
Burnout: A Review of Theory and Measurement



Abstract
:1. Introduction
2. Burnout: Definition and Development of This Construct
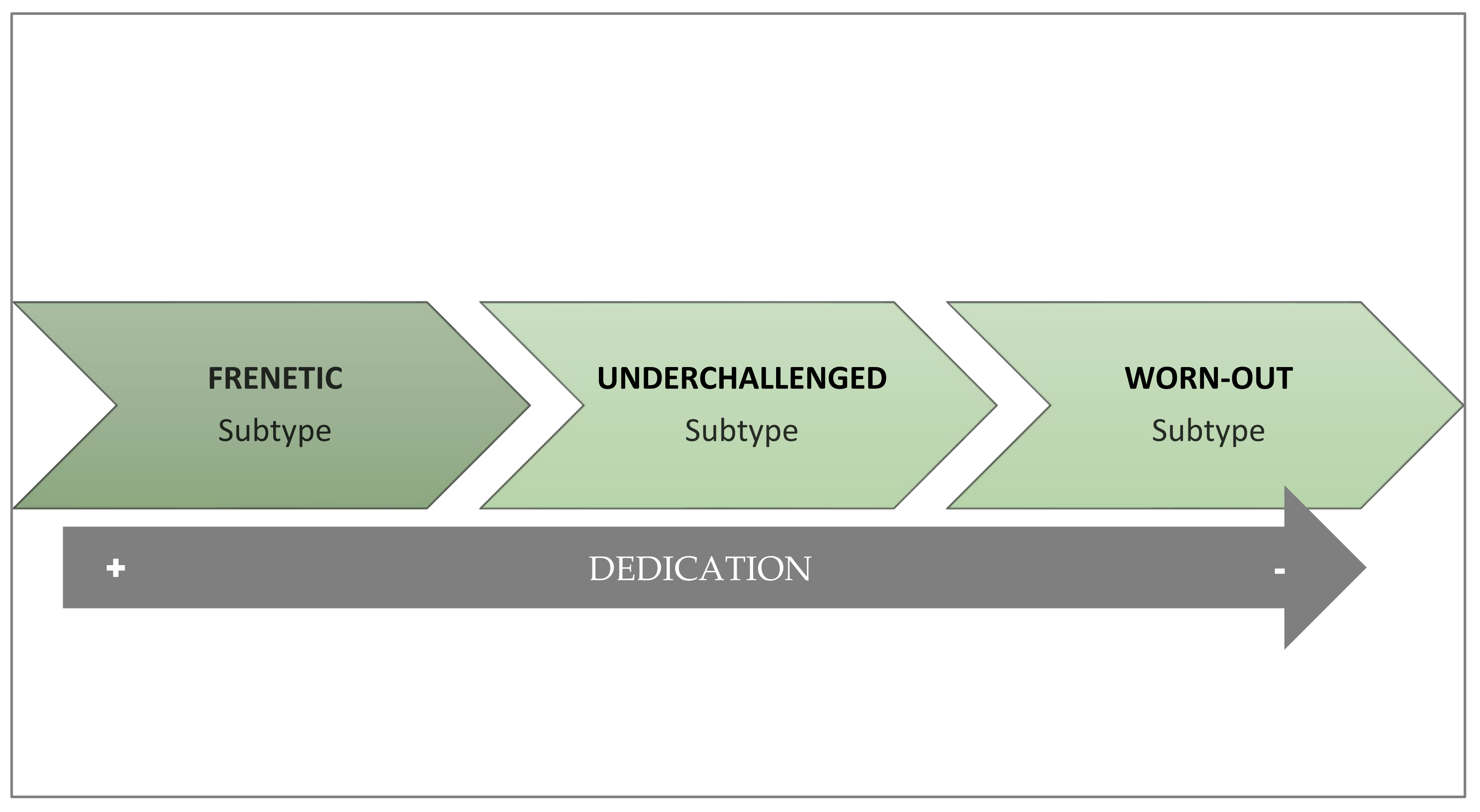
2.1. Subtypes of Burnout
2.2. Why Does Burnout Appear and How Does It Develop?
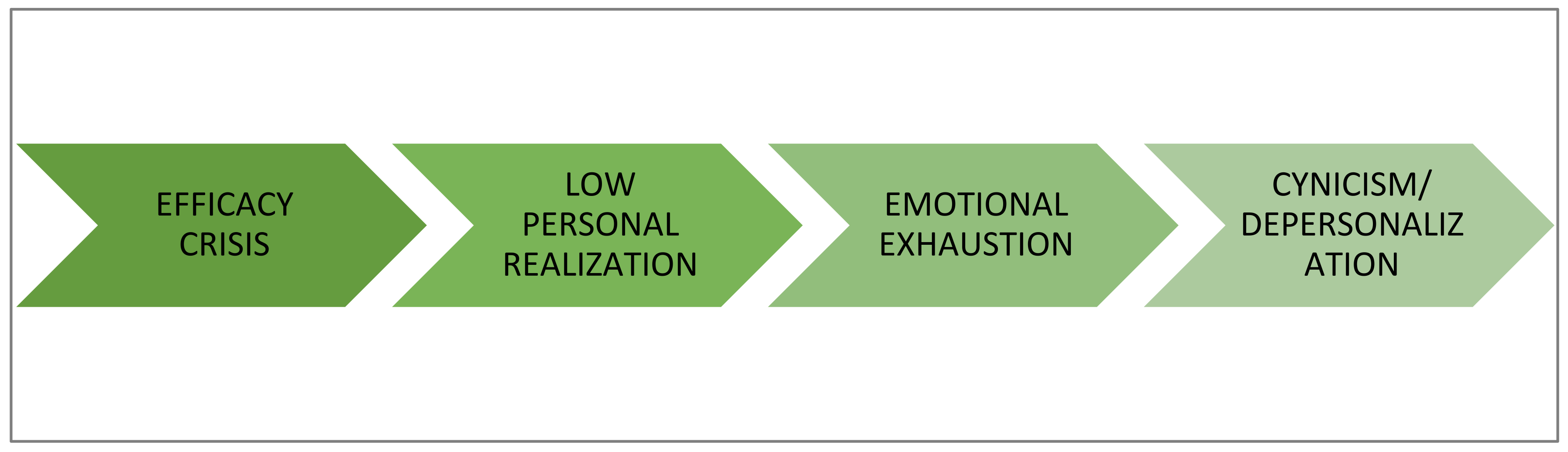
2.2.1. Social Cognitive Theory
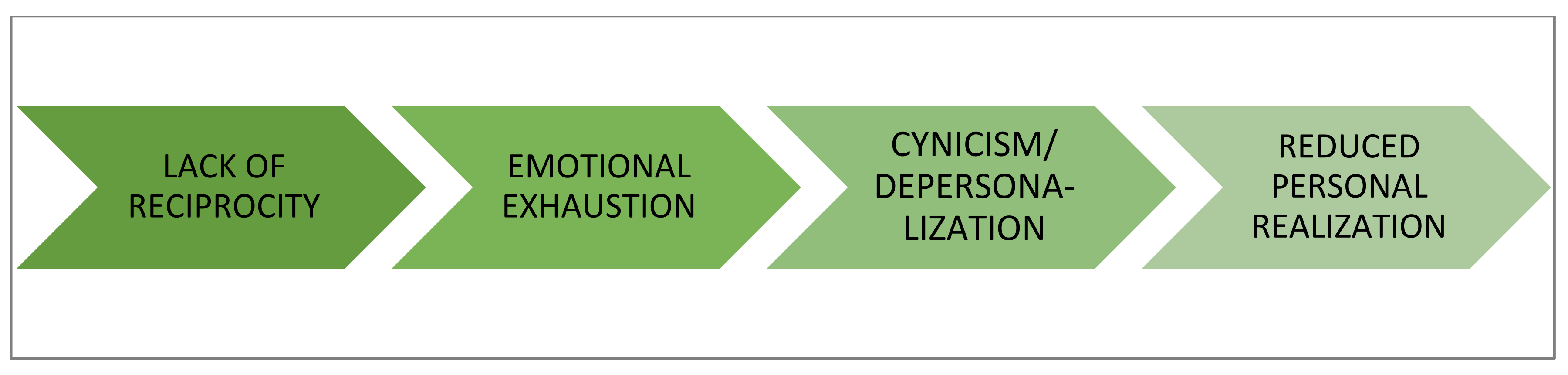
2.2.2. Social Exchange Theory
2.2.3. Organizational Theory
2.2.4. Demands–Resources Theory
2.2.5. Structural Theory
2.2.6. Theory of Emotional Contagion
3. What Circumstances Trigger Burnout?
3.1. Organizational Factors
3.1.1. Work Overload
3.1.2. Emotional Labor
3.1.3. Lack of Autonomy and Influence at Work
3.1.4. Ambiguity and Role Conflict
3.1.5. Inadequate Supervision and Perception of Injustice
3.1.6. Lack of Perceived Social Support
3.1.7. Poor Working Hours
3.2. Individual Factors Modulating Burnout
3.3. Future Research
4. Consequences of Burnout
4.1. Psychological Consequences
4.2. Health Consequences
4.3. Behavioral Consequences
- Mild: those affected have mild, unspecific physical symptoms (headaches, back pain, low back pain), show some fatigue, and become less operative.
- Moderate: insomnia, attention and concentration deficits appear. At this level, detachment, irritability, cynicism, fatigue, boredom, progressive loss of motivation, making the individual emotionally exhausted with feelings of frustration, incompetence, guilt, and negative self-esteem.
- Severe: increased absenteeism, task aversion and depersonalization, as well as alcohol and psychotropic drug abuse.
- Extreme: extreme behaviors of isolation, aggressiveness, existential crisis, chronic depression, and suicide attempts.
4.4. Organizational Consequences
4.5. Future Research
5. Prevention Strategies
5.1. Organizational Interventions Aimed at Work Structure
- Improving job characteristics. These actions are mainly aimed at quantitative workload reduction and qualitative work improvement through two main strategies:
- (1)
- Work redesign. This measure aims to partially change the objectives and tasks of the job while improving the quality of work by eliminating structural and/or procedural elements that interfere and generate stress [81]. It could also be considered job redesign the enrichment of jobs through the incorporation of new and more stimulating tasks that make the job more motivating and rewarding.
- (2)
- Modification of exposure times to potential stressors. This can be completed by reducing the time in which the worker is exposed to the most stressful elements of the job (such as, for example, attention to users or patients) through job rotation, or, if necessary, by performing other tasks or activities [82,83].
- Humanization of schedules and implementation of work–life balance plans. This intervention involves organizing and making work schedules and shifts more flexible to allow for the reconciliation of personal and professional life [84]. In this sense, variable work shifts and long working hours exceeding 8 h should be eliminated.
- Managers’ leadership development. Supervisor support and leadership is considered an important work resource capable of reducing burnout levels in employees. However, not all supervisors employ an adequate leadership style. In this sense, several studies have shown that authentic [54], transformational [85], and servant [86] leadership styles are related to decreased burnout and have positive effects on employees’ psychological resources [87]. For this reason, these are the leadership styles that should be developed and trained to avoid the occurrence of this syndrome. Additionally, the performance of leaders and specifically leadership behaviors should also be regularly evaluated by the individuals working with them to identify potentially adverse aspects that could trigger burnout.
- Use of rewards and incentives that are not only financial. Employees can be motivated by rewards that do not always need to be of a financial nature. Recognizing work well done is a very efficient way to increase workers’ motivation levels and prevent burnout [48]. As indicated previously, one of the factors causing efficiency crises, which in turn were triggers of burnout, was the lack of reinforcement and appraisal by supervisors. In addition to recognition of accomplishment, other types of rewards such as greater time flexibility (which can facilitate work–life balance) or protected time to achieve personally meaningful work goals can enhance well-being. In contrast, employing simple financial rewards may be less effective by encouraging overwork and pressure to achieve goals, which promote burnout.
