
A Comparative Cross-Sectional Study Assessing the Psycho-Emotional State of Intensive Care Units’ Physicians and Nurses of COVID-19 Hospitals of a Russian Metropolis

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Research Conditions and Respondents
2.3. Questionnaire Composition
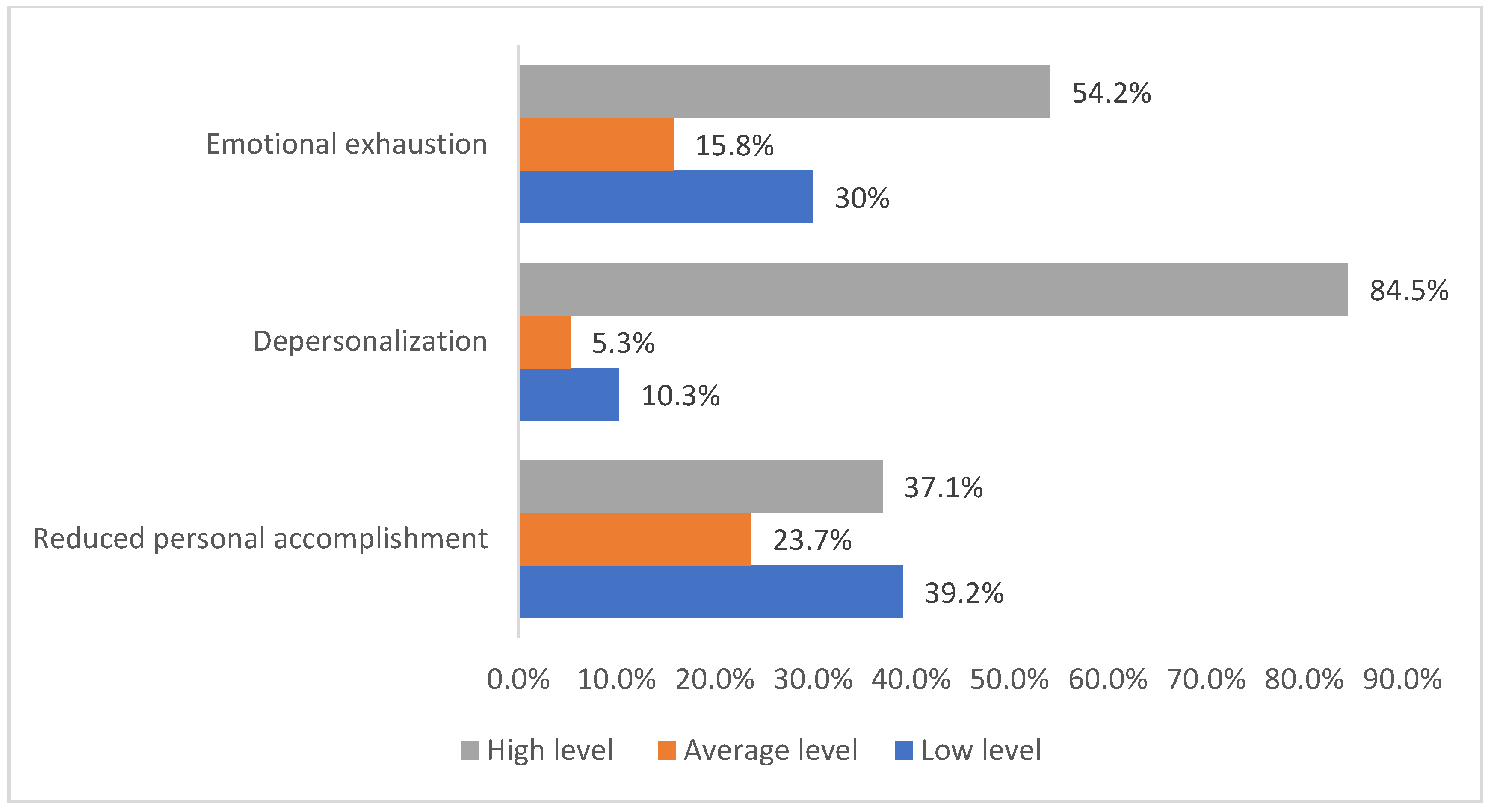
- Emotional exhaustion, which is expressed by a loss of interest in others, life dissatisfaction, etc. The value ranges from 0 to 54 (max.). Low level (0 to 15), average level (16 to 24), and high level (25 and higher). The scale contains 9 questions (Cronbach’s α = 0.896);
- Depersonalization: the formality of performing occupational duties, lack of personal involvement and empathy, indifference, and emotional detachment. The value ranges from 0 to 30 (max.). Low level (0 to 5), average level (5 to 10), and high level (11 and higher). The scale contains 5 questions (Cronbach’s α = 0.896);
- Reduced personal accomplishment is expressed by a decrease in work motivation, an increase in negativity toward official duties, etc. The value ranges are from 0 to 48, where 48 is the maximum level of occupational success, and 0 is the maximum level of reduced personal accomplishment. Low level (37 and higher), average level (31 to 36), and high level (0 to 30). The scale contains 5 questions (Cronbach’s α = 0.896).
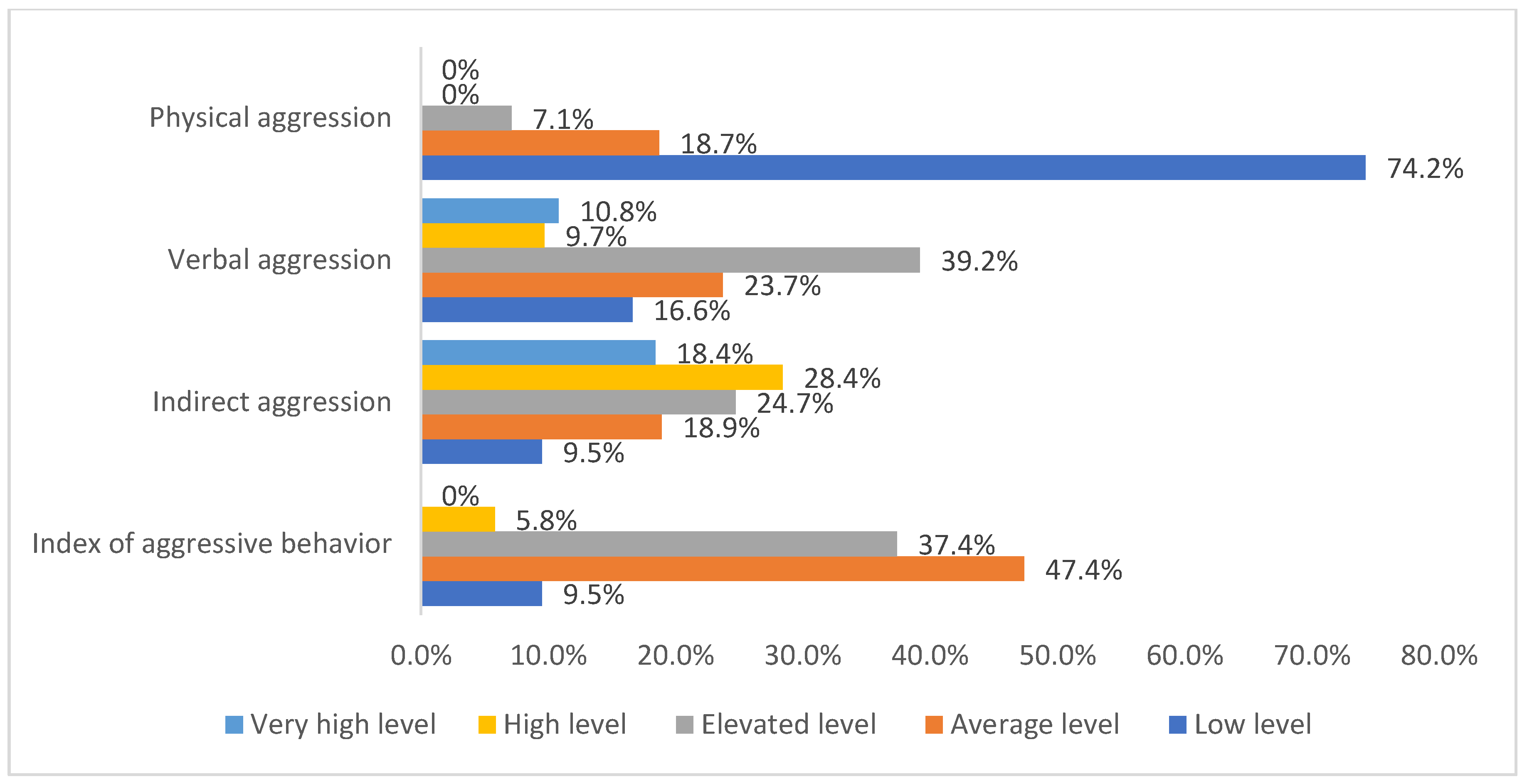
- Physical aggression is behavior causing or threatening physical harm toward others. The value ranges from 0 to 100 (max.). Low level (0 to 30), average level (31 to 52), advanced level (53 to 74), high level (75 to 85), and extremely high level (86 and higher). The scale contains 7 forward and 3 backward questions (Cronbach’s α = 0.422). Examples of statements: “I never get annoyed enough to throw things around” and “Anyone who insults me and my family asks for a fight”;
