5. Discussion
Italy was the first European country that was required to manage the COVID-19 emergency, and implemented a large number of social, economic, and healthcare changes [
33]. Nurses’ managers, as a consequence of hospitals’ re-organizations, had to deal with a contingent of nurses who were newly hired or moved into more complex clinical settings, and gap in critical care competencies had to be quickly filled [
34,
35]. Similar circumstances also occurred during the reconversion of general wards into COVID-19 acute care wards. Finally, nursing workloads during the COVID-19 pandemic increased significantly [
36,
37] with long work-shifts and inadequate time to rest [
38]. The high work pressure and uncertainty about the risks of COVID-19 increased nurses’ anxiety, depression, post-traumatic stress disorder [
39], emotional exhaustion [
38], and burnout [
40] rates.
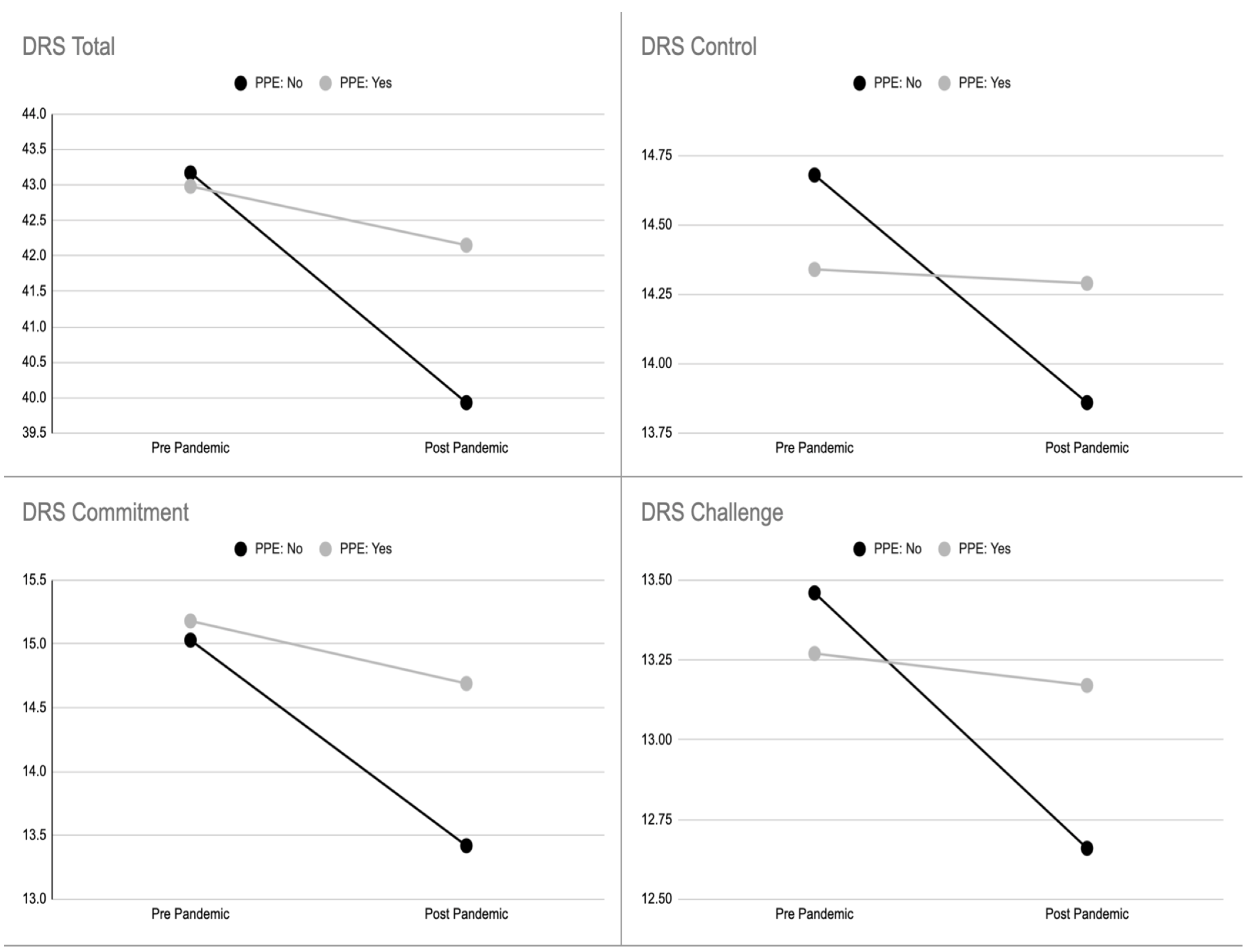
Noting these implications for nurses, we designed a study aiming specifically to assess the hardiness level, its dimensions, and their predictors. As expected, our results showed a significant difference in the hardiness’ level for nurses caring directly for COVID-19 patients (delta 1.0 ± 4.8 M ± SD) compared to those not involved directly with COVID-19 patients (delta 1.9 ± 5.3 M ± SD) (
Table 4).
