19: A mixed methods study of older cancer survivors. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2021, 29, 3389–3398. [Google Scholar] [CrossRef]
- Himbert, C.; Hathaway, C.A.; Daniels, B.; Salas, K.; Ashworth, A.; Gigic, B.; Lin, T.; Viskochil, R.; Kirchhoff, A.C.; Grossman, D.; et al. Factors associated with changes in exercise behaviors during the COVID-19 pandemic. Cancer Causes Control 2022, 33, 939–950. [Google Scholar] [CrossRef]
- Howden, K.; Glidden, C.; Romanescu, R.G.; Hatala, A.; Scott, I.; Deleemans, J.; Chalifour, K.; Eaton, G.; Gupta, A.A.; Bolton, J.M.; et al. A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults. Curr. Oncol. 2021, 28, 3201–3213. [Google Scholar] [CrossRef]
- Howden, K.; Yan, A.P.; Glidden, C.; Romanescu, R.G.; Scott, I.; Deleemans, J.M.; Chalifour, K.; Eaton, G.; Gupta, A.A.; Bolton, J.M.; et al. Loneliness among adolescents and young adults with cancer during the COVID-19 pandemic: A cross-sectional survey. Support. Care Cancer 2022, 30, 2215–2224. [Google Scholar] [CrossRef]
- Krok-Schoen, J.L.; Pisegna, J.L.; BrintzenhofeSzoc, K.; MacKenzie, A.R.; Canin, B.; Plotkin, E.; Boehmer, L.M.; Shahrokni, A. Experiences of healthcare providers of older adults with cancer during the COVID-19 pandemic. J. Geriatr. Oncol. 2021, 12, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Peoples, A.R.; Oswald, L.B.; Ose, J.; Daniels, B.; Himbert, C.; Hathaway, C.A.; Gigic, B.; Kirchhoff, A.C.; Lin, T.; Grossman, D.; et al. Impact of the COVID-19 pandemic on rural and urban cancer patients’ experiences, health behaviors, and perceptions. J. Rural. Health 2022, 38, 886–899. [Google Scholar] [CrossRef] [PubMed]
- Podubinski, T.; Townsin, L.; Thompson, S.C.; Tynan, A.; Argus, G. Experience of Healthcare Access in Australia during the First Year of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10687. [Google Scholar] [CrossRef]
- Rajan, S.; Akhtar, N.; Tripathi, A.; Kumar, V.; Chaturvedi, A.; Mishra, P.; Sharma, S.; Misra, S.; Gupta, S.; Singh, M. Impact of COVID-19 pandemic on cancer surgery: Patient’s perspective. J. Surg. Oncol. 2021, 123, 1188–1198. [Google Scholar] [CrossRef]
- Ratnapradipa, K.L.; Ranta, J.; Napit, K.; Luma, L.B.; Robinson, T.; Dinkel, D.; Schabloske, L.; Watanabe-Galloway, S. Qualitative analysis of cancer care experiences among rural cancer survivors and caregivers. J. Rural. Health 2022, 38, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Rai, C.; Ishan, R. Impact of COVID-19 lockdown on patients with cancer in North Bihar, India: A phone-based survey. Cancer Res. Stat. Treat. 2021, 4, 37–43. [Google Scholar] [CrossRef]
- Spencer-Bowdage, S.; Russell, B.; Rigby, J.; O’Kelly, J.; Kelly, P.; Page, M.; Raw, C.; Allchorne, P.; Harper, P.; Crew, J.; et al. The experience of UK patients with bladder cancer during the COVID-19 pandemic: A survey-based snapshot. BJU Int. 2021, 127, 179–181. [Google Scholar] [CrossRef]
- Zomerdijk, N.; Jongenelis, M.; Short, C.E.; Smith, A.; Turner, J.; Huntley, K. Prevalence and correlates of psychological distress, unmet supportive care needs, and fear of cancer recurrence among haematological cancer patients during the COVID-19 pandemic. Support. Care Cancer 2021, 29, 7755–7764. [Google Scholar] [CrossRef]
- Bird, W. Improving health in coastal communities. BMJ 2021, 374, n2214. [Google Scholar] [CrossRef]
