
Incidence of Voice Disorders among Private School Teachers in Taiwan: A Nationwide Longitudinal Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
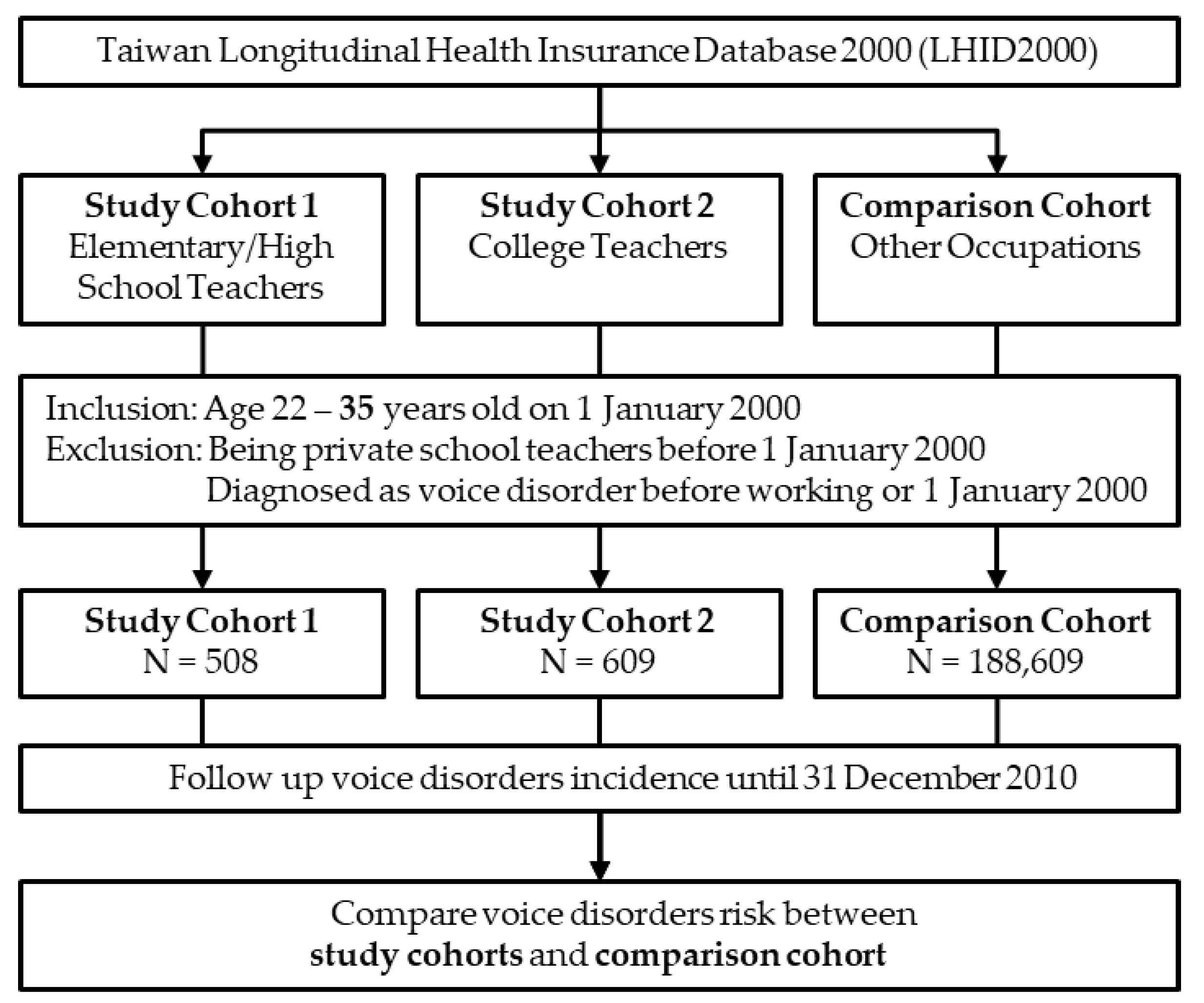
2.2. Participants
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics and Health Conditions of the Cohort Members
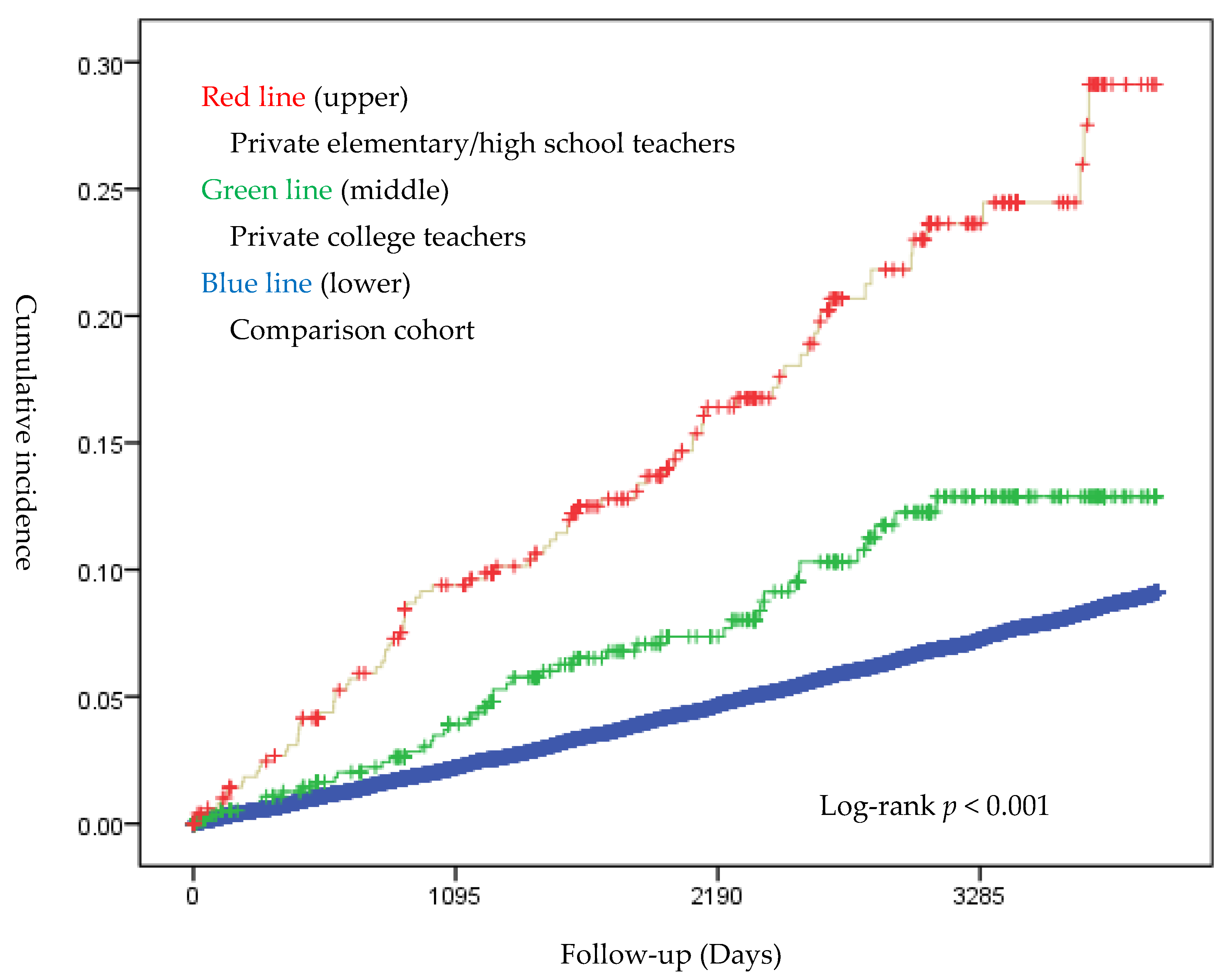
3.2. Incidence Estimation and Survival Analysis
4. Discussion
4.1. Voice Disorders in Private School Teachers
4.2. Other Risk Factors of Voice Disorders
4.3. Voice Disorders Occurred in Early Teaching Career
4.4. Impacts of Voice Disorders in Teachers
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heidel, S.E.; Torgerson, J.K. Vocal problems among aerobic instructors and aerobic participants. J. Commun. Disord. 1993, 26, 179–191. [Google Scholar] [CrossRef]
- Long, J.; Williford, H.N.; Olson, M.S.; Wolfe, V. Voice problems and risk factors among aerobics instructors. J. Voice 1998, 12, 197–207. [Google Scholar] [CrossRef]
- Jones, K.; Sigmon, J.; Hock, L.; Nelson, E.; Sullivan, M.; Ogren, F. Prevalence and risk factors for voice problems among telemarketers. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 571–577. [Google Scholar] [CrossRef] [Green Version]
- Phyland, D.; Oates, J.; Greenwood, K. Self-reported voice problems among three groups of professional singers. J. Voice 1999, 13, 602–611. [Google Scholar] [CrossRef]
- Williams, N.R. Occupational groups at risk of voice disorders: A review of the literature. Occup. Med. 2003, 53, 456–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, N.; Merrill, R.M.; Thibeault, S.; Parsa, R.A.; Gray, S.D.; Smith, E.M. Prevalence of voice disorders in teachers and the general population. J. Speech Lang. Hear. Res. 2004, 47, 281–293. [Google Scholar] [CrossRef]
