
Systematic Review for the Medical Applications of Meditation in Randomized Controlled Trials

 ,
, 

Abstract
:1. Introduction
2. Methods
2.1. Database and Searching Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Categorization of Meditation
2.5. Judgment of the Statistical Efficiency of the Intervention
2.6. Data Analysis
3. Results
3.1. General Characteristics of the RCTs
3.2. Diseases of the Participants and Types of Meditation in the RCTs
3.3. Target Measurements in the RCTs
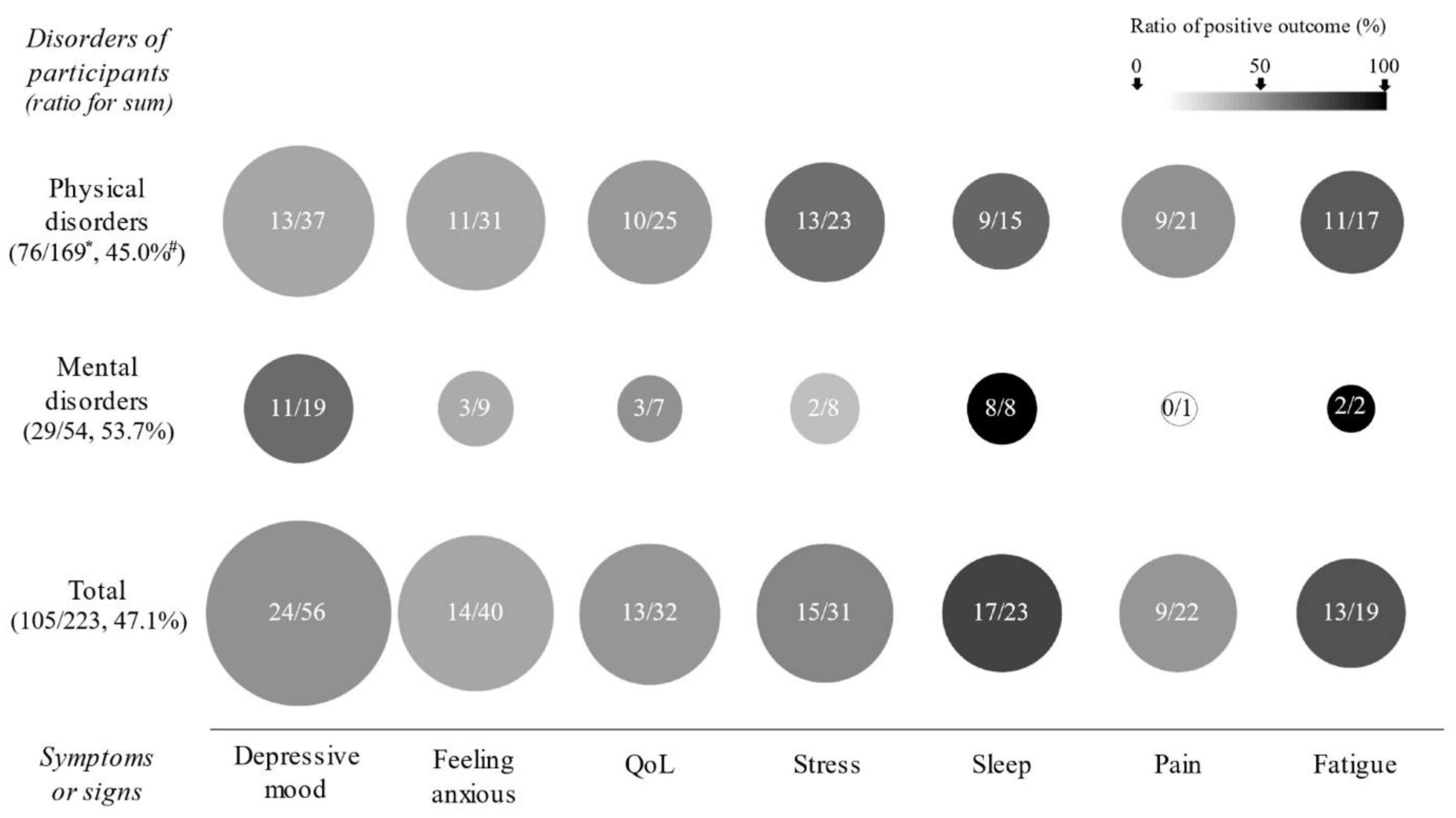
3.4. Clinical Outcomes for the Primary Measurement and Total Measurements
3.5. Clinical Outcomes According to the Type of Meditation
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Brandmeyer, T.; Delorme, A.; Wahbeh, H. The neuroscience of meditation: Classification, phenomenology, correlates, and mechanisms. Prog. Brain Res. 2019, 244, 1–29. [Google Scholar] [PubMed]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ospina, M.B.; Bond, K.; Karkhaneh, M.; Tjosvold, L.; Vandermeer, B.; Liang, Y.; Bialy, L.; Hooton, N.; Buscemi, N.; Dryden, D.M. Meditation practices for health: State of the research. Evid. Rep./Technol. Assess. 2007, 155, 1–263. [Google Scholar]
- Clarke, T.C.; Barnes, P.M.; Black, L.I.; Stussman, B.J.; Nahin, R.L. Use of Yoga, Meditation, and Chiropractors among US Adults Aged 18 and Over; Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2018.
- McConnell, B.; Applegate, M.; Keniston, A.; Kluger, B.; Maa, E. Use of complementary and alternative medicine in an urban county hospital epilepsy clinic. Epilepsy Behav. 2014, 34, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Bo, A.; Liu, T.; Zhang, P.; Chi, I. Effects of mindfulness-based stress reduction on depression in adolescents and young adults: A systematic review and meta-analysis. Front. Psychol. 2018, 9, 1034. [Google Scholar] [CrossRef] [PubMed]
- Piet, J.; Würtzen, H.; Zachariae, R. The effect of mindfulness-based therapy on symptoms of anxiety and depression in adult cancer patients and survivors: A systematic review and meta-analysis. J. Consult. Clin. Psychol. 2012, 80, 1007. [Google Scholar] [CrossRef] [Green Version]
- Cramer, H.; Lauche, R.; Haller, H.; Steckhan, N.; Michalsen, A.; Dobos, G. Effects of yoga on cardiovascular disease risk factors: A systematic review and meta-analysis. Int. J. Cardiol. 2014, 173, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Tailor, A.; Bhatt, T. Effects of yoga on brain waves and structural activation: A review. Complement. Ther. Clin. Pract. 2015, 21, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Matko, K.; Sedlmeier, P. What is meditation? Proposing an empirically derived classification system. Front. Psychol. 2019, 10, 2276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ospina, M.B.; Bond, K.; Karkhaneh, M.; Buscemi, N.; Dryden, D.M.; Barnes, V.; Carlson, L.E.; Dusek, J.A.; Shannahoff-Khalsa, D. Clinical trials of meditation practices in health care: Characteristics and quality. J. Altern. Complement. Med. 2008, 14, 1199–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionson, E.; Limbachia, J.; Rej, S.; Puka, K.; Newman, R.I.; Wetmore, S.; Burhan, A.M.; Vasudev, A. Effects of Sahaj Samadhi meditation on heart rate variability and depressive symptoms in patients with late-life depression. Br. J. Psychiatry 2019, 214, 218–224. [Google Scholar] [CrossRef]
- Nidich, S.; Mills, P.J.; Rainforth, M.; Heppner, P.; Schneider, R.H.; Rosenthal, N.E.; Salerno, J.; Gaylord-King, C.; Rutledge, T. Non-trauma-focused meditation versus exposure therapy in veterans with post-traumatic stress disorder: A randomised controlled trial. Lancet Psychiatry 2018, 5, 975–986. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Clark, H.D.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.R.; Fergusson, D.; Laupacis, A. Assessing the quality of randomized trials: Reliability of the Jadad scale. Control. Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef]
- Henneghan, A.M.; Becker, H.; Harrison, M.L.; Inselmann, K.; Fico, B.; Schafer, H.; King, E.; Patt, D.; Kesler, S. A randomized control trial of meditation compared to music listening to improve cognitive function for breast cancer survivors: Feasibility and acceptability. Complement. Ther. Clin. Pract. 2020, 41, 101228. [Google Scholar] [CrossRef] [PubMed]
- Gok, M.Z.; Karadas, C.; Izgu, N.; Ozdemir, L.; Demirci, U. Effects of progressive muscle relaxation and mindfulness meditation on fatigue, coping styles, and quality of life in early breast cancer patients: An assessor blinded, three-arm, randomized controlled trial. Eur. J. Oncol. Nurs. Off. J. Eur. Oncol. Nurs. Soc. 2019, 42, 116. [Google Scholar]
- Stoerkel, E.; Bellanti, D.; Paat, C.; Peacock, K.; Aden, J.; Setlik, R.; Walter, J.; Inman, A. Effectiveness of a self-care toolkit for surgical breast cancer patients in a military treatment facility. J. Altern. Complement. Med. 2018, 24, 916–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, M.R.; Olmstead, R.; Carrillo, C.; Sadeghi, N.; Nicassio, P.; Ganz, P.A.; Bower, J.E. Tai Chi Chih compared with cognitive behavioral therapy for the treatment of insomnia in survivors of breast cancer: A randomized, partially blinded, noninferiority trial. J. Clin. Oncol. 2017, 35, 2656. [Google Scholar] [CrossRef] [Green Version]
- Rao, R.M.; Raghuram, N.; Nagendra, H.R.; Kodaganur, G.S.; Bilimagga, R.S.; Shashidhara, H.; Diwakar, R.B.; Patil, S.; Rao, N. Effects of a yoga program on mood states, quality of life, and toxicity in breast cancer patients receiving conventional treatment: A randomized controlled trial. Indian J. Palliat. Care 2017, 23, 237. [Google Scholar] [CrossRef]
- Cramer, H.; Rabsilber, S.; Lauche, R.; Kümmel, S.; Dobos, G. Yoga and meditation for menopausal symptoms in breast cancer survivors—a randomized controlled trial. Cancer 2015, 121, 2175–2184. [Google Scholar] [CrossRef] [PubMed]
- Peppone, L.J.; Janelsins, M.C.; Kamen, C.; Mohile, S.G.; Sprod, L.K.; Gewandter, J.S.; Kirshner, J.J.; Gaur, R.; Ruzich, J.; Esparaz, B.T. The effect of YOCAS©® yoga for musculoskeletal symptoms among breast cancer survivors on hormonal therapy. Breast Cancer Res. Treat. 2015, 150, 597–604. [Google Scholar] [CrossRef]
- Larkey, L.K.; Roe, D.J.; Weihs, K.L.; Jahnke, R.; Lopez, A.M.; Rogers, C.E.; Oh, B.; Guillen-Rodriguez, J. Randomized controlled trial of Qigong/Tai Chi Easy on cancer-related fatigue in breast cancer survivors. Ann. Behav. Med. 2015, 49, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Bower, J.E.; Crosswell, A.D.; Stanton, A.L.; Crespi, C.M.; Winston, D.; Arevalo, J.; Ma, J.; Cole, S.W.; Ganz, P.A. Mindfulness meditation for younger breast cancer survivors: A randomized controlled trial. Cancer 2015, 121, 1231–1240. [Google Scholar] [CrossRef]