- Verbal aggression (quarrels, threats, etc.). The value ranges from 0 to 104 (max.). Low level (0 to 30), average level (31 to 52), advanced level (53 to 74), high level (75 to 85), and extremely high level (86 and higher). The scale contains 9 forward and 4 backward questions (Cronbach’s α = 0.648). Examples of statements: “If I disapprove of my friends’ behavior, I let them feel it” and “When they shout at me, I start shouting back”;
- Indirect aggression (directed indirectly toward others): gossip, hitting objects, shouting, or stamping your feet in a fit of rage. The value ranges from 0 to 99 (max.). Low level (0 to 14), average level (15 to 36), advanced level (37 to 58), high level (59 to 69), and extremely high level (70 and higher). The scale contains 6 forward and 3 backward questions (Cronbach’s α = 0.665). Examples of statements: “I am never gloomy with anger” and “When I get annoyed, I slam doors”.
- Physical aggression, indirect aggression, and verbal aggression together form a total index of aggressive behavior. The value ranges from 0 to 101.
- Contingency tables (Pearson’s χ2 Test) were used to analyze the joint frequency distributions and assess their statistical reliability.
- Mann–Whitney U-criterion was used to assess the differences between two independent samples of respondents (HCWs) in COVID-19 and non-COVID-19 ICUs regarding the level of aggressive behavior, components of occupational burnout, and occupational stress.