- Byeon, H. The risk factors related to voice disorder in teachers: A systematic review and meta-analysis. Int. J. Environ. Res. Public Heal. 2019, 16, 3675. [Google Scholar] [CrossRef] [Green Version]
- Kiakojoury, K.; Dehghan, M.; Hajizade, F.; Khafri, S. Etiologies of dysphonia in patients referred to ENT clinics based on videolaryngoscopy. Iran. J. Otorhinolaryngol. 2014, 26, 169–174. [Google Scholar] [PubMed]
- Feierabend, R.H.; Shahram, M.N. Hoarseness in adults. Am. Fam. Physician 2009, 80, 363–370. [Google Scholar] [PubMed]
- Sułkowski, W.J.; Kowalska, S. Occupational voice disorders: An analysis of diagnoses made and certificates issued in 1999-2004. Int. J. Occup. Med. Environ. Heal. 2005, 18, 341–349. [Google Scholar]
- Lai, Y.-T.; Wang, Y.-H.; Yen, Y.-C.; Yu, T.-Y.; Chao, P.-Z.; Lee, F.-P.; Dailey, S. The epidemiology of benign voice disorders in Taiwan: A nationwide population-based study. Ann. Otol. Rhinol. Laryngol. 2019, 128, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Tung, C.-Y.; Yin, Y.-W.; Huang, C.-C.; Sung, H.-C.; Chang, C.-J. Teacher occupational disease assessment survey-self-perceived voice health problem. Chin. J. Sch. Health 2002, 40, 1–21. [Google Scholar]
- Gau, C.-S.; Chang, I.-S.; Wu, F.-L.L.; Yu, H.-T.; Huang, Y.-W.; Chi, C.-L.; Chien, S.-Y.; Lin, K.-M.; Liu, M.-Y.; Wang, H.-P. Usage of the claim database of national health insurance programme for analysis of cisapride-erythromycin co-medication in Taiwan. Pharmacoepidemiol. Drug Saf. 2006, 16, 86–95. [Google Scholar] [CrossRef]
- Chen, L.; Lu, H.-M.; Shih, S.-F.; Kuo, K.N.; Chen, C.-L.; Huang, L.C. Poverty related risk for potentially preventable hospitalisations among children in Taiwan. BMC Health Serv. Res. 2010, 10, 196. [Google Scholar] [CrossRef] [Green Version]
- da Rocha, L.M.; Bach, S.D.L.; Amaral, P.L.D.; Behlau, M.; Souza, L.D.D.M. Risk factors for the incidence of perceived voice disorders in elementary and middle school teachers. J. Voice 2017, 31, 258.e7–258.e12. [Google Scholar] [CrossRef] [PubMed]