- Development of welcoming programs. Since role conflicts and ambiguities are potential triggers of burnout, it is advisable for organizations to develop welcoming processes for new workers, where the mission of the position, tasks, and objectives to be fulfilled are explained with absolute clarity and they are progressively introduced to the most stressful elements of the job, always offering support from the supervisor or other colleagues [88].
- Burnout monitoring and design of customized plans. This consists of periodically conducting surveys and measurements of workers to “monitor” the organization’s burnout levels and compare the scores of workers according to units, location, position, supervisor, etc. (e.g., [89]). The aim is basically to identify the appearance of the first symptoms, thus preventing the syndrome from becoming chronic. It is important that, in addition to the levels of burnout, the organization identifies as precisely as possible the risk factors in the work environment that may be present to eliminate or minimize them. Additionally, since the specific way in which symptoms manifest themselves and which dimension is dominant varies in each work unit, to be effective it will be necessary to design interventions specific to the causes and consequences/symptoms identified.
- Institutionalization of occupational health and safety. This intervention refers to the obligation of organizations to incorporate in their structure departments or devices in the form of agreements with other entities to ensure the health and reduction of burnout in workers [90]. This intervention translates into (e.g., [91]):
- (1)
- Delivery of psychoeducational workshops on stress and burnout that can be scheduled in the same organization or by outsourcing the service.
- (2)
- Counseling services for workers with work-related problems. This action can be carried out within the organization or by outsourcing the service by referring the employee to a counseling specialist.
- (3)
- Referral to specialized health promotion services such as psychologists and medical specialists.
5.2. Interventions Promoted by the Organization Aimed at Employees
- Training. Through training, employees can acquire new skills and technical knowledge that increase their coping resources and improve their self-efficacy expectations. However, in addition to technical skills related to the job, organizations should plan training actions aimed at developing other types of personal and social skills that facilitate workers to implement individual strategies to promote their well-being and adjustment to the job [88,92]. Table 5 includes examples of training actions to prevent or manage burnout.
- Strengths-based interventions. Strengths-based interventions work from the premise that people have personal resources that can be used to cope with adversity. Using strengths is intrinsically motivating and satisfying. A strengths intervention typically unfolds in three phases, as described in Table 6.
- Coaching and guidance. These are non-directive methods that encourage employees to regain control of their emotional state and well-being on their own, so the coach/counselor will not “prescribe” any treatment. Instead, the coach/counselor will guide the employee to come up with (or with some assistance) coping strategies on their own [93]. This type of intervention is usually typical of secondary prevention, in the early stages of the syndrome, when it is assumed that the person still has the capacity to redirect it.
- Creation of support groups. Peer and team support has always been critical in helping professionals cope with the difficulties and challenges of day-to-day life. This support encompasses a wide range of activities, including the celebration of achievements or the creation of formal support groups. In this sense, organizations should incorporate activities into work processes that are conducive to such a sense of community as dedicating time to share ideas and knowledge about how to act and deal with day-to-day professional challenges [88]. Support groups refer to any group of coworkers, whether formal (expressly created by the organization) or informal (not created by the organization but arising spontaneously) that meet regularly to exchange information, give each other emotional support and/or solve work problems. What these groups have in common is that they offer recognition for work completed (even if objectives have not been achieved), comfort, help, and companionship. The primary objective of the support groups is to reduce the professionals’ feelings of loneliness and emotional exhaustion, as well as the exchange of knowledge to develop effective ways of dealing with problems. This intervention (e.g., two hours every two weeks) is one of the most widely employed interventions for intervening on burnout and its benefits have been repeatedly demonstrated [73]. While the creation of support groups is an individual focus intervention, in many cases it is encouraged by the organization, or should be.
