
Designing a Patient-Friendly Website for Newly Diagnosed Cancer Patients with the Participatory Health Research Approach


 ,
,
Abstract
:1. Introduction
1.1. Background Patient Information Material (PIM)
1.2. The Need for a Patient-Friendly Website for a New Psycho-Oncological Care Programme
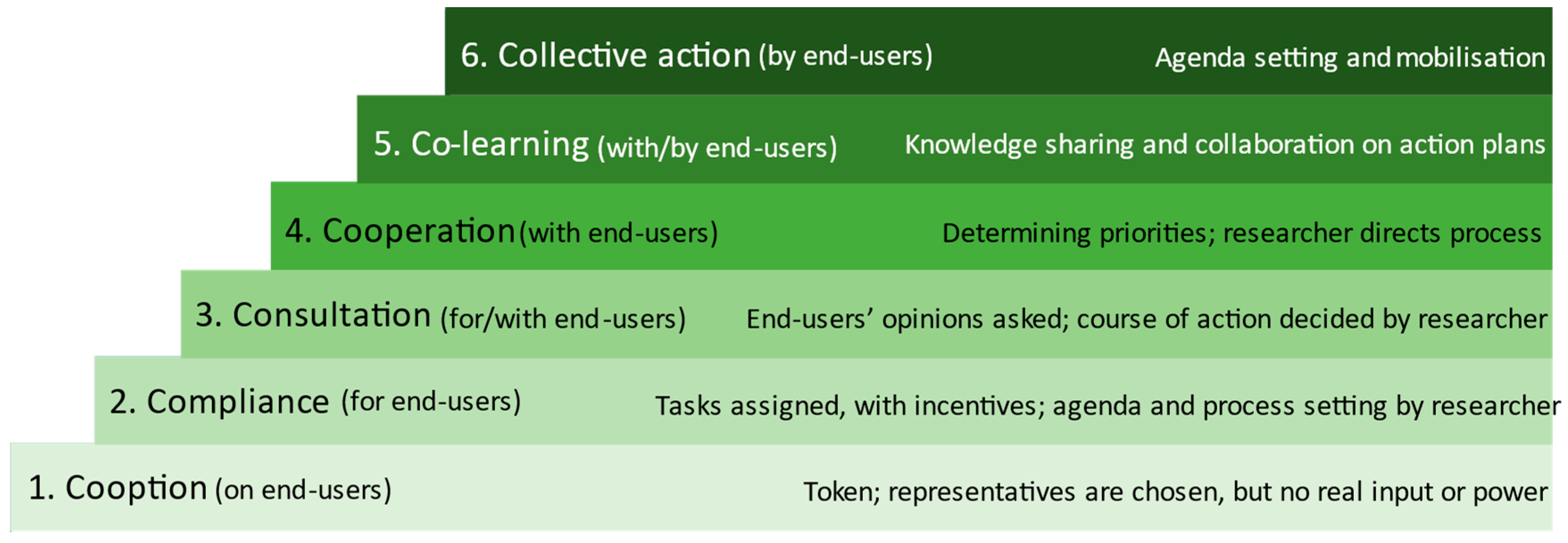
1.3. Participatory Approaches in PIM Development Processes
1.4. Objectives and Research Questions of this Study
2. Materials and Methods
2.1. Study Design, Approach, and Participants
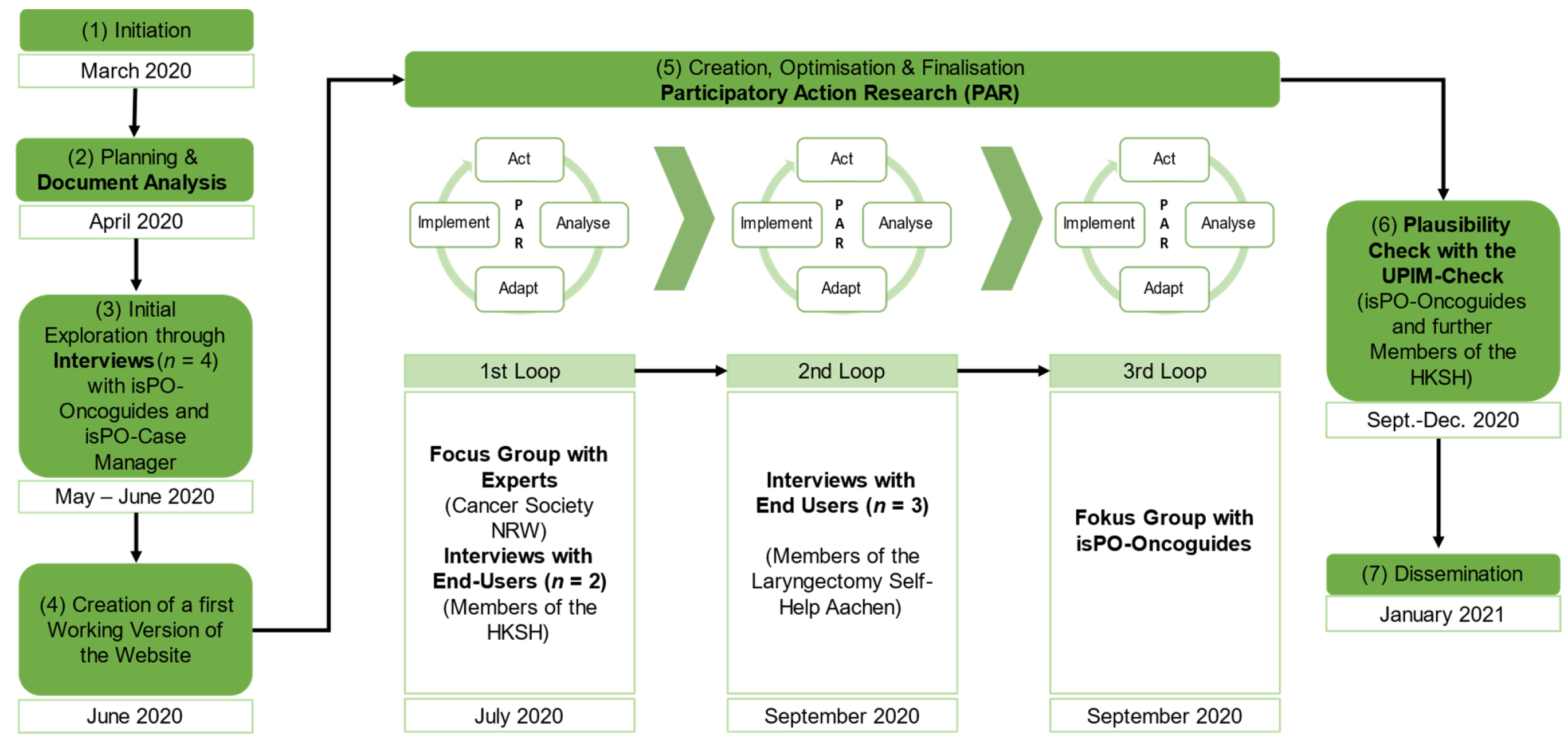
2.2. Research Process
2.3. Data Collection and Analysis
2.3.1. Qualitative Data Collection and Analysis
2.3.2. Quantitative Analysis Using the UPIM-Check Instrument for Descriptive Analysis
3. Results
3.1. Outcomes from Step 2—Document Analysis
3.2. Outcomes from Step 3—Initial Exploration through Interviews
- (1)
- Assessment of the existing information material: The structure of the flyer and the tree motif were perceived to be a positive and stimulating signal. The participants noted that the illustration of the chronological sequences of the questionnaires, as presented on the one-pager, was “too complex” and “overwhelming”, and thus hard to understand. Moreover, the content material of the preliminary working version of the isPO website was considered to be “too text-heavy”.
- (2)
- Exploring a suitable patient-friendly design and structure of the website: Participants confirmed a positive association with the green colour scheme and the tree motif. In addition, they emphasized that we should consider a “good balance between text parts and illustrations”.
- (3)
- Reflecting on the meaningful content of the website: All participants suggested that the stepped-care approach of isPO and the different professions involved in the care provision (isPO team) should be carefully elucidated. The interviewees emphasised the importance of offering comprehensive information on what psycho-oncological care is and entails, as “potentially many patients are unfamiliar with this care approach” in Germany and it, thus, may help diminish perceived stigmatisation around psychosocial distress among cancer patients.