Despite the amount of literature, to date, few studies have been published about psychological hardiness levels of nurses and other healthcare professionals during the COVID-19 pandemic. In Italy, Vagni et al. studied the levels of hardiness and stress in 140 healthcare workers and 96 emergency workers (ambulance personnel, firefighters, police, and Civil Protection) involved in the COVID-19 pandemic, using DRS-15 [
26]. They did not find statistically significant differences between the mean scores of the commitment subscale (9.81 ± 1.88, versus 10.49 ± 1.97), and the control subscale (10.39 ± 1.96, versus 10.65 ± 2.67), whereas a slight difference emerged between the scores of the challenge subscale of healthcare workers and emergency workers (7.96 ± 2.18 and 7.92 ± 1.90, respectively;
p < 0.01) [
27]. Moreover, there were no significant differences in the mean scores of the DRS-15 subscales between those who directly cared for COVID-19 patients and those who did not (control 10.47 ± 1.98 versus 10.53 ± 2.24; challenge 7.89 ± 2.15 versus 8.01 ± 1.95), with the exception of the commitment subscale (9.87 ± 1.98 versus 10.38 ± 1.86,
p < 0.05) [
27].
Overall, healthcare workers showed moderate to high levels of resilience during the COVID-19 pandemic [
10]. In particular, the resilience levels among healthcare professionals caring directly for COVID-19 patients reported by a literature review performed on 32 studies were found to lie in a range of moderate scores [
9]. Accordingly, another study, performed by Jose et al. (2020), reported that 47.5% of 120 nurses in an Indian emergency department during the COVID-19 pandemic showed moderate to high levels of hardiness [
40], assessed with the subscale “Hardiness” (8 items) of the Connor–Davidson Resilience Scale-25 [
40]. Indeed, in our sample, statistically significant differences in hardiness levels (as a forecaster of the resilience), between nurses caring for COVID-19 patients and those who did not, were also confirmed for the subcategories of commitment, challenge, and control.
Importantly, hardiness is not an intrinsic personal trait, but it can be learned and internalized [
41], as demonstrated by many studies on diverse populations (nurses, other healthcare workers, sport coaches, military personnel, and undergraduate students) [
42].
Regarding the geographical area, working in the North of Italy was associated with lower scores of hardiness compared to the Central Italy; indeed, the earliest phase of the COVID-19 pandemic mainly affected the North of Italy, with tragic consequences for the healthcare system and a higher number of deaths [
43]. Southern Italy was not included in the analysis due to the small number of participants. Lasalvia et al. reported in their study that the psychological impact of the COVID-19 pandemic on healthcare staff working in a highly burdened geographical area of north-east Italy was relevant and, to some extent, greater than that reported in China [
44].
Furthermore, the organizational settings changed during the pandemic and forced the healthcare systems to adapt immediately with new COVID-19 units and COVID-19 ICUs, to deal promptly with the healthcare emergency. Considering the change in clinical setting, it would be expected that the assignment of nurses to COVID-19 units had a great impact on the hardiness level. However, our results did not completely confirm this hypothesis, as shown by the small delta values (
Table 3 and
Table 4). Despite this, the linear relationship between the satisfaction regarding the work setting reallocation showed a significant and positive association with the hardiness levels, with a variance between 10% and 25%, and a particular impact on the measures of commitment and control. A positive perception of the work setting reallocation, here, is strictly linked to a higher hardiness level. Thus, taking into account the perception of nurses, and health professionals in general, may have a positive impact on hardiness.
Regarding the supply of PPE, an interesting difference between the perception of being provided with adequate PPE, or not, was observed. Thus, nurses who claimed to have received adequate PPE according to the government standards of provisions reported a higher level of total hardiness and commitment assessed during the first wave of the COVID-19 pandemic. It is largely reported in the literature that PPE made the difference in individuals’ perception, and that stress and anxiety increased when people were not adequately protected [
45,
46]. Maiorano et al. found that caring for COVID-19 patients, female sex, unforeseen events, and lack of PPE were found to be risk factors for emergency workers’ stress [
25].
A recent study performed on Iranian nurses involved in the care of COVID-19 patients showed moderate levels of negative correlations between hardiness and stress, and a positive correlation with mental health (Pearson correlation coefficient −0.581,
p < 0.05 and 0.474,
p < 0.01, respectively) [
47]. Similar results were found by Park et al. on 187 nurses in a South Korean Hospital during the MERS virus outbreak in 2015 (Pearson’s coefficients −0.401,
p < 0.001 and 0.439,
p < 0.001, respectively) [
24].
