
Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review


Abstract
:1. Introduction
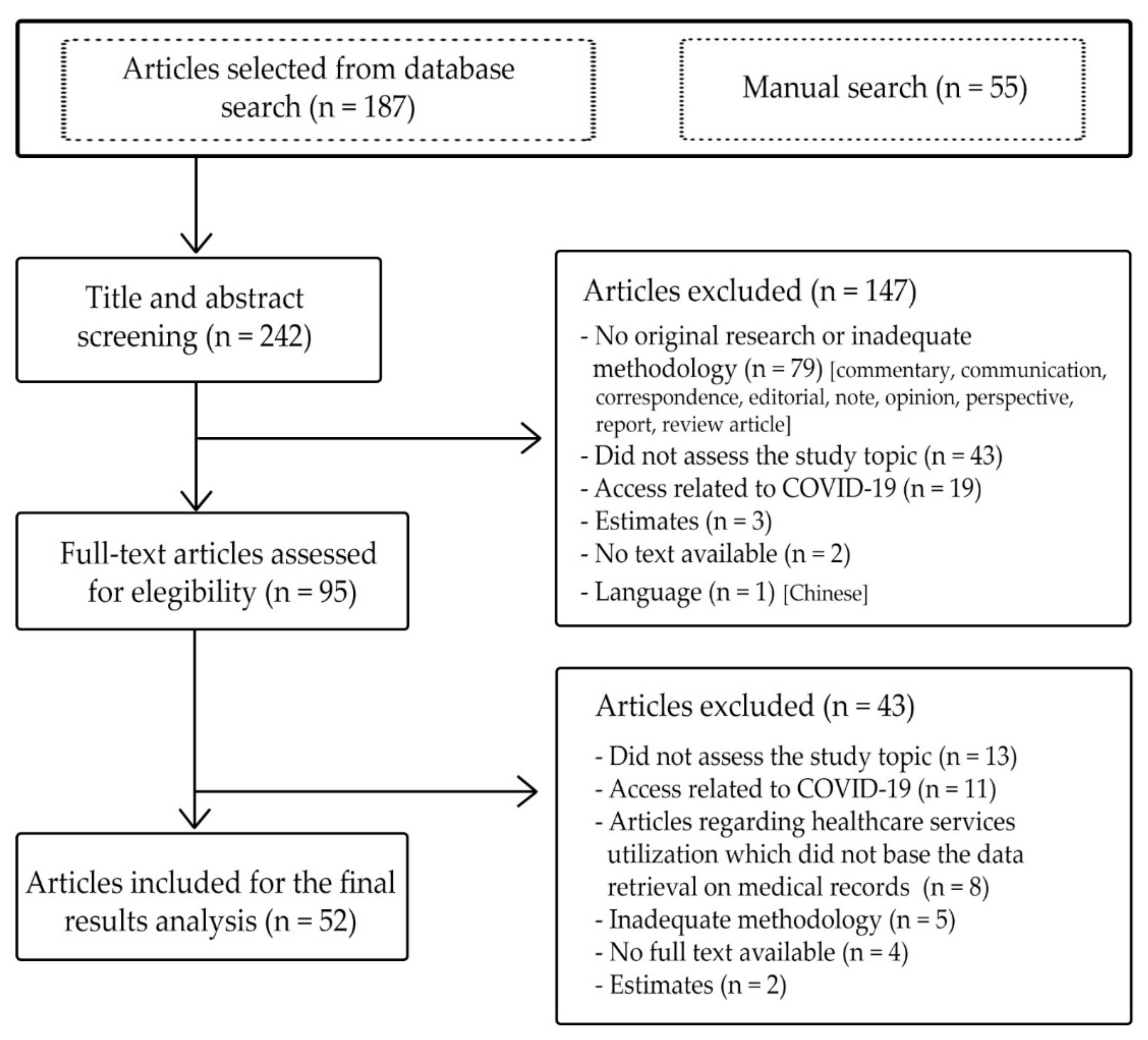
2. Materials and Methods
3. Results
3.1. Changes in the Utilization of Health Services and Influencing Factors
3.2. Potential Access: Barriers Related to Characteristics of the Services and Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
Search Strategy in Medline
- Access to health care services: (((((((((((((((health services accessibility[MeSH Terms]) OR (health services accessibility)) OR (accessing)) OR (accessibility)) OR (access)) OR (utilization)) OR (delivery of health care)) OR (healthcare services)) OR (Health Services Needs and Demand[MeSH Terms])) OR (Healthcare Disparities[MeSH Terms])) OR (Needs Assessment[MeSH Terms])) OR (Health Policy[MeSH Terms])) OR (Equipment and Supplies Utilization[MeSH Terms])) OR (Facilities and Services Utilization[MeSH Terms]))
- AND
- COVID-19: ((((((((coronavirus disease) OR (COVID-19)) OR (coronavirus)) OR (SARS-CoV-2)) OR (Coronavirus Infections[MeSH Terms])) OR (COVID-19[MeSH Terms])) OR (SARS-CoV-2[MeSH Terms])) OR (coronavirus[MeSH Terms]))
- Filters: December 2019–March 2021/March–September 2021.
References
- Organización Mundial de la Salud Cronología de la Respuesta de la OMS a la COVID-19. Available online: https://www.who.int/es/news/item/29-06-2020-covidtimeline (accessed on 6 November 2020).
- Hussein, J. COVID-19: What implications for sexual and reproductive health and rights globally? Sex. Reprod. Health Matters 2020, 28, 1746065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linn, L.; Oliel, S.; Baldwin, A. La COVID-19 afectó el Funcionamiento de los Servicios de Salud para Enfermedades no Transmisibles en las Américas—OPS/OMS|Organización Panamericana de la Salud. Available online: https://www.paho.org/es/noticias/17-6-2020-covid-19-afecto-funcionamiento-servicios-salud-para-enfermedades-no (accessed on 12 October 2020).
- World Health Organization. Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic: Interim Report, 27 August 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Second Round of the National Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic: January–March 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Global Health Cluster COVID-19 Task Team. Essential Health Services: A guidance Note. How to Prioritize and Plan Essential Health Services during COVID-19 Response in Humanitarian Settings; Health Cluster: Geneva, Switzerland, 2020. [Google Scholar]
- Ma, X.; Vervoort, D.; Reddy, C.L.; Park, K.B.; Makasa, E. Emergency and essential surgical healthcare services during COVID-19 in low- and middle-income countries: A perspective. Int. J. Surg. 2020, 79, 43–46. [Google Scholar] [CrossRef]
- Teslya, A.; Pham, T.M.; Godijk, N.G.; Kretzschmar, M.E.; Bootsma, M.C.J.J.; Rozhnova, G. Impact of self-imposed prevention measures and short-term government-imposed social distancing on mitigating and delaying a COVID-19 epidemic: A modelling study. PLoS Med. 2020, 17, e1003499. [Google Scholar] [CrossRef]
- Porthé, V.; Vargas, I.; Sanz-Barbero, B.; Plaza-Espuña, I.; Bosch, L.; Vázquez, M.L. Changes in access to health care for immigrants in Catalonia during the economic crisis: Opinions of health professionals and immigrant users. Health Policy 2016, 120, 1293–1303. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, L.; Ogunwole, S.M.; Cooper, L.A. Historical Insights on Coronavirus Disease 2019 (COVID-19), the 1918 Influenza Pandemic, and Racial Disparities: Illuminating a Path Forward. Ann. Intern. Med. 2020, 173, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, J.; Schaaf, M.; Contractor, S.Q.; Banda, A.; Viana, M.; Kashyntseva, O.; Ruano, A.L. Axes of alienation: Applying an intersectional lens on the social contract during the pandemic response to protect sexual and reproductive rights and health. Int. J. Equity Health 2020, 19, 130. [Google Scholar] [CrossRef]
- Skogberg, N.; Koponen, P.; Lilja, E.; Austero, S.; Prinkey, T.; Castaneda, A.E. Impact of COVID-19 on the Health and Wellbeing of Persons Who Migrated to Finland: The MigCOVID Survey 2020–2021; Finnish Institute of Health and Welfare’s: Helsinki, Finland, 2021. [Google Scholar]
- Frohlich, K.L.; Potvin, L. Transcending the known in public health practice: The inequality paradox: The population approach and vulnerable populations. Am. J. Public Health 2008, 98, 216–221. [Google Scholar] [CrossRef]
- Suhrcke, M.; Stuckler, D.; Suk, J.E.; Desai, M.; Senek, M.; McKee, M.; Tsolova, S.; Basu, S.; Abubakar, I.; Hunter, P.; et al. The impact of economic crises on communicable disease transmission and control: A systematic review of the evidence. PLoS ONE 2011, 6, e20724. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Oikawa, M.; Tamura, T.; Egami, Y.; Fujita, N. Can we apply lessons learned from Ebola experience in West Africa for COVID-19 in lower income countries? Glob. Health Med. 2020, 2, 140–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuzzo, J.B.; Meyer, D.; Snyder, M.; Ravi, S.J.; Lapascu, A.; Souleles, J.; Andrada, C.I.; Bishai, D. What makes health systems resilient against infectious disease outbreaks and natural hazards? Results from a scoping review. BMC Public Health 2019, 19, 1310. [Google Scholar] [CrossRef] [Green Version]
- Phillips, D.E.; Bhutta, Z.A.; Binagwaho, A.; Boerma, T.; Freeman, M.C.; Hirschhorn, L.R.; Panjabi, R. Learning from Exemplars in Global Health: A road map for mitigating indirect effects of COVID-19 on maternal and child health. BMJ Glob. Health 2020, 5, e003430. [Google Scholar] [CrossRef]
- Wilhelm, J.A.; Helleringer, S. Utilization of non-Ebola health care services during Ebola outbreaks: A systematic review and meta-analysis. J. Glob. Health 2019, 9, 010406. [Google Scholar] [CrossRef]
- UNDG. Socio-Economic Impact of Ebola Virus Disease in West African Countries; United Nations Depelopment Group Western and Central Africa: Dakar, Senegal, 2015. [Google Scholar]
- Elston, J.W.T.; Cartwright, C.; Ndumbi, P.; Wright, J. The health impact of the 2014–15 Ebola outbreak. Public Health 2017, 143, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.J.; Huang, N.; Lee, C.H.; Hsu, Y.J.; Hsieh, C.J.; Chou, Y.J. The Impact of the SARS Epidemic on the Utilization of Medical Services: SARS and the Fear of SARS. Am. J. Public Health 2004, 94, 562–564. [Google Scholar] [CrossRef] [PubMed]
- Schull, M.J.; Stukel, T.A.; Vermeulen, M.J.; Zwarenstein, M.; Alter, D.A.; Manuel, D.G.; Guttmann, A.; Laupacis, A.; Schwartz, B. Effect of widespread restrictions on the use of hospital services during an outbreak of severe acute respiratory syndrome. Cmaj 2007, 176, 1827–1832. [Google Scholar] [CrossRef] [Green Version]