- Correlation analysis of connections (Ro–Spearman) was used to study the connections between the studied signs.
- Multiple linear regression analysis was used to assess the size of the contribution of predictors to changes in the variance of dependent variables.
- The Kruskal–Wallace H-test was used to assess the differences between several independent samples of physicians and nurses with different employment experiences.
- Cluster analysis (k-means clustering) was used to determine the levels of occupational burnout in the sample.
3. Results
- (1)
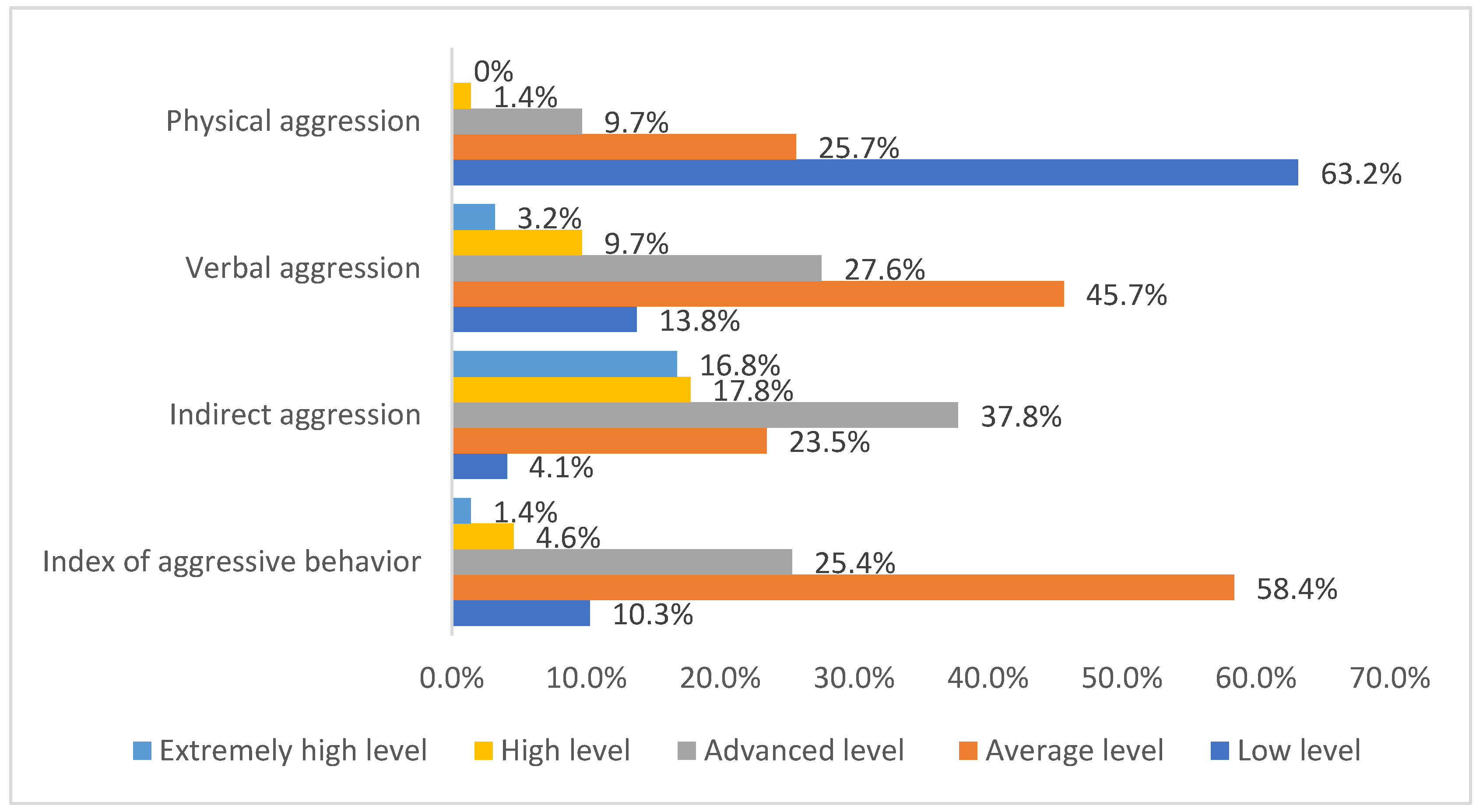
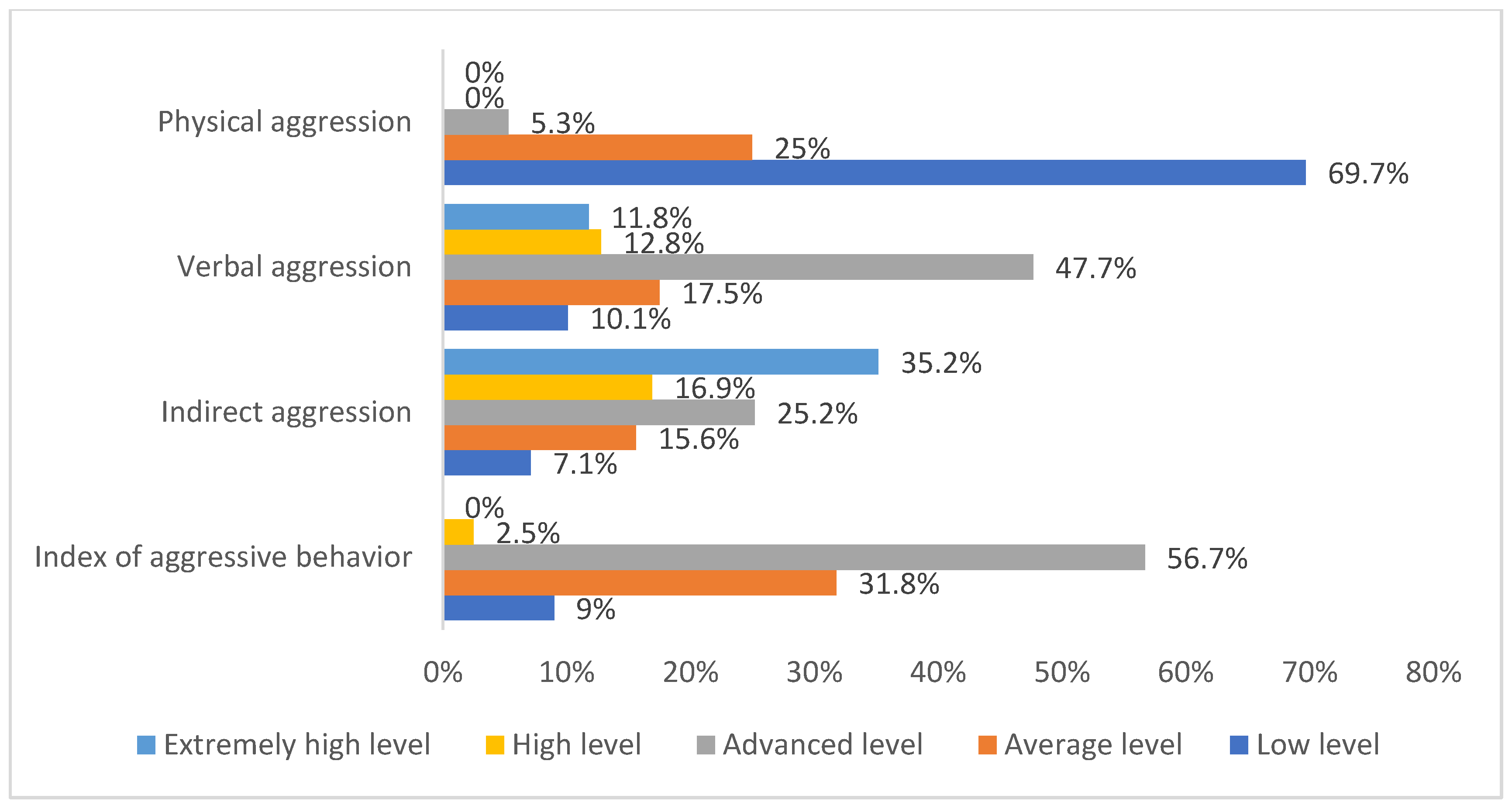
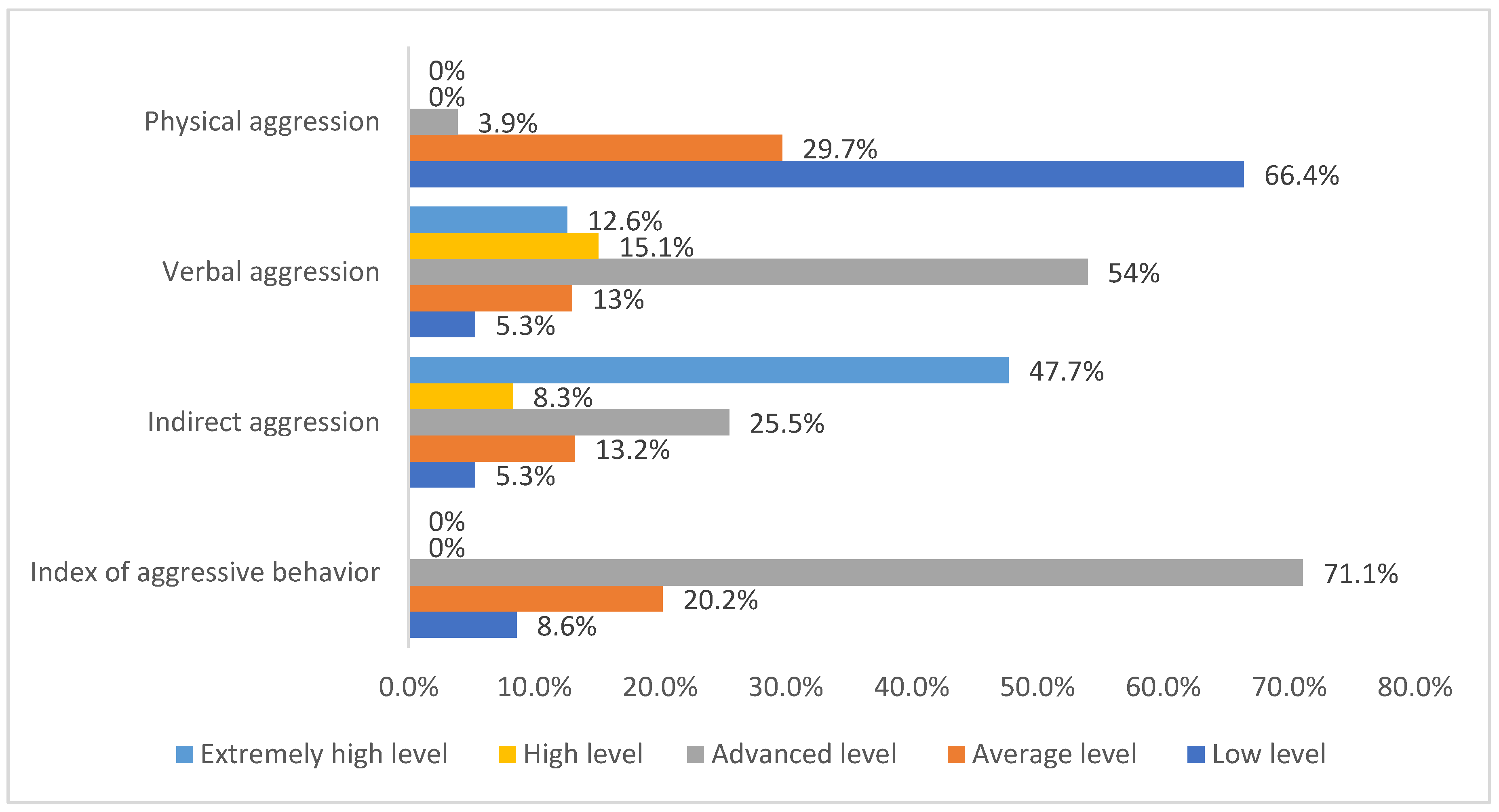
- Significant differences were found in the level of aggressive behavior of COVID-19 ICUs HCWs (χ2 = 77.059; p = 0.000). The analysis showed that in non-COVID-19 ICUs, the number of HCWs with an average level of aggressive behavior was higher than expected, and the number of HCWs with an advanced level of aggressive behavior was lower than expected. In non-COVID-19 ICUs, the number of HCWs with an advanced level of aggressive behavior was higher than expected, and the number of HCWs with an average level of aggressive behavior was lower than expected. The number of HCWs with other levels of aggressive behavior in non-COVID-19 ICUs was almost non-existent. Not as expected, non-COVID-19 ICUs had more HCWs with an average level of aggressive behavior, and COVID-19 ICUs had more HCWs with an advanced level of aggressive behavior. Therefore, HCWs in non-COVID-19 ICU HCWs had an average level of aggressive behavior, while COVID-19 ICU HCWs had an advanced level of aggressive behavior.