3.3. Outcomes from Step 4—Creation of an Initial Working Version of the Website
3.4. Outcomes from Step 5—Optimisation Loop 1
3.5. Outcomes from Step 5—Optimisation Loop 2
3.6. Outcomes from Step 5—Optimisation Loop 3
3.7. Outcomes from Step 6—Plausibility Check
4. Discussion
4.1. Principal Findings
4.2. Why a Patient-Friendly Website Is Needed
4.3. How to Design this Website
4.4. Why the Plausibility Check was Necessary but Challenging
4.5. Methodological Issues (PHR and PAR)
4.6. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sänger, S.; Lang, B.; Klemperer, D.; Thomeczek, C.; Dierks, M.-L. Manual Patienteninformation: Empfehlungen zur Erstellung Evidenzbasierter Patienteninformationen; ÄZQ: Berlin, Germany, 2006; ISBN 978-3-9811002-0-4. [Google Scholar]
- Coulter, A. Evidence based patient information. Is important, so there needs to be a national strategy to ensure it. BMJ 1998, 317, 225–226. [Google Scholar] [CrossRef] [PubMed]
- Ernstmann, N.; Sautermeister, J.; Halbach, S. Gesundheitskompetenz. In Gesundheitswissenschaften; Haring, R., Ed.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 1–9. ISBN 978-3-662-54179-1. [Google Scholar]
- Banasiak, N.C.; Meadows-Oliver, M. Evaluating asthma websites using the Brief DISCERN instrument. J. Asthma Allergy 2017, 10, 191–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tait, A.R.; Voepel-Lewis, T.; Levine, R. Using digital multimedia to improve parents’ and children’s understanding of clinical trials. Arch. Dis. Child. 2015, 100, 589–593. [Google Scholar] [CrossRef]
- Kildea, J.; Battista, J.; Cabral, B.; Hendren, L.; Herrera, D.; Hijal, T.; Joseph, A. Design and Development of a Person-Centered Patient Portal Using Participatory Stakeholder Co-Design. J. Med. Internet Res. 2019, 21, e11371. [Google Scholar] [CrossRef] [PubMed]
- Roberto, A.; Colombo, C.; Candiani, G.; Satolli, R.; Giordano, L.; Jaramillo, L.; Castagno, R.; Mantellini, P.; Falini, P.; Carnesciali, E.; et al. A dynamic web-based decision aid to improve informed choice in organised breast cancer screening. A pragmatic randomised trial in Italy. Br. J. Cancer 2020, 123, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Herm, K.; Linden, M. Qualitätssicherung von schriftlichen Patienteninformationen. Psychother. Psych. Med. 2013, 63, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Community Health 1999, 53, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoemaker, S.J.; Wolf, M.S.; Brach, C. Development of the Patient Education Materials Assessment Tool (PEMAT): A new measure of understandability and actionability for print and audiovisual patient information. Patient Educ. Couns. 2014, 96, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köpke, S.; Berger, B.; Steckelberg, A.; Meyer, G. In Deutschland gebräuchliche Bewertungsinstrumente für Patienteninformationen - eine kritische Analyse. Z. Ärztl. Fortbild. Qual. Gesundh. Wes. 2005, 99, 353–357. [Google Scholar]
- Salm, S.; Mollenhauer, J.; Hornbach, C.; Cecon, N.; Dresen, A.; Houwaart, S.; Arning, A.; Göttel, A.; Schwickerath, K.; Pfaff, H.; et al. Participatory Development and Preliminary Psychometric Properties of the User-Friendly Patient Information Material Checklist (UPIM-Check). Int. J. Environ. Res. Public Health 2021, 18, 8773. [Google Scholar] [CrossRef] [PubMed]
- Salm, S. Optimizing the patient information material for cancer patients using the participatory health research approach. Eur. J. Public Health 2020, 30, ckaa165.1436. [Google Scholar] [CrossRef]
- Pew Research Center. Health Topics. Available online: https://www.pewresearch.org/internet/2011/02/01/health-topics-4/ (accessed on 14 December 2021).