5.3. Individual-Focused Interventions Promoted by the Individual
- Mindfulness training. A systematic review [96] of various specialized databases published between 2008 and 2017 concluded that mindfulness practice is effective in reducing burnout syndrome, both in its total values and in those corresponding to its dimensions, mitigating the negative psychosomatic and emotional effects of the syndrome, and increasing other positive ones such as empathy or concentration.
- Self-assessment. This intervention involves the self-observation of possible signs that could point to burnout. The way to do this is, for example, by keeping a diary of stress symptoms and related events such as specific symptoms, thoughts, feelings, and ways of coping with them. On the other hand, in addition to this type of diary, it is also important to measure the degree of burnout with a properly validated test, such as those indicated in the following section, and to compare one’s own score with that of a reference group or with oneself over time.
- Psychotherapy. Psychotherapeutic treatment of burnout syndrome is carried out in the most severe and serious cases (i.e., when the syndrome and its consequences are already being suffered). Psychotherapeutic treatment basically consists of developing emotional self-regulation and relaxation skills, problem solving, development of self-efficacy, and assertiveness and is generally based on the principles of cognitive-behavioral therapy [73,92]. This intervention may be funded by the organization; however, it will always be the individual him/herself who will make the decision to initiate a psychotherapy process. There are three types of techniques used to reduce burnout:
- (1)
- Cognitive techniques: these are aimed at the individual reevaluating and restructuring their appreciation and vision of stressful or problematic situations, so that they can deal with these situations more effectively. This type of technique is useful because people perceive situations subjectively and individually and, therefore, in a biased way. Cognitive techniques are aimed at identifying and modifying errors in the perception of reality to influence the emotions they provoke and the behavior they trigger.
- (2)
- Physiological deactivation techniques: the aim of this type of technique is to teach the person mechanisms to control, through relaxation, the increased physiological activation and anxiety caused by stressful stimuli.
- (3)
- Training in healthy lifestyle habits: physical exercise, a balanced diet, and restful sleep can help to reduce the symptoms of burnout.
5.4. Individually Driven, Work-Focused Interventions
- Time management. Employees who are at risk of burnout often feel that they lack the time to fulfill all their responsibilities or that they work long hours with no time for personal use and rest. Self-management of time consists of correctly planning one’s time by making efficient use of the time available, organizing tasks realistically, and delegating them when appropriate, as well as dedicating daily time for personal activities and recreation [79,80]. Although this intervention is promoted by each worker, to facilitate proper time management, organizations as indicated above can or should provide training and coaching actions to their workers [97].
- Job crafting. Unlike job redesign (explained above), which is managed and planned by the organization, job crafting is an individual bottom-up intervention, initiated by the employees themselves, which consists of actively modifying their job (as long as the job mission is fulfilled) by reconfiguring the way they approach tasks and negotiating the job content, allowing employees to adjust their jobs to their personal knowledge, skills and abilities, and to their preferences and needs. In other words, through job crafting, the work to be performed does not change but is adjusted to experience it in a more meaningful way. These adjustments can be of four types [98] and are summarized in Table 7.
5.5. Future Research
6. Assessment and Measurement
6.1. Generic Instruments
6.2. Specific Instruments
6.3. Future Research
7. Special Issue on “Occupational Stress and Health: Psychological Burden and Burnout”
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Han, S.; Shanafelt, T.D.; Sinsky, C.A.; Awad, K.M.; Dyrbye, L.N.; Fiscus, L.C.; Trockel, M.; Goh, J. Estimating the attributable cost of physician burnout in the United States. Ann. Intern. Med. 2019, 170, 784–790. [Google Scholar] [CrossRef]
- Simionato, G.; Simpson, S.; Reid, C. Burnout as an ethical issue in psychotherapy. Psychotherapy 2019, 56, 470–482. [Google Scholar] [CrossRef]
- Grow, H.M.; McPhillips, H.A.; Batra, M. Understanding physician burnout. Curr. Probl. Pediatric Adolesc. Health Care 2019, 49, 100656. [Google Scholar] [CrossRef]
- Epstein, E.G.; Haizlip, J.; Liaschenko, J.; Zhao, D.; Bennett, R.; Marshall, M.F. Moral distress, mattering, and secondary traumatic stress in provider burnout: A call for moral community. AACN Adv. Crit. Care 2020, 31, 146–157. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. Maslach Burnout Inventory. Manual; Consulting Psychologists Press: Palo Alto, CA, USA, 1981. [Google Scholar]
- Salanova, M.; Schaufeli, W.; Llorens, S.; Peiró, J.M.; Grau, R. Desde el “burnout” al “engagement”: ¿una nueva perspectiva? Rev. De Psicol. Del Trab. Y De Las Organ. 2000, 16, 117–134. [Google Scholar]
- Schaufeli, W.B.; Bakker, A.B.; van der Heijden, F.; Prins, J.T. Workaholism, burnout and well-being among junior doctors: The mediating role of role conflict. Work. Stress 2009, 23, 155–172. [Google Scholar] [CrossRef]
- Hewitt, D.B.; Ellis, R.J.; Hu, Y.Y.; Cheung, E.O.; Moskowitz, J.T.; Agarwal, G.; Bilimoria, K.Y. Evaluating the association of multiple burnout definitions and thresholds with prevalence and outcomes. JAMA Surg. 2020, 155, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; De Waele, J.; Ferrer, R.; Staudinger, T.; Borkowska, M.; Povoa, P.; Iliopoulou, K.; Artigas, A.; Schaller, S.J.; Shankar Hari, M.; et al. Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann. Intensive Care 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290. [Google Scholar] [CrossRef]
- Matsuo, T.; Kobayashi, D.; Taki, F.; Sakamoto, F.; Uehara, Y.; Mori, N.; Fukui, T. Prevalence of health care worker burnout during the coronavirus disease 2019 (COVID-19) pandemic in Japan. JAMA Netw. Open 2020, 3, e2017271. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, J.; Luo, C.; Hu, S.; Lin, X.; Anderson, A.E.; Bruera, E.; Yang, X.; Wei, S.; Qian, Y. A comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan, China. J. Pain Symptom Manag. 2020, 60, e60–e65. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Kamrai, D.; Mekala, H.; Mann, B.; Desai, K.; Patel, R.S. Focus on mental health during the coronavirus (COVID-19) pandemic: Applying learnings from the past outbreaks. Cureus 2020, 12, e7405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel Hadi, S.; Bakker, A.B.; Häusser, J.A. The role of leisure crafting for emotional exhaustion in telework during the COVID-19 pandemic. Anxiety Stress Coping 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Barriga Medina, H.R.; Campoverde Aguirre, R.; Coello-Montecel, D.; Ochoa Pacheco, P.; Paredes-Aguirre, M.I. The influence of work–family conflict on burnout during the COVID-19 pandemic: The effect of teleworking overload. Int. J. Environ. Res. Public Health 2021, 18, 10302. [Google Scholar] [PubMed]