- Vazquez, J.; Islam, T.; Gursky, J.; Beller, J.; Correa, D.J. Access to Care Matters: Remote Health Care Needs During COVID-19. Telemed. e-Health 2020, 27, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Ly, J.; Sathananthan, V.; Griffiths, T.; Kanjee, Z.; Kenny, A.; Gordon, N.; Basu, G.; Battistoli, D.; Dorr, L.; Lorenzen, B.; et al. Facility-Based Delivery during the Ebola Virus Disease Epidemic in Rural Liberia: Analysis from a Cross-Sectional, Population-Based Household Survey. PLoS Med. 2016, 13, e1002096. [Google Scholar] [CrossRef]
- UNFPA. Coronavirus (2019-nCoV) Guidance Document 2020; UNFPA Asia-Pacific Regional Office: Bangkok, Thailand, 2020. [Google Scholar]
- Correa, M. Impacto del COVID-19 en la salud sexual y reproductiva. Rev. Int. Salud Matern. Fetal 2020, 5, 5–8. [Google Scholar]
- Masresha, B.G.; Luce, R.; Weldegebriel, G.; Katsande, R.; Gasasira, A.; Mihigo, R. The impact of a prolonged ebola outbreak on measles elimination activities in Guinea, Liberia and Sierra Leone, 2014–2015. Pan Afr. Med. J. 2020, 35, 8. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef]
- Andrews, E.; Berghofer, K.; Long, J.; Prescott, A.; Caboral-Stevens, M. Satisfaction with the use of telehealth during COVID-19: An integrative review. Int. J. Nurs. Stud. Adv. 2020, 2, 100008. [Google Scholar] [CrossRef]
- Parker, R.; Figures, E.; Paddison, C.; Matheson, J.; Blane, D.; Ford, J. Inequalities in General Practice Remote Consultations: A Systematic Review. BJGP Open 2021, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Garfan, S.; Alamoodi, A.H.; Zaidan, B.B.; Al-Zobbi, M.; Hamid, R.A.; Alwan, J.K.; Ahmaro, I.Y.Y.; Khalid, E.T.; Jumaah, F.M.; Albahri, O.S.; et al. Telehealth utilization during the COVID-19 pandemic: A systematic review. Comput. Biol. Med. 2021, 138, 104878. [Google Scholar] [CrossRef]
- Khoshrounejad, F.; Hamednia, M.; Mehrjerd, A.; Pichaghsaz, S.; Jamalirad, H.; Sargolzaei, M.; Hoseini, B.; Aalaei, S. Telehealth-Based Services During the COVID-19 Pandemic: A Systematic Review of Features and Challenges. Front. Public Health 2021, 9, 977. [Google Scholar] [CrossRef]
- Montagnoli, C.; Zanconato, G.; Ruggeri, S.; Cinelli, G.; Tozzi, A.E. Restructuring maternal services during the COVID-19 pandemic: Early results of a scoping review for non-infected women. Midwifery 2021, 94, 102916. [Google Scholar] [CrossRef] [PubMed]
- Olorunsaiye, C.Z.; Yusuf, K.K.; Reinhart, K.; Salihu, H.M. COVID-19 and Child Vaccination: A Systematic Approach to Closing the Immunization Gap. Int. J. Matern. Child Health AIDS 2020, 9, 381–385. [Google Scholar] [CrossRef]
- Dhada, S.; Stewart, D.; Cheema, E.; Hadi, M.A.; Paudyal, V. Cancer services during the COVID-19 pandemic: Systematic review of patient’s and caregiver’s experiences. Cancer Manag. Res. 2021, 13, 5875–5887. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Mendes, R.G.; Alghamdi, S.M.; Miravitlles, M.; Mandal, S.; Hurst, J.R. Reduction in hospitalised COPD exacerbations during COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0255659. [Google Scholar] [CrossRef] [PubMed]
- Gulliford, M.; Figueroa-Munoz, J.; Morgan, M.; Hughes, D.; Gibson, B.; Beech, R.; Hudson, M. What does “access to health care” mean? J. Health Serv. Res. Policy 2002, 7, 186–188. [Google Scholar] [CrossRef]
- Babitsch, B.; Gohl, D.; von Lengerke, T. Re-revisiting Andersen’s Behavioral Model of Health Services Use: A systematic review of studies from 1998–2011. GMS Psycho-Soc.-Med. 2012, 9, 1–15. [Google Scholar] [CrossRef]
- Aday, L.A.; Andersen, R. A framework for the study of access to medical care. Health Serv. Res. 1974, 9, 208–220. [Google Scholar]
- Andersen, R.M.; Davidson, P.L. Improving Access to Care in America: Individual and Contextual Indicators. In Changing the US Health Care System: Key Issues in Health Services Policy and Management; Andersen, R., Rice, T.S., Kominski, J., Eds.; Jossey-Bass: San Francisco, CA, USA, 2001; pp. 3–31. ISBN 978-0787954048. [Google Scholar]
- Donabedian, A. Aspects of Medical Care Administration: Specifying Requirements for Health Care; Harvard University Press: Cambridge, UK, 1973. [Google Scholar]
- Pechansky, R.; Thomas, W. The concept of access. Definition and relationship to costumer satisfaction. Med. Care 1981, XIX, 127–140. [Google Scholar]
- Frenk, J. El concepto y la medición de la accesibilidad. Salud Pública Mex 1985, 27, 438–453. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abebe, W.; Worku, A.; Moges, T.; Tekle, N.; Amogne, W.; Haile, T.; Mekonen, D.; Habtamu, A.; Deressa, W. Trends of follow-up clinic visits and admissions three-months before and during COVID-19 pandemic at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia: An interrupted time series analysis. BMC Health Serv. Res. 2021, 21, 731. [Google Scholar] [CrossRef]
- Howarth, A.; Munro, M.; Theodorou, A.; Mills, P.R. Trends in healthcare utilisation during COVID-19: A longitudinal study from the UK. BMJ Open 2021, 11, e048151. [Google Scholar] [CrossRef] [PubMed]
- Siedner, M.J.; Kraemer, J.D.; Meyer, M.J.; Harling, G.; Mngomezulu, T.; Gabela, P.; Dlamini, S.; Gareta, D.; Majozi, N.; Ngwenya, N.; et al. Access to primary healthcare during lockdown measures for COVID-19 in rural South Africa: An interrupted time series analysis. BMJ Open 2020, 10, e043763. [Google Scholar] [CrossRef]
- Whaley, C.M.; Pera, M.F.; Cantor, J.; Chang, J.; Velasco, J.; Hagg, H.K.; Sood, N.; Bravata, D.M. Changes in Health Services Use Among Commercially Insured US Populations During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2024984. [Google Scholar] [CrossRef]
- Zhang, Y.N.; Chen, Y.; Wang, Y.; Li, F.; Pender, M.; Wang, N.; Yan, F.; Ying, X.H.; Tang, S.L.; Fu, C.W. Reduction in healthcare services during the COVID-19 pandemic in China. BMJ Glob. Health 2020, 5, e003421. [Google Scholar] [CrossRef]
- Ojetti, V.; Covino, M.; Brigida, M.; Petruzziello, C.; Saviano, A.; Migneco, A.; Candelli, M.; Franceschi, F. Non-COVID diseases during the pandemic: Where have all other emergencies gone? Medicina 2020, 56, 512. [Google Scholar] [CrossRef] [PubMed]
- Mahmassani, D.; Tamim, H.; Makki, M.; Hitti, E. The impact of COVID-19 lockdown measures on ED visits in Lebanon. Am. J. Emerg. Med. 2021, 46, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Cano-Valderrama, O.; Morales, X.; Ferrigni, C.J.; Martín-Antona, E.; Turrado, V.; García, A.; Cuñarro-López, Y.; Zarain-Obrador, L.; Duran-Poveda, M.; Balibrea, J.M.; et al. Acute Care Surgery during the COVID-19 pandemic in Spain: Changes in volume, causes and complications. A multicentre retrospective cohort study. Int. J. Surg. 2020, 80, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Sokolski, M.; Gajewski, P.; Zymliński, R.; Biegus, J.; Berg, J.M.T.; Bor, W.; Braunschweig, F.; Caldeira, D.; Cuculi, F.; D’Elia, E.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on Acute Admissions at the Emergency and Cardiology Departments Across Europe. Am. J. Med. 2021, 134, 482–489. [Google Scholar] [CrossRef]