- Amante, D.J.; Hogan, T.P.; Pagoto, S.L.; English, T.M.; Lapane, K.L. Access to care and use of the Internet to search for health information: Results from the US National Health Interview Survey. J. Med. Internet Res. 2015, 17, e106. [Google Scholar] [CrossRef]
- Reifegerste, D.; Bachl, M.; Baumann, E. Surrogate health information seeking in Europe: Influence of source type and social network variables. Int. J. Med. Inform. 2017, 103, 7–14. [Google Scholar] [CrossRef]
- Snyder, C.F.; Wu, A.W.; Miller, R.S.; Jensen, R.E.; Bantug, E.T.; Wolff, A.C. The role of informatics in promoting patient-centered care. Cancer J. 2011, 17, 211–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soobrah, R.; Clark, S.K. Your patient information website: How good is it? Colorectal Dis. 2012, 14, e90–e94. [Google Scholar] [CrossRef]
- Risk, A.; Petersen, C. Health information on the internet: Quality issues and international initiatives. JAMA 2002, 287, 2713–2715. [Google Scholar] [CrossRef]
- Refai, M.; Andolfi, M.; Gentili, P.; Pelusi, G.; Manzotti, F.; Sabbatini, A. Enhanced recovery after thoracic surgery: Patient information and care-plans. J. Thorac. Dis. 2018, 10, S512–S516. [Google Scholar] [CrossRef] [Green Version]
- Jenniches, I.; Lemmen, C.; Cwik, J.C.; Kusch, M.; Labouvie, H.; Scholten, N.; Gerlach, A.; Stock, S.; Samel, C.; Hagemeier, A.; et al. Evaluation of a complex integrated, cross-sectoral psycho-oncological care program (isPO): A mixed-methods study protocol. BMJ Open 2020, 10, e034141. [Google Scholar] [CrossRef]
- Kusch, M.; Labouvie, H.; Schiewer, V.; Talalaev, N.; Cwik, J.C.; Bussmann, S.; Vaganian, L.; Gerlach, A.; Dresen, A.; Cecon, N.; et al. Integrated, cross-sectoral psycho-oncology (isPO): A new form of care for newly diagnosed cancer patients in Germany. Manuscr. Submitt. Publ. 2020. [Google Scholar]
- Salm, S.; Houwaart, S. 32.K. Skills building seminar: Using participatory health research to optimise psycho-oncological patient information material. Eur. J. Public Health 2020, 30, ckaa165.1434. [Google Scholar] [CrossRef]
- Krieger, T.; Salm, S.; Dresen, A.; Arning, A.; Schwickerath, K.; Göttel, A.; Houwaart, S.; Pfaff, H.; Cecon, N. Patient’s perspective matters: Optimising patient information material for a new psycho-oncological care programme using a Participatory Health Research Approach in Germany. Int. J. Environ. Res. Public Health 2022, 19, 1518. [Google Scholar] [CrossRef]
- Wright, M.T. Was ist Partizipative Gesundheitsforschung? Prävention Und Gesundh. 2013, 8, 122–131. [Google Scholar] [CrossRef]
- von Unger, H. Partizipative Forschung: Einführung in die Forschungspraxis, 1st ed.; Springer VS: Wiesbaden, Germany, 2014; ISBN 978-3-658-01289-2. [Google Scholar]
- International Collaboration for Participatory Health Research. Position Paper 1: What is Participatory Health Research? Mai 2013; International Collaboration for Participatory Health Research: Berlin, Germany, 2013. [Google Scholar]
- Arnstein, S.R. A Ladder Of Citizen Participation. J. Am. Inst. Plan. 1969, 35, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Pretty, J.N. Participatory learning for sustainable agriculture. World Dev. 1995, 23, 1247–1263. [Google Scholar] [CrossRef]
- Cornwall, A. Part IV Participatory Research Methods: First Steps in a Participatory Process: Towards Participatory Practice: Participatory Rural Appraisal (PRA) and the Participatory Process. In ParticipatoryResearch in Health: Issues and Experiences; Zed Books: London, UK, 1996; pp. 94–107. [Google Scholar]