- Lizana, P.A.; Vega-Fernadez, G. Teacher teleworking during the covid-19 pandemic: Association between work hours, work–family balance and quality of life. Int. J. Environ. Res. Public Health 2021, 18, 7566. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, J.Á.; Lázaro-Pérez, C.; Gómez-Galán, J. Predictors of burnout in social workers: The COVID-19 pandemic as a scenario for analysis. Int. J. Environ. Res. Public Health 2021, 18, 5416. [Google Scholar] [CrossRef]
- Daumiller, M.; Rinas, R.; Hein, J.; Janke, S.; Dickhäuser, O.; Dresel, M. Shifting from face-to-face to online teaching during COVID-19: The role of university faculty achievement goals for attitudes towards this sudden change, and their relevance for burnout/engagement and student evaluations of teaching quality. Comput. Hum. Behav. 2021, 118, 106677. [Google Scholar] [CrossRef]
- Panisoara, I.O.; Lazar, I.; Panisoara, G.; Chirca, R.; Ursu, A.S. Motivation and continuance intention towards online instruction among teachers during the COVID-19 pandemic: The mediating effect of burnout and technostress. Int. J. Environ. Res. Public Health 2020, 17, 8002. [Google Scholar] [CrossRef]
- Pressley, T. Factors contributing to teacher burnout during COVID-19. Educ. Res. 2021, 50, 325–327. [Google Scholar] [CrossRef]
- Sokal, L.; Trudel, L.E.; Babb, J. Canadian teachers’ attitudes toward change, efficacy, and burnout during the COVID-19 pandemic. Int. J. Educ. Res. Open 2020, 1. [Google Scholar] [CrossRef]
- Griffith, A.K. Parental burnout and child maltreatment during the COVID-19 pandemic. J. Fam. Violence 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Woine, A.; Mikolajczak, M.; Gross, J.; van Bakel, H.; Roskam, I. The role of cognitive appraisals in parental burnout: A preliminary analysis during the COVID-19 quarantine. Curr. Psychol. 2022, 1–14. [Google Scholar] [CrossRef]
- Montero-Marín, J. El síndrome de burnout y sus diferentes manifestaciones clínicas: Una propuesta para la intervención [The burnout syndrome and its various clinical manifestations: A proposal for intervention]. Anest. Analg. Reanim. 2016, 29, 1–16. [Google Scholar]
- Maslach, C. Understanding job burnout. In Stress and Quality of Working Life: Current Perspectives in Occupational Health; Rossi, A.M., Perrewé, P.L., Sauter, S.L., Eds.; Information Age Publishing: Charlotte, NC, USA, 2006; pp. 37–52. [Google Scholar]
- Bouza, E.; Gil-Monte, P.R.; Palomo, E.; Cortell-Alcocer, M.; Del Rosario, G.; González, J.; Gracia, D.; Martínez Moreno, A.; Melero Moreno, C.; Molero García, J.M.; et al. Síndrome de quemarse por el trabajo (burnout) en los médicos de España. Rev. Clínica Española 2020, 220, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Freudenberger, H.J. Staff burn-out. J. Soc. Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Bumout. Hum. Behav. 1976, 5, 16–22. [Google Scholar]
- Taris, T.W.; Le Blanc, P.M.; Schaufeli, W.B.; Schreurs, P.J. Are there causal relationships between the dimensions of the Maslach Burnout Inventory? A review and two longitudinal tests. Work. Stress 2005, 19, 238–255. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.B.; Buunk, B.P. Burnout: An overview of 25 years of research and theorizing. In The Handbook of Work and Health Psychology, 2nd ed.; Schabracq, M.J., Winnubst, J.A.M., Cooper, C.L., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2003; pp. 282–424. [Google Scholar]
- Salanova, M.; Llorens, S.; García-Renedo, M.; Burriel, R.; Bresó, E.; Schaufeli, W.B. Towards a four-dimensional model of burnout: A multigroup factor-analytic study including depersonalization and cynicism. Educ. Psychol. Meas. 2005, 65, 807–819. [Google Scholar] [CrossRef]
- Montero-Marin, J.; Prado-Abril, J.; Piva Demarzo, M.M.; Gascon, S.; García-Campayo, J. Coping with stress and types of burnout: Explanatory power of different coping strategies. PLoS ONE 2014, 9, e89090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demarzo, M.; García-Campayo, J.; Martínez-Rubio, D.; Pérez-Aranda, A.; Miraglia, J.L.; Hirayama, M.S.; de Salvo, V.M.A.; Cicuto, K.; Favarato, M.L.; Terra, V.; et al. Frenetic, under-challenged, and worn-out burnout subtypes among Brazilian primary care personnel: Validation of the Brazilian “burnout clinical subtype questionnaire”(BCSQ-36/BCSQ-12). Int. J. Environ. Res. Public Health 2020, 17, 1081. [Google Scholar] [CrossRef] [Green Version]
- Pines, A.M. Teacher burnout: A psychodynamic existential perspective. Teach. Teach. 2002, 8, 121–140. [Google Scholar] [CrossRef]
- Cherniss, C. Role of professional self-efficacy in the etiology and amelioration of burnout. In Professional Burnout: Recent Developments in Theory and Research; Schaufeli, W.B., Maslach, C., Marek, T., Eds.; Taylor & Francis: Abingdone, UK, 1993; pp. 135–149. [Google Scholar]
- Llorens, S.; García-Renedo, M.; Salanova, M. Burnout como consecuencia de una crisis de eficacia: Un estudio longitudinal en profesores de secundaria. Rev. De Psicol. Del Trab. Y De Las Organ. 2005, 21, 55–70. [Google Scholar]
- Manzano-García, G.; Ayala-Calvo, J.C. New perspectives: Towards an integration of the concept “burnout” and its explanatory models. An. De Psicol. 2013, 29, 800–809. [Google Scholar]
- Llorens, S.; Salanova, M. Burnout: Un problema psicológico y social. Riesgo Labor. 2011, 37, 26–28. [Google Scholar]
- Schaufeli, W.B.; Maassen, G.H.; Bakker, A.B.; Sixma, H.J. Stability and change in burnout: A 10-year follow-up study among primary care physicians. J. Occup. Organ. Psychol. 2011, 84, 248–267. [Google Scholar] [CrossRef] [Green Version]
- Cox, T.; Kuk, G.; Leiter, M. Burnout, health, work stress and organizational healthiness. In Professional Burnout: Recent Developments in Theory and Research; Schaufeli, W.B., Maslach, C., Marek, T., Eds.; Taylor & Francis: Abingdone, UK, 1993; pp. 177–193. [Google Scholar]
- Golembiewski, R.T.; Munzenrider, R.; Carter, D. Phases of progressive burnout and their work site covariants: Critical issues in OD research and praxis. J. Appl. Behav. Sci. 1983, 19, 461–481. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E. Job demands–resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Manzano, G.; Ramos, F. Enfermería hospitalaria y síndrome de burnout. Rev. De Psicol. Del Trab. Y De Las Organ. 2000, 16, 197–213. [Google Scholar]
- Hatfield, E.; Cacioppo, J.T.; Rapson, R.L. Emotional contagion. Curr. Dir. Psychol. Sci. 1993, 2, 96–100. [Google Scholar] [CrossRef]
- Bakker, A.B.; Schaufeli, W.B. Burnout contagion processes among teachers. J. Appl. Soc. Psychol. 2000, 30, 2289–2308. [Google Scholar] [CrossRef]