- Tsioufis, K.; Chrysohoou, C.; Kariori, M.; Leontsinis, I.; Dalakouras, I.; Papanikolaou, A.; Charalambus, G.; Sambatakou, H.; Siasos, G.; Panagiotakos, D.; et al. The mystery of “missing” visits in an emergency cardiology department, in the era of COVID-19.; a time-series analysis in a tertiary Greek General Hospital. Clin. Res. Cardiol. 2020, 109, 1483–1489. [Google Scholar] [CrossRef]
- Choi, A.; Bae, W.; Kim, K.; Kim, S. Impact of COVID-19 on the visit of pediatric patients with injuries to the emergency department in korea. Children 2021, 8, 568. [Google Scholar] [CrossRef] [PubMed]
- Dopfer, C.; Wetzke, M.; Zychlinsky Scharff, A.; Mueller, F.; Dressler, F.; Baumann, U.; Sasse, M.; Hansen, G.; Jablonka, A.; Happle, C. COVID-19 related reduction in pediatric emergency healthcare utilization—A concerning trend. BMC Pediatr. 2020, 20, 427. [Google Scholar] [CrossRef]
- Finkelstein, Y.; Maguire, B.; Zemek, R.; Osmanlliu, E.; Kam, A.J.; Dixon, A.; Desai, N.; Sawyer, S.; Emsley, J.; Lynch, T.; et al. Effect of the COVID-19 Pandemic on Patient Volumes, Acuity, and Outcomes in Pediatric Emergency Departments: A Nationwide Study. Pediatr. Emerg. Care 2021, 37, 427–434. [Google Scholar] [CrossRef]
- Goldman, R.D.; Grafstein, E.; Barclay, N.; Irvine, M.A.; Portales-Casamar, E. Paediatric patients seen in 18 emergency departments during the COVID-19 pandemic. Emerg. Med. J. 2020, 37, 773–777. [Google Scholar] [CrossRef]
- Percul, C.; Cruz, M.; Meza, A.C.; González, G.; Lerendegui, L.; Malzone, M.C.; Liberto, D.; Lobos, P.; Imach, B.E.; Moldes, J.M.; et al. Impact of the COVID-19 pandemic on the pediatric population with acute appendicitis: Experience at a general, tertiary care hospital. Arch. Argent. Pediatr. 2021, 119, 224–229. [Google Scholar] [CrossRef]
- Yamamoto, H.; Morikawa, Y.; Hagiwara, Y.; Hataya, H. Pediatric emergency healthcare utilization during the COVID-19 pandemic in Tokyo. Pediatr. Int. 2021. [Google Scholar] [CrossRef]
- Ball, S.; Banerjee, A.; Berry, C.; Boyle, J.R.; Bray, B.; Bradlow, W.; Chaudhry, A.; Crawley, R.; Danesh, J.; Denniston, A.; et al. Monitoring indirect impact of COVID-19 pandemic on services for cardiovascular diseases in the UK. Heart 2020, 106, 1890–1897. [Google Scholar] [CrossRef] [PubMed]
- Kute, V.B.; Gupta, A.; Patel, H.V.; Engineer, D.P.; Banerjee, S.; Rizvi, S.J.; Mishra, V.V.; Patel, A.H.; Navadiya, V.V. The impact of COVID-19 pandemic on nephrology and transplant services and clinical training in India. Exp. Clin. Transplant. 2021, 19, 651–658. [Google Scholar] [CrossRef]
- Morris, E.J.A.; Goldacre, R.; Spata, E.; Mafham, M.; Finan, P.J.; Shelton, J.; Richards, M.; Spencer, K.; Emberson, J.; Hollings, S.; et al. Impact of the COVID-19 pandemic on the detection and management of colorectal cancer in England: A population-based study. Lancet Gastroenterol. Hepatol. 2021, 6, 199–208. [Google Scholar] [CrossRef]
- Pareek, A.; Patel, A.A.; Harshavardhan, A.; Kuttikat, P.G.; Pendse, S.; Dhyani, A.; Sharma, S.; Agarwal, N.; Maji, D.; Reddy, R.G.; et al. Impact of nationwide lockdown on cancer care during COVID-19 pandemic: A retrospective analysis from western India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102131. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.; Huang, J.; Pi, M.; Chen, X.; Li, X.; Ding, Y.; Zhang, H.; Xiao, D.; Huang, G.; Ming, T.; et al. Impact of early Coronavirus Disease 2019 pandemic on pediatric cardiac surgery in China. J. Thorac. Cardiovasc. Surg. 2021, 161, 1605–1614.e4. [Google Scholar] [CrossRef]
- Ambrosetti, J.; Macheret, L.; Folliet, A.; Wullschleger, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Prada, P.; Kaiser, S.; Bondolfi, G.; et al. Impact of the COVID-19 pandemic on psychiatric admissions to a large swiss emergency department: An observational study. Int. J. Environ. Res. Public Health 2021, 18, 1174. [Google Scholar] [CrossRef]
- Aragona, M.; Barbato, A.; Cavani, A.; Costanzo, G.; Mirisola, C. Negative impacts of COVID-19 lockdown on mental health service access and follow-up adherence for immigrants and individuals in socio-economic difficulties. Public Health 2020, 186, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Jesenšek Papež, B.; Šošić, L.; Bojnec, V. The consequences of COVID-19 outbreak on outpatient rehabilitation services: A single-center experience in Slovenia. Eur. J. Phys. Rehabil. Med. 2021, 57, 451–457. [Google Scholar] [CrossRef]
- Farrugia, Y.; Spiteri Meilak, B.P.; Grech, N.; Asciak, R.; Camilleri, L.; Montefort, S.; Zammit, C. The Impact of COVID-19 on Hospitalised COPD Exacerbations in Malta. Pulm. Med. 2021, 2021, 5533123. [Google Scholar] [CrossRef]
- Burt, J.F.; Ouma, J.; Lubyayi, L.; Amone, A.; Aol, L.; Sekikubo, M.; Nakimuli, A.; Nakabembe, E.; Mboizi, R.; Musoke, P.; et al. Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda. BMJ Glob. Health 2021, 6, e006102. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.; McKerrow, N.H. Child health services during a COVID-19 outbreak in KwaZulu-Natal Province, South Africa. S. Afr. Med. J. 2020, 111, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Justman, N.; Shahak, G.; Gutzeit, O.; Ben Zvi, D.; Ginsberg, Y.; Solt, I.; Vitner, D.; Beloosesky, R.; Weiner, Z.; Zipori, Y. Lockdown with a Price: The impact of the COVID-19 Pandemic on Prenatal Care and Perinatal Outcomes in a Tertiary Care Center. Isr. Med. Assoc. J. 2020, 22, 533–537. [Google Scholar] [PubMed]
- KC, A.; Gurung, R.; Kinney, M.V.; Sunny, A.K.; Moinuddin, M.; Basnet, O.; Paudel, P.; Bhattarai, P.; Subedi, K.; Shrestha, M.P.; et al. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. Lancet Glob. Health 2020, 8, e1273–e1281. [Google Scholar] [CrossRef]
- Marques-Fernandez, L.; Sharma, S.; Mannu, U.; Chong, H.P. Impact of COVID-19 on attendances for a 1stepisode of reduced fetal movements: A retrospective observational study. PLoS ONE 2021, 16, e0253796. [Google Scholar] [CrossRef]
- Shakespeare, C.; Dube, H.; Moyo, S.; Ngwenya, S. Resilience and vulnerability of maternity services in Zimbabwe: A comparative analysis of the effect of COVID-19 and lockdown control measures on maternal and perinatal outcomes, a single-centre cross-sectional study at Mpilo Central Hospital. BMC Pregnancy Childbirth 2021, 21, 416. [Google Scholar] [CrossRef]
- Spurlin, E.E.; Han, E.S.; Silver, E.R.; May, B.L.; Tatonetti, N.P.; Ingram, M.A.; Jin, Z.; Hur, C.; Advincula, A.P.; Hur, H.C. Where Have All the Emergencies Gone? The Impact of the COVID-19 Pandemic on Obstetric and Gynecologic Procedures and Consults at a New York City Hospital. J. Minim. Invasive Gynecol. 2020, 28, 1411–1419.e1. [Google Scholar] [CrossRef]