- (2)
- Significant differences were found in the level of physical aggression of HCWs in COVID-19 ICUs (χ2 = 9.843; p = 0.020). The analysis showed that in non-COVID-ICUs, the number of HCWs with a low level of physical aggression was lower than expected, and the number of HCWs with an advanced level of physical aggression was higher than expected. In COVID-19 ICUs, the number of HCWs with high levels of physical aggression was lower than expected, and the number of HCWs with low levels of physical aggression was higher than expected. Additionally, the number of HCWs with other levels of physical aggression in the COVID-19 and non-COVID-19 ICUs was the same as expected, and HCWs with an extremely high level of aggression were not found in the sample. Thus, HCWs in non-COVID-19 ICUs had an advanced level of physical aggression, and HCWs in COVID-19 ICUs had a low level of physical aggression. Both COVID-19 and non-COVID-19 ICUs had a larger number of HCWs with a low level of aggressive behavior, but in COVID-19 ICUs, this percentage was higher (70%). In non-COVID-19 ICUs, there was a larger percentage of HCWs with other levels of aggressive behavior.
- (3)
- Significant differences were found in the level of verbal aggression of the HCWs of COVID-19 ICUs (χ2 = 82.676; p = 0.000). The analysis showed that in non-COVID-19 ICUs, the number of HCWs with low and average levels of verbal aggression was higher than expected, and the number of HCWs with advanced, high, and extremely high levels of verbal aggression was lower than expected. In COVID-19 ICUs, the number of HCWs with low and average levels of verbal aggression was lower than expected, and the number of HCWs with advanced, high, and extremely high levels of verbal aggression was higher than expected. Therefore, non-COVID-19 ICU HCWs had a low and average level of verbal aggression, while COVID-19 ICU HCWs had an advanced, high, and extremely high level of verbal aggression. Non-COVID-19 ICUs had a higher number of HCWs with an average level of verbal aggression, and COVID-19 ICUs had a higher number of HCWs with an advanced level of verbal aggression.
- (4)
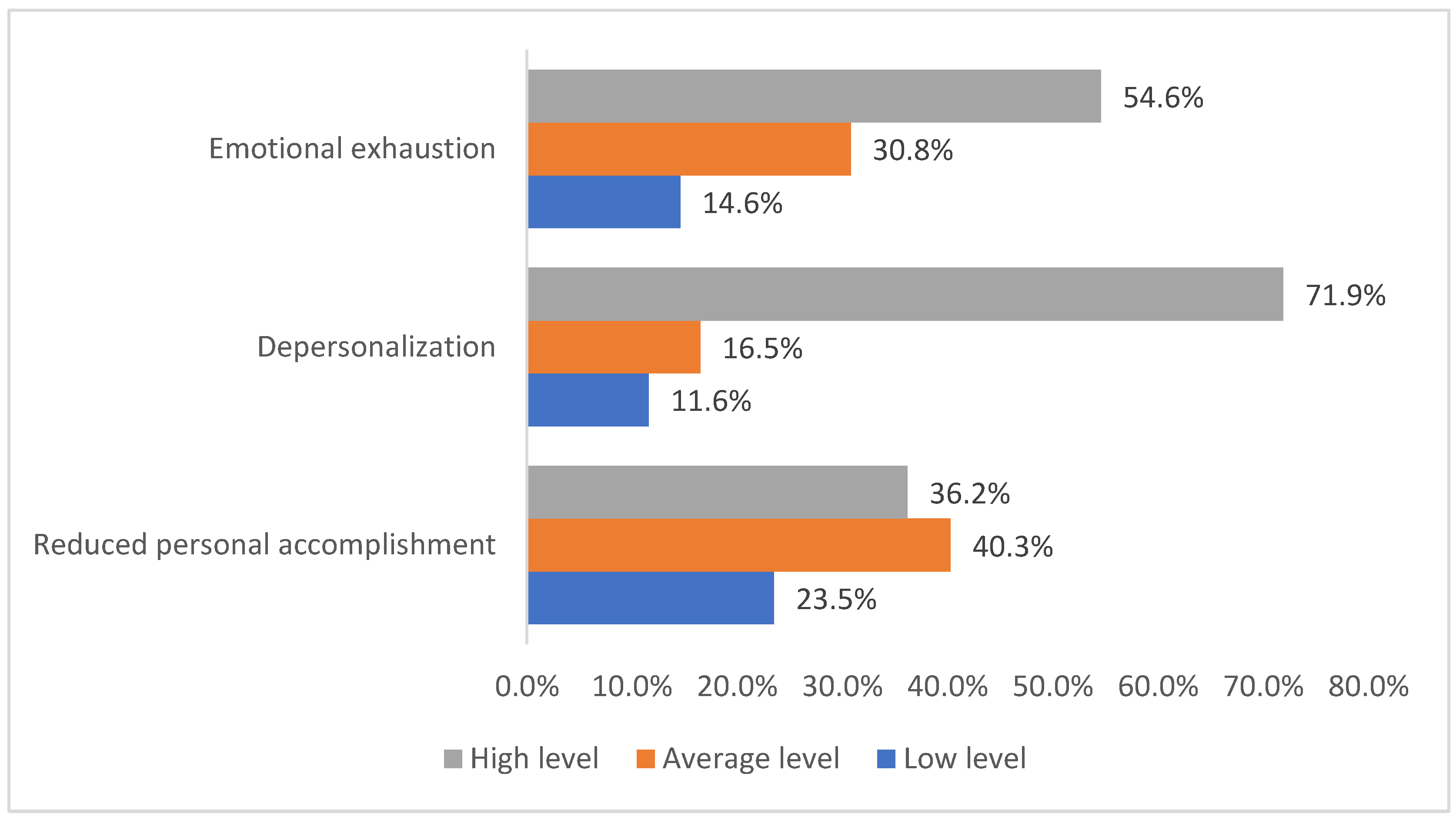
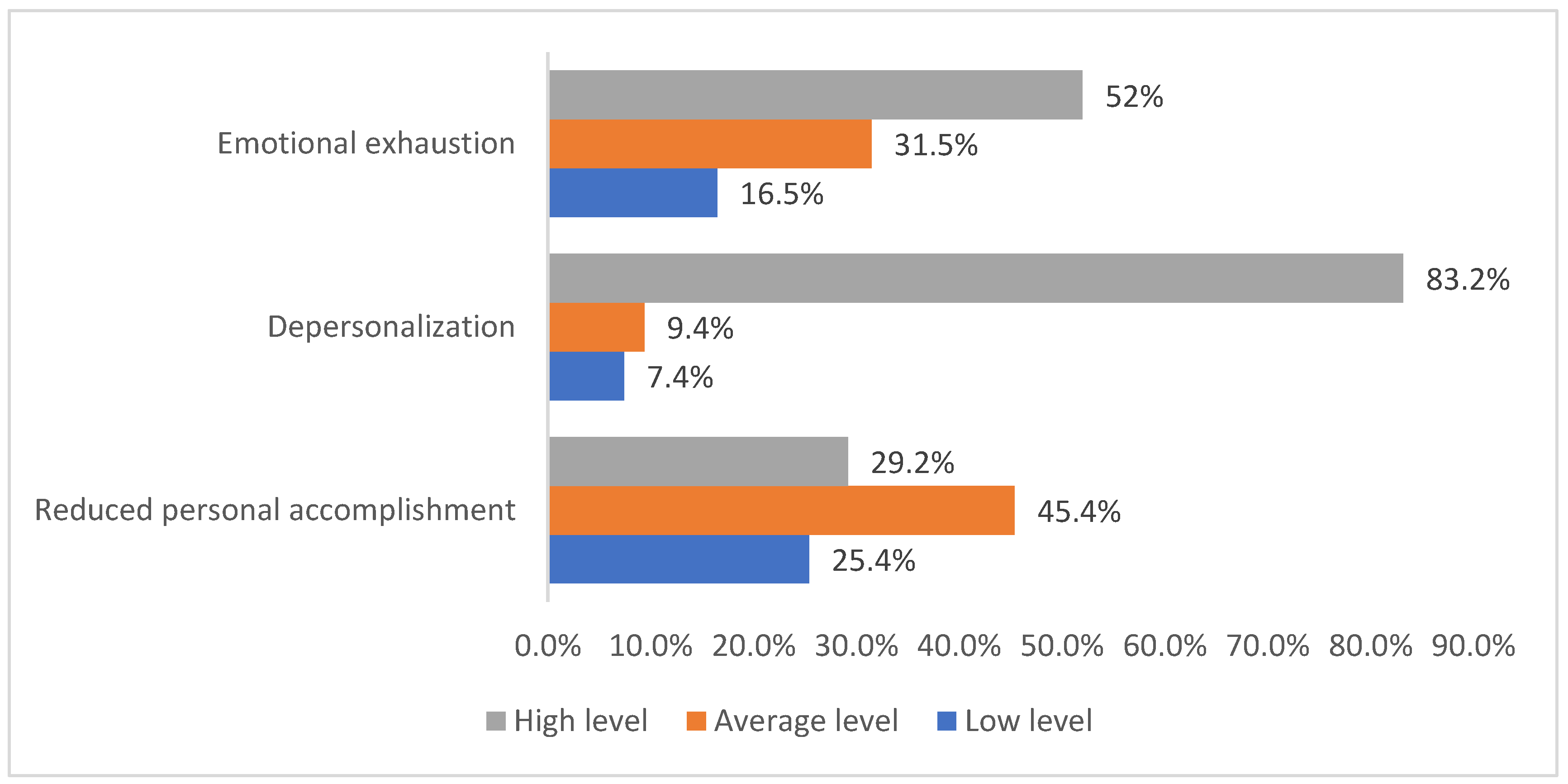
- Significant differences were found in the level of depersonalization of HCWs in COVID-19 ICUs (χ2 = 12.410; p = 0.002). The analysis showed that in non-COVID-19 ICUs, the number of HCWs with low and average levels of depersonalization was higher than expected, and the number of HCWs with high levels of depersonalization was lower than expected. In COVID-19 ICUs, the number of HCWs with low and average levels of depersonalization was lower than expected, and the number of HCWs with high levels of depersonalization was higher than expected. Therefore, HCWs in non-COVID-ICUs had a low and average level of depersonalization, and HCWs in COVID-19 ICUs had a high level of depersonalization. COVID-19 and non-COVID-19 ICUs had a larger number of HCWs with a high level of depersonalization, but in COVID-19 ICUs, this percentage was higher (61.6%), as well as the percentage of HCWs with an average level of depersonalization (30.5%). In non-COVID-19 ICUs, there was a higher percentage of HCWs with a low level of depersonalization (17%).
