
Bicycle Touring 480 km in Seven Days: Effects on Body Composition and Physical Fitness—A Case Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Procedures
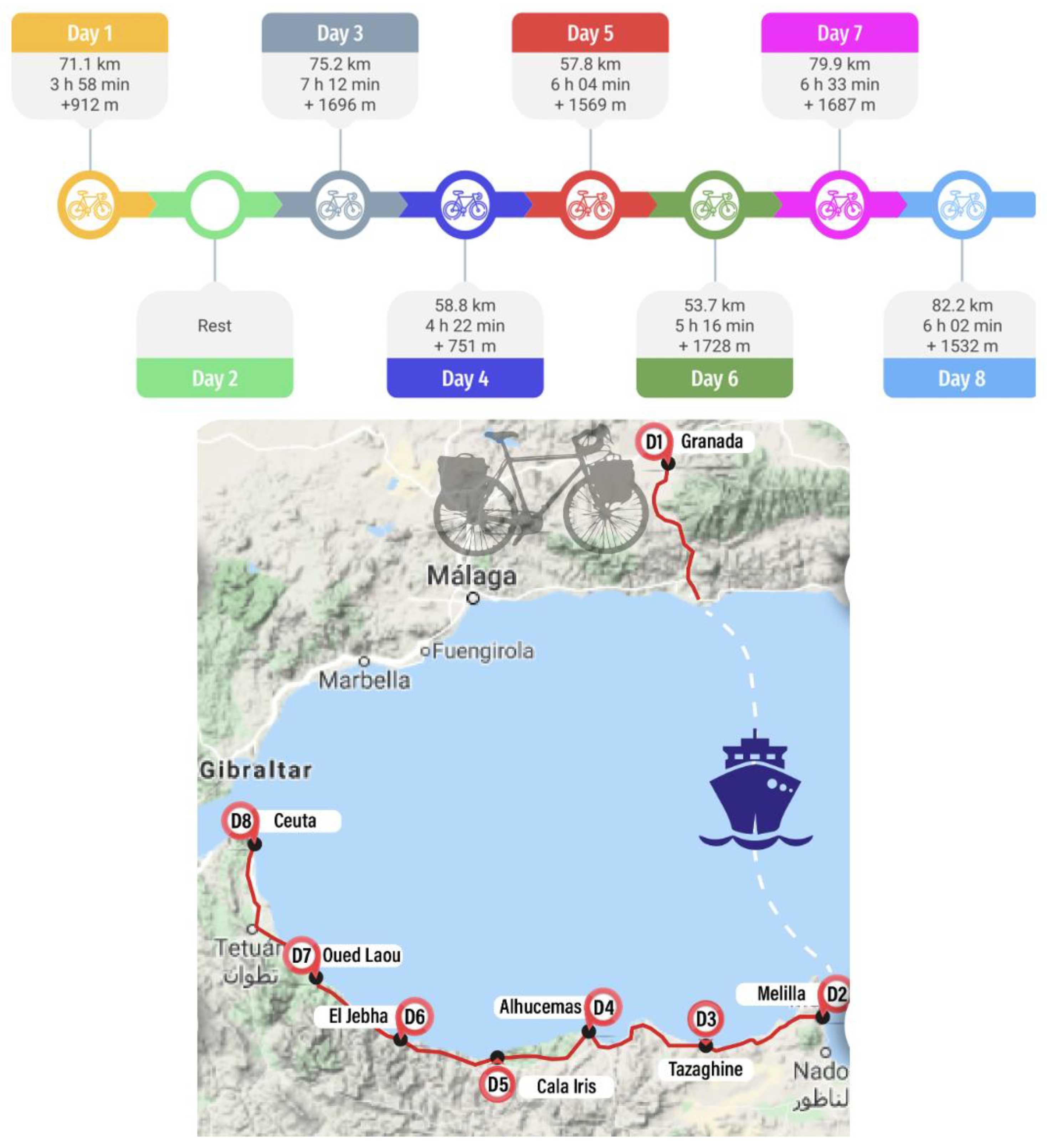