- Bhatia, S.; Landier, W.; Paskett, E.D.; Peters, K.B.; Merrill, J.K.; Phillips, J.; Osarogiagbon, R.U. Rural–Urban Disparities in Cancer Outcomes: Opportunities for Future Research. J. Natl. Cancer Inst. 2022, 114, 940–952. [Google Scholar] [CrossRef]
- Scandurra, C.; Muzii, B.; La Rocca, R.; Di Bello, F.; Bottone, M.; Califano, G.; Longo, N.; Maldonato, N.M.; Mangiapia, F. Social Support Mediates the Relationship between Body Image Distress and Depressive Symptoms in Prostate Cancer Patients. Int. J. Environ. Res. Public Health 2022, 19, 4825. [Google Scholar] [CrossRef] [PubMed]
- Parsons, K.; Gaudine, A.; Swab, M. Experiences of older adults accessing specialized health care services in rural and remote areas: A qualitative systematic review. JBI Evid. Synth. 2021, 19, 1328–1343. [Google Scholar] [CrossRef] [PubMed]
- Adjei Boakye, E.; Jenkins, W.; Sharma, A. Disproportionate impact of COVID-19 pandemic on head and neck cancer survivors. Head Neck 2020, 42, 1329–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterson, C.; Bacon, R.; Dwyer, R.; Morrison, K.S.; Toohey, K.; O’Dea, A.; Slade, J.; Mortazavi, R.; Roberts, C.; Pranavan, G.; et al. The Role of Telehealth During the COVID-19 Pandemic Across the Interdisciplinary Cancer Team: Implications for Practice. Semin. Oncol. Nurs. 2020, 36, 151090. [Google Scholar] [CrossRef]
- Paterson, C.; Gobel, B.; Gosselin, T.; Haylock, P.J.; Papadopoulou, C.; Slusser, K.; Rodriguez, A.; Pituskin, E. Oncology Nursing During a Pandemic: Critical Reflections in the Context of COVID-19. Semin. Oncol. Nurs. 2020, 36, 151028. [Google Scholar] [CrossRef]
- Hincapié, M.A.; Gallego, J.C.; Gempeler, A.; Piñeros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine during the COVID-19 Pandemic: A Scoping Review. J. Prim. Care Community Health 2020, 11, 2150132720980612. [Google Scholar] [CrossRef]
- Seah, K.M. COVID-19: Exposing digital poverty in a pandemic. Int. J. Surg. 2020, 79, 127–128. [Google Scholar] [CrossRef]
- Arcury, T.A.; Sandberg, J.C.; Melius, K.P.; Quandt, S.A.; Leng, X.; Latulipe, C.; Miller, D.P.; Smith, D.A.; Bertoni, A.G. Older Adult Internet Use and eHealth Literacy. J. Appl. Gerontol. 2018, 39, 141–150. [Google Scholar] [CrossRef]
- Morra, S.; Napolitano, L.; Collà Ruvolo, C.; Celentano, G.; La Rocca, R.; Capece, M.; Creta, M.; Passaro, F.; Di Bello, F.; Cirillo, L.; et al. Could YouTubeTM encourage men on prostate checks? A contemporary analysis. Arch. Ital. Urol. Androl. 2022, 94, 285–290. [Google Scholar] [CrossRef]
- Di Bello, F.; Collà Ruvolo, C.; Cilio, S.; La Rocca, R.; Capece, M.; Creta, M.; Celentano, G.; Califano, G.; Morra, S.; Iacovazzo, C.; et al. Testicular cancer and YouTube: What do you expect from a social media platform? Int. J. Urol. 2022, 29, 685–691. [Google Scholar] [CrossRef]
- Gessert, C.; Waring, S.; Bailey-Davis, L.; Conway, P.; Roberts, M.; VanWormer, J. Rural definition of health: A systematic literature review. BMC Public Health 2015, 15, 378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girgis, A.; Lambert, S. Cost of informal caregiving in cancer care. Cancer Forum 2017, 41, 16–22. [Google Scholar]
- Nelson, D.; Mansfield, P.; Kane, R. Carers of people affected by cancer and other long-term conditions at end of life: A qualitative study of providing a bespoke package of support in a rural setting. Palliat. Med. 2016, 31, 158–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Challinor, J.M.; Alqudimat, M.R.; Teixeira, T.O.A.; Oldenmenger, W.H. Oncology nursing workforce: Challenges, solutions, and future strategies. Lancet Oncol. 2020, 21, e564–e574. [Google Scholar] [CrossRef] [PubMed]