- (5)
- No differences were found in the level of reduced personal accomplishment, emotional exhaustion, and occupational stress. In the analysis of indirect aggression, the same results were obtained as in the use of Mann–Whitney U-criterion (Table 2).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosted, E.; Thomsen, T.G.; Krogsgaard, M.; Busk, H.; Geisler, A.; Hansen, T.S.; Kjerholt, M.; Mortensen, C.B.; Thomsen, T.H.; Beck, M.; et al. On the frontline treating COVID-19: A pendulum experience-from meaningful to overwhelming-for Danish healthcare professionals. J. Clin. Nurs. 2021, 30, 3448–3455. [Google Scholar] [CrossRef]
- El-Hage, W.; Hingray, C.; Lemogne, C.; Yrondi, A.; Brunault, P.; Bienvenu, T.; Etain, B.; Paquet, C.; Gohier, B.; Bennabi, D.; et al. Les professionnels de santé face à la pandémie de la maladie à coronavirus (COVID-19): Quels risques pour leur santé mentale? [Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks?]. Encephale 2020, 46, S73–S80. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, E.M.; Martino, M.M.F.; França, S.P.S. Burnout and depressive symptoms in intensive care nurses: Relationship analysis. Rev. Bras. Enferm. 2018, 71, 135–141. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 14 September 2021).
- van Mol, M.M.; Kompanje, E.J.; Benoit, D.D.; Bakker, J.; Nijkamp, M.D. The Prevalence of Compassion Fatigue and Burnout among Healthcare Professionals in Intensive Care Units: A Systematic Review. PLoS ONE 2015, 10, e0136955. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, C.; Ribeiro, O.; Fonseca, A.M.; Carvalho, A.S. Burnout in intensive care units-a consideration of the possible prevalence and frequency of new risk factors: A descriptive correlational multicentre study. BMC Anesthesiol. 2013, 13, 38. [Google Scholar] [CrossRef] [Green Version]
- Jain, V.; Yuan, J.M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 65, 533–546. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.B.; Lockhart, S.; Reed, K.; Griesmer, C.; Glasgow, R.E.; Moss, M.; Douglas, I.S.; Morris, M.A. Drivers of Burnout Among Critical Care Providers: A Multi-Center Mixed Methods Study. Chest 2021, 8, S0012–S3692. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, H.; Xie, J.; Zhang, J.; Li, H.; Liu, S.; Li, Q.; Yang, Y.; Huang, Y. Burnout in ICU doctors and nurses in mainland China-A national cross-sectional study. J. Crit. Care 2021, 62, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Vodopyanova, N.E.; Starchenkova, E.S.; Nasledov, A.D.; Petrova, T.N. Standardized questionnaire “Professional burnout” for specialists of socioeconomic professions. Bulletin of St. Petersburg University. Sociology 2013, 4, 17–27. (In Russian) [Google Scholar]
- Chvan, A.A.; Zaytceva, U.A.; Kuznecova, U.A. Standardized Questionnaire for Measuring Aggressive and Hostile Reactions; Bass, A., Darki, A., Eds.; Psychological diagnosis; KRIPKiPRO: Kemerovo, Russia, 2008; p. 68. (In Russian) [Google Scholar]
- Weissman, Arlene Nancy, “The Dysfunctional Attitude Scale: A Validation Study” (1979). Publicly Accessible Penn Dissertations. 1182. Available online: https://repository.upenn.edu/edissertations/1182 (accessed on 14 September 2021).
