
The Cost of Loneliness: Assessing the Social Relationships of the Elderly via an Abbreviated Sociotype Questionnaire for inside and outside the Clinic

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Component Studies
2.1.1. Study 1
2.1.2. Study 2
2.1.3. Study 3
2.1.4. Study 4
2.2. Participants
2.3. Procedure and Ethics
2.4. Statistical Procedure
- First phase: selection process of the most representative item within each of the three dimensions of the SOCQ. To accomplish this, the weights from the exploratory factor analysis by the Principal Component method were taken as references (previously making sure that these factors for elderly people were no different from those obtained for the general population).
- Second phase: for the selection of a 4th item, we searched among all the other discarded items (removing those previously selected), and we selected that which obtained the highest correlation with the GDS, Barthel, Pfeiffer, EPQ, UCLA, GHQ12, MMSE, EuroQol-5D, and Goldberg scales (taking into account that each test only applied to some determined population).
- Third phase: once we selected the 4 items, they were dichotomized assigning the value of 1 to the answers of the upper categories of the SOCQ and the value 0 to the remaining categories. Then, the validity of this new, “binary” scale was confirmed.
3. Results
3.1. SOCQ Differential Results in Study 1: The Aging Population versus General Population
3.2. Construction of the Abbreviated Geriatric Sociotype Scale (SOCG-4)
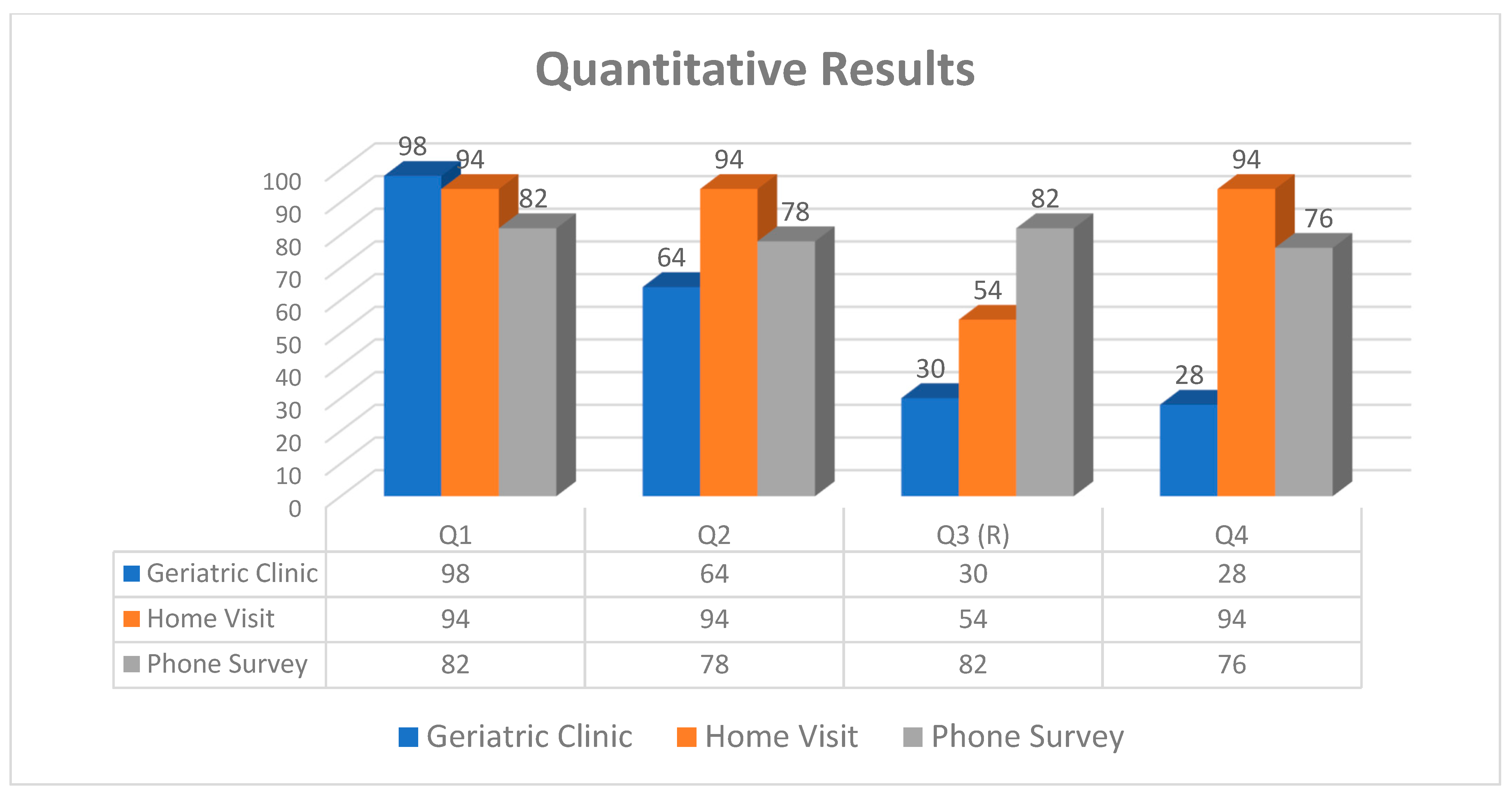
- I talk and relate with my family;
- I talk and relate with my friends;
- (R)It is difficult for me to make conversation with people I do not know;
- I have fun and laugh with my friends.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Use of SOCG-4
Appendix A.1. Comments from Interviewers
Appendix A.2. Quantitative Results

References
- Perissinotto, C.M.; Covinsky, K.E. Living Alone, Socially Isolated or Lonely—What are We Measuring? J. Gen. Intern. Med. 2014, 29, 1429–1431. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.; Cacioppo, S. Loneliness Is a Modern Epidemic in Need of Treatment. 2014, Volume 19, p. 2016. Available online: https://www.newscientist.com/article/dn26739-loneliness-is-a-modern-epidemic-in-need-of-treatment/ (accessed on 20 January 2022).
- Holt-Lunstad, J.; Robles, T.F.; Sbarra, A.D. Advancing social connection as a public health priority in the United States. Am. Psychol. 2017, 72, 517. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronson, N. Elderhood: Redefining Aging, Transforming Medicine, Reimagining Life; Bloomsbury Publishing: London, UK, 2019. [Google Scholar]
- WHO. Mental Health and Psychosocial Considerations during COVID-19 Outbreak; World Health Organization: Geneva, Switzerland, 2020; pp. 1–6. [Google Scholar]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; McKenna-Plumley, P.E.; McGlinchey, E.; Armour, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 9, e0239698. [Google Scholar] [CrossRef] [PubMed]
- Granovetter, M. The impact of social structure on economic outcomes. In The Sociology of Economic Life, 3rd ed.; Routledge: Oxfordshire, UK, 2018. [Google Scholar] [CrossRef]