| Search Terms | N |
|---|---|
| Cancer Terms | |
| “Cancer survivors” | 176,739 |
| “Cancer survivorship” | 11,372 |
| “Living with and beyond cancer” | 376 |
| “Cancer patient” | 155,316 |
| “People affected by cancer” | 708 |
| “People living with cancer” | 846 |
| “People living with and beyond cancer” | 180 |
| “Cancer survivors” OR “Cancer survivorship” OR “Living with and beyond cancer” OR “Cancer patient” OR “People affected by cancer” OR “People living with cancer” OR “People living with and beyond cancer” | 220,420 |
| Rural Terms | |
| “Rural health” | 102,640 |
| “Rural health service*” | 29,762 |
| Rural* | 1,384,440 |
| Remote | 871,244 |
| “Rural population” | 120,872 |
| “Rural communit*” | 95,636 |
| “Medically underserved area” | 12,659 |
| Non-urban | 3986 |
| Nonurban | 2266 |
| Non-metropolitan | 4722 |
| “Geographic isolat*” | 4315 |
| “Rural health” OR “Rural health service*” OR Rural* OR Remote OR “Rural population” OR “Rural communit*” OR “Medically underserved area” OR Non-urban OR Nonurban OR Non-metropolitan OR “Geographic isolat*” | 2,226,458 |
| COVID-19 Terms | |
| COVID-19 | 1,077,712 |
| Coronavirus | 790,904 |
| 2019-nCoV | 255,918 |
| SARS-CoV-2 | 255,990 |
| COV-19 | 1,077,712 |
| “COVID-19 pandemic” | 506,126 |
| COVID-19 OR Coronavirus OR 2019-nCoV OR SARS-CoV-2 OR COV-19 OR “COVID-19 pandemic” | 1,255,900 |
| Combine above (1) Cancer terms (2) Rural terms and (3) COVID-19 terms with AND | 144 |
| “Cancer survivors” OR “Cancer survivorship” OR “Living with and beyond cancer” OR “Cancer patient” OR “People affected by cancer” OR “People living with cancer” OR “People living with and beyond cancer” AND “Rural health” OR “Rural health service*” OR Rural* OR Remote OR “Rural population” OR “Rural communit*” OR “Medically underserved area” OR Non-urban OR Nonurban OR Non-metropolitan OR “Geographic isolat*” AND COVID-19 OR Coronavirus OR 2019-nCoV OR SARS-CoV-2 OR COV-19 OR “COVID-19 pandemic” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nelson, D.; Cooke, S.; McLeod, B.; Nanyonjo, A.; Kane, R.; Gussy, M. A Rapid Systematic Review on the Experiences of Cancer Survivors Residing in Rural Areas during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 16863. https://doi.org/10.3390/ijerph192416863
Nelson D, Cooke S, McLeod B, Nanyonjo A, Kane R, Gussy M. A Rapid Systematic Review on the Experiences of Cancer Survivors Residing in Rural Areas during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(24):16863. https://doi.org/10.3390/ijerph192416863
Chicago/Turabian StyleNelson, David, Samuel Cooke, Ben McLeod, Agnes Nanyonjo, Ros Kane, and Mark Gussy. 2022. "A Rapid Systematic Review on the Experiences of Cancer Survivors Residing in Rural Areas during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 24: 16863. https://doi.org/10.3390/ijerph192416863
APA StyleNelson, D., Cooke, S., McLeod, B., Nanyonjo, A., Kane, R., & Gussy, M. (2022). A Rapid Systematic Review on the Experiences of Cancer Survivors Residing in Rural Areas during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(24), 16863. https://doi.org/10.3390/ijerph192416863