- Chiba, H.; Lewis, M.; Benjamin, E.R.; Jakob, D.A.; Liasidis, P.; Wong, M.D.; Navarrete, S.; Carreon, R.; Demetriades, D. “Safer at home”: The effect of the COVID-19 lockdown on epidemiology, resource utilization, and outcomes at a large urban trauma center. J. Trauma Acute Care Surg. 2021, 90, 708–713. [Google Scholar] [CrossRef]
- Horan, J.; Duddy, J.C.; Gilmartin, B.; Amoo, M.; Nolan, D.; Corr, P.; Husien, M.B.; Bolger, C. The impact of COVID-19 on trauma referrals to a National Neurosurgical Centre. Ir. J. Med. Sci. 2021, 190, 1281–1293. [Google Scholar] [CrossRef]
- Alexander, G.C.; Tajanlangit, M.; Heyward, J.; Mansour, O.; Qato, D.M.; Stafford, R.S. Use and Content of Primary Care Office-Based vs Telemedicine Care Visits During the COVID-19 Pandemic in the US. JAMA Netw. Open 2020, 3, e2021476. [Google Scholar] [CrossRef]
- Sato, K.; Mano, T.; Niimi, Y.; Iwata, A.; Toda, T.; Iwatsubo, T. The impact of COVID-19 pandemic on the utilization of ambulatory care for patients with chronic neurological diseases in Japan: Evaluation of an administrative claims database. Biosci. Trends 2021, 15, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Bergman, A.; Chen, A.T.; Ellis, D.; David, G.; Friedman, A.B.; Bond, A.M.; Bailey, J.M.; Brooks, R.; Smith-McLallen, A. Disruptions in preventive care: Mammograms during the COVID-19 pandemic. Health Serv. Res. 2021, 56, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, A.B.; Yildiz, Y.; Çiki, K.; Akar, H.T.; Erdal, I.; Dursun, A.; Tokatli, A.; Sivri, H.S. Invisible burden of COVID-19: Enzyme replacement therapy disruptions. J. Pediatr. Endocrinol. Metab. 2021, 34, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, E.; McDonnell, T.; Conlon, C.; Barrett, M.; Cummins, F.; Hensey, C.; McAuliffe, E. Parental Hesitancy and Concerns around Accessing Paediatric Unscheduled Healthcare during COVID-19: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 9264. [Google Scholar] [CrossRef]
- Benjamen, J.; Girard, V.; Jamani, S.; Magwood, O.; Holland, T.; Sharfuddin, N.; Pottie, K. Access to refugee and migrant mental health care services during the first six months of the COVID-19 pandemic: A canadian refugee clinician survey. Int. J. Environ. Res. Public Health 2021, 18, 5266. [Google Scholar] [CrossRef]
- Halley, M.C.; Stanley, T.; Maturi, J.; Goldenberg, A.J.; Bernstein, J.A.; Wheeler, M.T.; Tabor, H.K. “It seems like COVID-19 now is the only disease present on Earth”: Living with a rare or undiagnosed disease during the COVID-19 pandemic. Genet. Med. 2021, 23, 837–844. [Google Scholar] [CrossRef]
- Adelekan, B.; Goldson, E.; Abubakar, Z.; Mueller, U.; Alayande, A.; Ojogun, T.; Ntoimo, L.; Williams, B.; Muhammed, I.; Okonofua, F. Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: A cross-sectional study. Reprod. Health 2021, 18, 166. [Google Scholar] [CrossRef]
- Karavadra, B.; Stockl, A.; Prosser-Snelling, E.; Simpson, P.; Morris, E. Women’s perceptions of COVID-19 and their healthcare experiences: A qualitative thematic analysis of a national survey of pregnant women in the United Kingdom. BMC Pregnancy Childbirth 2020, 20, 600. [Google Scholar] [CrossRef]
- Khan, M.S.; Rego, S.; Rajal, J.B.; Bond, V.; Fatima, R.K.; Isani, A.K.; Sutherland, J.; Kranzer, K. Mitigating the impact of COVID-19 on tuberculosis and HIV services: A cross-sectional survey of 669 health professionals in 64 low and middle-income countries. PLoS ONE 2021, 16, e0244936. [Google Scholar] [CrossRef]
- García-Rojo, E.; Manfredi, C.; Santos-Pérez-de-la-Blanca, R.; Tejido-Sánchez, A.; García-Gómez, B.; Aliaga-Benítez, M.; Romero-Otero, J.; Rodriguez-Antolín, A. Impact of COVID-19 outbreak on urology surgical waiting lists and waiting lists prioritization strategies in the Post-COVID-19 era. Actas Urol. Esp. 2021, 45, 207–214. [Google Scholar] [CrossRef]
- Zambrano-Barragán, P.; Ramírez Hernández, S.; Freier, L.F.; Luzes, M.; Sobczyk, R.; Rodríguez, A.; Beach, C. The impact of COVID-19 on Venezuelan migrants’ access to health: A qualitative study in Colombian and Peruvian cities. J. Migr. Health 2021, 3, 100029. [Google Scholar] [CrossRef] [PubMed]
- Danhieux, K.; Buffel, V.; Pairon, A.; Benkheil, A.; Remmen, R.; Wouters, E.; van Olmen, J. The impact of COVID-19 on chronic care according to providers: A qualitative study among primary care practices in Belgium. BMC Fam. Pract. 2020, 21, 255. [Google Scholar] [CrossRef] [PubMed]
- Gichuna, S.; Hassan, R.; Sanders, T.; Campbell, R.; Mutonyi, M.; Mwangi, P. Access to Healthcare in a time of COVID-19: Sex Workers in Crisis in Nairobi, Kenya. Glob. Public Health 2020, 15, 1430–1442. [Google Scholar] [CrossRef] [PubMed]
- Hailemariam, S.; Agegnehu, W.; Derese, M. Exploring COVID-19 Related Factors Influencing Antenatal Care Services Uptake: A Qualitative Study among Women in a Rural Community in Southwest Ethiopia. J. Prim. Care Community Health 2021, 12, 2150132721996892. [Google Scholar] [CrossRef]
- Mizrak Sahin, B.; Kabakci, E.N. The experiences of pregnant women during the COVID-19 pandemic in Turkey: A qualitative study. Women Birth 2020, 34, 162–169. [Google Scholar] [CrossRef]
- Dos Santos, F.L.; Souza, L.L.L.; Bruce, A.T.I.; De Almeida Crispim, J.; Arroyo, L.H.; Ramos, A.C.V.; Berra, T.Z.; Alves, Y.M.; Scholze, A.R.; Da Costa, F.B.P.; et al. Patients’ perceptions regarding multidrugresistant tuberculosis and barriers to seeking care in a priority city in Brazil during COVID-19 pandemic: A qualitative study. PLoS ONE 2021, 16, e0249822. [Google Scholar] [CrossRef]
- Ahmed, S.A.K.S.; Ajisola, M.; Azeem, K.; Bakibinga, P.; Chen, Y.-F.; Choudhury, N.N.; Fayehun, O.; Griffiths, F.; Harris, B.; Kibe, P.; et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: Results of pre-COVID and COVID-19 lockdown stakeholder engagements. BMJ Glob. Health 2020, 5, e003042. [Google Scholar] [CrossRef]
- das Neves Martins Pires, P.H.; Macaringue, C.; Abdirazak, A.; Mucufo, J.R.; Mupueleque, M.A.; Zakus, D.; Siemens, R.; Belo, C.F. COVID-19 pandemic impact on maternal and child health services access in Nampula, Mozambique: A mixed methods research. BMC Health Serv. Res. 2021, 21, 860. [Google Scholar] [CrossRef]
- UNFPA. COVID-19: Un Enfoque de Género. Proteger la Salud y los Derechos Sexuales y Reproductivos y Promover la Igualdad de Género; United Nations Population Fund: New York, NY, USA, 2020. [Google Scholar]
- World Health Organization. COVID-19 Pandemic Leads to Major Backsliding on Childhood Vaccinations, New WHO, UNICEF Data Shows. Available online: https://www.who.int/news/item/15-07-2021-covid-19-pandemic-leads-to-major-backsliding-on-childhood-vaccinations-new-who-unicef-data-shows (accessed on 18 July 2021).