- McPherson, M.; Smith-Lovin, L.; Brashears, M.E. Social isolation in America: Changes in core discussion networks over two decades. Am. Sociol. Rev. 2006, 71, 353–375. [Google Scholar] [CrossRef] [Green Version]
- Larg, A.; Moss, J.R. Cost-of-illness studies: A guide to critical evaluation. PharmacoEconomics 2011, 29, 653–671. [Google Scholar] [CrossRef]
- Mihalopoulos, C.; Le Khanh-Dao, L.; Chatterton, M.L.; Bucholc, J.; Holt-Lunstad, J.; Lim, M.H.; Engel, L. The economic costs of loneliness: A review of cost-of-illness and economic evaluation studies. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 823–836. [Google Scholar] [CrossRef]
- Putnam, R. Bowling Alone; Simon & Schuster: New York, NY, USA, 2000. [Google Scholar]
- Shankar, A.; McMunn, A.; Banks, J.; Steptoe, A. Loneliness, Social Isolation, and Behavioral and Biological Health Indicators in Older Adults. Health Psychol. 2011, 30, 377. [Google Scholar] [CrossRef] [Green Version]
- Shor, E.; Roelfs, D.J.; Yogev, T. The strength of family ties: A meta-analysis and meta-regression of self-reported social support and mortality. Soc. Netw. 2013, 35, 626–638. [Google Scholar] [CrossRef]
- Qualter, P.; Vanhalst, J.; Harris, R.; van Roekel, E.; van Roekel, E.; Lodder, G.; Bangee, M.; Maes, M.; Verhagen, M. Loneliness Across the Life Span. Perspect. Psychol. Sci. 2015, 10, 250–264. [Google Scholar] [CrossRef]
- Booth, R. Loneliness as a component of psychiatric disorders. Medscape Gen. Med. 2000, 2, 1–7. [Google Scholar]
- Grant, N.; Hamer, M.; Steptoe, A. Social isolation and stress-related cardiovascular, lipid, and cortisol responses. Ann. Behav. Med. 2009, 37, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacioppo, J.T.; Cacioppo, S.; Capitanio, J.P.; Cole, S.W. The neuroendocrinology of social isolation. Annu. Rev. Psychol. 2015, 66, 733–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruan, H.; Wu, C.F. Social interaction-mediated lifespan extension of Drosophila Cu/Zn superoxide dismutase mutants. Proc. Natl. Acad. Sci. USA 2008, 105, 7506–7510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doane, L.D.; Adam, E.K. Loneliness and cortisol: Momentary, day-to-day, and trait associations. Psychoneuroendocrinology 2010, 35, 430–441. [Google Scholar] [CrossRef] [Green Version]
- Campisi, J.; Kapahi, P.; Lithgow, G.J.; Melov, S.; Newman, J.C.; Verdin, E. From discoveries in ageing research to therapeutics for healthy ageing. Nature 2019, 571, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Berkman, L.F. Social epidemiology: Social determinants of health in the United States: Are we losing ground? Annu. Rev. Public Health 2009, 30, 27–41. [Google Scholar] [CrossRef] [Green Version]
- Perissinotto, C.M.; Cenzer, I.S.; Covinsky, K.E. Loneliness in older persons: A predictor of functional decline and death. Arch. Intern. Med. 2012, 172, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Coyle, C.E.; Dugan, E. Social isolation, loneliness and health among older adults. J. Aging Health 2012, 24, 1346–1363. [Google Scholar] [CrossRef]
- Luo, Y.; Waite, L.J. Loneliness and mortality among older adults in China. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 633–645. [Google Scholar] [CrossRef] [Green Version]