- Carlson, L.E.; Doll, R.; Stephen, J.; Faris, P.; Tamagawa, R.; Drysdale, E.; Speca, M. Randomized controlled trial of mindfulness-based cancer recovery versus supportive expressive group therapy for distressed survivors of breast cancer. J. Clin. Oncol. 2013, 31, 3119–3126. [Google Scholar] [CrossRef]
- Mustian, K.M.; Sprod, L.K.; Janelsins, M.; Peppone, L.J.; Palesh, O.G.; Chandwani, K.; Reddy, P.S.; Melnik, M.K.; Heckler, C.; Morrow, G.R. Multicenter, randomized controlled trial of yoga for sleep quality among cancer survivors. J. Clin. Oncol. 2013, 31, 3233. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.R.; Würtzen, H.; Steding-Jessen, M.; Christensen, J.; Andersen, K.K.; Flyger, H.; Mitchelmore, C.; Johansen, C.; Dalton, S.O. Effect of mindfulness-based stress reduction on sleep quality: Results of a randomized trial among Danish breast cancer patients. Acta Oncol. 2013, 52, 336–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.H.; Kim, H.J.; Do Ahn, S.; Seo, Y.J.; Kim, S.H. Effects of meditation on anxiety, depression, fatigue, and quality of life of women undergoing radiation therapy for breast cancer. Complement. Ther. Med. 2013, 21, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Bränström, R.; Kvillemo, P.; Moskowitz, J.T. A randomized study of the effects of mindfulness training on psychological well-being and symptoms of stress in patients treated for cancer at 6-month follow-up. Int. J. Behav. Med. 2012, 19, 535–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nidich, S.I.; Fields, J.Z.; Rainforth, M.V.; Pomerantz, R.; Cella, D.; Kristeller, J.; Salerno, J.W.; Schneider, R.H. A randomized controlled trial of the effects of transcendental meditation on quality of life in older breast cancer patients. Integr. Cancer Ther. 2009, 8, 228–234. [Google Scholar] [CrossRef]
- Speca, M.; Carlson, L.E.; Goodey, E.; Angen, M. A randomized, wait-list controlled clinical trial: The effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosom. Med. 2000, 62, 613–622. [Google Scholar] [CrossRef] [Green Version]
- Gautam, S.; Tolahunase, M.; Kumar, U.; Dada, R. Impact of yoga based mind-body intervention on systemic inflammatory markers and co-morbid depression in active Rheumatoid arthritis patients: A randomized controlled trial. Restor. Neurol. Neurosci. 2019, 37, 41–59. [Google Scholar] [CrossRef]
- Innes, K.E.; Selfe, T.K.; Kandati, S.; Wen, S.; Huysmans, Z. Effects of mantra meditation versus music listening on knee pain, function, and related outcomes in older adults with knee osteoarthritis: An exploratory Randomized Clinical Trial (RCT). Evid.-Based Complement. Altern. Med. 2018, 2018, 7683897. [Google Scholar] [CrossRef] [Green Version]
- Van Gordon, W.; Shonin, E.; Dunn, T.J.; Garcia-Campayo, J.; Griffiths, M.D. Meditation awareness training for the treatment of fibromyalgia syndrome: A randomized controlled trial. Br. J. Health Psychol. 2017, 22, 186–206. [Google Scholar] [CrossRef] [Green Version]
- Cherkin, D.C.; Sherman, K.J.; Balderson, B.H.; Cook, A.J.; Anderson, M.L.; Hawkes, R.J.; Hansen, K.E.; Turner, J.A. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA 2016, 315, 1240–1249. [Google Scholar] [CrossRef]
- Michalsen, A.; Kunz, N.; Jeitler, M.; Brunnhuber, S.; Meier, L.; Lüdtke, R.; Büssing, A.; Kessler, C. Effectiveness of focused meditation for patients with chronic low back pain—a randomized controlled clinical trial. Complement. Ther. Med. 2016, 26, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Cash, E.; Salmon, P.; Weissbecker, I.; Rebholz, W.N.; Bayley-Veloso, R.; Zimmaro, L.A.; Floyd, A.; Dedert, E.; Sephton, S.E. Mindfulness meditation alleviates fibromyalgia symptoms in women: Results of a randomized clinical trial. Ann. Behav. Med. 2015, 49, 319–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeitler, M.; Brunnhuber, S.; Meier, L.; Lüdtke, R.; Büssing, A.; Kessler, C.; Michalsen, A. Effectiveness of jyoti meditation for patients with chronic neck pain and psychological distress—A randomized controlled clinical trial. J. Pain 2015, 16, 77–86. [Google Scholar] [CrossRef]
- la Cour, P.; Petersen, M. Effects of mindfulness meditation on chronic pain: A randomized controlled trial. Pain Med. 2015, 16, 641–652. [Google Scholar] [CrossRef] [PubMed]
- Ebnezar, J.; Nagarathna, R.; Bali, Y.; Nagendra, H.R. Effect of an integrated approach of yoga therapy on quality of life in osteoarthritis of the knee joint: A randomized control study. Int. J. Yoga 2011, 4, 55. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.Y.-S.; Chan, F.W.-K.; Wong, R.L.-P.; Chu, M.-C.; Lam, Y.-Y.K.; Mercer, S.W.; Ma, S.H. Comparing the effectiveness of mindfulness-based stress reduction and multidisciplinary intervention programs for chronic pain: A randomized comparative trial. Clin. J. Pain 2011, 27, 724–734. [Google Scholar] [CrossRef]
- Schmidt, S.; Grossman, P.; Schwarzer, B.; Jena, S.; Naumann, J.; Walach, H. Treating fibromyalgia with mindfulness-based stress reduction: Results from a 3-armed randomized controlled trial. Pain 2011, 152, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Tekur, P.; Singphow, C.; Nagendra, H.R.; Raghuram, N. Effect of short-term intensive yoga program on pain, functional disability and spinal flexibility in chronic low back pain: A randomized control study. J. Altern. Complement. Med. 2008, 14, 637–644. [Google Scholar] [CrossRef]
- Zautra, A.J.; Davis, M.C.; Reich, J.W.; Nicassario, P.; Tennen, H.; Finan, P.; Kratz, A.; Parrish, B.; Irwin, M.R. Comparison of cognitive behavioral and mindfulness meditation interventions on adaptation to rheumatoid arthritis for patients with and without history of recurrent depression. J. Consult. Clin. Psychol. 2008, 76, 408. [Google Scholar] [CrossRef]
- Pradhan, E.K.; Baumgarten, M.; Langenberg, P.; Handwerger, B.; Gilpin, A.K.; Magyari, T.; Hochberg, M.C.; Berman, B.M. Effect of mindfulness-based stress reduction in rheumatoid arthritis patients. Arthritis Care Res. 2007, 57, 1134–1142. [Google Scholar] [CrossRef]
- Cherup, N.P.; Strand, K.L.; Lucchi, L.; Wooten, S.V.; Luca, C.; Signorile, J.F. Yoga Meditation Enhances Proprioception and Balance in Individuals Diagnosed with Parkinson’s Disease. Percept. Mot. Ski. 2021, 128, 304–323. [Google Scholar] [CrossRef]
- Jong, M.C.; Boers, I.; van Wietmarschen, H.; Tromp, E.; Busari, J.; Wennekes, R.; Snoeck, I.; Bekhof, J.; Vlieger, A. Hypnotherapy or transcendental meditation versus progressive muscle relaxation exercises in the treatment of children with primary headaches: A multi-centre, pragmatic, randomised clinical study. Eur. J. Pediatr. 2019, 178, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalera, C.; Rovaris, M.; Mendozzi, L.; Pugnetti, L.; Garegnani, M.; Castelnuovo, G.; Molinari, E.; Pagnini, F. Online meditation training for people with multiple sclerosis: A randomized controlled trial. Mult. Scler. J. 2019, 25, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Wachholtz, A.B.; Malone, C.D.; Pargament, K.I. Effect of different meditation types on migraine headache medication use. Behav. Med. 2017, 43, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Pagnini, F.; Marconi, A.; Tagliaferri, A.; Manzoni, G.M.; Gatto, R.; Fabiani, V.; Gragnano, G.; Rossi, G.; Volpato, E.; Banfi, P. Meditation training for people with amyotrophic lateral sclerosis: A randomized clinical trial. Eur. J. Neurol. 2017, 24, 578–586. [Google Scholar] [CrossRef]