- Petitta, L.; Jiang, L. How emotional contagion relates to burnout: A moderated mediation model of job insecurity and group member prototypicality. Int. J. Stress Manag. 2020, 27, 12. [Google Scholar] [CrossRef]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. New insights into burnout and health care: Strategies for improving civility and alleviating burnout. Med. Teach. 2017, 39, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, J.S.; Choe, K.; Kwak, Y.; Song, J.S. Mediating effects of workplace violence on the relationships between emotional labour and burnout among clinical nurses. J. Adv. Nurs. 2018, 74, 2331–2339. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, M.; Santos, A.; Chern, G.T. Emotional intelligence as a moderator in the emotional labour-burnout relationship: Evidence from Malaysian HR professionals. Int. J. Work. Organ. Emot. 2016, 7, 143–164. [Google Scholar] [CrossRef]
- Orgambídez, A.; Almeida, H. Core burnout and power in portuguese nursing staff: An explanatory model based on structural empowerment. Workplace Health Saf. 2019, 67, 391–398. [Google Scholar] [CrossRef]
- Kaya, Ç.; Altınkurt, Y. Role of psychological and structural empowerment in the relationship between teachers’ psychological capital and their levels of burnout. Educ. Sci. /Egit. Ve Bilim 2018, 42, 193. [Google Scholar] [CrossRef] [Green Version]
- Acker, G.M. Role conflict and ambiguity: Do they predict burnout among mental health service providers? Soc. Work. Ment. Health 2003, 1, 63–80. [Google Scholar] [CrossRef]
- Laschinger, H.K.S.; Borgogni, L.; Consiglio, C.; Read, E. The effects of authentic leadership, six areas of worklife, and occupational coping self-efficacy on new graduate nurses’ burnout and mental health: A cross-sectional study. Int. J. Nurs. Stud. 2015, 52, 1080–1089. [Google Scholar] [CrossRef]
- Boland, L.L.; Mink, P.J.; Kamrud, J.W.; Jeruzal, J.N.; Stevens, A.C. Social support outside the workplace, coping styles, and burnout in a cohort of EMS providers from Minnesota. Workplace Health Saf. 2019, 67, 414–422. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.D.C.; Molero Jurado, M.D.M.; Martos Martínez, Á.; Gázquez Linares, J.J. Burnout and engagement: Personality profiles in nursing professionals. J. Clin. Med. 2019, 8, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galaiya, R.; Kinross, J.; Arulampalam, T. Factors associated with burnout syndrome in surgeons: A systematic review. Ann. R. Coll. Surg. Engl. 2020, 102, 401–407. [Google Scholar] [CrossRef]
- Kim, L.E.; Jörg, V.; Klassen, R.M. A meta-analysis of the effects of teacher personality on teacher effectiveness and burnout. Educ. Psychol. Rev. 2019, 31, 163–195. [Google Scholar] [CrossRef] [PubMed]
- McCrae, R.R.; Costa, P.T. Validation of the five-factor model of personality across instruments and observers. J. Personal. Soc. Psychol. 1987, 52, 81. [Google Scholar] [CrossRef]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. Gen. Appl. 1966, 80, 1–28. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, K.; Neff, D.M.; Pitman, S. Burnout in mental health professionals: A systematic review and meta-analysis of prevalence and determinants. Eur. Psychiatry 2018, 53, 74–99. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.F.; Kuo, C.C.; Chien, T.W.; Wang, Y.R. A meta-analysis of the effects of coping strategies on reducing nurse burnout. Appl. Nurs. Res. 2016, 31, 100–110. [Google Scholar] [CrossRef]
- Friganović, A.; Selič, P.; Ilić, B.; Sedić, B. Stress and burnout syndrome and their associations with coping and job satisfaction in critical care nurses: A literature review. Psychiatr. Danub. 2019, 31, 21–31. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Costa, B.; Pinto, I.C. Stress, burnout and coping in health professionals: A literature review. J. Psychol. Brain Stud. 2017, 14, 1–8. [Google Scholar]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; de Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Bryan, C.; Goodman, T.; Chappelle, W.; Thompson, W.; Prince, L. Occupational stressors, burnout, and predictors of suicide ideation among US Air Force remote warriors. Mil. Behav. Health 2018, 6, 3–12. [Google Scholar] [CrossRef]
- Giorgi, G.; Arcangeli, G.; Perminiene, M.; Lorini, C.; Ariza-Montes, A.; Fiz-Perez, J.; Di Fabio, A.; Mucci, N. Work-related stress in the banking sector: A review of incidence, correlated factors, and major consequences. Front. Psychol. 2017, 8, 2166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penz, M.; Stalder, T.; Miller, R.; Ludwig, V.M.; Kanthak, M.K.; Kirschbaum, C. Hair cortisol as a biological marker for burnout symptomatology. Psychoneuroendocrinology 2018, 87, 218–221. [Google Scholar] [CrossRef]
- Melamed, S.; Shirom, A.; Toker, S.; Shapira, I. Burnout and risk of type 2 diabetes: A prospective study of apparently healthy employed persons. Psychosom. Med. 2006, 68, 863–869. [Google Scholar] [CrossRef]
- Rössler, W. Stress, burnout, and job dissatisfaction in mental health workers. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Ahola, K.; Toppinen-Tanner, S.; Seppänen, J. Interventions to alleviate burnout symptoms and to support return to work among employees with burnout: Systematic review and meta-analysis. Burn. Res. 2017, 4, 1–11. [Google Scholar] [CrossRef]
- Han, S.J.; Bonn, M.A.; Cho, M. The relationship between customer incivility, restaurant frontline service employee burnout and turnover intention. Int. J. Hosp. Manag. 2016, 52, 97–106. [Google Scholar] [CrossRef]
- Metin, U.B.; Taris, T.W.; Peeters, M.C.W. Measuring procrastination at work and its associated workplace aspects. Personal. Individ. Differ. 2016, 101, 254–263. [Google Scholar] [CrossRef]
- Ugwu, L.I.; Enwereuzor, I.K.; Fimber, U.S.; Ugwu, D.I. Nurses’ burnout and counterproductive work behavior in a Nigerian sample: The moderating role of emotional intelligence. Int. J. Afr. Nurs. Sci. 2017, 7, 106–113. [Google Scholar] [CrossRef]
- Guitart, A.A. El síndrome del burnout en las empresas. In Proceedings of the Tercer Congreso de Escuelas de Psicologia de las Universidades Red Anahuac, Mérida, Mexico, 26–27 April 2007; pp. 1–7. [Google Scholar]
- Humborstad, S.I.; Humborstad, B.; Whitfield, R. Burnout and service employees’ willingness to deliver quality service. J. Hum. Resour. Hosp. Tour. 2007, 7, 45–64. [Google Scholar] [CrossRef]
- Le Blanc, P.M.; Schaufeli, W.B. Burnout interventions: An overview and illustration. In Handbook of Stress and Burnout in Health Care; Halbesleben, J.R.B., Ed.; Nova Science Publisher: Hauppauge, NY, USA, 2008; pp. 201–215. [Google Scholar]
- Schaufeli, W.B. Intervenciones sobre el síndrome de burnout. In Jornada “El Síndorme de Quemarse por el Trabajo en Servicios Sociales”; Gil-Monte, P.R., Salanova, M., Aragón, J.L., Eds.; Diputación de Valencia: Valencia, Spain, 2006; pp. 61–75. [Google Scholar]
- Grant, A.M.; Parker, S.K. Redesigning work design theories: The rise of relational and proactive perspectives. Acad. Manag. Ann. 2009, 3, 317–375. [Google Scholar] [CrossRef]
- De Simone, S.; Vargas, M.; Servillo, G. Organizational strategies to reduce physician burnout: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 883–894. [Google Scholar] [CrossRef] [PubMed]
- DeChant, P.F.; Acs, A.; Rhee, K.B.; Boulanger, T.S.; Snowdon, J.L.; Tutty, M.A.; Sinsky, C.A.; Thomas Craig, K.J. Effect of organization-directed workplace interventions on physician burnout: A systematic review. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 384–408. [Google Scholar] [CrossRef] [Green Version]