- Rowe, J.W.; Fulmer, T.; Fried, L. Preparing for Better Health and Health Care for an Aging Population: A Vital Direction for Health and Health Care. NAM Perspect. 2016, 6, 1643–1644. [Google Scholar] [CrossRef]
- Marijuán, P.C.; Montero-Marín, J.; Navarro, J.; García-Campayo, J.; del Moral, R. The ‘sociotype’ construct: Gauging the structure and dynamics of human sociality. PLoS ONE 2017, 12, e0189568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunbar, R. The Human Story; Faber and Faber: London, UK, 2004. [Google Scholar]
- Marijuán, P.C.; del Moral, R.; Ji, S.; Lacruz, M.G.; Gómez-Quintero, J.D.; Navarro, J. Fundamental, Quantitative Traits of the ‘Sociotype’. BioSystems 2019, 180, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gierveld, J.D.J.; van Tilburg, T. A 6-item scale for overall, emotional, and social loneliness: Confirmatory tests on survey data. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef]
- Cornwell, E.Y.; Waite, L.J. Measuring social isolation among older adults using multiple indicators from the nshap study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, i38–i46. [Google Scholar] [CrossRef] [Green Version]
- Domènech-Abella, J.; Lara, E.; Rubio-Valera, M.; Olaya, B.; Moneta, M.V.; Rico-Uribe, L.A.; Ayuso-Mateos, J.L.; Mundó, J.; Haro, J.M. Loneliness and depression in the elderly: The role of social network. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 381–390. [Google Scholar] [CrossRef]
- Marijuan, P.C.; Navarro, J. The Bonds of Laughter: A Multidisciplinary Inquiry into the Information Processes of Human Laughter. arXiv 2010, arXiv:1010.5602. [Google Scholar]
- Navarro, J.; Rosell, M.F.; Castellanos, A.; del Moral, R.; Lahoz-Beltra, R.; Marijuán, P.C. Plausibility of a Neural Network Classifier-Based Neuroprosthesis for Depression Detection via Laughter Records. Front. Neurosci. 2019, 13, 267. [Google Scholar] [CrossRef] [Green Version]
- Navarro, J.; del Moral, R.; Alonso, M.F.; Loste, P.; Garcia-Campayo, J.; Lahoz-Beltra, R.; Marijuán, P.C. Validation of laughter for diagnosis and evaluation of depression. J. Affect. Disord. 2014, 160, 43–49. [Google Scholar] [CrossRef]
- Martin, R.A. Is laughter the best medicine? Humor, laughter, and physical health. Curr. Dir. Psychol. Sci. 2002, 11, 216–220. [Google Scholar] [CrossRef]
- Uekermann, J.; Channon, S.; Lehmkämper, C.; Abdel-Hamid, M.; Vollmoeller, W.; Daum, I. Executive function, mentalizing and humor in major depression. J. Int. Neuropsychol. Soc. 2008, 14, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Hasan, H.; Hasan, T.F. Laugh yourself into a healthier person: A cross cultural analysis of the effects of varying levels of laughter on health. Int. J. Med. Sci. 2009, 6, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, M.; Hashimoto, R.; Kudo, T.; Okochi, M.; Tagami, S.; Morihara, T.; Sadick, G.; Tanaka, T. Laughter and humor as complementary and alternative medicines for dementia patients. BMC Complementary Altern. Med. 2010, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klinenberg, E. Social Isolation, Loneliness, and Living Alone: Identifying the Risks for Public Health. Am. J. Public Health 2016, 106, 786–787. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]