The nurses included in our study showed a level of state anxiety that was 90% higher than that of the general population [
48]. The state anxiety level significantly affected all the spheres of hardiness, i.e., both the delta and the assessment after the first pandemic wave. Hardiness and anxiety have a relevant role in the well-being of healthcare providers and ultimately, therefore, in the quality of care provided.
Numerous studies have focused on risk and protective factors to address strategies for developing interventions to reduce and strengthen these psychological issues, respectively [
8,
22]. Resilience resources are factors that are able to counterbalance stressful events or risk factors for stress, and can be found at multiple levels: personality, family, community, and society [
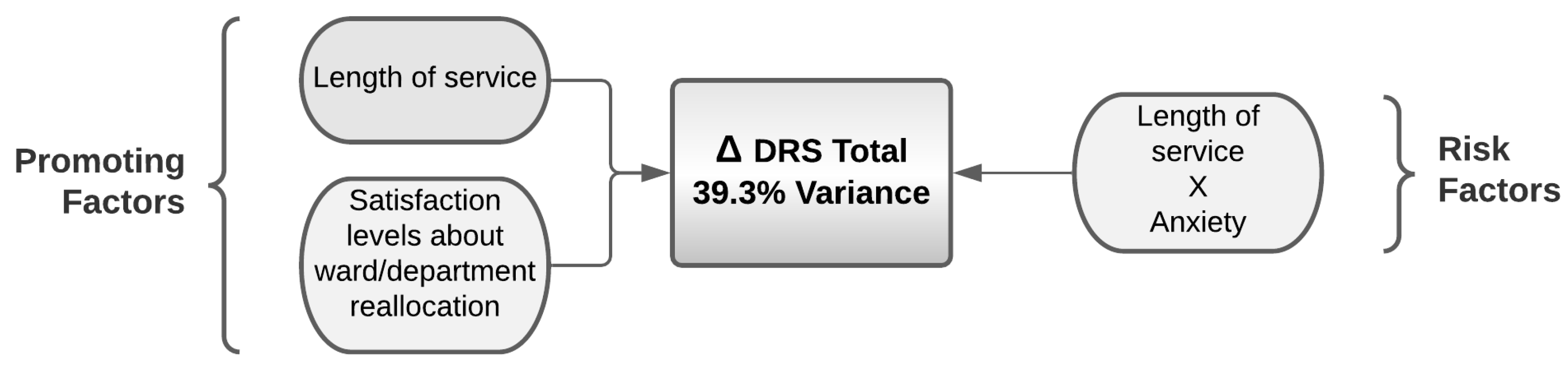
13]. However, the association of anxiety with length of service seems to have a negative impact on hardiness level; thus, anxiety has an indirect negative impact on hardiness level. In particular, as the level of anxiety increased, the dispositional resilience of subjects with a longer length of service was reduced. Our results showed a different level of hardiness before and during the pandemic, which has not changed significantly. In addition, nurses with a longer length of service and no anxiety experienced higher levels of hardiness compared with colleagues with a shorter length of service, whereas nurses with a longer length of service, combined with anxiety, experienced lower hardiness’ levels.