- Kossek, E.E.; Hammer, L.B.; Kelly, E.L.; Moen, P. Designing work, family & health organizational change initiatives. Organ. Dyn. 2014, 43, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildenbrand, K.; Sacramento, C.A.; Binnewies, C. Transformational leadership and burnout: The role of thriving and followers’ openness to experience. J. Occup. Health Psychol. 2018, 23, 31–43. [Google Scholar] [CrossRef] [Green Version]
- Kaya, N.; Aydin, S.; Ongun, G. The impacts of servant leadership and organizational politics on burnout: A research among mid-level managers. Int. J. Bus. Adm. 2016, 7, 26–32. [Google Scholar] [CrossRef]
- Molero, F.; Mikulincer, M.; Shaver, P.R.; Laguía, A.; Moriano, J.A. The development and validation of the leader as security provider scale. J. Work. Organ. Psychol. 2019, 35, 183–193. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Noseworthy, J.H. Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin. Proc. 2017, 92, 129–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannampallil, T.; Abraham, J.; Lou, S.S.; Payne, P.R.O. Conceptual considerations for using EHR-based activity logs to measure clinician burnout and its effects. J. Am. Med. Inform. Assoc. 2021, 28, 1032–1037. [Google Scholar] [CrossRef]
- Herrera-Sánchez, I.M.; León-Pérez, J.M.; León-Rubio, J.M. Steps to ensure a successful implementation of occupational health and safety interventions at an organizational level. Front. Psychol. 2017, 8, 2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, O.H.; Holman, D. A participative intervention to improve employee well-being in knowledge work jobs: A mixed-methods evaluation study. Work. Stress 2014, 28, 67–86. [Google Scholar] [CrossRef]
- Vargas-Cruz, L.D.; Niño-Cardozo, C.L.; Acosta-Maldonado, J.Y. Estrategias que modulan el síndrome de Burnout en enfermeros(as): Una revisión bibliográfica. Rev. Cienc. Cuid. 2017, 14, 111–131. [Google Scholar] [CrossRef] [Green Version]
- Grant, A.M. Solution-focused cognitive-behavioral coaching for sustainable high performance and circumventing stress, fatigue, and burnout. Consult. Psychol. J. Pract. Res. 2017, 69, 98. [Google Scholar] [CrossRef]
- Naczenski, L.M.; de Vries, J.D.; van Hooff, M.L.; Kompier, M.A. Systematic review of the association between physical activity and burnout. J. Occup. Health 2017, 59, 477–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochentel, O.; Humphrey, C.; Pfeifer, K. Efficacy of exercise therapy in persons with burnout. A systematic review and meta-analysis. J. Sports Sci. Med. 2018, 17, 475–484. [Google Scholar] [PubMed]
- Milanés-Sánchez, S.F.; Gómez-Díaz, M. El síndrome de burnout y la práctica de mindfulness: Una revisión sistemática. Presencia 2018, 14. [Google Scholar]
- Ravari, A.K.; Farokhzadian, J.; Nematollahi, M.; Miri, S.; Foroughameri, G. The effectiveness of a time management workshop on job stress of nurses working in emergency departments: An experimental study. J. Emerg. Nurs. 2020, 46, 548.e1–548.e11. [Google Scholar] [CrossRef]
- Bakker, A.B.; Ficapal-Cusí, P.; Torrent-Sellens, J.; Boada-Grau, J.; Hontangas-Beltrán, P.M. The Spanish version of the Job Crafting Scale. Psicothema 2018, 30, 136–142. [Google Scholar]
- Schaufeli, W.B.; Leiter, M.P.; Maslach, C.; Jackson, S.E. Maslach Burnout Inventory–General Survey. In The Maslach Burnout Inventory-Test Manual, 3rd ed.; Maslach, C., Jackson, S.E., Leiter, M.P., Eds.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Loera, B.; Converso, D.; Viotti, S. Evaluating the psychometric properties of the Maslach Burnout Inventory-Human Services Survey (MBI-HSS) among Italian nurses: How many factors must a researcher consider? PLoS ONE 2014, 9, e114987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocéréan, C.; Dupret, E.; Feltrin, M. Maslach Burnout Inventory-General Survey: French validation in a representative sample of employees. SCIREA J. Health 2019, 3, 24–61. [Google Scholar]
- Hu, Q.; Schaufeli, W.B. The factorial validity of the Maslach burnout inventory-student survey in China. Psychol. Rep. 2009, 105, 394–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibtissam, S.; Hala, S.; Sanaa, S.; Hussein, A.; Nabil, D. Burnout among Lebanese nurses: Psychometric properties of the Maslach burnout inventory-human services survey (MBI-HSS). Health 2012, 4, 644–652. [Google Scholar]
- Gil-Monte, P.R. CESQT Cuestionario para la Evaluación del Síndrome de Quemarse por el Trabajo; TEA Ediciones: Madrid, Spain, 2011. [Google Scholar]
- Bosle, A.; Gil-Monte, P.R. Psychometric properties of the spanish burnout inventory in german professionals: Preliminary results. Ansiedad Estrés 2010, 16, 283–291. [Google Scholar]
- Zawieja, P.; Guarnieri, F. Épuisement Professionnel: Principales Approches Conceptuelles, Cliniques et Psychométriques; Armand Colin: Paris, France, 2013; pp. 11–34. [Google Scholar]
- Guidetti, G.; Viotti, S.; Gil-Monte, P.R.; Converso, D. Feeling guilty or not guilty. Identifying burnout profiles among Italian teachers. Curr. Psychol. 2018, 37, 769–780. [Google Scholar] [CrossRef]
- Figueiredo-Ferraz, H.; Gil-Monte, P.R.; Queirós, C.; Passos, F. Validacao fatorial do “Spanish Burnout Inventory” em policiais portugueses. Psicol. Reflexão Crítica 2014, 27, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Misiołek, A.; Gorczyca, P.; Misiołek, H.; Gierlotka, Z. The prevalence of burnout syndrome in Polish anaesthesiologists. Anaesthesiol. Intensive Ther. 2014, 46, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Lambert, E.G.; Hogan, N.L.; Griffin, M.L.; Kelley, T. The correctional staff burnout literature. Crim. Justice Stud. 2015, 28, 397–443. [Google Scholar] [CrossRef]
- Milićević-Kalašić, A. Burnout examination. In Burnout for Experts; Bährer-Kohler, S., Ed.; Springer: Boston, MA, USA, 2013; pp. 169–183. [Google Scholar]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work. Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Vardakou, I.; Kantas, A. The convergent validity of two burnout instruments. Eur. J. Psychol. Assess. 2003, 19, 12–23. [Google Scholar] [CrossRef]
- Montero-Marín, J.; García-Campayo, J. A newer and broarder definition of burnout: Validation of the “Burnout Clinical Subtype Quetionnaire (BCSQ-36). BMC Public Health 2010, 10, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero-Marín, J.; Skapinakis, P.; Araya, R.; Gili, M.; García Campayo, J. Towards a brief definition of burnout síndrome by subtypes: Development of the “Burnout Clinical Subtypes Questionnaire (BCSQ-12). Health Qual. Live Outcomes 2011, 9, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abeltina, M.; Stokenberga, L.; Skudra, J.; Rascevska, M.; Kolesovs, A. Burnout Clinical Subtypes Questionnaire (BCSQ-36): Reliability and validity study in Latvia. Psychol. Health Med. 2020, 25, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bauernhofer, K.; Tanzer, N.; Paechter, M.; Papousek, I.; Fink, A.; Weiss, E.M. Frenetic, underchallenged, and worn-out: Validation of the German “Burnout Clinical Subtypes Questionnaire”—Student survey and exploration of three burnout risk groups in university students. Front. Educ. 2019, 4, 1–19. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout Assessment Tool (BAT)-development, validity, and reliability. Int. J. Environ. Res. Public Health 2020, 17, 9495. [Google Scholar] [CrossRef]