{kind=link}
| Number | % Population | ||
|---|---|---|---|
| Gender | Women | 646 | 70.6% |
| Men | 269 | 29.4% | |
| Total | 915 | 100.0% | |
| Age segments | From 65 to 75 | 333 | 38.5% |
| From 76 to 85 | 406 | 46.9% | |
| More than 85 | 126 | 14.6% | |
| Total | 865 | 94.5% | |
| Stable relationships | Married/with partner | 372 | 40.7% |
| Single | 102 | 11.1% | |
| Separate/divorced | 32 | 3.5% | |
| Widow/widower | 409 | 44.7% | |
| Total | 915 | 100.0% | |
| Connivence | Alone | 353 | 38.6% |
| Partner | 310 | 33.9% | |
| Partner and offspring | 50 | 5.5% | |
| Other family | 53 | 5.8% | |
| Friends | 2 | 0.2% | |
| Residence | 105 | 11.5% | |
| Other | 42 | 4.6% | |
| Total | 915 | 100.0% | |
| Education | Illiterate | 28 | 3.1% |
| No studies | 372 | 40.7% | |
| Primary | 324 | 35.4% | |
| High school | 99 | 10.8% | |
| University | 79 | 8.6% | |
| Other | 13 | 1.4% | |
| Total | 915 | 100.0% | |
| Income | No income | 35 | 7.3% |
| Minimal pension | 137 | 28.5% | |
| Average pension | 232 | 48.3% | |
| High pension | 61 | 12.7% | |
| Maximal pension | 15 | 3.1% | |
| Total | 480 | 52.5% | |
| SOCQ * | Mn | SD | DI | h2 | w1 | w2 | w3 |
|---|---|---|---|---|---|---|---|
| Family | |||||||
| 1. I speak and relate with my family | 4.35 | 1.13 | 0.48 | 0.79 | 0.87 | 0.07 | 0.15 |
| 2. My family is important to me | 4.73 | 0.85 | 0.40 | 0.66 | 0.80 | 0.03 | 0.11 |
| 3. The family members care about me | 4.40 | 1.18 | 0.46 | 0.78 | 0.87 | 0.08 | 0.11 |
| 4. I have fun and laugh with my family | 3.63 | 1.40 | 0.48 | 0.62 | 0.72 | 0.32 | 0.04 |
| Friends | |||||||
| 5. I speak and relate with my friends | 3.21 | 1.71 | 0.69 | 0.85 | 0.10 | 0.90 | 0.17 |
| 6. I have friends to tell and share problems | 2.89 | 1.85 | 0.65 | 0.82 | 0.05 | 0.88 | 0.21 |
| 7. I consider it important to maintain relationships with friends | 3.78 | 1.62 | 0.63 | 0.76 | 0.11 | 0.85 | 0.16 |
| 8. I have fun and laugh with my friends | 3.02 | 1.64 | 0.69 | 0.77 | 0.23 | 0.83 | 0.18 |
| Acquaintances | |||||||
| 9. I speak and relate comfortably with acquaintances | 3.83 | 1.27 | 0.57 | 0.54 | 0.27 | 0.29 | 0.62 |
| 10. It is difficult for me to make conversation with people I do not know (r) | 3.08 | 1.59 | 0.32 | 0.59 | 0.04 | 0.05 | 0.76 |
| 11. It is easy for me to win support from acquaintances | 2.57 | 1.58 | 0.29 | 0.31 | 0.02 | 0.19 | 0.53 |
| 12. Relations with my acquaintances are forced (r) | 3.76 | 1.27 | 0.41 | 0.60 | 0.14 | 0.12 | 0.75 |
| % of variance (real-data) | 17.73 | 38.59 | 11.12 |
| General SOCQ | Mn | SD | h2 | w1 | w2 | w3 |
|---|---|---|---|---|---|---|
| Family | ||||||
| 1. I speak and relate with my family | 4.39 | 0.97 | 0.81 | −0.16 | 0.94 | 0.02 |
| 2. My family is important to me | 4.74 | 0.76 | 0.83 | −0.12 | 0.91 | 0.10 |
| 3. The family members care about me | 4.49 | 1.00 | 0.64 | −0.04 | 0.81 | −0.01 |
| 4. I have fun and laugh with my family | 3.65 | 1.20 | 0.43 | 0.26 | 0.55 | −0.12 |
| Friends | ||||||
| 5. I speak and relate with my friends | 3.44 | 1.48 | 0.81 | 0.89 | −0.06 | 0.09 |
| 6. I have friends to tell and share problems | 3.45 | 1.65 | 0.83 | 0.92 | −0.07 | 0.06 |