2.4. Intervention
2.5. Outcomes
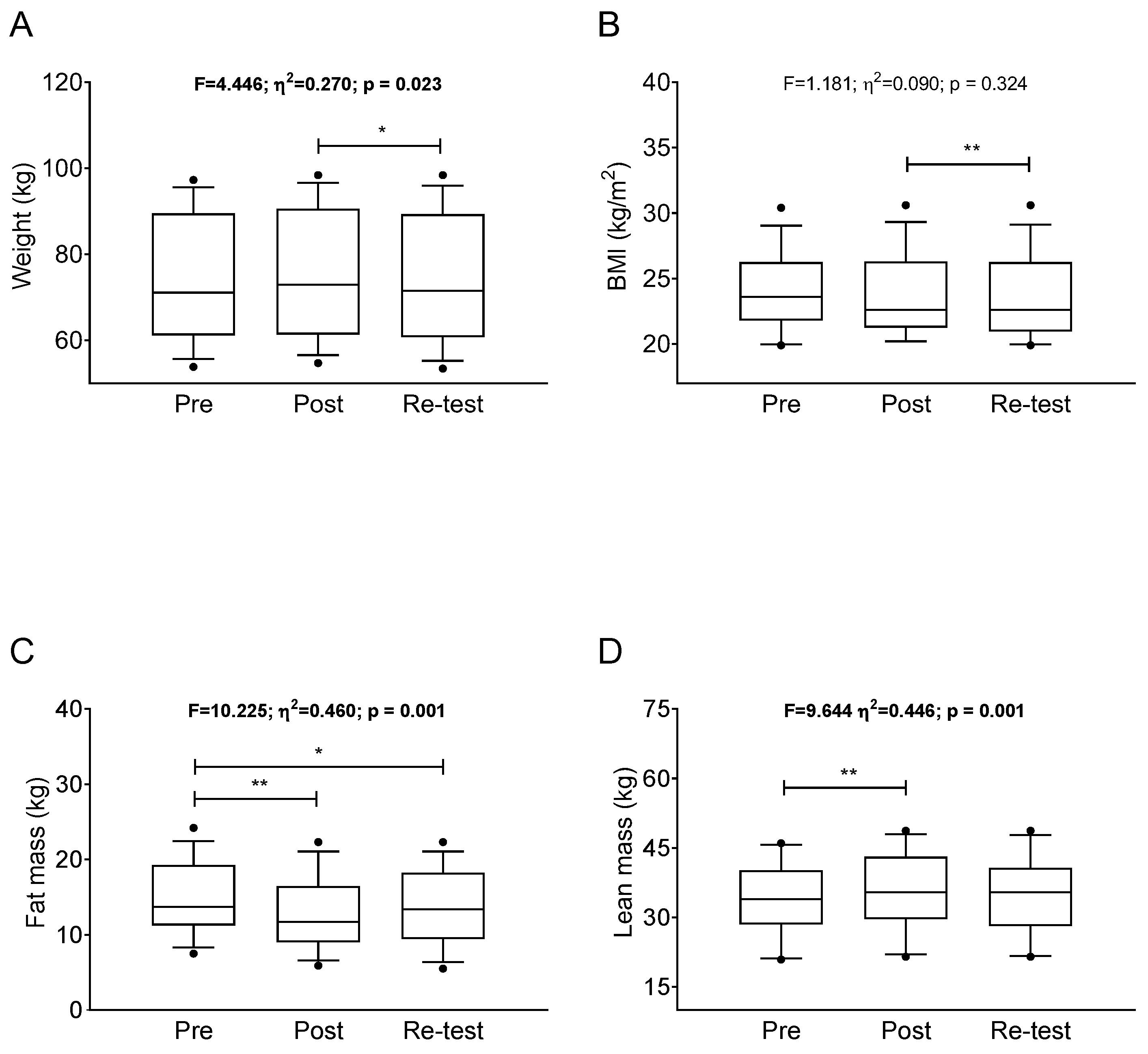
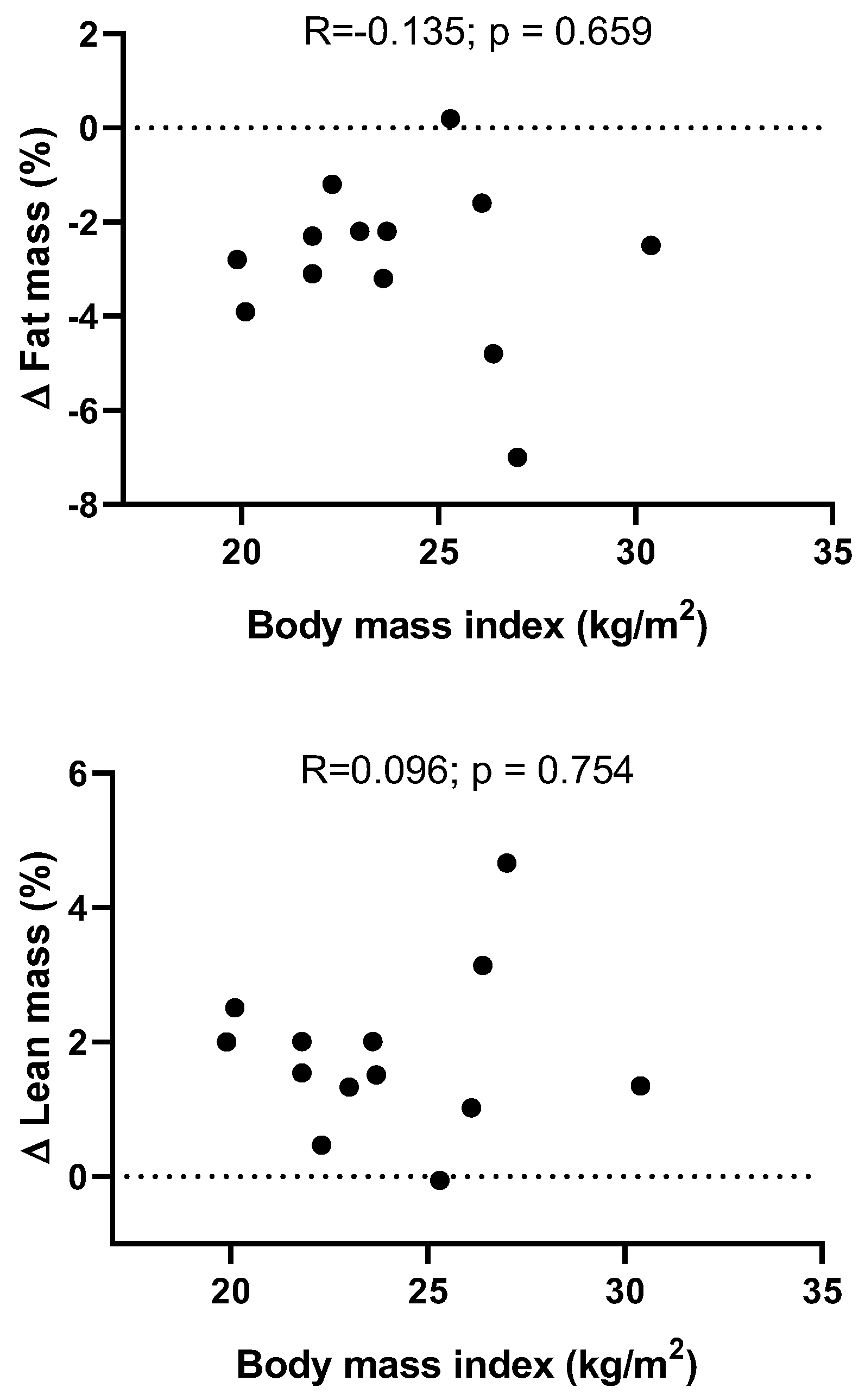
2.5.1. Anthropometry and Body Composition