- Abdelbadee, A.Y.; Abbas, A.M. Impact of COVID-19 on reproductive health and maternity services in low resource countries. Eur. J. Contracept. Reprod. Health Care 2020, 25, 402–404. [Google Scholar] [CrossRef] [PubMed]
- Kimani, R.W.; Maina, R.; Shumba, C.; Shaibu, S. Maternal and newborn care during the COVID-19 pandemic in Kenya: Re-contextualising the community midwifery model. Hum. Resour. Health 2020, 18, 75. [Google Scholar] [CrossRef]
- Chattu, V.K.; Yaya, S. Emerging infectious diseases and outbreaks: Implications for women’s reproductive health and rights in resource-poor settings. Reprod. Health 2020, 17, 43. [Google Scholar] [CrossRef] [Green Version]
- Murewanhema, G.; Makurumidze, R. Essential health services delivery in Zimbabwe during the COVID-19 pandemic: Perspectives and recommendations. Pan Afr. Med. J. 2020, 35, 143. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, S.; Diamond-Smith, N.; Srinivasan, K.; Dalvie, S. Preparing for an Increased Need for Abortion Access in India during and after COVID-19: Challenges and Strategies. Stud. Fam. Plann. 2020, 51, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, A.; Kantorová, V.; Ueffing, P. The impact of the COVID-19 crisis on meeting needs for family planning: A global scenario by contraceptive methods used. Gates Open Res. 2020, 4, 102. [Google Scholar] [CrossRef]
- Kumar, N. COVID 19 era: A beginning of upsurge in unwanted pregnancies, unmet need for contraception and other women related issues. Eur. J. Contracept. Reprod. Health Care 2020, 25, 323–325. [Google Scholar] [CrossRef]
- Tang, K.; Gaoshan, J.; Ahonsi, B. Sexual and reproductive health (SRH): A key issue in the emergency response to the coronavirus disease (COVID-19) outbreak. Reprod. Health 2020, 17, 59. [Google Scholar] [CrossRef] [PubMed]
- Nandagiri, R.; Coast, E.; Strong, J. COVID-19 and abortion: Making structural violence visible. Int. Perspect. Sex. Reprod. Health 2020, 46, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Onwuzurike, C.; Meadows, A.R.; Nour, N.M. Examining Inequities Associated With Changes in Obstetric and Gynecologic Care Delivery During the Coronavirus Disease 2019 (COVID-19) Pandemic. Obstet. Gynecol. 2020, 136, 37–41. [Google Scholar] [CrossRef]
- Suh-Burgmann, E.J.; Alavi, M.; Schmittdiel, J. Endometrial Cancer Detection During the Coronavirus Disease 2019 (COVID-19) Pandemic. Obstet. Gynecol. 2020, 136, 842–843. [Google Scholar] [CrossRef]
- Sharma, K.A.; Zangmo, R.; Kumari, A.; Roy, K.K.; Bharti, J. Family planning and abortion services in COVID 19 pandemic. Taiwan. J. Obstet. Gynecol. 2020, 59, 808–811. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, P.; Singh, K.; Shekhar, S.; Agrawal, N.; Misra, S. The effect of the COVID-19 pandemic on maternal health due to delay in seeking health care: Experience from a tertiary center. Int. J. Gynecol. Obstet. 2021, 152, 231–235. [Google Scholar] [CrossRef]
- Tirado, V.; Chu, J.; Hanson, C.; Ekström, A.M.; Kågesten, A. Barriers and facilitators for the sexual and reproductive health and rights of young people in refugee contexts globally: A scoping review. PLoS ONE 2020, 15, e0236316. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Shinan-Altman, S.; Levkovich, I.; Tavori, G. Healthcare utilization among breast cancer patients during the COVID-19 outbreak. Palliat. Support. Care 2020, 18, 385–391. [Google Scholar] [CrossRef]
- Marzo-Castillejo, M.; Guiriguet Capdevila, C.; Coma Redon, E. The impact of COVID-19 on cancer diagnosis delay: Possible consequences. Aten. Primaria 2021, 53, 102142. [Google Scholar] [CrossRef]
- Arolas, H.P.i.; Vidal-Alaball, J.; Gil, J.; López, F.; Nicodemo, C.; Saez, M. Missing diagnoses during the COVID-19 pandemic: A year in review. Int. J. Environ. Res. Public Health 2021, 18, 5335. [Google Scholar] [CrossRef]
- Chau, S.W.H.; Wong, O.W.H.; Ramakrishnan, R.; Chan, S.S.M.; Wong, E.K.Y.; Li, P.Y.T.; Raymont, V.; Elliot, K.; Rathod, S.; Delanerolle, G.; et al. History for some or lesson for all? A systematic review and meta-analysis on the immediate and long-term mental health impact of the 2002–2003 Severe Acute Respiratory Syndrome (SARS) outbreak. BMC Public Health 2021, 21, 670. [Google Scholar] [CrossRef]
- Weinberger, M.; Hayes, B.; White, J.; Skibiak, J. Doing things differently: What it would take to ensure continued access to contraception during COVID-19. Glob. Health Sci. Pract. 2020, 8, 169–175. [Google Scholar] [CrossRef] [PubMed]
- McLean, M.; Abuelaish, I. Access to reproductive health care services in countries of conflict: The double impact of conflict and COVID-19. Med. Confl. Surviv. 2020, 36, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Abdela, S.G.; Van Griensven, J.; Seife, F.; Enbiale, W. Neglecting the effect of COVID-19 on neglected tropical diseases: The Ethiopian perspective. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 730–732. [Google Scholar] [CrossRef] [PubMed]
- UNFPA; Avenir Health; John Hopkins University; Victoria University. Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-Based Violence, Female Genital Mutilation and Child Marriage; United Nations Population Fund: New York, NY, USA, 2020. [Google Scholar]
- Organización Mundial de la Salud Los Servicios de Salud Mental se Están Viendo Perturbados por la COVID-19 en la Mayoría de los Países, Según un Estudio de la OMS. Available online: https://www.who.int/es/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey (accessed on 12 July 2021).
- Karos, K.; McParland, J.L.; Bunzli, S.; Devan, H.; Hirsh, A.; Kapos, F.P.; Keogh, E.; Moore, D.; Tracy, L.M.; Ashton-James, C.E. The social threats of COVID-19 for people with chronic pain. Pain 2020, 161, 2229–2235. [Google Scholar] [CrossRef]
- Diamond, L.C.; Jacobs, E.A.; Karliner, L. Providing equitable care to patients with limited dominant language proficiency amid the COVID-19 pandemic. Patient Educ. Couns. 2020, 103, 1451–1452. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, J.A.; Rosenberg, M.A.; Zevallos, A.; Brown, J.R.; Mileski, M. The Impact of COVID-19 on Telemedicine Utilization Across Multiple Service Lines in the United States. Healthcare 2020, 8, 380. [Google Scholar] [CrossRef]
- Fryer, K.; Delgado, A.; Foti, T.; Reid, C.N.; Marshall, J. Implementation of Obstetric Telehealth During COVID-19 and Beyond. Matern. Child Health J. 2020, 24, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Contreras, C.M.; Metzger, G.A.; Beane, J.D.; Dedhia, P.H.; Ejaz, A.; Pawlik, T.M. Telemedicine: Patient-Provider Clinical Engagement During the COVID-19 Pandemic and Beyond. J. Gastrointest. Surg. 2020, 24, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, A.; Yu, M.; Drangsholt, S.; Ng, E.; Culligan, P.J.; Schlegel, P.N.; Hu, J.C. Patient satisfaction with telemedicine during the COVID-19 pandemic: Retrospective cohort study. J. Med. Internet Res. 2020, 22, e20786. [Google Scholar] [CrossRef]
- Aiken, A.R.A.; Starling, J.E.; Gomperts, R.; Tec, M.; Scott, J.G.; Aiken, C.E. Demand for Self-Managed Online Telemedicine Abortion in the United States During the Coronavirus Disease 2019 (COVID-19) Pandemic. Obstet. Gynecol. 2020, 136, 835–837. [Google Scholar] [CrossRef]
- Eberly, L.A.; Kallan, M.J.; Julien, H.M.; Haynes, N.; Khatana, S.A.M.; Nathan, A.S.; Snider, C.; Chokshi, N.P.; Eneanya, N.D.; Takvorian, S.U.; et al. Patient Characteristics Associated With Telemedicine Access for Primary and Specialty Ambulatory Care During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2031640. [Google Scholar] [CrossRef]
- Mann, D.M.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. J. Am. Med. Inform. Assoc. 2020, 27, 1132–1135. [Google Scholar] [CrossRef]
- Limaye, M.A.; Lantigua-Martinez, M.; Trostle, M.E.; Penfield, C.A.; Conroy, E.M.; Roman, A.S.; Mehta-Lee, S.S. Differential Uptake of Telehealth for Prenatal Care in a Large New York City Academic Obstetrical Practice during the COVID-19 Pandemic. Am. J. Perinatol. 2020, 1, 18–20. [Google Scholar] [CrossRef]
- Futterman, I.; Rosenfeld, E.; Toaff, M.; Boucher, T.; Golden-Espinal, S.; Evans, K.; Clare, C.A. Addressing Disparities in Prenatal Care via Telehealth during COVID-19: Prenatal Satisfaction Survey in East Harlem. Am. J. Perinatol. 2021, 38, 88–92. [Google Scholar] [CrossRef]
- Schweiberger, K.; Hoberman, A.; Iagnemma, J.; Schoemer, P.; Squire, J.; Taormina, J.; Wolfson, D.; Ray, K.N. Practice-level variation in telemedicine use in a pediatric primary care network during the COVID-19 pandemic: Retrospective analysis and survey study. J. Med. Internet Res. 2020, 22, e24345. [Google Scholar] [CrossRef]
- Riley, T.; Sully, E.; Ahmed, Z.; Biddlecom, A. Estimates of the Potential Impact of the COVID-19 Pandemic on Sexual and Reproductive Health in Low- and Middle-Income Countries. Int. Perspect. Sex. Reprod. Health 2020, 46, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, 10–11. [Google Scholar] [CrossRef]
- Shayganfard, M.; Mahdavi, F.; Haghighi, M.; Bahmani, D.S.; Brand, S. Health anxiety predicts postponing or cancelling routine medical health care appointments among women in perinatal stage during the COVID-19 lockdown. Int. J. Environ. Res. Public Health 2020, 17, 8272. [Google Scholar] [CrossRef] [PubMed]
- Mauro, V.; Lorenzo, M.; Paolo, C.; Sergio, H. Treat all COVID 19-positive patients, but do not forget those negative with chronic diseases. Intern. Emerg. Med. 2020, 15, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Pant, S.; Koirala, S.; Subedi, M. Access to Maternal Health Services during COVID-19. Eur. J. Med. Sci. 2020, 2, 48–52. [Google Scholar] [CrossRef]
- Nab, M.; van Vehmendahl, R.; Somers, I.; Schoon, Y.; Hesselink, G. Delayed emergency healthcare seeking behaviour by Dutch emergency department visitors during the first COVID-19 wave: A mixed methods retrospective observational study. BMC Emerg. Med. 2021, 21, 56. [Google Scholar] [CrossRef]
- Jones, S.A.; Gopalakrishnan, S.; Ameh, C.A.; White, S.; Van Den Broek, N.R.; Van Den Broek, N.R. ‘Women and babies are dying but not of Ebola’: The effect of the Ebola virus epidemic on the availability, uptake and outcomes of maternal and newborn health services in Sierra Leone. BMJ Glob. Health 2016, 1, 65. [Google Scholar] [CrossRef] [Green Version]