- Advocat, J.; Enticott, J.; Vandenberg, B.; Hassed, C.; Hester, J.; Russell, G. The effects of a mindfulness-based lifestyle program for adults with Parkinson’s disease: A mixed methods, wait list controlled randomised control study. BMC Neurol. 2016, 16, 166. [Google Scholar] [CrossRef] [Green Version]
- Najafidoulatabad, S.; Mohebbi, Z. Yoga effects on physical activity and sexual satisfaction among Iranian women with multiple sclerosis: A randomized controlled trial. Afr. J. Tradit. Complement. Altern. Med. 2014, 11, 78–82. [Google Scholar] [CrossRef] [Green Version]
- Pickut, B.A.; Van Hecke, W.; Kerckhofs, E.; Mariën, P.; Vanneste, S.; Cras, P.; Parizel, P.M. Mindfulness based intervention in Parkinson’s disease leads to structural brain changes on MRI: A randomized controlled longitudinal trial. Clin. Neurol. Neurosurg. 2013, 115, 2419–2425. [Google Scholar] [CrossRef]
- Wachholtz, A.B.; Pargament, K.I. Migraines and meditation: Does spirituality matter? J. Behav. Med. 2008, 31, 351–366. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kang, J. Effect of virtual reality meditation on sleep quality of intensive care unit patients: A randomised controlled trial. Intensive Crit. Care Nurs. 2020, 59, 102849. [Google Scholar] [CrossRef]
- Cramer, H.; Sellin, C.; Schumann, D.; Dobos, G. Yoga in arterial hypertension: A three-armed, randomized controlled trial. Dtsch. Ärzteblatt Int. 2018, 115, 833. [Google Scholar]
- Blom, K.; Baker, B.; How, M.; Dai, M.; Irvine, J.; Abbey, S.; Abramson, B.L.; Myers, M.G.; Kiss, A.; Perkins, N.J. Hypertension analysis of stress reduction using mindfulness meditation and yoga: Results from the harmony randomized controlled trial. Am. J. Hypertens. 2014, 27, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Jayadevappa, R.; Johnson, J.C.; Bloom, B.S.; Nidich, S.; Desai, S.; Chhatre, S.; Raziano, D.B.; Schneider, R.H. Effectiveness of transcendental meditation on functional capacity and quality of life of African Americans with congestive heart failure: A randomized control study. Ethn. Dis. 2007, 17, 72. [Google Scholar] [PubMed]
- Paul-Labrador, M.; Polk, D.; Dwyer, J.H.; Velasquez, I.; Nidich, S.; Rainforth, M.; Schneider, R.; Merz, C.N.B. Effects of a randomized controlled trial of transcendental meditation on components of the metabolic syndrome in subjects with coronary heart disease. Arch. Intern. Med. 2006, 166, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.H.; Alexander, C.N.; Staggers, F.; Orme-Johnson, D.W.; Rainforth, M.; Salerno, J.W.; Sheppard, W.; Castillo-Richmond, A.; Barnes, V.A.; Nidich, S.I. A randomized controlled trial of stress reduction in African Americans treated for hypertension for over one year. Am. J. Hypertens. 2005, 18, 88–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Richmond, A.; Schneider, R.H.; Alexander, C.N.; Cook, R.; Myers, H.; Nidich, S.; Haney, C.; Rainforth, M.; Salerno, J. Effects of stress reduction on carotid atherosclerosis in hypertensive African Americans. Stroke 2000, 31, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.B.; Mahnert, N.D.; Foote, J.; Saunders, K.T.; Mourad, J.; Huberty, J. Mindfulness Effects in Obstetric and Gynecology Patients During the Coronavirus Disease 2019 (COVID-19) Pandemic: A Randomized Controlled Trial. Obstet. Gynecol. 2021, 137, 1032. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G.; Newton, S.; Calvete, C.C.; Birch, J.; Dodds, J.; Steed, L.; Rivas, C.; Khan, K.; Röhricht, F.; Taylor, S. MEMPHIS: A smartphone app using psychological approaches for women with chronic pelvic pain presenting to gynaecology clinics: A randomised feasibility trial. BMJ Open 2020, 10, e030164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, N.-Y.; Kim, S.-D. Effects of a yoga program on menstrual cramps and menstrual distress in undergraduate students with primary dysmenorrhea: A single-blind, randomized controlled trial. J. Altern. Complement. Med. 2016, 22, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Jayabharathi, B.; Judie, A. Complementary health approach to quality of life in menopausal women: A community-based interventional study. Clin. Interv. Aging 2014, 9, 1913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, S.; Khandwe, R.; Bapat, D.; Deshmukh, U. Effect of yoga on menopausal symptoms. Menopause Int. 2011, 17, 78–81. [Google Scholar] [CrossRef]
- Chattha, R.; Raghuram, N.; Venkatram, P.; Hongasandra, N.R. Treating the climacteric symptoms in Indian women with an integrated approach to yoga therapy: A randomized control study. Menopause 2008, 15, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Chattha, R.; Nagarathna, R.; Padmalatha, V.; Nagendra, H. Effect of yoga on cognitive functions in climacteric syndrome: A randomised control study. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Izgu, N.; Gok Metin, Z.; Karadas, C.; Ozdemir, L.; Metinarikan, N.; Corapcıoglu, D. Progressive muscle relaxation and mindfulness meditation on neuropathic pain, fatigue, and quality of life in patients with type 2 diabetes: A randomized clinical trial. J. Nurs. Scholarsh. 2020, 52, 476–487. [Google Scholar] [CrossRef]
- Imeni, M.; Sabouhi, F.; Abazari, P.; Iraj, B. The effect of spiritual care on the body image of patients undergoing amputation due to type 2 diabetes: A randomized clinical trial. Iran. J. Nurs. Midwifery Res. 2018, 23, 322. [Google Scholar] [PubMed]
- Adler, E.; Dhruva, A.; Moran, P.J.; Daubenmier, J.; Acree, M.; Epel, E.S.; Bacchetti, P.; Prather, A.A.; Mason, A.; Hecht, F.M. Impact of a mindfulness-based weight-loss intervention on sleep quality among adults with obesity: Data from the SHINE randomized controlled trial. J. Altern. Complement. Med. 2017, 23, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, H.Y.; Lee, H.; Park, J. Comparison of the effects of K orean mindfulness-based stress reduction, walking, and patient education in diabetes mellitus. Nurs. Health Sci. 2015, 17, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.K.; Kristeller, J.L.; Headings, A.; Nagaraja, H. Comparison of a mindful eating intervention to a diabetes self-management intervention among adults with type 2 diabetes: A randomized controlled trial. Health Educ. Behav. 2014, 41, 145–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarino, V.; Kondwani, K.A.; Kelley, M.E.; Murrah, N.V.; Boyd, L.; Ahmed, Y.; Meng, Y.X.; Gibbons, G.H.; Hooper, W.C.; De Staercke, C. Effect of meditation on endothelial function in Black Americans with metabolic syndrome: A randomized trial. Psychosom. Med. 2013, 75, 591. [Google Scholar] [CrossRef] [Green Version]