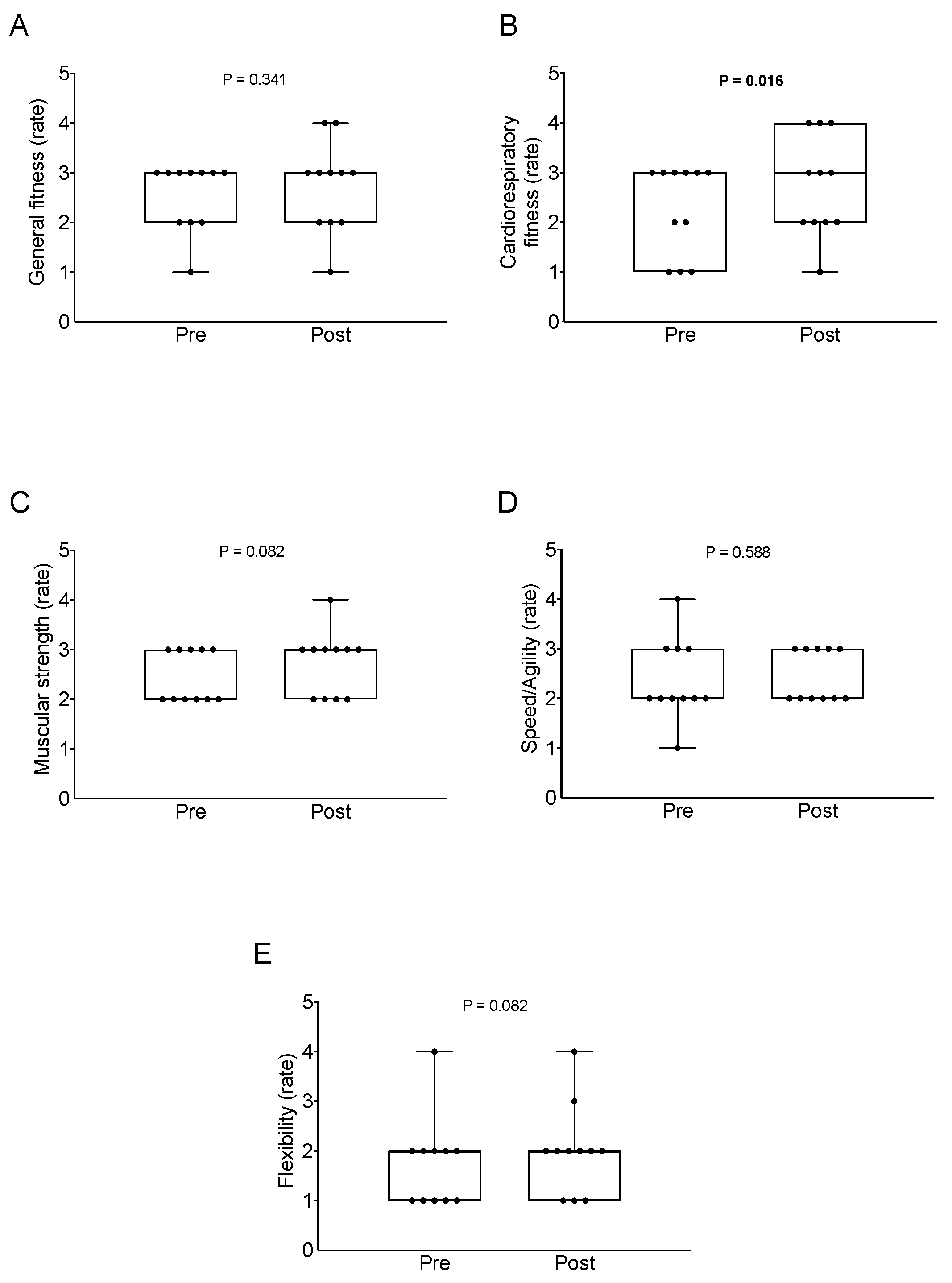
2.5.2. Physical Fitness
2.5.3. Heart Rate
2.5.4. Perceived Exertion
2.5.5. Emotion (Affective Slider)
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Committee, P.A.G.A. Physical Activity Guidelines Advisory Committee Report, 2008; US Department of Health and Human Services: Washington, DC, USA, 2008; Volume 2008, pp. A1–H14.