- Curry, L.; Nunez-Smith, M. Mixed Methods in Health Sciences Research: A Practical Primer; Sage Publications, Inc: Thousand Oaks, CA, USA, 2015; ISBN 9781483306773. [Google Scholar]
- Fetterman, D. Empowerment evaluation at the Stanford University School of Medicine: Using a critical friend to improve the clerkship experience. Ens. Avaliação E Políticas Públicas Em Educ. 2009, 17, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenmenger, R. WordPress 5: Das Umfassende Handbuch; Rheinwerk Computing: Bonn, Germany, 2020; ISBN 978-3-8362-5681-0. [Google Scholar]
- Krug, S.; Dubau, J. Don’t make Me Think!: Web Usability—Das Intuitive Web; Wie Webuser Tatsächlich Mit Websites Umgehen; Verblüffend Einfache Website-Strategien; Layout und Navigation Benutzerfreundlich Gestalten; New Riders: Bonn, Germany, 2006; ISBN 3826615956. [Google Scholar]
- Krieger, T.; Salm, S.; Mollenhauer, J.; Cecon, N.; Dresen, A.; Houwaart, S.; Schwickerath, K.; Göttel, A.; Arning, A. UPIM-Check: User-friendly Patient Information Material Checklist. 2021. Available online: https://www.imvr.de/wp-content/uploads/UPIM-Check_English.pdf (accessed on 14 December 2021).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Mayring, P. Einführung in die Qualitative Sozialforschung: Eine Anleitung zu Qualitativem Denken; Beltz: Weinheim, Germany, 1999; ISBN 3621271783. [Google Scholar]
- Krieger, T.; Salm, S.; Cecon, N.; Pfaff, H.; Dresen, A. Ergebnisbericht der Zweiten Externen Formativen Evaluation des Projekts isPO: Forschungsbericht 03-2021; Veröffentlichungsreihe des Instituts für Medizinsoziologie, Versorgungsforschung und Rehabilitationswissenschaft; IMVR: Cologne, Germany, 2021. [Google Scholar]
- Ream, E.; Blows, E.; Scanlon, K.; Richardson, A. An investigation of the quality of breast cancer information provided on the internet by voluntary organisations in Great Britain. Patient Educ. Couns. 2009, 76, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Vogel, B.A.; Bengel, J.; Helmes, A.W. Information and decision making: Patients’ needs and experiences in the course of breast cancer treatment. Patient Educ. Couns. 2008, 71, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Krieger, T.; Salm, S.; Cecon, N.; Pfaff, H.; Dresen, A. Vorläufige Summative Evaluation des Projekts isPO: Forschungsbericht 10-2021; Veröffentlichungsreiche des Instituts für Medizinsoziologie, Versorgungsforschung und Rehabilitationswissenschaft; IMVR: Cologne, Germany, 2021. [Google Scholar]
- Adnan, M.; Warren, J.; Suominen, H. 10 Patient empowerment via technologies for patient-friendly personalized language. In Information Technology for Patient Empowerment in Healthcare; Grando, M., Rozenblum, R., Bates, D., Eds.; Walter De Gruyter: Berlin, Germany, 2015; pp. 153–164. ISBN 978-1-61451-592-0. [Google Scholar]
- Bergold, J.; Thomas, S. Partizipative Forschung. In Handbuch Qualitative Forschung in der Psychologie; Mey, G., Mruck, K., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2020; pp. 113–133. ISBN 978-3-658-26886-2. [Google Scholar]
- Cornwall, A. Unpacking ’Participation’ Models, meanings and practices. Community Dev. J. 2008, 43. [Google Scholar] [CrossRef] [Green Version]
- van Beusekom, M.M.; Kerkhoven, A.H.; Bos, M.J.W.; Guchelaar, H.-J.; van den Broek, J.M. The extent and effects of patient involvement in pictogram design for written drug information: A short systematic review. Drug Discov. Today 2018, 23, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Torre, M.E.; Ayala, J. Envisioning Participatory Action Research Entremundos. Fem. Psychol. 2009, 19, 387–393. [Google Scholar] [CrossRef]