- Dada, T.; Bhai, N.; Midha, N.; Shakrawal, J.; Kumar, M.; Chaurasia, P.; Gupta, S.; Angmo, D.; Yadav, R.; Dada, R. Effect of mindfulness meditation on intraocular pressure and trabecular meshwork gene expression: A randomized controlled trial. Am. J. Ophthalmol. 2021, 223, 308–321. [Google Scholar] [CrossRef] [PubMed]
- Gagrani, M.; Faiq, M.A.; Sidhu, T.; Dada, R.; Yadav, R.K.; Sihota, R.; Kochhar, K.P.; Verma, R.; Dada, T. Meditation enhances brain oxygenation, upregulates BDNF and improves quality of life in patients with primary open angle glaucoma: A randomized controlled trial. Restor. Neurol. Neurosci. 2018, 36, 741–753. [Google Scholar] [CrossRef]
- Dada, T.; Mittal, D.; Mohanty, K.; Faiq, M.A.; Bhat, M.A.; Yadav, R.K.; Sihota, R.; Sidhu, T.; Velpandian, T.; Kalaivani, M. Mindfulness meditation reduces intraocular pressure, lowers stress biomarkers and modulates gene expression in glaucoma: A randomized controlled trial. J. Glaucoma 2018, 27, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Arif, M.; Sadlier, M.; Rajenderkumar, D.; James, J.; Tahir, T. A randomised controlled study of mindfulness meditation versus relaxation therapy in the management of tinnitus. J. Laryngol. Otol. 2017, 131, 501–507. [Google Scholar] [CrossRef] [PubMed]
- McKenna, L.; Marks, E.M.; Hallsworth, C.A.; Schaette, R. Mindfulness-based cognitive therapy as a treatment for chronic tinnitus: A randomized controlled trial. Psychother. Psychosom. 2017, 86, 351–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haisley, K.R.; Straw, O.J.; Müller, D.T.; Antiporda, M.A.; Zihni, A.M.; Reavis, K.M.; Bradley, D.D.; Dunst, C.M. Feasibility of implementing a virtual reality program as an adjuvant tool for peri-operative pain control; results of a randomized controlled trial in minimally invasive foregut surgery. Complement. Ther. Med. 2020, 49, 102356. [Google Scholar] [CrossRef]
- Korterink, J.J.; Ockeloen, L.E.; Hilbink, M.; Benninga, M.A.; Deckers-Kocken, J.M. Yoga therapy for abdominal pain-related functional gastrointestinal disorders in children: A randomized controlled trial. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berrill, J.W.; Sadlier, M.; Hood, K.; Green, J.T. Mindfulness-based therapy for inflammatory bowel disease patients with functional abdominal symptoms or high perceived stress levels. J. Crohn’s Colitis 2014, 8, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.L.; Yeh, M.L.; Lai, Y.H.; Lin, K.C.; Yu, C.J.; Chang, J.S. Two-month breathing-based walking improves anxiety, depression, dyspnoea and quality of life in chronic obstructive pulmonary disease: A randomised controlled study. J. Clin. Nurs. 2019, 28, 3632–3640. [Google Scholar] [CrossRef] [PubMed]
- Kuloor, A.; Kumari, S.; Metri, K. Impact of yoga on psychopathologies and quality of life in persons with HIV: A randomized controlled study. J. Bodyw. Mov. Ther. 2019, 23, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Sudhanshu, A.; Sharma, U.; Vadiraja, H.; Rana, R.K.; Singhal, R. Impact of yoga on periodontal disease and stress management. Int. J. Yoga 2017, 10, 121. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.R.; Reilly-Spong, M.; Park, T.; Zhao, R.; Gurvich, O.V.; Ibrahim, H.N. Telephone-adapted Mindfulness-based Stress Reduction (tMBSR) for patients awaiting kidney transplantation. Contemp. Clin. Trials 2017, 57, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Brazier, A.; Mulkins, A.; Verhoef, M. Evaluating a yogic breathing and meditation intervention for individuals living with HIV/AIDS. Am. J. Health Promot. 2006, 20, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Manocha, R.; Marks, G.; Kenchington, P.; Peters, D.; Salome, C. Sahaja yoga in the management of moderate to severe asthma: A randomised controlled trial. Thorax 2002, 57, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Cullen, B.; Eichel, K.; Lindahl, J.R.; Rahrig, H.; Kini, N.; Flahive, J.; Britton, W.B. The contributions of focused attention and open monitoring in mindfulness-based cognitive therapy for affective disturbances: A 3-armed randomized dismantling trial. PLoS ONE 2021, 16, e0244838. [Google Scholar] [CrossRef] [PubMed]
- Bressington, D.; Mui, J.; Yu, C.; Leung, S.F.; Cheung, K.; Wu, C.S.T.; Bollard, M.; Chien, W.T. Feasibility of a group-based laughter yoga intervention as an adjunctive treatment for residual symptoms of depression, anxiety and stress in people with depression. J. Affect. Disord. 2019, 248, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Tolahunase, M.R.; Sagar, R.; Dada, R. 5-HTTLPR and MTHFR 677C > T polymorphisms and response to yoga-based lifestyle intervention in major depressive disorder: A randomized active-controlled trial. Indian J. Psychiatry 2018, 60, 410. [Google Scholar]
- Tolahunase, M.R.; Sagar, R.; Faiq, M.; Dada, R. Yoga-and meditation-based lifestyle intervention increases neuroplasticity and reduces severity of major depressive disorder: A randomized controlled trial. Restor. Neurol. Neurosci. 2018, 36, 423–442. [Google Scholar] [CrossRef] [PubMed]
- Chu, I.-H.; Wu, W.-L.; Lin, I.-M.; Chang, Y.-K.; Lin, Y.-J.; Yang, P.-C. Effects of yoga on heart rate variability and depressive symptoms in women: A randomized controlled trial. J. Altern. Complement. Med. 2017, 23, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Winnebeck, E.; Fissler, M.; Gärtner, M.; Chadwick, P.; Barnhofer, T. Brief training in mindfulness meditation reduces symptoms in patients with a chronic or recurrent lifetime history of depression: A randomized controlled study. Behav. Res. Ther. 2017, 99, 124–130. [Google Scholar] [CrossRef] [Green Version]
- de Jong, M.; Lazar, S.W.; Hug, K.; Mehling, W.E.; Hölzel, B.K.; Sack, A.T.; Peeters, F.; Ashih, H.; Mischoulon, D.; Gard, T. Effects of mindfulness-based cognitive therapy on body awareness in patients with chronic pain and comorbid depression. Front. Psychol. 2016, 7, 967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesa, A.; Castagner, V.; Andrisano, C.; Serretti, A.; Mandelli, L.; Porcelli, S.; Giommi, F. Mindfulness-based cognitive therapy vs. psycho-education for patients with major depression who did not achieve remission following antidepressant treatment. Psychiatry Res. 2015, 226, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.G.; Crane, C.; Barnhofer, T.; Brennan, K.; Duggan, D.S.; Fennell, M.J.; Hackmann, A.; Krusche, A.; Muse, K.; Von Rohr, I.R. Mindfulness-based cognitive therapy for preventing relapse in recurrent depression: A randomized dismantling trial. J. Consult. Clin. Psychol. 2014, 82, 275. [Google Scholar] [CrossRef] [PubMed]