- Wiklund, P. The role of physical activity and exercise in obesity and weight management: Time for critical appraisal. J. Sport Health Sci. 2016, 5, 151–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, S.A.; Fulton, J.E.; Pratt, M.; Yang, Z.; Adams, E.K. Inadequate physical activity and health care expenditures in the United States. Prog. Cardiovasc. Dis. 2015, 57, 315–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.P.; Arena, R.; Kokkinos, P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: Their independent and interwoven importance to health status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; Berrington De Gonzalez, A.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [Green Version]
- McKinney, J.; Lithwick, D.; Bohk, H.I.S.; McKinney, J.; Lithwick, D.; Isserow, S.; Heilbron, B.; Krahn, A. The health benefits of physical activity and cardiorespiratory fitness. BC Med. J. 2016, 58, 131–133. [Google Scholar]
- Kumanyika, S.; Jeffery, R.W.; Morabia, A.; Ritenbaugh, C.; Antipatis, V.J. Obesity prevention: The case for action. Int. J. Obes. 2002, 26, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Chin, S.H.; Kahathuduwa, C.N.; Binks, M. Physical activity and obesity: What we know and what we need to know. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2016, 17, 1226–1244. [Google Scholar] [CrossRef]
- Chiu, C.-H.; Ko, M.-C.; Wu, L.-S.; Yeh, D.-P.; Kan, N.-W.; Lee, P.-F.; Hsieh, J.-W.; Tseng, C.-Y.; Ho, C.-C. Benefits of different intensity of aerobic exercise in modulating body composition among obese young adults: A pilot randomized controlled trial. Health Qual. Life Outcomes 2017, 15, 168. [Google Scholar] [CrossRef]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Blair, S.N.; Cheng, Y.; Scott Holder, J. Is physical activity or physical fitness more important in defining health benefits? Med. Sci. Sport. Exerc. 2001, 33, S379–S399. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, B.W. Bicycle tourism in the South Island of New Zealand: Planning and management issues. Tour. Manag. 1998, 19, 567–582. [Google Scholar] [CrossRef]
- Ritchie, B.W.; Tkaczynski, A.; Faulks, P. Understanding the Motivation and Travel Behavior of Cycle Tourists Using Involvement Profiles. J. Travel Tour. Mark. 2010, 27, 409–425. [Google Scholar] [CrossRef]
- Han, H.; Meng, B.; Kim, W. Bike-traveling as a growing phenomenon: Role of attributes, value, satisfaction, desire, and gender in developing loyalty. Tour. Manag. 2017, 59, 91–103. [Google Scholar] [CrossRef]
- Nordengen, S.; Andersen, L.B.; Solbraa, A.K.; Riiser, A. Cycling is associated with a lower incidence of cardiovascular diseases and death: Part 1—Systematic review of cohort studies with meta-analysis. Br. J. Sport. Med. 2019, 53, 870–878. [Google Scholar] [CrossRef]
- Gazzola, P.; Pavione, E.; Grechi, D.; Ossola, P. Cycle Tourism as a Driver for the Sustainable Development of Little-Known or Remote Territories: The Experience of the Apennine Regions of Northern Italy. Sustainability 2018, 10, 1863. [Google Scholar] [CrossRef] [Green Version]
- Ilieş, D.C.; Herman, G.; Dehoorne, O.; Mǎduţa, F. The role and the importance of Cyclotourism in the development of the Oradea Metropolitan Area (Romania). GeoJ. Tour. Geosites 2013, 12, 101–110. [Google Scholar]
- Watthanaklang, D.; Ratanavaraha, V.; Chatpattananan, V.; Jomnonkwao, S. Measuring the motivation to ride bicycles for tourism through a comparison of tourist attractions. Transp. Policy 2016, 52, 153–163. [Google Scholar] [CrossRef]
- Wulf, C.; Werker, J.; Zapp, P.; Schreiber, A.; Schlör, H.; Kuckshinrichs, W. Sustainable Development Goals as a Guideline for Indicator Selection in Life Cycle Sustainability Assessment. Procedia CIRP 2018, 69, 59–65. [Google Scholar] [CrossRef]