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef] [PubMed]
- Amin, F.; Sharif, S.; Saeed, R.; Durrani, N.; Jilani, D. COVID-19 pandemic- knowledge, perception, anxiety and depression among frontline doctors of Pakistan. BMC Psychiatry 2020, 20, 459. [Google Scholar] [CrossRef] [PubMed]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- Guirardello, E.B. Impact of critical care environment on burnout, perceived quality of care and safety attitude of the nursing team. Rev. Lat Am. Enfermagem. 2017, 25, e2884. [Google Scholar] [CrossRef]
- Vasconcelos, E.M.; Martino, M.M.F. Predictors of burnout syndrome in intensive care nurses. Rev Gauch. Enferm. 2018, 38, e65354. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of Burnout Among Physicians: A Systematic Review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef] [Green Version]
- Galehdar, N.; Kamran, A.; Toulabi, T.; Heydari, H. Exploring nurses’ experiences of psychological distress during care of patients with COVID-19: A qualitative study. BMC Psychiatry 2020, 20, 489. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, F.T.; Leão, B.A.; Tavares, G.M.; Santos, J.G. Burnout syndrome and weekly workload of on-call physicians: Cross-sectional study. Sao Paulo Med. J. 2012, 130, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Prada, M.; González-Cabrera, J.; Iribar-Ibabe, C.; Peinado, J.M. Riesgos psicosociales y estrés como predictores del burnout en médicos internos residentes en el Servicio de Urgencias [Psychosocial risks and stress as predictors of burnout in junior doctors performing emergency guards]. Gac. Med. Mex. 2017, 153, 450–458. (In Spanish) [Google Scholar] [CrossRef]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to Sars-Cov-2 (Covid-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef] [PubMed]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Testoni, I.; Franco, C.; Gallo Stampino, E.; Iacona, E.; Crupi, R.; Pagano, C. Facing COVID-19 Between Sensory and Psychoemotional Stress, and Instrumental Deprivation: A Qualitative Study of Unmanageable Critical Incidents with Doctors and Nurses in Two Hospitals in Northern Italy. Front. Psychol. 2021, 12, 622894. [Google Scholar] [CrossRef] [PubMed]
- Raudenská, J.; Steinerová, V.; Javůrková, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]
- Abdelhafiz, A.S.; Ali, A.; Ziady, H.H.; Maaly, A.M.; Alorabi, M.; Sultan, E.A. Prevalence, Associated Factors, and Consequences of Burnout Among Egyptian Physicians During COVID-19 Pandemic. Front. Public Health 2020, 8, 590190. [Google Scholar] [CrossRef]
- Lasalvia, A.; Amaddeo, F.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Bonetto, C. Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: A cross-sectional study in a tertiary hospital of a highly burdened area of north-east Italy. BMJ Open 2021, 11, e045127. [Google Scholar] [CrossRef]
- Vincent-Höper, S.; Stein, M.; Nienhaus, A.; Schablon, A. Workplace Aggression and Burnout in Nursing—The Moderating Role of Follow-Up Counseling. Int. J. Environ. Res. Public Health 2020, 17, 3152. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, E.; Lee, H. Association between workplace bullying and burnout, professional quality of life, and turnover intention among clinical nurses. PLoS ONE 2019, 14, e0226506, Erratum in PLoS ONE 2020, 15, e0228124. [Google Scholar] [CrossRef]
- De Looff, P.; Nijman, H.; Didden, R.; Embregts, P. Burnout symptoms in forensic psychiatric nurses and their associations with personality, emotional intelligence and client aggression: A cross-sectional study. J. Psychiatr. Ment. Health Nurs. 2018, 25, 506–516. [Google Scholar] [CrossRef]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [Green Version]
- Yates, S.W. Physician Stress and Burnout. Am. J. Med. 2020, 133, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romani, M.; Ashkar, K. Burnout among Physicians. 2014. Available online: https://doi.org/10.3402/ljm.v9.23556 (accessed on 14 September 2021).
- Torres, L.-A.P.-D.; Atalaya, J.C.V.-M.; García-Campayo, J.; Roldán-Villalobos, A.; Magallón-Botaya, R.; Bartolomé-Moreno, C.; Moreno-Martos, H.; Melús-Palazón, E.; Liétor-Villajos, N.; Valverde-Bolívar, F.J.; et al. Controlled clinical trial comparing the effectiveness of a mindfulness and self-compassion 4-session programme versus an 8-session programme to reduce work stress and burnout in family and community medicine physicians and nurses: MINDUUDD study protocol. BMC Fam. Pract. 2019, 20, 24. [Google Scholar] [CrossRef]
- Jose, S.; Dhandapani, M.; Cyriac, M.C. Burnout and Resilience among Frontline Nurses during COVID-19 Pandemic: A Cross-sectional Study in the Emergency Department of a Tertiary Care Center, North India. Indian J. Crit. Care Med. 2020, 24, 1081–1088. [Google Scholar] [CrossRef]
- Edward, K.L.; Ousey, K.; Warelow, P.; Lui, S. Nursing and aggression in the workplace: A systematic review. Br. J. Nurs. 2014, 23, 653–654. [Google Scholar] [CrossRef] [Green Version]
- Giménez-Espert, M.D.C.; Prado-Gascó, V.; Soto-Rubio, A. Psychosocial Risks, Work Engagement, and Job Satisfaction of Nurses During COVID-19 Pandemic. Front. Public Health 2020, 8, 566896. [Google Scholar] [CrossRef] [PubMed]
- Elghazally, S.A.; Alkarn, A.F.; Elkhayat, H.; Ibrahim, A.K.; Elkhayat, M.R. Burnout Impact of COVID-19 Pandemic on Health-Care Professionals at Assiut University Hospitals, 2020. Int. J. Environ. Res. Public Health 2021, 18, 5368. [Google Scholar] [CrossRef] [PubMed]
- Firew, T.; Sano, E.D.; Lee, J.W.; Flores, S.; Lang, K.; Salman, K.; Greene, M.C.; Chang, B.P. Protecting the front line: A cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open 2020, 10, e042752. [Google Scholar] [CrossRef]