- Britton, W.B.; Haynes, P.L.; Fridel, K.W.; Bootzin, R.R. Mindfulness-based cognitive therapy improves polysomnographic and subjective sleep profiles in antidepressant users with sleep complaints. Psychother. Psychosom. 2012, 81, 296–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keune, P.M.; Bostanov, V.; Hautzinger, M.; Kotchoubey, B. Mindfulness-based cognitive therapy (MBCT), cognitive style, and the temporal dynamics of frontal EEG alpha asymmetry in recurrently depressed patients. Biol. Psychol. 2011, 88, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Britton, W.B.; Haynes, P.L.; Fridel, K.W.; Bootzin, R.R. Polysomnographic and subjective profiles of sleep continuity before and after mindfulness-based cognitive therapy in partially remitted depression. Psychosom. Med. 2010, 72, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, A.J.; Malaktaris, A.L.; Casmar, P.; Baca, S.A.; Golshan, S.; Harrison, T.; Negi, L. Compassion meditation for posttraumatic stress disorder in veterans: A randomized proof of concept study. J. Trauma. Stress 2019, 32, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Bormann, J.E.; Thorp, S.R.; Smith, E.; Glickman, M.; Beck, D.; Plumb, D.; Zhao, S.; Ackland, P.E.; Rodgers, C.S.; Heppner, P. Individual treatment of posttraumatic stress disorder using mantram repetition: A randomized clinical trial. Am. J. Psychiatry 2018, 175, 979–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahbeh, H.; Goodrich, E.; Goy, E.; Oken, B.S. Mechanistic pathways of mindfulness meditation in combat veterans with posttraumatic stress disorder. J. Clin. Psychol. 2016, 72, 365–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.Y.; Zaharlick, A.; Akers, D. Impact of meditation on mental health outcomes of female trauma survivors of interpersonal violence with co-occurring disorders: A randomized controlled trial. J. Interpers. Violence 2017, 32, 2139–2165. [Google Scholar] [CrossRef] [PubMed]
- Seppälä, E.M.; Nitschke, J.B.; Tudorascu, D.L.; Hayes, A.; Goldstein, M.R.; Nguyen, D.T.; Perlman, D.; Davidson, R.J. Breathing-based meditation decreases posttraumatic stress disorder symptoms in US Military veterans: A randomized controlled longitudinal study. J. Trauma. Stress 2014, 27, 397–405. [Google Scholar] [CrossRef]
- Catani, C.; Kohiladevy, M.; Ruf, M.; Schauer, E.; Elbert, T.; Neuner, F. Treating children traumatized by war and Tsunami: A comparison between exposure therapy and meditation-relaxation in North-East Sri Lanka. BMC Psychiatry 2009, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Muratori, P.; Conversano, C.; Levantini, V.; Masi, G.; Milone, A.; Villani, S.; Bögels, S.; Gemignani, A. Exploring the efficacy of a mindfulness program for boys with attention-deficit hyperactivity disorder and oppositional defiant disorder. J. Atten. Disord. 2021, 25, 1544–1553. [Google Scholar] [CrossRef]
- Janssen, L.; Kan, C.C.; Carpentier, P.J.; Sizoo, B.; Hepark, S.; Schellekens, M.P.; Donders, A.R.T.; Buitelaar, J.K.; Speckens, A.E. Mindfulness-based cognitive therapy v. treatment as usual in adults with ADHD: A multicentre, single-blind, randomised controlled trial. Psychol. Med. 2019, 49, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Hoxhaj, E.; Sadohara, C.; Borel, P.; D’Amelio, R.; Sobanski, E.; Müller, H.; Feige, B.; Matthies, S.; Philipsen, A. Mindfulness vs psychoeducation in adult ADHD: A randomized controlled trial. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 321–335. [Google Scholar] [CrossRef]
- Boettcher, J.; Åström, V.; Påhlsson, D.; Schenström, O.; Andersson, G.; Carlbring, P. Internet-based mindfulness treatment for anxiety disorders: A randomized controlled trial. Behav. Ther. 2014, 45, 241–253. [Google Scholar] [CrossRef] [Green Version]
- Goldin, P.; Ziv, M.; Jazaieri, H.; Hahn, K.; Gross, J.J. MBSR vs aerobic exercise in social anxiety: fMRI of emotion regulation of negative self-beliefs. Soc. Cogn. Affect. Neurosci. 2013, 8, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Koszycki, D.; Benger, M.; Shlik, J.; Bradwejn, J. Randomized trial of a meditation-based stress reduction program and cognitive behavior therapy in generalized social anxiety disorder. Behav. Res. Ther. 2007, 45, 2518–2526. [Google Scholar] [CrossRef]
- Huberty, J.L.; Green, J.; Puzia, M.E.; Larkey, L.; Laird, B.; Vranceanu, A.-M.; Vlisides-Henry, R.; Irwin, M.R. Testing a mindfulness meditation mobile app for the treatment of sleep-related symptoms in adults with sleep disturbance: A randomized controlled trial. PLoS ONE 2021, 16, e0244717. [Google Scholar] [CrossRef]
- Black, D.S.; O’Reilly, G.A.; Olmstead, R.; Breen, E.C.; Irwin, M.R. Mindfulness meditation and improvement in sleep quality and daytime impairment among older adults with sleep disturbances: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Ong, J.C.; Manber, R.; Segal, Z.; Xia, Y.; Shapiro, S.; Wyatt, J.K. A randomized controlled trial of mindfulness meditation for chronic insomnia. Sleep 2014, 37, 1553–1563. [Google Scholar] [CrossRef] [Green Version]
- Zgierska, A.E.; Burzinski, C.A.; Mundt, M.P.; McClintock, A.S.; Cox, J.; Coe, C.L.; Miller, M.M.; Fleming, M.F. Mindfulness-based relapse prevention for alcohol dependence: Findings from a randomized controlled trial. J. Subst. Abus. Treat. 2019, 100, 8–17. [Google Scholar] [CrossRef]
- Hsu, S.H.; Collins, S.E.; Marlatt, G.A. Examining psychometric properties of distress tolerance and its moderation of mindfulness-based relapse prevention effects on alcohol and other drug use outcomes. Addict. Behav. 2013, 38, 1852–1858. [Google Scholar] [CrossRef]
- Loizzo, J. Meditation research, past, present, and future: Perspectives from the Nalanda contemplative science tradition. Ann. N. Y. Acad. Sci. 2014, 1307, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, P.M.; Powell-Griner, E.; McFann, K.; Nahin, R.L. Complementary and Alternative Medicine Use among Adults: United States, 2002. In Seminars in Integrative Medicine; Elsevier: Amsterdam, The Netherlands, 2004; pp. 54–71. [Google Scholar]
- Upchurch, D.M.; Johnson, P.J. Gender differences in prevalence, patterns, purposes, and perceived benefits of meditation practices in the United States. J. Women’s Health 2019, 28, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Gibby, C.C.; Aday, L.A.; Anderson, K.O.; Mendoza, T.R.; Cleeland, C.S. Pain, depression, and fatigue in community-dwelling adults with and without a history of cancer. J. Pain Symptom Manag. 2006, 32, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Kwekkeboom, K.L.; Cherwin, C.H.; Lee, J.W.; Wanta, B. Mind-body treatments for the pain-fatigue-sleep disturbance symptom cluster in persons with cancer. J. Pain Symptom Manag. 2010, 39, 126–138. [Google Scholar] [CrossRef]