- Scotto di Palumbo, A.; Guerra, E.; Orlandi, C.; Bazzucchi, I.; Sacchetti, M. Effect of combined resistance and endurance exercise training on regional fat loss. J. Sport. Med. Phys. Fit. 2017, 57, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; España-Romero, V.; Vicente-Rodriguez, G.; Martínez-Gómez, D.; Manios, Y.; Béghin, L.; Molnar, D.; Widhalm, K.; Moreno, L.A.; et al. The International Fitness Scale (IFIS): Usefulness of self-reported fitness in youth. Int. J. Epidemiol. 2011, 40, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Oja, P.; Titze, S.; Bauman, A.; de Geus, B.; Krenn, P.; Reger-Nash, B.; Kohlberger, T. Health benefits of cycling: A systematic review. Scand. J. Med. Sci. Sport. 2011, 21, 496–509. [Google Scholar] [CrossRef]
- Nordengen, S.; Andersen, L.B.; Solbraa, A.K.; Riiser, A. Cycling and cardiovascular disease risk factors including body composition, blood lipids and cardiorespiratory fitness analysed as continuous variables: Part 2—Systematic review with meta-analysis. Br. J. Sports Med. 2019, 53, 879–885. [Google Scholar] [CrossRef]
- Hamer, M.; Chida, Y. Active commuting and cardiovascular risk: A meta-analytic review. Prev. Med. 2008, 46, 9–13. [Google Scholar] [CrossRef]
- Kelly, P.; Kahlmeier, S.; Gotschi, T.; Orsini, N.; Richards, J.; Roberts, N.; Scarborough, P.; Foster, C. Systematic review and meta-analysis of reduction in all-cause mortality from walking and cycling and shape of dose response relationship. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Wanner, M.; Gotschi, T.; Martin-Diener, E.; Kahlmeier, S.; Martin, B.W. Active transport, physical activity, and body weight in adults: A systematic review. Am. J. Prev. Med. 2012, 42, 493–502. [Google Scholar] [CrossRef] [Green Version]
- Hochsmann, C.; Meister, S.; Gehrig, D.; Gordon, E.; Li, Y.; Nussbaumer, M.; Rossmeissl, A.; Schafer, J.; Hanssen, H.; Schmidt-Trucksass, A. Effect of E-Bike Versus Bike Commuting on Cardiorespiratory Fitness in Overweight Adults: A 4-Week Randomized Pilot Study. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2018, 28, 255–265. [Google Scholar] [CrossRef]
- Hoj, T.H.; Bramwell, J.J.; Lister, C.; Grant, E.; Crookston, B.T.; Hall, C.; West, J.H. Increasing Active Transportation Through E-Bike Use: Pilot Study Comparing the Health Benefits, Attitudes, and Beliefs Surrounding E-Bikes and Conventional Bikes. JMIR Public Health Surveill. 2018, 4, e10461. [Google Scholar] [CrossRef] [PubMed]
- Vujko, A.; Dragosavac, M.; Kisin, N.; Maksimović, B. The influence of cyclo-tourism on health and economic destination development. Facta Univ. Ser. Phys. Educ. Sport 2017, 15, 227–237. [Google Scholar]
- Malavolti, M.; Mussi, C.; Poli, M.; Fantuzzi, A.L.; Salvioli, G.; Battistini, N.; Bedogni, G. Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21–82 years. Ann. Hum. Biol. 2003, 30, 380–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolezal, B.A.; Lau, M.J.; Abrazado, M.; Storer, T.W.; Cooper, C.B. Validity of two commercial grade bioelectrical impedance analyzers for measurement of body fat percentage. J. Exerc. Physiol. Online 2013, 16, 74. [Google Scholar]
- Ortega, F.B.; Sanchez-Lopez, M.; Solera-Martinez, M.; Fernandez-Sanchez, A.; Sjostrom, M.; Martinez-Vizcaino, V. Self-reported and measured cardiorespiratory fitness similarly predict cardiovascular disease risk in young adults. Scand. J. Med. Sci. Sports 2013, 23, 749–757. [Google Scholar] [CrossRef]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur. J. Appl. Physiol. 2013, 113, 147–155. [Google Scholar] [CrossRef]
- Betella, A.; Verschure, P.F. The Affective Slider: A Digital Self-Assessment Scale for the Measurement of Human Emotions. PLoS ONE 2016, 11, e0148037. [Google Scholar] [CrossRef] [Green Version]
- Peeters, A.; Barendregt, J.J.; Willekens, F.; Mackenbach, J.P.; Mamun, A.A.; Bonneux, L.; The Netherlands Epidemiology and Demography Compression of Morbidity Research Group. Obesity in Adulthood and Its Consequences for Life Expectancy: A Life-Table Analysis. Ann. Intern. Med. 2003, 138, 24–32. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Allison, D.B.; Zannolli, R.; Faith, M.S.; Heo, M.; Pietrobelli, A.; VanItallie, T.B.; Pi-Sunyer, F.X.; Heymsfield, S.B. Weight loss increases and fat loss decreases all-cause mortality rate: Results from two independent cohort studies. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1999, 23, 603–611. [Google Scholar] [CrossRef] [Green Version]