- Leão, S.H.D.S.; Oates, J.M.; Purdy, S.C.; Scott, D.; Morton, R.P. Voice problems in New Zealand teachers: A national survey. J. Voice 2015, 29, 645.e1–645.e13. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-C.; Chen, J.-S. A study on performance of advanced technological and vocational educational institutes in Taiwan. Commer. Manag. Q. 2003, 4, 261–280. [Google Scholar]
- Charn, T.C.; Mok, P.K.H. Voice problems amongst primary school teachers in Singapore. J. Voice 2012, 26, e141–e147. [Google Scholar] [CrossRef]
- Devadas, U.; Bellur, R.; Maruthy, S. Prevalence and risk factors of voice problems among primary school teachers in India. J. Voice 2016, 31, 117.e1–117.e10. [Google Scholar] [CrossRef]
- Seifpanahi, S.; Izadi, F.; Jamshidi, A.-A.; Torabinezhad, F.; Sarrafzadeh, J.; Sobhani-Rad, D.; Ganjuie, M. Prevalence of voice disorders and associated risk factors in teachers and nonteachers in Iran. J. Voice 2015, 30, 506.e19–506.e23. [Google Scholar] [CrossRef]
- Lee, S.Y.-Y.; Lao, X.Q.; Yu, I.T.-S. A cross-sectional survey of voice disorders among primary school teachers in Hong Kong. J. Occup. Heal. 2010, 52, 344–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, E.J.; Tanner, K.; Smith, M.E. Gender differences affecting vocal health of women in vocally demanding careers. Logop. Phoniatr. Vocology 2010, 36, 128–136. [Google Scholar] [CrossRef]
- Chen, S.H.; Chiang, S.-C.; Chung, Y.-M.; Hsiao, L.-C.; Hsiao, T.-Y. Risk factors and effects of voice problems for teachers. J. Voice 2010, 24, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Moy, F.M.; Hoe, V.; Hairi, N.N.; Chu, A.H.Y.; Bulgiba, A.; Koh, D. Determinants and effects of voice disorders among secondary school teachers in Peninsular Malaysia using a validated Malay version of VHI-10. PLoS ONE 2015, 10, e0141963. [Google Scholar] [CrossRef]