- Melamed, S.; Kushnir, T.; Shirom, A. Burnout and risk factors for cardiovascular diseases. Behav. Med. 1992, 18, 53–60. [Google Scholar] [CrossRef]
- Shirom, A.; Melamed, S. A comparison of the construct validity of two burnout measures in two groups of professionals. Int. J. Stress Manag. 2006, 13, 176–200. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero Jurado, M.M.; Martos Martínez, A.; Gázquez Linares, J.J. New burnout evaluation model based on the Brief Burnout Questionnaire: Psychometric properties for nursing. Int. J. Environ. Res. Public Health 2018, 15, 2718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Jimenez, B.; Barbaranelli, C.; Galvez Herrer, M.; Garrosa Hernández, E. The Physician Burnout Questionnaire: A new definition and measure. TPM Test. Psychom. Methodol. Appl. Psychol. 2012, 19, 325–344. [Google Scholar] [CrossRef]
- Friedman, I. Teacher Burnout: The Concept and Its Measurement; Henrietta Szold Institute: Jerusalem, Israel, 1999. [Google Scholar]
- Ackerley, G.D.; Burnell, J.; Holder, D.C.; Kurdek, L.A. Burnout among licensed psychologists. Prof. Psychol. Res. Pract. 1988, 19, 624–631. [Google Scholar] [CrossRef]
- Rupert, P.A.; Stevanovic, P.; Hunley, H.A. Work-family conflict and burnout among practicing psychologists. Prof. Psychol. Res. Pract. 2009, 40, 54–61. [Google Scholar] [CrossRef]
- Raedeke, T.D.; Smith, A.L. Development and preliminary validation of an athlete burnout measure. J. Sport Exerc. Psychol. 2001, 23, 281–306. [Google Scholar] [CrossRef]
- Raedeke, T.D.; Smith, A.L. The Athlete Burnout Questionnaire Manual; Fitness Information Technology: Morgantown, WV, USA, 2009. [Google Scholar]
- Salmela-Aro, K.; Kiuru, N.; Leskinen, E.; Nurmi, J.E. School burnout inventory (SBI) reliability and validity. Eur. J. Psychol. Assess. 2009, 25, 48–57. [Google Scholar] [CrossRef]
- Roskam, I.; Raes, M.E.; Mikolajczak, M. Exhausted parents: Development and preliminary validation of the parental burnout inventory. Front. Psychol. 2017, 8, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirom, A. Reflections on the study of burnout. Work. Stress 2005, 19, 263–270. [Google Scholar] [CrossRef]
- Dias Campos, F.; Chambel, M.J.; Lopes, S.; Dias, P.C. Post-traumatic stress disorder in the Military Police of Rio de Janeiro: Can a risk profile be identified? Int. J. Environ. Res. Public Health 2021, 18, 2594. [Google Scholar] [CrossRef]
- Lee, S.-J.; Jung, S.I.; Kim, M.-G.; Park, E.; Kim, A.-R.; Kim, C.H.; Hwang, J.-M.; Jung, T.-D. The influencing factors of gender differences on mental burdens in young physiotherapists and occupational therapist. Int. J. Environ. Res. Public Health 2021, 18, 2858. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.-Y.; Lee, B.; Kwon, O.-J.; Kim, M.-S.; Sim, K.-L.; Choi, Y.-H. Emotional labor, burnout, medical error, and turnover intention among South Korean nursing staff in a University Hospital setting. Int. J. Environ. Res. Public Health 2021, 18, 10111. [Google Scholar] [CrossRef]
- Chatani, Y.; Nomura, K.; Hiraike, H.; Tsuchiya, A.; Okinaga, H. Multiple physical symptoms are useful to identify high risk individuals for burnout: A study on faculties and hospital workers in Japan. Int. J. Environ. Res. Public Health 2021, 18, 3246. [Google Scholar] [CrossRef] [PubMed]
- Sarabia-Cobo, C.; Pérez, V.; de Lorena, P.; Fernández-Rodríguez, Á.; González-López, J.R.; González-Vaca, J. Burnout, compassion fatigue and psychological flexibility among geriatric nurses: A multicenter study in Spain. Int. J. Environ. Res. Public Health 2021, 18, 7560. [Google Scholar] [CrossRef]
- Gago-Valiente, F.-J.; Mendoza-Sierra, M.-I.; Moreno-Sánchez, E.; Arbinaga, F.; Segura-Camacho, A. Emotional exhaustion, depersonalization, and mental health in nurses from Huelva: A cross-cutting study during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7860. [Google Scholar] [CrossRef]
- Drüge, M.; Schladitz, S.; Wirtz, M.A.; Schleider, K. Psychosocial burden and strains of pedagogues—Using the Job Demands-Resources Theory to predict burnout, job satisfaction, general state of health, and life satisfaction. Int. J. Environ. Res. Public Health 2021, 18, 7921. [Google Scholar] [CrossRef]
- Pérez-Luño, A.; Díez Piñol, M.; Dolan, S.L. Exploring high vs. low burnout amongst public sector wducators: COVID-19 antecedents and profiles. Int. J. Environ. Res. Public Health 2022, 19, 780. [Google Scholar] [CrossRef]
- Sequera-Martín, M.; Ramos-Fuentes, M.I.; Garrido-Ardila, E.M.; Sánchez-Sánchez, C.; de la Torre-Risquez, A.; Rodríguez-Mansilla, J. Prevalence of burnout syndrome and job satisfaction in music therapists in Spain: A cross-sectional, descriptive study. Int. J. Environ. Res. Public Health 2021, 18, 9108. [Google Scholar] [CrossRef]
- Bebiroglu, N.; Bayot, M.; Brion, B.; Denis, L.; Pirsoul, T.; Roskam, I.; Mikolajczak, M. An instrument to operationalize the balance between risks and resources and predict job burnout. Int. J. Environ. Res. Public Health 2021, 18, 9416. [Google Scholar] [CrossRef] [PubMed]
- Sandoval-Reyes, J.; Restrepo-Castro, J.C.; Duque-Oliva, J. Work intensification and psychological detachment: The mediating role of job resources in health service workers. Int. J. Environ. Res. Public Health 2021, 18, 12228. [Google Scholar] [CrossRef]
- Leclercq, C.; Braeckman, L.; Firket, P.; Babic, A.; Hansez, I. Interest of a joint use of two diagnostic tools of burnout: Comparison between the Oldenburg Burnout Inventory and the Early Detection Tool of Burnout Completed by Physicians. Int. J. Environ. Res. Public Health 2021, 18, 10544. [Google Scholar] [CrossRef] [PubMed]
- Kerkamm, F.; Dengler, D.; Eichler, M.; Materzok-Köppen, D.; Belz, L.; Neumann, F.A.; Zyriax, B.C.; Harth, V.; Oldenburg, M. Measurement methods of fatigue, sleepiness, and sleep behaviour aboard ships: A systematic review. J. Environ. Res. Public Health 2022, 19, 120. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Trousselard, M.; Pereira, B.; Schmidt, J.; Clinchamps, M.; Thivel, D.; Ugbolue, U.C.; Moustafa, F.; Occelli, C.; Vallet, G.; et al. Protocol of the Study on Emergency Health Care Workers’ Responses evaluated by Karasek Questionnaire: The SEEK-Study Protocol. Int. J. Environ. Res. Public Health 2021, 18, 4068. [Google Scholar] [CrossRef]
- Mérida-López, S.; Extremera, N.; Chambel, M.J. Linking self- and other-focused emotion regulation abilities and occupational commitment among pre-service teachers: Testing the mediating role of study engagement. Int. J. Environ. Res. Public Health 2021, 18, 5434. [Google Scholar] [CrossRef] [PubMed]
- Siu, O.-L.; Kong, Q.; Ng, T.-K. Psychological capital and family satisfaction among employees: Do occupational stressors moderate the relationship? Int. J. Environ. Res. Public Health 2021, 18, 12260. [Google Scholar] [CrossRef] [PubMed]