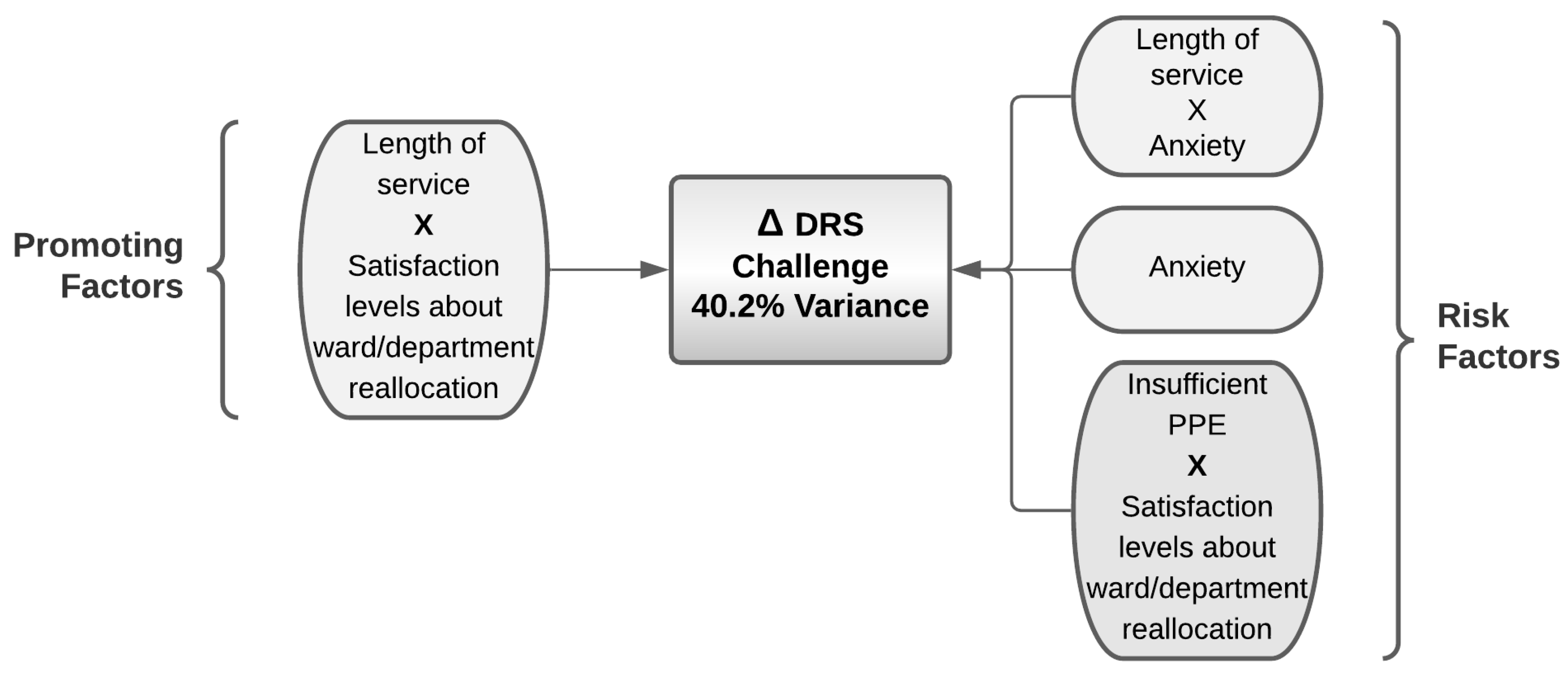
Given the ambiguity of these results, the role of anxiety was hypothesized to have an interaction with the length of service in affecting the perception of hardiness. According to the results mentioned above, length of service is a protective factor for hardiness, and particularly in regard to commitment and challenge. Nonetheless, the interaction of length of service with higher levels of anxiety is a risk factor that negatively affects all spheres of hardiness.
By comparison, the same length of service, associated with higher levels of satisfaction for work setting reallocation, is a protective factor for challenge, as an antecedent of hardiness. Interestingly, in the sphere of commitment, despite the nurses claiming that they did not receive adequate PPE, the positive evaluation of the unit reallocation allowed it to be a protective factor.
Limitations and Suggestions of the Study
Some limitations of the present study must be mentioned. Self-selection bias may have occurred among nurses who decided to complete the questionnaire; the survey was also only disseminated through a critical care nurses’ association (Aniarti).
Moreover, the choice of administering the hardiness scale DRS-15 twice, i.e., asking the participant about their current level of hardiness and their hardiness before the pandemic, may have resulted in recall bias. However, the study was designed during the pandemic and it was not possible to assess this variable previously.
Additionally, the national representativeness of the sample is lacking because it did not include Southern Italy. There were few participants from this geographical area, even though they comprised the population of nurses less affected by COVID-19 during the first wave. Finally, despite the large number of participants, we recognize that a huge number of surveys were available during the same period, affecting the willingness of healthcare professionals to participate in our survey.
6. Conclusions
Our results showed statistically significant differences in hardiness levels between nurses directly caring for COVID-19 patients and those who did not. DRS variance was found to be significant and higher in the first group of nurses.
Based on this study, the role of anxiety levels needs to be closely reconsidered because it may seem to be contradictory. Indeed, when dealing with the predictors of hardiness, anxiety has the role of a hardiness proxy. Promoting factors for hardiness in nurses involved in the care of COVID-19 patients were length of service, positive assessment of department reallocation, and, surprisingly, inadequate PPE when considering a positive assessment of department reallocation. In contrast, the risk factors, which reduced levels of hardiness, were anxiety alone and associated with length of service, a negative assessment of department reallocation, and insufficient PPE when associated with a negative assessment of department reallocation.
Given the pivotal role of hardiness on the quality of care and on the individual health of nurses globally, future research should address this topic in order to establish the actual role of the predictors of hardiness, and to confirm or disagree with our findings. The variation in hardiness levels suggests that this personal trait may be affected by contingencies. Indeed, predictive factors in terms of risk or promotion need to be addressed using a more structured study design.


 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}