- Van Houtte, E.; Claeys, S.; Wuyts, F.; Van Lierde, K. The impact of voice disorders among teachers: Vocal complaints, treatment-seeking behavior, knowledge of vocal care, and voice-related absenteeism. J. Voice 2011, 25, 570–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Number (%) or Mean ± SD | p Value | ||
|---|---|---|---|---|
| Other Occupations n = 188,145 | College Teachers n = 609 | Elementary/High-School Teachers n = 508 | ||
| Sex | ||||
| Male | 96,944 (51.5) | 283 (46.5) | 181 (35.6) | <0.001 |
| Female | 91,201 (48.5) | 326 (53.5) | 327 (64.4) | |
| Age (year) | 28.0 ± 4.0 | 27.7 ± 4.0 | 26.6 ± 3.5 | <0.001 |
| Income (NTD 1/month) | 18,041 ± 11,676 | 49,868 ± 19,409 | 36,468 ± 11,388 | <0.001 |
| ≤15,840 | 78,847 (41.9) | 1 (0.2) | 1 (0.2) | <0.001 |
| 15,841~25,000 | 75,518 (40.1) | 61 (10.0) | 95 (18.7) | |
| ≥25,001 | 33,895 (18.0) | 547 (90.0) | 412 (81.1) | |
| Voice disorders | 15,016 (8.0) | 47 (7.7) | 86 (16.9) | <0.001 |
| Comorbidity | ||||
| GERD 2 | 5048 (2.7) | 19 (3.1) | 15 (3.0) | 0.745 |
| Sinusitis | 61,091 (32.5) | 232 (38.1) | 254 (50.0) | <0.001 |
| Laryngitis | 42,806 (22.7) | 541 (24.8) | 617 (33.9) | <0.001 |
| Asthma | 6131 (3.3) | 22 (3.6) | 22 (4.3) | 0.351 |
| Mania | 126 (0.1) | 0 (0.0) | 1 (0.0) | 0.688 |
| Major depression | 1643 (0.9) | 7 (1.2) | 5 (1.0) | 0.738 |
| Anxiety disorder | 1716 (0.9) | 2 (0.3) | 2 (0.4) | 0.150 |
| Characteristics | Number (%) or Mean ± SD | p Value | ||
|---|---|---|---|---|
| Other Occupations n = 188,145 | College Teachers n = 609 | Elementary/High-School Teachers n = 508 | ||
| Sex | ||||
| Male | 96,944 (51.5) | 283 (46.5) | 181 (35.6) | <0.001 |
| Female | 91,201 (48.5) | 326 (53.5) | 327 (64.4) | |
| Age (year) | 28.0 ± 4.0 | 27.7 ± 4.0 | 26.6 ± 3.5 | <0.001 |
| Voice disorders | <0.001 | |||
| Occur in 3 years | 3842 (2.0) | 20 (3.3) | 43 (8.5) | |