- Townsend, R.; Chmielewska, B.; Barratt, I.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Global changes in maternity care provision during the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine 2021, 37, 100947. [Google Scholar] [CrossRef]
- Germain, S.; Yong, A. COVID-19 Highlighting Inequalities in Access to Healthcare in England: A Case Study of Ethnic Minority and Migrant Women. Fem. Leg. Stud. 2020, 28, 301–310. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author, Year | Data Source | Study Area | Study Population and Sample | Study Period | Health Service | Main Results |
|---|---|---|---|---|---|---|
| Abebe, 2021 | Medical records from Tikur Anbessa Specialized Hospital | Ethiopia | Follow-up visits (n = 7717) and admissions (n = 3310) between December 2018–June 2019 and follow-up visits (n = 4597) and admissions (n = 2383) between December 2019–June 2020 | December–June 2018–2019 vs. 2019–2020 | General 1 | Reduction in follow-up visits (40%) and admissions (28%) from March 2020, compared with the same period in 2019. Visits reduced especially among patients receiving renal, neurological, cardiac, and antiretroviral treatment (68–51.4%). No significant changes were observed among pediatric and adult admissions. |
| Howarth, 2021 | Private health insurer claims records | United Kingdom (UK) | Claims to private health centers in the United Kingdom (n = aggregated data) 2 | January 2018–August 2020 | General | Reduction in healthcare claims in general (70%) from March 2020 (lockdown), undergoing an increase over the following months without reaching the pre-pandemic levels. Visits in mental health differed from the general pattern, with increased utilization (20%) compared to previous years. 3 |
| Siedner, 2020 | Africa Health Research Institute Demographic Health Surveillance System | KwaZulu Natal, South Africa | Visit to rural clinics (n = 46,523) 2 | January–March vs. March–April vs. May–June 2018 vs. 2019 vs. 2020 | General | Reduction in the number of childcare visits (50%), including preventive procedures, and sustained utilization of HIV services and adult outpatient clinics during the national lockdown (March–June 2020), compared to the previous periods. No significant changes were observed at a general level in the use of services. Childcare visits recovered over the following three months to pre-lockdown levels. |
| Whaley, 2020 | Aggregate data on health insurance claims | United States of America (USA) | Population with health insurance in 2018 (n = 5.6 million), 2019 (n = 6.4 million), and 2020 (n = 6.8 million) | January–February and March–April 2018 vs. 2019 vs. 2020 | General | Reduction in the utilization of a number of preventive services, elective procedures, and in-person office visits (different values according to the type of service or procedure) in March and April 2020. No significant changes in emergency care, maternal health, or medication prescription were observed. Utilization of telemedicine visits increased. Associated factors (AF): patients living in poor areas and most ethnic/racialized minorities were less likely to experience a reduction in in-person visits but also to have fewer visits of telemedicine. |
| Zhang, 2020 | Aggregate data on China UnionPay Healthcare bank transactions | China | Health care transactions (n = 300 million) 2 | January–March 2019 vs. December 2019–February 2020 vs. November 2019–April 2020 | General | Reduction in daily expenditure on health (37.8%) and in number of visits to health services (40.8%) from January 2020. AF: higher probability of utilization of health services was associated with cities with lower rates of COVID-19 cases, less strict measures, and not located in the western region of the country. |
| Ojetti, 2020 | Medical records from an urban tertiary teaching hospital | Italy | Admissions to the emergency department (ED) (n = 16,281) | February–March 2019 vs. 2020 | ED | Reduction in ED admissions (37.6%) for several diseases in 2020 compared to 2019. There was an increase in triage emergency levels for ED admissions and in hospitalization rates (different values according to the type of admission). |
| Mahmassani, 2021 | Administrative records of the emergency department of the American University of Beirut Medical Center | Beirut, Lebanon | ED visits, between November 2019–February 2020 (n = 16,271) and February–May 2020 (n = 8587) | November 2019–February 2020 vs. February–May 2020 | ED | Reduction in general (47.2%) and pediatric (66.6%) ED visits from February 2020, compared to previous months.AF: higher probability of utilization was associated with elderly patients and those who required hospital admission and/or critical care, with a higher mortality rate, and with non-communicable diseases and bacterial infections. |
| Cano-Valderrama, 2020 | Medical records from 3 hospitals | Spain | Patients who underwent emergency surgery in 2019 (n = 285) and 2020 (n = 117) | May–April 2019 vs. 2020 | ED (Acute Surgery Care) | Reduction in surgeries (58.9%) during lockdown (March–May 2020). Longer waiting time between the onset of symptoms and arrival at the emergency room and a greater number of complications (especially in elective procedures) were observed. |
| Sokolski, 2021 | Medical records from cardiology departments of 15 health centers in 12 countries | 15 centers in 12 European countries and USA | Patients admitted to the emergency and cardiology departments (n = 54,331) 2 | March–April 2019 vs. 2020 | ED (cardiology) | Reduction in patient admissions (IRR 0.68) in 2020, compared to 2019, across the various pathologies treated (different levels of reduction that vary from IRR 0.66–0.68). |
| Tsioufis, 2020 | Medical records from a tertiary General Hospital | Athens, Greece | Visits to the Emergency Cardiology Department and admissions to Cardiology Wards and Intensive Care Unit (n = aggregated data) 2 | January–April 2018 vs. 2019 vs. 2020 | ED (cardiology) | Reduction in visits to the emergency cardiology department during March (41.1%) and April (32.7%) 2020, compared to previous periods. |
| Ball, 2020 | Aggregate data on hospital activity from 9 NHS hospitals | UK | Admissions and visits to ED for cardiovascular disease October 2018–May 2019: admissions (n = 599,372) and ED visits (n = 506,516); October 2019–May 2020: admissions (n = 513,703) and ED visits (n = 435,653) | October–May 2018–2019 vs. 2019–2020 | ED (cardiovascular diseases) | Reduction in admissions (57.9%) and ED visits (52.9%) from March 2020, compared to the previous period. |
| Choi, 2021 | Medical records from 6 hospitals | South Korea | Patients under 18 years of age seen in pediatric ED (n = aggregated data) 2 | January 2017–November 2020 | ED (pediatrics) | Reduction in pediatric ED visits (43.6%) in 2020 compared to previous years, although a significantly increased proportion of visits for injuries (9.4%) during the COVID-19 outbreak. AF: higher probability of use was associated with male patients. |
| Dopfer, 2020 | Medical records from the University Hospital of Hannover | Hanover, Germany | Pediatric ED visits (n = 5424) 2 | January–April 2019 vs. 2020 | ED (pediatrics) | Reduction in pediatric ED visits (63.8%) from lockdown in 2020. AF: higher probability of using services was associated with patients under one year of age and cases requiring hospitalization, although not with intensive care admissions. |
| Finkelstein, 2021 | Medical records from the Pediatric Emergency Research Network | Canada | Patients under 18 years of age who attended the ED in 2018 (n = 211,085), 2019 (n = 207,673), and 2020 (n = 159,049) | January 2018–January 2020 vs. January–March 2020 vs. March–April 2020 | ED (pediatrics) | Reduction in weekly pediatric ED visits (58%), in re-visits (55%), in visits to trauma (increase in proportion of total visits), and to mental health (56 to 60% depending on the age group) from March 2020, compared to previous years. Increase in the proportion of ward (OR 1.39) and ICU (OR 1.2) admissions. |
| Goldman, 2020 | Medical records from 18 pediatric emergency departments | British Columbia, Canada | Pediatric ED visits (0–16 years): March–April 2019 (n = 22,654); December 2019–January 2020 (n = 31,525); January–March 2020 (n = 26,654); March–April 2020 (n = 7535) | March–April 2019 vs. December 2019–January 2020 vs. January–March 2020 vs. March–April 2020 | ED (pediatrics) | Reduction in visits to pediatric emergencies (57 to 70%), especially during the peak of the pandemic (March–April 2020), compared to previous periods. Admission proportion almost doubled (4% pre-pandemic to 7% during the peak pandemic period). Average acuity of illness was higher during the pandemic period. |
| Percul, 2021 | Medical records from the Italian Hospital of Buenos Aires | Buenos Aires, Argentina | Patients under 18 years of age treated for appendicitis in 2019 (n = 117) and 2020 (n = 50) | March–August 2019 vs. 2020 | ED (pediatrics) | Reduction in appendicitis admissions (25%) in 2020 compared to 2019, with no significant differences in the mean time to consultation. An increase in peritonitis cases was observed, although the incidence of complications decreased (not significant in both cases). |
| Yamamoto, 2021 | Medical records from the Tokyo Metropolitan Children’s Medical Center | Tokyo, Japan | Patients under 18 years of age seen in pediatric ED between January–September 2017–2019 (mean n = 26,948 *) and January–September 2020 (n = 15,998) | January–September 2017–2019 vs. 2020 | ED (pediatrics) | Reduction in pediatric ED visits (40.6%) in 2020 compared to previous periods, with an increase in the proportion of visits for exogenous causes (6.6% vs 3%). Visits increased slightly as of May until September2020, without reaching levels of previous years. 3 |