- Miguel-Puga, J.A.; Cooper-Bribiesca, D.; Avelar-Garnica, F.J.; Sanchez-Hurtado, L.A.; Colin-Martínez, T.; Espinosa-Poblano, E.; Anda-Garay, J.C.; González-Díaz, J.I.; Segura-Santos, O.B.; Vital-Arriaga, L.C.; et al. Burnout, depersonalization, and anxiety contribute to post-traumatic stress in frontline health workers at COVID-19 patient care, a follow-up study. Brain Behav. 2021, 11, e02007. [Google Scholar] [CrossRef]
- Sharma, M.; Creutzfeldt, C.J.; Lewis, A.; Patel, P.V.; Hartog, C.; E Jannotta, G.; Blissitt, P.; Kross, E.K.; Kassebaum, N.; Greer, D.M.; et al. Health-care Professionals’ Perceptions of Critical Care Resource Availability and Factors Associated with Mental Well-being During Coronavirus Disease 2019 (COVID-19): Results from a US Survey. Clin. Infect. Dis. 2021, 72, e566–e576. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number (%) of Respondents |
|---|---|
| Male | 684 (54.3%) |
| Female | 575 (45.7%) |
| Employment in COVID-19 ICUs | |
| Employed | 889 (70.6%) |
| Non-employed | 370 (29.4%) |
| Duration of work (employment) in COVID-19 ICUs at the time of the survey | |
| More than 1 year | 124 (9.8%) |
| 11 months–1 year | 128 (10.2%) |
| 9–10 months | 154 (12.2%) |
| 7–8 months | 136 (10.8%) |
| 5–6 months | 152 (12.1%) |
| 3–4 months | 197 (15.6%) |
| 1–2 months | 65 (5.2%) |
| Do not work in COVID-19 ICUs | 303 (24.1%) |
| Job position in the ICU | |
| Physician | 767 (60.9%) |
| Nurse | 492 (39.1%) |
| Duration of work in the specified job position (the specialty) | |
| More than 8 years | 535 (42.5%) |
| 5–7 years | 196 (15.6%) |
| 2–4 years | 171 (13.6%) |
| 6 months–1 year | 232 (18.4%) |
| 4–5 months | 95 (7.5%) |
| 1–3 months | 30 (2.4%) |
| Specialty in the COVID-19 ICU at the time of the survey | |
| Practice their specialty | 864 (68.6%) |
| Were retrained for another specialty | 34 (2.7%) |
| Do not practice their specialty | 358 (28.7%) |
| Scale | Non-COVID-19 Hospitals | COVID-19 Hospitals | Reliability of Differences |
|---|---|---|---|
| Physical aggression | M = 31.62 SD = 17.990 | M = 27.16 SD = 16.307 | U = 58,435.000 p = 0.000 |
| Indirect aggression | M = 51.55 SD = 20.340 | M = 58.51 SD = 24.686 | U = 55,849.500 p = 0.000 |
| Verbal aggression | M = 49.54 SD = 20.340 | M = 61.92 SD = 21.166 | U = 44,937.000 p = 0.000 |
| Index of aggressive behavior | M = 44.2360 SD = 14.325 | M = 49.1982 SD = 15.532 | U = 50,431.500 p = 0.000 |
| Occupational stress | M = 40.62 SD = 8.595 | M = 42.91 SD = 8.889 | U = 55,097.500 p = 0.000 |
| Emotional exhaustion | M = 27.80 SD = 11.288 | M = 26.59 SD = 10.055 | U = 63,052.000 p = 0.063 |
| Depersonalization | M = 13.35 SD = 5.775 | M = 14.34 SD = 5.461 | U = 62,966.000 p = 0.059 |
| Scale | Occupational Burnout | Validity of Differences | ||
|---|---|---|---|---|
| Average Level | High Level | Mann-Whitney U-Test | p-Value | |
| Emotional exhaustion | 19 | 37 | 601.000 | 0.000 |
| Depersonalization | 11 | 17 | 22,068.000 | 0.000 |
| Reduced personal accomplishment (reverse scale) | 35 | 29 | 33,118.500 | 0.000 |
| Number | 408 | 332 | ||
| Occupational Burnout | ||||
|---|---|---|---|---|
| Average Level | High Level | |||
| Profile of hospital admissions | Non-COVDI-19 hospitals | Actual frequency | 190 | 180 |
| Expected frequency | 204 | 166 | ||
| COVID-19 hospitals | Actual frequency | 218 | 152 | |
| Expected frequency | 204 | 166 | ||
| χ2 = 4283, p = 0.038 | ||||
| Scale | Emotional Exhaustion | Depersonalization | Reduced Personal Accomplishment (Reverse) | Indirect Aggression | Verbal Aggression | Index of Aggressive Behavior |
|---|---|---|---|---|---|---|
| Occupational stress | Ro = 0.486 ** | Ro = 0.413 ** | Ro = −0.255 ** | Ro = 0.391 ** | Ro = 0.269 ** | Ro = 0.312 ** |
| Emotional exhaustion | - | - | - | Ro = 0.325 ** | - | Ro = 0.272 ** |
| Depersonalization | - | - | - | Ro = 0.301 ** | Ro = 0.246 ** | Ro = 0.301 ** |
| Reduced personal accomplishment (reverse) | - | - | - | Ro = −0.216 ** | - | - |
| Scale | Emotional Exhaustion | Depersonalization | Reduced Personal Accomplishment (Reverse) | Physical Aggression | Indirect Aggression | Verbal Aggression | Index of Aggressive Behavior |
|---|---|---|---|---|---|---|---|
| Employment duration | - | - | - | Ro = −0.224 ** | - | Ro = −0.259 ** | Ro = −0.323 ** |
| Age | - | - | Ro = 0.204 ** | Ro = −0.257 ** | Ro = −0.427 ** | Ro = −0.232 ** | Ro = −0.398 ** |
| Occupational stress | Ro = 0.539 ** | Ro = 0.404 ** | Ro = −0.331 ** | − | Ro = 0.327 ** | - | - |
| Emotional exhaustion | - | - | - | Ro = 0.218 ** | Ro = 0.395 ** | - | Ro = 0.341 ** |
| Depersonalization | - | - | - | Ro = 0.330 ** | - | - | - |
| Reduced personal accomplishment (reverse) | - | - | - | Ro = −0.225 ** | Ro = −0.515 ** | Ro = −0.331 ** | Ro = −0.483 ** |
| Scale | R-Squared | F-Criteria | Durbin–Watson Criteria | |
|---|---|---|---|---|
| Constant | β = −3.316 p = 0.153 | 0.342 | F = 95.517 p = 0.000 | 1.978 |
| Occupational stress | β = 0.665 p = 0.000 | |||
| Indirect aggression | β = 0.080 p = 0.003 | |||
| Scale | R-Squared | F-Criteria | Durbin–Watson Criteria | |
|---|---|---|---|---|
| Constant | β = 0.662 p = 0.609 | 0.219 | F = 51.548 p = 0.000 | 1.992 |
| Occupational stress | β = 0.265 p = 0.000 | |||
| Indirect aggression | β = 0.037 p = 0.012 | |||
| Scale | R-Squared | F-Criteria | Durbin–Watson Criteria | |
|---|---|---|---|---|
| Constant | β = 41.436 p = 0.000 | 0.122 | F = 16.935 p = 0.000 | 2.360 |
| Occupational stress | β = −0.197 p = 0.000 | |||
| Indirect aggression | β = −0.059 p = 0.001 | |||
| Verbal aggression | β = 0.035 p = 0.042 | |||
| Scale | R-Squared | F-Criteria | Durbin–Watson Criteria | |
| Constant | β = −0.804 p = 0.714 | 0.325 | F = 58.874 p = 0.000 | 2.439 |
| Occupational stress | β = 0.466 p = 0.000 | |||
| Indirect aggression | β = 0.086 p = 0.000 | |||
| Physical aggression | β = 0.088 p = 0.001 | |||