- Shapiro, D.H.; Giber, D. Meditation and psychotherapeutic effects: Self-regulation strategy and altered state of consciousness. Arch. Gen. Psychiatry 1978, 35, 294–302. [Google Scholar] [CrossRef]
- Wang, J.; Wu, X.; Lai, W.; Long, E.; Zhang, X.; Li, W.; Zhu, Y.; Chen, C.; Zhong, X.; Liu, Z. Prevalence of depression and depressive symptoms among outpatients: A systematic review and meta-analysis. BMJ Open 2017, 7, e017173. [Google Scholar] [CrossRef] [Green Version]
- Gullich, I.; Ramos, A.B.; Zan, T.R.A.; Scherer, C.; Mendoza-Sassi, R.A. Prevalence of anxiety in patients admitted to a university hospital in southern Brazil and associated factors. Rev. Bras. Epidemiol. 2013, 16, 644–657. [Google Scholar] [CrossRef] [Green Version]
- Kasala, E.R.; Bodduluru, L.N.; Maneti, Y.; Thipparaboina, R. Effect of meditation on neurophysiological changes in stress mediated depression. Complement. Ther. Clin. Pract. 2014, 20, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Finsterer, J.; Mahjoub, S.Z. Fatigue in healthy and diseased individuals. Am. J. Hosp. Palliat. Med. 2014, 31, 562–575. [Google Scholar] [CrossRef]
- Ravindra, P.; Kutty, B.M. Functional importance of sleep: An overview. Indian J. Sleep Med. 2012, 7, 42–44. [Google Scholar]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Querstret, D.; Morison, L.; Dickinson, S.; Cropley, M.; John, M. Mindfulness-based stress reduction and mindfulness-based cognitive therapy for psychological health and well-being in nonclinical samples: A systematic review and meta-analysis. Int. J. Stress Manag. 2020, 27, 394–411. [Google Scholar] [CrossRef]
- Della Valle, E.; Palermi, S.; Aloe, I.; Marcantonio, R.; Spera, R.; Montagnani, S.; Sirico, F. Effectiveness of Workplace Yoga Interventions to Reduce Perceived Stress in Employees: A Systematic Review and Meta-Analysis. J. Funct. Morphol. Kinesiol. 2020, 5, 33. [Google Scholar] [CrossRef]
- Selye, H. Stress in Health and Disease; Butterworth-Heinemann: Oxford, UK, 2013. [Google Scholar]
- Huebner, J.; Prott, F.J.; Micke, O.; Muecke, R.; Senf, B.; Dennert, G.; Muenstedt, K. Online survey of cancer patients on complementary and alternative medicine. Oncol. Res. Treat. 2014, 37, 304–308. [Google Scholar] [CrossRef]
- Davidson, R.J.; Kaszniak, A.W. Conceptual and methodological issues in research on mindfulness and meditation. Am. Psychol. 2015, 70, 581. [Google Scholar] [CrossRef]
- Kessels, E.; Husson, O.; Van der Feltz-Cornelis, C.M. The effect of exercise on cancer-related fatigue in cancer survivors: A systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 2018, 14, 479. [Google Scholar] [CrossRef] [Green Version]
- Estévez-López, F.; Maestre-Cascales, C.; Russell, D.; Álvarez-Gallardo, I.C.; Rodriguez-Ayllon, M.; Hughes, C.M.; Davison, G.W.; Sañudo, B.; McVeigh, J.G. Effectiveness of exercise on fatigue and sleep quality in fibromyalgia: A systematic review and meta-analysis of randomized trials. Arch. Phys. Med. Rehabil. 2021, 102, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Razazian, N.; Kazeminia, M.; Moayedi, H.; Daneshkhah, A.; Shohaimi, S.; Mohammadi, M.; Jalali, R.; Salari, N. The impact of physical exercise on the fatigue symptoms in patients with multiple sclerosis: A systematic review and meta-analysis. BMC Neurol. 2020, 20, 93. [Google Scholar] [CrossRef]
- Niemeijer, A.; Lund, H.; Stafne, S.N.; Ipsen, T.; Goldschmidt, C.L.; Jørgensen, C.T.; Juhl, C.B. Adverse events of exercise therapy in randomised controlled trials: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 1073–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groenvold, M.; Petersen, M.A.; Idler, E.; Bjorner, J.B.; Fayers, P.M.; Mouridsen, H.T. Psychological distress and fatigue predicted recurrence and survival in primary breast cancer patients. Breast Cancer Res. Treat. 2007, 105, 209–219. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Count |
|---|---|
| N. of RCT | 104 |
| N. of participants (female) | 10,139 (7022) |
| Mean N. of participant (the number ± SD) | 97.3 ± 71.4 |
| Mean age (year ± SD) A | 47.6 ± 13.1 |
| Mean treatment period (week ± SD) | 10.3 ± 9.1 |
| Disorders of the participants (N. of RCT, %) | 104 (100) |
| Cancer | 16 (15.4) |
| Diseases of the musculoskeletal and connective tissues | 14 (13.5) |
| Affective mood disorder | 13 (12.5) |
| Disease of the nervous system | 9 (8.7) |
| Disease of the circulatory system | 7 (6.7) |
| Gynecological disorder | 7 (6.7) |
| Post-traumatic stress disorder (PTSD) | 7 (6.7) |
| Metabolic disorder | 6 (5.8) |
| Disease of otorhinolaryngology | 5 (4.8) |
| Others | 20 (19.2) |
| Type of meditation B (N. of RCTs, %) | |
| Mindfulness-based meditation | 51 (49.0) |
| Yoga-based meditation | 32 (30.8) |
| Transcendental meditation | 14 (13.5) |
| Others | 11 (10.6) |
| Main clinical outcomes B, C (N. of RCTs, %) | |
| Mean N. of measurements per RCT (the number ± SD) | 3.9 ± 2.5 |
| Depressive mood | 56 (53.8) |
| Feeling anxious | 40 (38.5) |
| Quality of life (QoL) | 32 (30.8) |
| Stress | 31 (29.8) |
| Sleep | 23 (22.1) |
| Pain | 22 (21.2) |
| Fatigue | 19 (18.3) |
| Disorder [Reference] | Kind of Meditation (Category *) | N. of Participants # (N. of Arms, Controls) | Period (Weeks) | Clinical Finding (Statistical) | |
|---|---|---|---|---|---|
| Significant | Not Significant | ||||
| Cancer | |||||
| Breast cancer [16] | Kirtan Kriya (Y + T) | 31 (2, music listening) | 8 | depressive mood, fatigue, cognitive functions A, | feeling anxious, stress, self-efficacy |
| Breast cancer [17] | MM (M) | 92 (3, muscle relaxation, education) | 12 | fatigue A | QoL |
| Breast cancer [18] | Self-care toolkit (other) | 100 (2, usual care) | 2 | pain | depressive mood, feeling anxious A, sleep, fatigue, social role, physical functions, nausea |
| Breast cancer [19] | Tai chi (other) | 90 (2, CBT) | 12 | depressive mood, sleep A, fatigue | - |
| Breast cancer [20] | Yoga (Y) | 69 (2, counseling) | 24 | depressive mood, feeling anxious, cancer symptoms | - |
| Breast cancer [21] | Hatha yoga (Y) | 40 (2, waitlist) | 12 | QoL, fatigue, menopausal symptoms A | depressive mood, feeling anxious |
| Breast cancer [22] | YOCAS (Y) | 167 (2, waitlist) | 4 | fatigue | - |
| Breast cancer [23] | Qigong + Tai chi (other) | 87 (2, sham qigong) | 12 | fatigue A | depressive mood, sleep |
| Breast cancer [24] | Mindful awareness practices (M) | 71 (2, usual care) | 6 | stress A, sleep, fatigue, hot flashes, affect | depressive mood A, pain, fear, intrusive thoughts |
| Breast cancer [25] | Mindfulness-based cancer recovery (M) | 271 (3, supportive therapy, stress management) | 8 | stress, mood A | health-related functions, social support |
| Cancer [26] | Yoga (Y) | 410 (2, usual care) | 4 | sleep A | - |
| Breast cancer [27] | MBSR (M) | 336 (2, usual care) | 8 | - | sleep A |
| Breast cancer [28] | Danhak (other) | 102 (2, usual care) | 6 | feeling anxious A, fatigue, QoL | depressive mood A, dyspnea |