- Gillam, S.; Newbould, J. Patient participation groups in general practice: What are they for, where are they going? BMJ 2016, 352, i673. [Google Scholar] [CrossRef]
- Castro, E.M.; van Regenmortel, T.; Vanhaecht, K.; Sermeus, W.; van Hecke, A. Patient empowerment, patient participation and patient-centeredness in hospital care: A concept analysis based on a literature review. Patient Educ. Couns. 2016, 99, 1923–1939. [Google Scholar] [CrossRef]
- Bergold, J.; Thomas, S. Participatory Research Methods: A Methodological Approach in Motion. Hist. Soc. Res. Hist. Soz. 2012, 37, 191–222. [Google Scholar]
- von Unger, H. Partizipative Gesundheitsforschung: Wer partizipiert woran? Forum Qual. Soz. Forum: Qual. Soc. Res. 2012, 13, 29. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, Y.; Xie, B. Quality of health information for consumers on the web: A systematic review of indicators, criteria, tools, and evaluation results. J. Assoc. Inf. Sci. Technol. 2015, 66, 2071–2084. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Participant and Background | Sex (F/M) | Type (I/FG) | Setting/Affiliation |
|---|---|---|---|
| isPO-Oncoguide Former cancer patient | F | Interview | Johanna Etienne Hospital Neuss |
| isPO-Oncoguide Former cancer patient | M | Interview | University Hospital of Cologne |
| isPO-Oncoguide Former cancer patient | F | Interview | Maria Hilf Hospital Mönchengladbach |
| isPO-Case Manager The patient’s contact person | F | Interview | University Hospital of Cologne |
| Experts In the cancer support sector | F (n = 3) | Focus Group | Members of KG NRW |
| Potential end-users Former cancer patient | F | Interview | Member of the House of Cancer Self-Help |
| Potential end-users Former cancer patient | F | Interview | Member of the House of Cancer Self-Help |
| Potential end-users Former cancer patient | M | Interview | Member of the District Association of Laryngectomists Aachen e.V. |
| Potential end-users Former cancer patient | F | Interview | Member of the District Association of Laryngectomists Aachen e.V. |
| Potential end-users Former cancer patient | M | Interview | Member of the District Association of Laryngectomists Aachen e.V. |
| isPO-Oncoguides Former cancer patients | F (n = 5) M (n = 2) | Focus Group | University Hospital of Cologne, Johanna Etienne Hospital Neuss, Maria Hilf Hospital Mönchengladbach, GFO Troisdorf Hospital |
| isPO PIM (Optimised from 03/2021) | Utilisation in isPO | Content | Design Features | Suitable Element for Utilisation on the Patient-Friendly Website |
|---|---|---|---|---|
| Poster | For all patients (e.g., in the waiting room) | Mention of rough key data; the description in key points; call to address in case of interest | Tree motif; green colour scheme; isPO logo |
|
| Leaflet | For potential isPO patients and interested parties (e.g., distributed on oncological units) | Explanation of what isPO is, what the care looks like, what patients receive in the care; specific contacts | Tree motif; green colour design |
|
| Patient information folder | The potential isPO patients receive the patient map during the educational talk (handover by the isPO-Case Manager) | Information on the isPO care programme and the isPO study | Four-page information map with isPO logo |
|
| “One-Pager” (study information overview) | isPO patients receive the one-pager when enrolling in the study (handover by the isPO-Case Manager) | Description of the isPO study | Coloured timeline of the isPO programme and isPO study |