| Kute, 2021 | Medical records from the Kidney Disease Institute and Research Center | India | Patients treated in kidney disease services in 2019 (n = 109,572) and 2020 (n = 87,714) | January 2019–December 2020 | SC: nephrology | Reduction in visits and admissions, transplants, and other elective procedures (different values according to the type of service or procedure) in 2020, compared to 2019. Slight increase in activity between July and October, without reaching previous levels, with a further reduction starting in November 2020. 3 |
| Morris, 2021 | NHS population-based datasets | UK | Patients referred for suspected or diagnosed colorectal cancer (n = monthly average mean) 2 | January–December 2019 vs. January–October 2020 | SC: oncology | Reduction in the monthly number of referrals for suspected cancer (63%) and for treatment (22%), colonoscopies (92%), and surgeries (31%) from April 2020, compared to 2019 and the preceding months. Relative increase in radiotherapy use (44%) due to increased use of short-course regimens. Monthly rate of referrals and other procedures returned to 2019 levels by October 2020. |
| Pareek, 2021 | Medical records from the Gujarat Cancer Research Institute | Gujarat, India | Cancer patients visits to the oncology department between January–March (n = 4363) and March–May (n = 895) 2020 | January–March vs. March–May 2020 | SC: oncology | Reduction in visits from lockdown (different values according to the type of cancer) in March 2020, compared to the previous months. 3 |
| Shi, 2021 | Medical records from 13 pediatric tertiary cardiac centers | China | Patients who underwent cardiac surgery in 2018 (n = 19,398), 2019 (n = 19,620) and 2020 (n = 4740) | January–April 2018 vs. 2019 vs. 2020 | SC: pediatric surgery | Reduction in the total surgical volume median (25 cases) compared to 2018 (148 cases) and 2019 (158 cases). Increase in the proportion of emergency operations (6.3%) during 2020, compared to previous years. Increase in patients followed-up via the internet or phone (26.4% in 2020 vs 9.5% and 8.9% in 2019 and 2018). |
| Ambrosetti, 2021 | Medical records from the University Hospital of Geneva | Geneva, Switzerland | Admissions to the psychiatric ED from April to May 2016 (n = 702) and 2020 (n = 579) | April–May 2016 vs. 2020 | SC: psychiatry | Reduction in admissions (17.5%) in psychiatric ED in 2020 compared to 2016. AF: the probability to be admitted was more associated with severe psychopathologies and single patients, who arrived by ambulance, with suicidal behaviors, behavioral disorders, and psychomotor agitation, and were more likely to be involuntarily hospitalized after consultation in ED. |
| Aragona, 2020 | Medical records from the National Institute for Health, Migration and Poverty | Italy | Patients in a vulnerable situation who received at least one psychiatric intervention from February (n = 286) or March (n = 269) from 2017 to 2020 2 | February–March 2017 vs. 2018. vs. 2019 vs. 2020 | SC: psychiatry | Reduction in visits (46.6%) to mental health in March 2020. Follow-up visits of patients from February to March decreased more (17.5% patients), compared to previous years (30% patients). |
| Jesenšek, 2021 | Medical records from the Institute of Physical Medicine and Rehabilitation | Slovenia | Patients referred to rehabilitation in 2019 (n = 4132) and 2020 (n = 2317) | March–August 2019 vs. 2020 | SC: rehabilitation | Reduction in the global volume of patients (44%), first visits (42%), and follow-ups (60.9%), as well as number of sessions (71.1%), from lockdown in March 2020, compared to 2019. |
| Farrugia, 2021 | Medical records from Mater Dei Hospital | Malta | Admissions for acute exacerbations of chronic obstructive pulmonary disease in 2019 (n = 259) and 2020 (n = 119) | March–May 2019 vs. 2020 | SC: respiratory diseases | Reduction in admissions (54.2%) in 2020 compared to 2019. Increase in the mortality of admitted patients (19.3% vs. 8.4%). |
| Burt, 2021 | Medical records from Kawempe National Referral Hospital | Kawempe, Uganda | Visits to antenatal (n = 14,401), maternal health (n = 33,499), childcare (n = 111,658) and SRH (n = 57,174) services 2 | July 2019–December 2020 | SC: sexual and reproductive health (SRH) (antenatal, maternal, pediatrics, and family planning) | Reduction in antenatal, childcare, and family planning visits, as well as hospital deliveries (different values according to the type of service or procedure), during the lockdown months (March–June 2020), compared to previous months, without clear subsequent recovery. Increase in pregnancy complications and fetal and infant outcomes. |
| Das Neves, 2021 | Medical records from Marrere Health Center and monthly official statistics from the Ministry of Health | Nampula, Mozambique | Visits to SRH services (n = aggregated data) 2 | March–May 2019 and 2020 | SC: SRH (maternal and child health) | Reduction in family planning visits (28%), elective C-sections (28%), first antenatal visits (26%), hospital deliveries (4%) (increase in out-of-hospital deliveries by 74%), and child vaccination (20%). Only hospital deliveries drops were statistically significant. |
| Jensen and McKerrow, 2020 | Medical records from the KwaZulu-Natal District Health Information System | KwaZulu-Natal district, South Africa | Visits to child health services (aggregated data) 2 | January 2018–June 2020 | SC: SRH (maternal and child health) | Reduction in clinical visits (36%), hospital admissions (50%), delivery of services (from 6% to 54% depending on the service) in children under 5 years of age from March 2020. Modest increase in clinic visits as of May 2020, without reaching levels of preceding years. Among delivery of services, immunization coverage increased almost to pre-pandemic levels. |
| Justman, 2020 | Medical records from a tertiary referral center | Haifa, Israel | Pregnant women (n = aggregated data) 2 | March–April 2019–2020 | SC: SRH (maternal and child health) | Reduction in visits (from 18.1% to 36.4% according to the type of visit), deliveries (17.1%) and admissions (22.3%) to the obstetrics and gynecology department in 2020 compared to 2019. No significant changes were observed in the rate of C-sections, although a greater number of vaginal births during the outbreak (16.7% in 2020 vs. 6.8% in 2019), between the two periods. |
| KC, 2020 | Data collected from a prospective observational study in 9 hospitals (SUSTAIN and REFINE studies) | Nepal | Pregnant women (n = 21,763) | January–March vs. March–May 2020 | SC: SRH (maternal and child health) | Reduction in hospital deliveries (52.4%), especially vaginal births, from lockdown in March 2020. Increase in preterm births (24.5% before lockdown vs. 26.2% during lockdown), neonatal deaths (13 per 1000 livebirths vs. 40 per 1000 livebirths) and women admitted with complications during labor (6.7% vs. 8.7%, not statistically significant). AF: lower utilization of SRH services was less likely among users of disadvantaged ethnic groups and poor perceived quality of care. |
| Marqués, 2021 | Medical records from the Cambridge University Hospitals NHS Foundation Trust | Cambridge, UK | Women complaining of a 1st episode of reduced fetal movements in 2019 (n = 810) and 2020 (n = 803) | March–April 2019 vs. 2020 | SC: SRH (maternal and child health) | Reduction in 1st visits for reduced fetal movements (RFM) during 2020, compared to the same period in 2019 (18% vs. 22%). AF: primiparous women were more likely to attend with RFM. |
| Shakespeare, 2021 | Medical records from Mpilo Central Hospital | Zimbabwe | Women who gave birth from January to June 2020 (n = aggregated data) 2 | January–March vs. April–June 2020 | SC: SRH (maternal and child health) | Reduction in visits (5.8%) for hospital deliveries from April 2020, compared to previous months. No significant changes were observed in maternal or perinatal mortality and morbidity, nor in workload, although the number of deliveries and C-sections fell. Neonatal deaths increased, not significantly. |
| Spurlin, 2020 | Medical records from the New York Presbyterian—Columbia University Irving Medical Center | New York, USA | Patients who attended OB-GYN (obstetrics–gynecology) services from February to March 2020 for emergency visits (n = 275), GYN surgeries (n = 212), OB surgeries (n = 237), and from March to April 2020 for emergency visits (n = 79), GYN surgeries (n = 79), OB surgeries (n = 181) | February–March vs. March–April 2020 | SC: SRH (obstetrics and gynecology) | Reduction in the average weekly OB-GYN ED consults (60.3%) and GYN surgeries (79.3%), whereas OB surgeries remained stable, from March 2020 compared to the previous period. No significant differences in the proportion of OB-GYN ED consults and GYN surgeries were observed, although the proportion of OB surgeries increased significantly (54.6% before March vs. 79.7% from March 2020). |
| Chiba, 2021 | Medical records from the Medical Center of the University of Southern California and Los Angeles County | Los Angeles, USA | Patients admitted to trauma in 2019 (n = 1143) and 2020 (n = 1202) | March–June 2019 vs. 2020 | SC: traumatology | Increase in the number admissions (different values according to the type of trauma) during the analyzed period of 2020, compared to 2019. Increase in admissions due to falls (32.4%) (especially elderly), injuries from the use of weapons (39.3%), suicides (38.5%, not statistically significant), and positivity in the use of substances (52.1% in 2020 vs. 40.2% in 2019). Reduction in severe trauma (38.7% vs. 46.7%), mortality (4.1% vs. 5.9%), and ICU admission rates (26.3% vs. 31.5%). There were non-significant reductions in admissions due to traffic accidents (pedestrian or motor). |
| Horan, 2021 | Medical records from the National Neurosurgical Center at Beaumont Hospital | Dublin, Ireland | Referrals to the trauma department in 2019 (n = 527) and 2020 (n = 437) | March–May 2019 vs. 2020 | SC: traumatology | Reduction in trauma referrals (17.1%) in 2020 compared to 2019. No significant changes were observed between the profiles most associated with shunts between the two years, although there were changes in the type of diagnosis (fewer brain and spinal injuries and cranial fractures). AF: referrals were more likely among men, people over 60, alcohol consumers. |