| 7. I consider it important to maintain relationships with friends | 4.14 | 1.39 | 0.81 | 0.90 | −0.01 | 0.01 |
| 8. I have fun and laugh with my friends | 3.59 | 1.41 | 0.68 | 0.82 | 0.09 | −0.11 |
| Acquaintances | ||||||
| 9. I speak and relate comfortably with acquaintances | 3.61 | 1.19 | 0.47 | 0.06 | 0.12 | 0.61 |
| 10. It is difficult for me to make conversation with people I do not know (r) | 3.19 | 1.33 | 0.34 | −0.01 | −0.08 | 0.61 |
| 11. It is easy for me to win support from acquaintances | 2.29 | 1.48 | 0.24 | 0.08 | −0.09 | 0.52 |
| 12. Relations with my acquaintances are forced (r) | 3.53 | 1.05 | 0.42 | −0.02 | 0.05 | 0.63 |
| % of variance (real-data) | 38.70 | 18.80 | 13.90 |
| Range of Values | Mn | SD | SOCG-4 Correlation | N | ||
|---|---|---|---|---|---|---|
| SOCG-4 | 0–4 | 2.98 | 1.12 | 1.00 | 915 | |
| SOCQ | 0–60 | 42.65 | 11.31 | 0.82 ** | 915 | |
| GDS | 0–14 | 2.90 | 3.07 | −0.10 ** | 469 | |
| PFEIFFER | 0–1 | 0.08 | 0.18 | −0.22 ** | 473 | |
| BARTHEL | 5–105 | 95.48 | 19.31 | 0.40 ** | 469 | |
| GHQ12 | 5–36 | 13.71 | 6.20 | −0.36 ** | 420 | |
| UCLA | 20–69 | 35.35 | 10.85 | −0.55 ** | 418 | |
| MMSE | 0.20–1 | 0.65 | 0.17 | −0.020 | 200 | |
| GOLDBERG | 1–2 | 1.72 | 0.39 | 0.05 | 200 | |
| EuroQol5D | Total | 1–2.83 | 1.60 | 0.44 | −0.45 ** | 200 |
| Health | 1–10 | 6.46 | 2.02 | 0.47 | 199 | |
| EPQ-R | E | 0–19 | 9.72 | 4.75 | 0.58 ** | 409 |
| N | 0–23 | 11.08 | 5.23 | −0.14 ** | 408 | |
| p | 0–16 | 4.83 | 2.90 | −0.04 | 408 | |
| Provenance | N | Mn | Sd | Standard Error | |
|---|---|---|---|---|---|
| SOCG-4 | Home dwelling | 100 | 3.00 | 1.19 | 0.12 |
| Residence | 100 | 1.99 | 1.37 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro, J.; Cañete, M.; Olivera, F.J.; Gil-Lacruz, M.; Gil-Lacruz, A.; Marijuán, P.C. The Cost of Loneliness: Assessing the Social Relationships of the Elderly via an Abbreviated Sociotype Questionnaire for inside and outside the Clinic. Int. J. Environ. Res. Public Health 2022, 19, 1253. https://doi.org/10.3390/ijerph19031253
Navarro J, Cañete M, Olivera FJ, Gil-Lacruz M, Gil-Lacruz A, Marijuán PC. The Cost of Loneliness: Assessing the Social Relationships of the Elderly via an Abbreviated Sociotype Questionnaire for inside and outside the Clinic. International Journal of Environmental Research and Public Health. 2022; 19(3):1253. https://doi.org/10.3390/ijerph19031253
Chicago/Turabian StyleNavarro, Jorge, Miguel Cañete, Francisco J. Olivera, Marta Gil-Lacruz, Ana Gil-Lacruz, and Pedro C. Marijuán. 2022. "The Cost of Loneliness: Assessing the Social Relationships of the Elderly via an Abbreviated Sociotype Questionnaire for inside and outside the Clinic" International Journal of Environmental Research and Public Health 19, no. 3: 1253. https://doi.org/10.3390/ijerph19031253
APA StyleNavarro, J., Cañete, M., Olivera, F. J., Gil-Lacruz, M., Gil-Lacruz, A., & Marijuán, P. C. (2022). The Cost of Loneliness: Assessing the Social Relationships of the Elderly via an Abbreviated Sociotype Questionnaire for inside and outside the Clinic. International Journal of Environmental Research and Public Health, 19(3), 1253. https://doi.org/10.3390/ijerph19031253