|
| Correctness & Validity of Content - Does the Content Seem to Be Correct? Does the Information Appear to Be Valid? | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q1.1 | Q1.2 | Q1.3 | Q1.4 | Q1.5 | Q1.6 | Q1.7 | Q1.8 | Q1.9 | ||
| Very Good | 44.4% | 60.0% | 50.0% | 80.0% | 30.0% | 70.0% | 40.0% | 40.0% | 20.0% | 10.0% | |
| Sufficient | 24.4% | 20.0% | 20.0% | 0.0% | 40.0% | 0.0% | 20.0% | 30.0% | 40.0% | 50.0% | |
| Unsatisfactory | 17.8% | 0.0% | 20.0% | 10.0% | 10.0% | 20.0% | 30.0% | 10.0% | 30.0% | 30.0% | |
| NI | 13.3% | 20.0% | 10.0% | 10.0% | 20.0% | 10.0% | 10.0% | 20.0% | 10.0% | 10.0% | |
| Readability of Content - Is the Content Easy to Read? | |||||||||||
| Q2 | Q2.1 | Q2.2 | Q2.3 | Q2.4 | Q2.5 | Q2.6 | Q2.7 | Q2.8 | |||
| Very Good | 50.0% | 50.0% | 60.0% | 70.0% | 60.0% | 30.0% | 60.0% | 50.0% | 20.0% | ||
| Sufficient | 25.0% | 30.0% | 10.0% | 10.0% | 20.0% | 50.0% | 20.0% | 40.0% | 20.0% | ||
| Unsatisfactory | 10.0% | 20.0% | 20.0% | 10.0% | 10.0% | 0.0% | 10.0% | 0.0% | 10.0% | ||
| NI | 15.0% | 0.0% | 10.0% | 10.0% | 10.0% | 20.0% | 10.0% | 10.0% | 50.0% | ||
| Structural Readability - Is the Structure of the Information Appropriate for the Target Group? | |||||||||||
| Q3 | Q3.1 | Q3.2 | Q3.3 | Q3.4 | |||||||
| Very Good | 70.0% | 80.0% | 80.0% | 80.0% | 40.0% | ||||||
| Sufficient | 17.5% | 10.0% | 10.0% | 10.0% | 40.0% | ||||||
| Unsatisfactory | 2.5% | 0.0% | 0.0% | 0.0% | 10.0% | ||||||
| NI | 10.0% | 10.0% | 10.0% | 10.0% | 10.0% | ||||||
| Graphical Readability - Is the Layout Addressing the Needs of the Target Group? | |||||||||||
| Q4 | Q4.1 | Q4.2 | Q4.3 | Q4.4 | Q4.5 | Q4.6 | Q4.7 | Q4.8 | Q4.9 | Q4.10 | |
| Very Good | 70.0% | 50.0% | 70.0% | 70.0% | 70.0% | 70.0% | 60.0% | 70.0% | 80.0% | 90.0% | 70.0% |
| Sufficient | 12.0% | 20.0% | 0.0% | 10.0% | 10.0% | 10.0% | 20.0% | 20.0% | 10.0% | 0.0% | 20.0% |
| Unsatisfactory | 7.0% | 30.0% | 10.0% | 10.0% | 10.0% | 10.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% |
| NI | 11.0% | 0.0% | 20.0% | 10.0% | 10.0% | 10.0% | 20.0% | 10.0% | 10.0% | 10.0% | 10.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rackerseder, J.; Hornbach, C.; Dicks, P.; Kerek-Bodden, H.; Krieger, T. Designing a Patient-Friendly Website for Newly Diagnosed Cancer Patients with the Participatory Health Research Approach. Int. J. Environ. Res. Public Health 2022, 19, 1969. https://doi.org/10.3390/ijerph19041969
Rackerseder J, Hornbach C, Dicks P, Kerek-Bodden H, Krieger T. Designing a Patient-Friendly Website for Newly Diagnosed Cancer Patients with the Participatory Health Research Approach. International Journal of Environmental Research and Public Health. 2022; 19(4):1969. https://doi.org/10.3390/ijerph19041969
Chicago/Turabian StyleRackerseder, Juliane, Carolin Hornbach, Peter Dicks, Hedy Kerek-Bodden, and Theresia Krieger. 2022. "Designing a Patient-Friendly Website for Newly Diagnosed Cancer Patients with the Participatory Health Research Approach" International Journal of Environmental Research and Public Health 19, no. 4: 1969. https://doi.org/10.3390/ijerph19041969
APA StyleRackerseder, J., Hornbach, C., Dicks, P., Kerek-Bodden, H., & Krieger, T. (2022). Designing a Patient-Friendly Website for Newly Diagnosed Cancer Patients with the Participatory Health Research Approach. International Journal of Environmental Research and Public Health, 19(4), 1969. https://doi.org/10.3390/ijerph19041969