| Occur in 4~6 years | 3951 (2.1) | 14 (2.3) | 24 (4.7) | |
| Occur in 7~9 years | 3932 (2.1) | 13 (2.1) | 15 (3.0) | |
| Person-years | 1,738,747 | 3515 | 3,146 | |
| Incidence rate 1 | 8.6 | 13.4 | 27.3 | |
| Characteristics | Adjusted Hazard Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Occupations | |||
| Other occupations | Reference | ||
| College teachers | 1.44 | 1.08–1.92 | 0.013 |
| Elementary/high-school teachers | 2.56 | 2.07–3.17 | <0.001 |
| Age (continuous variable) | 1.01 | 1.01–1.02 | <0.001 |
| Sex | |||
| Male | Reference | ||
| Female | 2.22 | 2.14–2.30 | <0.001 |
| Income (NTD/month) | |||
| ≤15,840 | Reference | ||
| 15,841–25,000 | 1.1 | 1.05–1.15 | <0.001 |
| ≥25,001 | 0.99 | 0.95–1.02 | 0.450 |
| Comorbidity | |||
| Sinusitis | 2.47 | 2.38–2.56 | <0.001 |
| Laryngitis | 1.73 | 1.67–1.79 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, B.-L.; Cheng, Y.-Y.; Lin, C.-Y.; Guo, H.-R. Incidence of Voice Disorders among Private School Teachers in Taiwan: A Nationwide Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 1130. https://doi.org/10.3390/ijerph19031130
Chen B-L, Cheng Y-Y, Lin C-Y, Guo H-R. Incidence of Voice Disorders among Private School Teachers in Taiwan: A Nationwide Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1130. https://doi.org/10.3390/ijerph19031130
Chicago/Turabian StyleChen, Bo-Lei, Ya-Yun Cheng, Cheng-Yu Lin, and How-Ran Guo. 2022. "Incidence of Voice Disorders among Private School Teachers in Taiwan: A Nationwide Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 3: 1130. https://doi.org/10.3390/ijerph19031130
APA StyleChen, B. -L., Cheng, Y. -Y., Lin, C. -Y., & Guo, H. -R. (2022). Incidence of Voice Disorders among Private School Teachers in Taiwan: A Nationwide Longitudinal Study. International Journal of Environmental Research and Public Health, 19(3), 1130. https://doi.org/10.3390/ijerph19031130