| Alexander, 2020 | IQVIA National Disease and Therapeutic Index | USA | Visits to primary care (n = 875.6 million) 2 | January 2018–June 2020 | PC | Reduction in PC health services (21.4%) in 2020 compared to 2018 and 2019. Decreases in in-person visits (50.2%) and increases in telemedicine visits (1.1%) were observed. Evaluations and medication prescriptions were less frequent. |
| Sato, 2021 | Administrative claims from the DeSC database (health insurance claims) | Japan | Patients with chronic neurological diseases 2 | March–November 2020 | PC | Reduction in visits for different chronic neurological diseases (RR 0.9), except one that increased (migraines, RR 1.15), from April 2020. Telephone appointments were most frequently used in April–May (representing 5% of the visits), especially in the case of migraines (OR 2.08). The changes yielded different effects depending on the disease. |
| Song, 2021 | Medical records from the Independence Blue Cross | USA | Women who had mammograms from January 2018 to March 2020 for screening (n = 213,168) and diagnosis (n = 55,879), and from March to July 2020 for screening (n = 27,970) and diagnosis (n = 10,233) | January 2018–March 2020 vs. March–July 2020 | Preventive services | Reduction in the volume of screening (58%) and diagnostic (38%) mammograms from March 2020, compared to the preceding months and to the previous years. Increase in activity from May 2020, remaining 14% below previous months levels. AF: greater use was associated with women with a previous diagnosis. |
| First Author, Year | Data Collection Method | Study Area | Study Population and Sample | Study Period | Health Service | Main Results |
|---|---|---|---|---|---|---|
| Kahraman et al., 2021 | Online survey | Turkey | Patients with lysosomal storage disease in enzyme replacement therapy (n = 75) | July–October 2020 | SC: endocrinology | Characteristics of the services: lack of resources (hospital beds) Characteristics of the population: fear of contagion, difficulties in obtaining medication, transport difficulties |
| Nicholson et al., 2020 | Online survey | Ireland | Parents of children under 16 (n = 1044) | June 2020 | SC: pediatrics | Characteristics of the population: fear of contagion, perception of overuse of services or lack of need, fear of being judged for seeking care, poor understanding of government messages, concern regarding travel (avoiding public transport). |
| Benjamen et al., 2021 | Online survey (n = 77, of which 11 were interviewed in depth) | Ottawa, Canada | Doctors with experience caring for refugee populations (n = 77) | May–August 2020 | SC: psychiatry | Characteristics of the services: limited availability of providers and community resources, slight increase in the offer of virtual care psychotherapy. Characteristics of the population: fear of contagion, perceived lack of services, technological barriers |
| Halley et al., 2021 | Online surve | USA | Relatives (n = 139) and patients affected by undiagnosed rare diseases (n = 275) | April–June 2020 | SC: undiagnosed rare diseases care | Characteristics of the services: barriers to access essential services (difficulties in contacting services, procedures re-scheduled, lack of medical supplies, insufficient telemedicine care offered), restrictions on companions. Characteristics of the population: fear of COVID-19 contagion; impact on physical and mental health (stress due to not being able to receive treatment or as an aggravating factor of the disease). |
| Adelekan et al., 2021 | Semi-structured interviewer-administered questionnaire | Nigeria | Head nurses and midwives in primary health centers (n = 307) | March–September 2020 | SC: SRH (maternal and child health) | Characteristics of the services: difficulties regarding out-of-stock drugs and contraceptives. Characteristics of the population: economic difficulties (not being able to afford cost of transportation). |
| Karavadra et al., 2020 | Online survey | UK | Women who were pregnant or gave birth during the COVID-19 pandemic (n = 1451) | May 2020 | SC: SRH (maternal and child health) | Characteristics of the services: reduced frequency of scans, redistribution of services in different “zoned areas” based on “COVID wards” and “non-COVID” wards, lack of information, ban on presence of partner. Characteristics of the population: fear of contagion, perception of “impersonal care” from virtual consultations. |
| Khan et al., 2021 | Online survey | 64 middle- and low-income countries of Africa, Asia, and Latin America | Health professionals from tuberculosis treatment (n = 567) and HIV (n = 346) services | May–August 2020 | SC: tuberculosis and HIV care | Characteristics of the services: lack of material and medical supplies, difficulties in obtaining medical treatment, lack of alternatives for non-face-to-face care (e.g., telemedicine), postponement of visits for diagnoses and treatments. Characteristics of the population: fear of contagion, stigma, difficulties in accessing health services (alterations in transportation, restrictions), worsening economic situation. |
| García-Rojo et al., 2021 | Medical records (Hospital 12 de Octubre) | Spain | Patients on the waiting list for urological surgery (n = 350) | May 2020 | SC: urology | Characteristics of the services: increased waiting times for urological surgeries (designated as elective). |
| First Author, Year | Data Collection Method | Study Area | Study Population and Sample | Study Period | Health Service | Main Results |
|---|---|---|---|---|---|---|
| Zambrano et al., 2021 | Online semi-structured interviews and life histories | Colombia and Peru | Venezuelan migrant populations living in large cities in Colombia (n = 96) and Peru (n = 34) | July–September 2020 | General | Characteristics of the services: access to health services linked to legal immigration status. Characteristics of the population: severe economic difficulties, perceived discrimination of healthcare services on the basis of nationality |
| Das Neves et al., 2021 | Semi-structured interviews by phone (12) and in-person (9) | Nampula, Mozambique | Health professionals (n = 9), traditional birth attendants (n = 6) and patients (n = 6) | March–May 2019 and 2020 | SC: SRH (maternal and child health) | Characteristics of the services: limited resources (workforce), increase in waiting times Characteristics of the population: fear of contagion, avoiding healthcare except in emergencies |
| Gichuna et al., 2020 | Semi-structured interviews via mobile phone (phone call or videocall) | Kariobangi, Roysambu, and Jogoo Road areas (Nairobi, Kenya) | Sex workers from the study areas (n = 117), and health professionals from the Bar Hostess Empowerment and Support Program Centers (n = 15) | April–May 2020 | SC: SRH (family planning) and HIV care | Characteristics of the services: reduced activity, lack of medical supplies Characteristics of the population: economic difficulties, stigma |
| Hailemariam et al., 2021 | Online focal groups (6) and semi-structured interviews (9) | Kebeles, Ethiopia | Pregnant women who did not attend SHR services and health workers | September–November 2020 | SC: SRH (maternal and child health) | Characteristics of the population: perceived low quality of services, fear of contagion, stigma, playing down care needs, refusal to attend antenatal services. |
| Mizrak Sahin, and Nur Kabakci, 2020 | Semi-structured interviews by phone | Turkey | Pregnant women | During 2020, months not specified | SC: SRH (maternal and child health) | Characteristics of the services: elective visits were cancelled or postponed, difficulties in getting first visits. Characteristics of the population: fear of contagion, difficulties in contacting services for first visits. |
| Dos Santos et al., 2021 | 7 semi-structured interviews by phone | Ribeirão Preto, Brazil | Patients over 18 years old undergoing treatment for tuberculosis | June–August 2020 | SC: tuberculosis care | Characteristics of the population: economic difficulties, fear of contagion |
| Ahmed et al., 2020 | Workshops and in-person meetings in three pre-pandemic phases (semi-structured interviews, group and individual meetings), and a fourth phase via mobile phone | Bangladesh, Kenya, Nigeria, Pakistan | Health professionals (medical doctors, nurses, community health workers and assistants, pharmacists, and patent medicine vendors), pregnant women and women with children, health service managers | March 2018–May 2020 | PC | Characteristics of the services: worse access to services that were difficult to access before the pandemic (mental health, gender-based violence services), and preventive services, increase in cost of healthcare, lack of drugs and medical supplies. Characteristics of the population: fear of contagion, economic difficulties. |
| Danhieux et al., 2020 | Online semi-structured interviews | Belgium | General practitioners, nurses, and dieticians (n = 21) in primary care who work individually, monodisciplinary or in multidisciplinary groups | April–June 2020 | PC | Characteristics of the services: limited resources to treat, identify, and contact non-COVID-19 patients because of the redistribution of resources, especially among high-risk and vulnerable patients. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pujolar, G.; Oliver-Anglès, A.; Vargas, I.; Vázquez, M.-L. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 1749. https://doi.org/10.3390/ijerph19031749
Pujolar G, Oliver-Anglès A, Vargas I, Vázquez M-L. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(3):1749. https://doi.org/10.3390/ijerph19031749
Chicago/Turabian StylePujolar, Georgina, Aida Oliver-Anglès, Ingrid Vargas, and María-Luisa Vázquez. 2022. "Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 3: 1749. https://doi.org/10.3390/ijerph19031749
APA StylePujolar, G., Oliver-Anglès, A., Vargas, I., & Vázquez, M. -L. (2022). Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. International Journal of Environmental Research and Public Health, 19(3), 1749. https://doi.org/10.3390/ijerph19031749