- Latorre, F.; Pérez-Nebra, A.R.; Queiroga, F.; Alcover, C.-M. How do teleworkers and organizations manage the COVID-19 crisis in Brazil? The role of flexibility i-Deals and work recovery in maintaining sustainable well-being at work. Int. J. Environ. Res. Public Health 2021, 18, 12522. [Google Scholar] [CrossRef]
- Lee, H.; An, S.; Lim, G.Y.; Sohn, Y.W. Ethical leadership and followers’ emotional exhaustion: Exploring the roles of three types of emotional labor toward leaders in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 10862. [Google Scholar] [CrossRef] [PubMed]
- van Dick, R.; Cordes, B.L.; Lemoine, J.E.; Steffens, N.K.; Haslam, S.A.; Akfirat, S.A.; Ballada, C.J.A.; Bazarov, T.; Aruta, J.J.B.R.; Avanzi, L.; et al. Identity leadership, employee burnout and the mediating role of team identification: Evidence from the Global Identity Leadership Development Project. Int. J. Environ. Res. Public Health 2021, 18, 12081. [Google Scholar] [CrossRef]
- Moriano, J.A.; Molero, F.; Laguía, A.; Mikulincer, M.; Shaver, P.R. Security Providing Leadership: A Job Resource to Prevent Employees’ Burnout. Int. J. Environ. Res. Public Health 2021, 18, 12551. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. A model of burnout and life satisfaction amongst nurses. J. Adv. Nurs. 2000, 32, 454–464. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimension | Definition |
|---|---|
| Emotional exhaustion | This dimension manifests in the form of feelings and sensation of being exhausted by the psychological efforts made at work. It is also described in terms of weariness, tiredness, fatigue, weakening, and the subjects who manifest this type of feelings show difficulties in adapting to the work environment since they lack sufficient emotional energy to cope with work tasks. |
| Cynicism or depersonalization | This dimension, the interpersonal component of burnout, is defined as a response of detachment, indifference and unconcern towards the work being performed and/or the people who receive it. It translates into negative or inappropriate attitudes and behaviors, irritability, loss of idealism, and interpersonal avoidance usually towards service users, patients, and/or clients. |
| Reduced personal achievement | This dimension is reflected in a negative professional self-evaluation and doubts about the ability to perform the job effectively, as well as a greater tendency to evaluate results negatively. It also translates into a decrease in productivity and capabilities, low morale, as well as lower coping skills. |
| Job Demands | Job Resources |
|---|---|
| Temporary pressure Interpersonal conflicts with clients and colleagues Task complexity Job insecurity Unfavorable schedule changes Qualitative and quantitative work overload Personal occupational hazards | Individual Technical knowledge and skills Socio-emotional skills Positive psychological capital (self-efficacy, optimism, hope and resilience) Creativity Organizational Time flexibility Job security Supervisor and peer support Material resources Autonomy Rewards |
| Protectors of Burnout | Enhancers of Burnout |
|---|---|
| Agreeableness Conscientiousness Extraversion Openness to experience Positive psychological capital Problem-focused coping | Neuroticism External locus of control Type A Personality Alexithymia Emotion-focused coping |
| Promoted by the Organization | Promoted by the Worker | ||
|---|---|---|---|
| Aimed at the Structure | Aimed at Employees | Aimed at Oneself | Aimed at Aspects of the Job |
| Improvement of contents and workstations | Training | Physical exercise | Time management |
| Humanization of work schedules and implementation of work–life balance plans | Strengths-based interventions | Mindfulness training | Job crafting |
| Managers’ leadership development | Coaching and guidance | Self-assessment | |
| Use of non-financial rewards and incentives | Creation of support groups | Psychotherapy | |
| Development of welcome programs | |||
| Burnout monitoring and design of tailor-made plans | |||
| Institutionalization of the Occupational Health and Safety Service | |||
| Actions |
|---|
| Self-regulation and emotional management Development of other personal resources, such as resilience, self-efficacy, hope, and optimism Conflict management Work stress management Time management Job-specific technical skills Problem solving Teamwork |
| 1. Identification of Competencies | 2. Strengths Development | 3. Utilization of Strengths |
|---|---|---|
| They usually result in a list of the most relevant strengths. Performance appraisals and other tools such as questionnaires and strengths scales can be used for this purpose. | Organizations often set up training workshops and individual development programs in which individuals are encouraged to cultivate and refine their strengths by developing a concrete action plan. | An attempt is made to match the types of tasks to be performed with the strengths of the employees. |
| 1. Increasing Structural Job Resources | 2. Decreasing Job Demands | 3. Increasing the Social Resources of Employment | 4. Increased Demand for Challenges at Work |
| Doing what is possible to develop professional skills and learn new things on the job. | Organizing work in such a way that it does not cause too much stress, is mentally less intense, as well as avoiding emotionally complicated situations with customers and colleagues and trying not to make difficult decisions at work. | Asking, if necessary, for help and feedback about the job from the supervisor and co-workers. | When an interesting project comes up, proactively offer to work on it, when there is little to do, offer help to co-workers and ask for more responsibility from the supervisor. |
| Generic Instruments | Specific Instruments |
| Maslach Burnout Inventory (MBI) Questionnaire for the Evaluation of Burnout Syndrome at Work (CESQT) Copenhagen Burnout Inventory (CBI) Oldenburg Burnout Inventory Burnout Clinical Subtypes Questionnaire (BCSQ-36/12) Burnout Assessment Tool (BAT) Shirom–Melamed Burnout Questionnaire (SMBQ) | Maslach Burnout Inventory-Human Services Survey (MBI-HSS) Brief Burnout Questionnaire Revised for nursing staff Physician Burnout Questionnaire Teacher Burnout Questionnaire Psychologist’s Burnout Inventory Burnout Questionnaire for Athletes School Burnout Inventory Parental Burnout Inventory |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edú-Valsania, S.; Laguía, A.; Moriano, J.A. Burnout: A Review of Theory and Measurement. Int. J. Environ. Res. Public Health 2022, 19, 1780. https://doi.org/10.3390/ijerph19031780
Edú-Valsania S, Laguía A, Moriano JA. Burnout: A Review of Theory and Measurement. International Journal of Environmental Research and Public Health. 2022; 19(3):1780. https://doi.org/10.3390/ijerph19031780
Chicago/Turabian StyleEdú-Valsania, Sergio, Ana Laguía, and Juan A. Moriano. 2022. "Burnout: A Review of Theory and Measurement" International Journal of Environmental Research and Public Health 19, no. 3: 1780. https://doi.org/10.3390/ijerph19031780
APA StyleEdú-Valsania, S., Laguía, A., & Moriano, J. A. (2022). Burnout: A Review of Theory and Measurement. International Journal of Environmental Research and Public Health, 19(3), 1780. https://doi.org/10.3390/ijerph19031780