| Cancer [29] | MBSR (M) | 71 (2, waitlist) | 24 | - | depressive mood, feeling anxious, stress, intrusive thoughts, avoidance, hyperarousal, positive thinking, self-efficacy |
| Breast cancer [30] | TM (T) | 130 (2, usual care) | 72 | QoL A, spiritual well-being, mental health | vitality |
| Cancer [31] | MBSR (M) | 90 (2, waitlist) | 7 | depressive mood, feeling anxious, stress, anger, vigor, confusion, mood, habitual patterns, irritability | fatigue, peripheral symptoms |
| Diseases of the musculoskeletal system and connective tissues | |||||
| Rheumatoid arthritis [32] | Yoga-based mind-body intervention (Y) | 72 (2, usual care) | 8 | depressive mood, inflammatory markers A | - |
| Knee osteoarthritis [33] | Mantra (Y + T) | 22 (2, music listening) | 8 | sleep, mood | QoL, stress, pain A, osteoarthritis symptoms A |
| Fibromyalgia [34] | Meditation awareness training (M) | 148 (2, CBT) | 8 | depressive mood A, feeling anxious A, stress A, sleep A, pain A, fibromyalgia symptoms A, nonattachment, civic engagement | - |
| Chronic low back pain [35] | MBSR (M) | 341 (3, CBT, usual care) | 8 | pain A, disability A, global impression | depressive mood, feeling anxious, QoL |
| Chronic low back pain [36] | Jyoti meditation (Y) | 68 (2, exercise) | 8 | stress | depressive mood, feeling anxious, QoL, pain A, disability |
| Fibromyalgia [37] | MBSR (M) | 91 (2, usual care) | 8 | stress, sleep, fatigue, fibromyalgia symptoms | physical function, salivary cortisol |
| Chronic neck pain [38] | Jyoti meditation (Y) | 89 (2, exercise) | 8 | pain A | depressive mood, feeling anxious, QoL, stress |
| Chronic pain [39] | MBSR (M) | 109 (2, waitlist) | 8 | depressive mood, feeling anxious, pain, vitality A, general mental health, engagement | physical function, catastrophic thinking |
| Knee osteoarthritis [40] | Yoga (Y) | 250 (2, physiotherapy exercise) | 14 | QoL | - |
| Chronic pain [41] | MBSR (M) | 99 (2, multidisciplinary pain intervention) | 8 | vigorous activity | depressive mood, feeling anxious, QoL, pain A, fatigue, anger, confusion |
| Fibromyalgia [42] | MBSR (M) | 168 (3, nonspecific MBSR, waitlist) | 8 | - | depressive mood, feeling anxious, QoL A, sleep, pain, mindfulness |
| Chronic low back pain [43] | Yoga (Y) | 80 (2, exercise) | 1 | pain, flexibility | |
| Rheumatoid arthritis [44] | MM (M) | 106 (3, CBT, education) | 8 | - | depressive mood A, pain A, affect A, swelling, tenderness |
| Rheumatoid arthritis [45] | MBSR (M) | 63 (2, waitlist) | 8 | depressive mood A, rheumatoid arthritis symptoms A, mental well-being, mindfulness | |
| Diseases of the nervous system | |||||
| Parkinson’s disease [46] | Yoga (Y) | 33 (2, proprioceptive training) | 12 | parkinsonismA | - |
| Headaches [47] | TM (T) | 131 (3, hypnotherapy, muscle relaxation) | 12 | - | pain A, depressive mood, feeling anxious, somatization |
| Multiple sclerosis [48] | Online MBSR (M) | 121 (2, psychoeducation) | 8 | depressive mood, feeling anxious, QoL A, sleep | fatigue |
| Migraines [49] | Spiritual meditation (T) | 83 (4, internally & externally focused secular meditations, muscle relaxation) | 4 | pain | spirituality |
| Amyotrophic lateral sclerosis [50] | MBSR (M) | 100 (2, usual care) | 8 | depressive mood, feeling anxious, QoL A | mindfulness |
| Parkinson’s disease [51] | Mindfulness-based lifestyle (M) | 57 (2, waitlist) | 6 | stress, mindfulness | depressive mood, feeling anxious, parkinsonism A, |
| Multiple sclerosis [52] | Yoga (Y) | 60 (2, no treatment) | 12 | - | QoL |
| Parkinson’s disease [53] | MBSR (M) | 27 (2, usual care) | 8 | brain MRI (gray matter density) A | - |
| Migraine [54] | Spiritual meditation (T) | 83 (4, internally & externally focused secular meditations, muscle relaxation) | 4 | pain | depressive mood, feeling anxious, QoL, emotion, spirituality |
| Diseases of the circulatory system | |||||
| Heart disease [55] | VR meditation (other) | 48 (2, eye mask or ear plugs) | 1 day | sleep | - |
| Hypertension [56] | Yoga (Y) | 75 (3, yoga without posture, waitlist) | 12 | blood pressure A | depressive mood, feeling anxious, QoL, stress, heart rate |
| Hypertension [57] | MBSR (M) | 101 (2, waitlist) | 8 | - | blood pressure A |
| Congestive heart failure [58] | TM (T) | 23 (2, education) | 24 | physical functions A | depressive mood, QoL, stress |
| Coronary heart disease [59] | TM (T) | 103 (2, education) | 16 | blood pressure, anger | depressive mood, feeling anxious, stress, blood lipid level, exercise, HRV |
| Hypertension [60] | TM (T) | 150 (3, education, muscle relaxation) | 48 | blood pressure A | - |
| Carotid atherosclerosis [61] | TM (T) | 60 (2, education) | 24 | carotid intima-media thickness A | blood pressure, blood lipid level, weight |
| Gynecological disorders | |||||
| Gynecological disease [62] | Mobile app Calm (M) | 101 (2, usual care) | 4 | depressive mood, feeling anxious, stress A, sleep | - |
| Chronic pelvic pain [63] | Mobile app-based MM (M) | 90 (3, muscle relaxation, usual care) | 8 | - | pain A |
| Dysmenorrhea [64] | Yoga (Y) | 36 (2, no treatment) | 12 | stress, pain | - |
| Menopausal disorder [65] | Yoga (Y) | 260 (2, no treatment) | 18 | QoL A | - |
| Menopausal disorder [66] | Yoga (Y) | 180 (2, no treatment) | 12 | menopausal symptoms A | - |
| Menopausal disorder [67] | Yoga (Y) | 120 (2, exercise) | 8 | stress, vasomotor symptoms, personality | psychological symptoms, somatic symptoms |
| Menopausal disorder [68] | Yoga (Y) | 108 (2, exercise) | 8 | cognitive function A | vasomotor symptoms A |
| Metabolic disorders | |||||
| DM type 2 [69] | MBSR (M) | 69 (3, muscle relaxation, education) | 12 | - | QoL, pain A, fatigue |
| DM type 2 + amputation [70] | TM (T) | 54 (2, diabetic care training) | 4 | amputee body image A | - |
| Obesity [71] | MBSR (M) | 194 (2, muscle relaxation) | 22 | - | sleep A |
| DM type 2 [72] | MBSR (M) | 56 (3, walking, education) | 8 | inflammatory response | stressA, blood glucose A |
| DM type 2 [73] | Mindful eating intervention (M) | 52 (2, self-management) | 12 | - | depressive mood, feeling anxious, DM symptoms A, mindfulness |
| Metabolic syndrome [74] | Consciously resting meditation (Y + T) | 68 (2, education) | 12 | stress, vascular functions A | depressive mood, feeling anxious, hostility, anger, physical activity, metabolic & inflammatory markers |
| Diseases of otorhinolaryngology | |||||
| Glaucoma [75] | MM (M) | 60 (2, medication) | 3 | QoL, IOPA | - |
| Glaucoma [76] | Breathing meditation (other) | 60 (2, usual care) | 6 | - | QoL, IOPA, blood markers |
| Glaucoma [77] | MBSR (M) | 90 (2, usual care) | 3 | QoL, IOP A, blood markers | visual field |
| Tinnitus [78] | MM (M) | 61 (2, relaxation) | 15 | tinnitus symptoms A | depressive mood, feeling anxious, body temperature |