| Scale | R-Squared | F-Criteria | Durbin–Watson Criteria | |
|---|---|---|---|---|
| Constant | β = 0.983 p = 0.421 | 0.312 | F = 41.305 p = 0.000 | 1.968 |
| Occupational stress | β = 0.262 p = 0.000 | |||
| Physical aggression | β = 0.098 p = 0.000 | |||
| Indirect aggression | β = −0.040 p = 0.000 | |||
| Verbal aggression | β = 0.029 p = 0.0047 | |||
| Scale | Nurses | Physicians | Reliability of Differences |
|---|---|---|---|
| Verbal aggression | M = 52.43 SD = 25.112 | M = 48.28 SD = 17.789 | U = 12,584.500 p = 0.047 |
| Indirect aggression | M = 55.88 SD = 16.973 | M = 49.67 SD = 21.397 | U = 11,159.500 p = 0.002 |
| Index of aggressive behavior | M = 47.32 SD = 14.418 | M = 42.9 SD = 14.103 | U = 11,159.500 p = 0.001 |
| Reduced personal accomplishment (reverse scale) | M = 33.09 SD = 6.087 | M = 31.71 SD = 6.728 | U = 12,296.000 p = 0.022 |
| Scale | Nurses | Physicians | Reliability of Differences |
|---|---|---|---|
| Verbal aggression | M = 59.58 SD = 23.820 | M = 64.66 SD = 17.912 | U = 88,855.500 p = 0.036 |
| Indirect aggression | M = 52.51 SD = 20.641 | M = 64.03 SD = 25.653 | U = 68,847.000 p = 0.000 |
| Index of aggressive behavior | M = 46.22 SD = 16.582 | M = 52.16 SD = 13.71 | U = 72,983.000 p = 0.000 |
| Depersonalization | M = 15.17 SD = 6.307 | M = 13.93 SD = 4.800 | U = 78,898.500 p = 0.000 |
| Scale | 1–4 Months | 5–8 Months | 9 Months–1 Year | Over 1 Year | Reliability of Differences |
|---|---|---|---|---|---|
| Physical aggression | M = 31.14 SD = 12.194 | M = 36.76 SD = 20.449 | M = 17.77 SD = 13.508 | M = 22.31 SD = 11.724 | H = 71.484 p = 0.000 |
| Verbal aggression | M = 80.20 SD = 11.456 | M = 45.33 SD = 24.647 | M = 57.65 SD = 24.721 | M = 60.31 SD = 14.106 | H = 94.789 p = 0.000 |
| Indirect aggression | M = 62.80 SD = 13.661 | M = 56.40 SD = 18.359 | M = 44.36 SD = 24.757 | M = 49.64 SD = 16.416 | H = 43.779 p = 0.000 |
| Index of aggressive behavior | M = 58.05 SD = 7.599 | M = 46.17 SD = 16.673 | M = 39.93 SD = 19.125 | M = 44.09 SD = 12.241 | H = 60.056 p = 0.000 |
| Occupational stress | M = 40.94 SD = 2.866 | M = 41.71 SD = 10.808 | M = 43.79 SD = 11.739 | M = 42.85 SD = 8.751 | H = 10.104 p = 0.018 |
| Emotional exhaustion | M = 22.53 SD = 5.597 | M = 32.00 SD = 11.471 | M = 26.19 SD = 11.259 | M = 24.23 SD = 11.034 | H = 34.789 p = 0.000 |
| Depersonalization | M = 13.61 SD = 1.690 | M = 15.92 SD = 9.186 | M = 14.82 SD = 5.532 | M = 16.33 SD = 5.448 | H = 17.153 p = 0.001 |
| Reduced personal accomplishment (reverse scale) | M = 33.19 SD = 4.000 | M = 27.88 SD = 12.408 | M = 30.86 SD = 9.727 | M = 33.05 SD = 6.212 | H = 10.111 p = 0.018 |
| Scale | 1–4 Months | 5–8 Months | 9 Months–1 Year | More Than 1 Year | Reliability of Differences |
|---|---|---|---|---|---|
| Physical aggression | M = 31.27 SD = 20.513 | M = 25.70 SD = 13.588 | M = 27.31 SD = 12.616 | M = 28.54 SD = 9.890 | H = 7.960 p = 0.047 |
| Verbal aggression | M = 62.98 SD = 25.257 | M = 67.91 SD = 16.326 | M = 65.23 SD = 8.336 | M = 52.88 SD = 19.422 | H = 30.686 p = 0.000 |
| Indirect aggression | M = 55.00 SD = 33.161 | M = 72.33 SD = 14.988 | M = 68.12 SD = 22.771 | M = 38.63 SD = 23.863 | H = 58.141 p = 0.000 |
| Index of aggressive behavior | M = 49.75 SD = 21.311 | M = 55.31 SD = 6.707 | M = 53.55 SD = 8.736 | M = 40.02 SD = 15.466 | H = 29.935 p = 0.000 |
| Occupational stress | M = 39.30 SD = 6.436 | M = 45.80 SD = 9.164 | M = 45.23 SD = 8.039 | M = 41.78 SD = 4.333 | H = 64.529 p = 0.000 |
| Emotional exhaustion | M = 26.39 SD = 12.917 | M = 26.26 SD = 8.854 | M = 29.91 SD = 5.401 | M = 20.29 SD = 6.535 | H = 76.483 p = 0.000 |
| Depersonalization | M = 11.47 SD = 4.768 | M = 15.30 SD = 4.725 | M = 15.03 SD = 4.213 | M = 11.05 SD = 2.915 | H = 63.588 p = 0.000 |
| Reduced personal accomplishment (reverse scale) | M = 35.65 SD = 4.713 | M = 31.80 SD = 4.157 | M = 28.82 SD = 4.469 | M = 32.76 SD = 3.967 | H = 111.989 p = 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashtanov, A.; Molotok, E.; Yavorovskiy, A.; Boyarkov, A.; Vasil’ev, Y.; Alsaegh, A.; Dydykin, S.; Kytko, O.; Meylanova, R.; Enina, Y.; et al. A Comparative Cross-Sectional Study Assessing the Psycho-Emotional State of Intensive Care Units’ Physicians and Nurses of COVID-19 Hospitals of a Russian Metropolis. Int. J. Environ. Res. Public Health 2022, 19, 1828. https://doi.org/10.3390/ijerph19031828
Kashtanov A, Molotok E, Yavorovskiy A, Boyarkov A, Vasil’ev Y, Alsaegh A, Dydykin S, Kytko O, Meylanova R, Enina Y, et al. A Comparative Cross-Sectional Study Assessing the Psycho-Emotional State of Intensive Care Units’ Physicians and Nurses of COVID-19 Hospitals of a Russian Metropolis. International Journal of Environmental Research and Public Health. 2022; 19(3):1828. https://doi.org/10.3390/ijerph19031828
Chicago/Turabian StyleKashtanov, Artem, Ekaterina Molotok, Andrey Yavorovskiy, Alexander Boyarkov, Yuriy Vasil’ev, Ali Alsaegh, Sergey Dydykin, Olesya Kytko, Renata Meylanova, Yulianna Enina, and et al. 2022. "A Comparative Cross-Sectional Study Assessing the Psycho-Emotional State of Intensive Care Units’ Physicians and Nurses of COVID-19 Hospitals of a Russian Metropolis" International Journal of Environmental Research and Public Health 19, no. 3: 1828. https://doi.org/10.3390/ijerph19031828
APA StyleKashtanov, A., Molotok, E., Yavorovskiy, A., Boyarkov, A., Vasil’ev, Y., Alsaegh, A., Dydykin, S., Kytko, O., Meylanova, R., Enina, Y., Troitskiy, V., Kapitonova, M., Vaits, S., Vaits, T., Saleev, R., Saleeva, G., & Saleev, N. (2022). A Comparative Cross-Sectional Study Assessing the Psycho-Emotional State of Intensive Care Units’ Physicians and Nurses of COVID-19 Hospitals of a Russian Metropolis. International Journal of Environmental Research and Public Health, 19(3), 1828. https://doi.org/10.3390/ijerph19031828