| Tinnitus [79] | MBCT (M) | 75 (2, relaxation) | 8 | tinnitus symptoms A, attention awareness | depressive mood, feeling anxious, stress A, social adjustment |
| Diseases of the digestive system | |||||
| Foregut surgery [80] | VR meditation (other) | 52 (2, usual care) | 1 day | - | feeling anxious, pain, nausea |
| Functional gastrointestinal disorders [81] | Yoga (Y) | 69 (2, usual care) | 10 | - | pain A, well-being |
| Inflammatory bowel disease [82] | Mindfulness-based therapy (M) | 66 (2, usual care) | 16 | - | stress, inflammatory bowel disease symptoms A, positive thinking, avoidance, seeking advice, self-blame |
| Others | |||||
| COPD [83] | Breathing-based walking (other) | 78 (2, usual care) | 8 | depressive mood, feeling anxious, COPD symptoms, | - |
| HIV [84] | Yoga (Y) | 60 (2, waitlist) | 8 | depressive mood, feeling anxious, QoL A, fatigue, well-being | - |
| Periodontitis [85] | Yoga (Y) | 80 (2, usual care) | 12 | stress, periodontitis symptoms | - |
| Renal disease [86] | Telephone MBSR (M) | 55 (2, telephone support) | 8 | depressive mood | feeling anxious A, QoL, sleep, pain, fatigue |
| HIV [87] | Yoga (Y) | 47 (2, usual care) | 12 | stress, positive affect A, mental well-being A, general health, social functions, cognitive functions | |
| Asthma [88] | Sahaja yoga (Y) | 47 (2, relaxation + group discussion + CBT-like exercise) | 16 | feeling anxious, fatigue, asthma symptoms A | depressive mood, QoL A, anger, vigor, confusion |
| Disorder [Reference] | Kind of Meditation (Category *) | N. of Participants # (N. of Arms, Controls) | Period (Weeks) | Clinical Finding (Statistical) | |
|---|---|---|---|---|---|
| Significant | Not Significant | ||||
| Mood disorder | |||||
| Affective disorder [89] | MBCT (M) | 104 (3, focused attention, open monitoring) | 8 | - | depressive mood A, feeling anxious A, stress A |
| Depression [12] | Sahaj Samadhi (Y) | 83 (2, usual care) | 12 | depressive mood, feeling anxious, global impression, | QoL, HRV A, physical activity, side effects |
| Depression [90] | Laughter yoga (Y) | 50 (2, usual care) | 4 | depressive mood, QoL | feeling anxious, stress |
| Depression [91] | Yoga-based lifestyle (Y) | 178 (2, medication) | 12 | depressive mood A | - |
| Depression [92] | Yoga-based lifestyle (Y) | 58 (2, no treatment) | 12 | depressive mood A, blood markers A | - |
| Depression [93] | Yoga (Y) | 26 (2, no treatment) | 12 | depressive mood, HRV | stress, heart rate |
| Depression [94] | MM (M) | 74 (2, psychoeducation + regular rest) | 2 | depressive mood A, mindfulness | - |
| Depression [95] | MBCT (M) | 29 (2, usual care) | 8 | interoceptive awareness | depressive mood, pain |
| Depression [96] | MBCT (M) | 43 (2, psychoeducation) | 26 | depressive mood, mindfulness, general mental health | feeling anxious |
| Depression [97] | MBCT (M) | 254 (3, CPE, usual care) | 8 | - | depressive mood A |
| Depression [98] | MBCT (M) | 24 (2, no treatment) | 8 | sleep | depressive mood |
| Depression [99] | MBCT (M) | 77 (2, waitlist) | 8 | depressive mood, rumination, mindfulness, positive thinking, negative thinking | |
| Depression [100] | MBCT (M) | 21 (2, waitlist) | 8 | sleep | depressive mood |
| Post-traumatic stress disorder (PTSD) | |||||
| PTSD [101] | CBCT (other) | 28 (2, Veteran. Calm) | 10 | PTSD symptoms A | alcohol use |
| PTSD [102] | Mantra (Y + T) | 173 (2, present-centered therapy) | 8 | sleep, PTSD symptoms A | QoL, general health, anger, well-being, mindfulness |
| PTSD [13] | TM (T) | 202 (3, prolonged exposure, education) | 12 | QoL, PTSD symptoms A, general health, mood | |
| PTSD [103] | MM (M) | 102 (4, MM + slow breathing, slow breathing, sitting quietly) | 6 | depressive mood, stress, sleep, PTSD symptoms A, global impression, adherence, respiration rate | affect, mindfulness, credibility, EEG, ECG, HRV |
| Trauma with co-occurring disorder [104] | Tibetan meditation (other) | 58 (2, usual care) | 6 | stress A, trauma symptoms | - |
| PTSD [105] | Yoga (Y) | 21 (2, waitlist) | 1 | feeling anxious, PTSD symptoms, arousal, respiration rate | depressive mood |
| PTSD [106] | Meditation-relaxation (other) | 31 (2, exposure therapy) | 4 | - | PTSD symptoms A, functional impairment, physical symptoms |
| Attention-deficit hyperactivity disorder (ADHD) | |||||
| ADHD + ODD [107] | MBSR (M) | 50 (2, waitlist) | 9 | ADHD symptoms | - |
| ADHD [108] | MBCT (M) | 120 (2, usual care) | 8 | ADHD symptoms A, mindfulness, compassion, mental health | executive functions |
| ADHD [109] | Mindful awareness practice (M) | 81 (2, psychoeducation) | 8 | mindfulness | depressive mood, QoL, ADHD symptoms A |
| Anxiety | |||||
| Anxiety disorder [110] | Mindful exercise + psychoeducation (M) | 91 (2, discussion forum) | 8 | depressive mood, feeling anxious A, QoL, sleep | - |
| Anxiety disorder [111] | MBSR (M) | 56 (2, exercise) | 8 | - | feeling anxious A |
| Social anxiety disorder [112] | MBSR (M) | 53 (2, CBT) | 8 | - | depressive mood, feeling anxious A, QoL, global impression A, social interaction A, social phobia A, interpersonal sensitivity |
| Sleep disorder | |||||
| Sleep disturbance [113] | Mobile app Calm (M) | 263 (2, waitlist) | 8 | sleep, fatigue A | - |
| Sleep disturbance [114] | Mindful awareness practice (M) | 49 (2, education) | 6 | depressive mood, sleep A, fatigue | feeling anxious, stress |
| Insomnia [115] | MBSR, MBTI (M) | 54 (3, self-monitoring) | 8 | sleep | - |
| Substance misuse disorder | |||||
| Alcohol dependence [116] | MBRP (M) | 112 (2, usual care) | 8 | - | stress, alcohol use A, mindfulness |
| Alcohol and other drug use disorder [117] | MBRP (M) | 168 (2, usual care) | 8 | - | alcohol or drug use, distress tolerance, mindfulness |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-Y.; Hong, S.-H.; Jang, S.-H.; Park, S.-H.; Noh, J.-H.; Seok, J.-M.; Jo, H.-J.; Son, C.-G.; Lee, E.-J. Systematic Review for the Medical Applications of Meditation in Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 1244. https://doi.org/10.3390/ijerph19031244
Kim D-Y, Hong S-H, Jang S-H, Park S-H, Noh J-H, Seok J-M, Jo H-J, Son C-G, Lee E-J. Systematic Review for the Medical Applications of Meditation in Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(3):1244. https://doi.org/10.3390/ijerph19031244
Chicago/Turabian StyleKim, Do-Young, Soo-Hwa Hong, Seung-Hyeon Jang, So-Hyeon Park, Jung-Hee Noh, Jung-Mi Seok, Hyun-Jeong Jo, Chang-Gue Son, and Eun-Jung Lee. 2022. "Systematic Review for the Medical Applications of Meditation in Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 3: 1244. https://doi.org/10.3390/ijerph19031244
APA StyleKim, D. -Y., Hong, S. -H., Jang, S. -H., Park, S. -H., Noh, J. -H., Seok, J. -M., Jo, H. -J., Son, C. -G., & Lee, E. -J. (2022). Systematic Review for the Medical Applications of Meditation in Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 19(3), 1244. https://doi.org/10.3390/ijerph19031244