- Wilmore, J.H.; Després, J.-P.; Stanforth, P.R.; Mandel, S.; Rice, T.; Gagnon, J.; Leon, A.S.; Rao, D.; Skinner, J.S.; Bouchard, C. Alterations in body weight and composition consequent to 20 wk of endurance training: The HERITAGE Family Study. Am. J. Clin. Nutr. 1999, 70, 346–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, D.; Karpe, F.; Lafontan, M.; Frayn, K. Physical Activity and Exercise in the Regulation of Human Adipose Tissue Physiology. Physiol. Rev. 2012, 92, 157–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R.; Dagnone, D.; Jones, P.J.; Smith, H.; Paddags, A.; Hudson, R.; Janssen, I. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. A randomized, controlled trial. Ann. Intern. Med. 2000, 133, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Møller, N.C.; Østergaard, L.; Gade, J.R.; Nielsen, J.L.; Andersen, L.B. The effect on cardiorespiratory fitness after an 8-week period of commuter cycling—A randomized controlled study in adults. Prev. Med. 2011, 53, 172–177. [Google Scholar] [CrossRef]
- Peterman, J.E.; Morris, K.L.; Kram, R.; Byrnes, W.C. Pedelecs as a physically active transportation mode. Eur. J. Appl. Physiol. 2016, 116, 1565–1573. [Google Scholar] [CrossRef]
- Srikanthan, P.; Horwich, T.B.; Tseng, C.H. Relation of Muscle Mass and Fat Mass to Cardiovascular Disease Mortality. Am. J. Cardiol. 2016, 117, 1355–1360. [Google Scholar] [CrossRef]
- Compa, F.; Toselli, S.; Mazzilli, M.; Gobbo, L.A.; Coratella, G. Assessment of Body Composition in Athletes: A Narrative Review of Available Methods with Special Reference to Quantitative and Qualitative Bioimpedance Analysis. Nutrients 2021, 13, 1620. [Google Scholar] [CrossRef]
- Christou, D.D.; Gentile, C.L.; DeSouza, C.A.; Seals, D.R.; Gates, P.E. Fatness Is a Better Predictor of Cardiovascular Disease Risk Factor Profile Than Aerobic Fitness in Healthy Men. Circulation 2005, 111, 1904–1914. [Google Scholar] [CrossRef]
- Stevens, J.; Cai, J.; Evenson, K.R.; Thomas, R. Fitness and Fatness as Predictors of Mortality from All Causes and from Cardiovascular Disease in Men and Women in the Lipid Research Clinics Study. Am. J. Epidemiol. 2002, 156, 832–841. [Google Scholar] [CrossRef] [Green Version]
- Barry, V.W.; Baruth, M.; Beets, M.W.; Durstine, J.L.; Liu, J.; Blair, S.N. Fitness vs. Fatness on All-Cause Mortality: A Meta-Analysis. Prog. Cardiovasc. Dis. 2014, 56, 382–390. [Google Scholar] [CrossRef]
- Fogelholm, M. Physical activity, fitness and fatness: Relations to mortality, morbidity and disease risk factors. A systematic review. Obes. Rev. 2010, 11, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Sandvik, L.; Erikssen, J.; Thaulow, E.; Erikssen, G.; Mundal, R.; Rodahl, K. Physical fitness as a predictor of mortality among healthy, middle-aged Norwegian men. N. Engl. J. Med. 1993, 328, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Farrell, S.W.; DeFina, L.F.; Radford, N.B.; Leonard, D.; Barlow, C.E.; Pavlovic, A.; Willis, B.L.; Haskell, W.L.; Lee, I.-M. Relevance of Fitness to Mortality Risk in Men Receiving Contemporary Medical Care. J. Am. Coll. Cardiol. 2020, 75, 1538–1547. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J. Is Active Commuting the Answer to Population Health? Sport. Med. 2008, 38, 751–758. [Google Scholar] [CrossRef] [PubMed]
- WHO. Moving around during the COVID-19 Outbreak. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/technical-guidance/moving-around-during-the-covid-19-outbreak 2020 (accessed on 1 January 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 13) | Men (n = 10) | Women (n = 3) | p | ||||
|---|---|---|---|---|---|---|---|
| Age (Years) | 35.62 | (11.68) | 36.70 | (12.49) | 32.00 | (9.54) | 0.564 |
| Anthropometry and body composition | |||||||
| Body weight (kg) | 75.10 | (14.58) | 80.35 | (12.16) | 57.60 | (3.47) | <0.001 |
| Body mass index (kg/m2) | 23.95 | (2.99) | 24.36 | (3.31) | 22.60 | (0.98) | 0.395 |
| Fat mass (%) | 20.12 | (6.35) | 18.00 | (4.91) | 27.17 | (6.07) | 0.020 |
| Lean mass (%) | 45.09 | (4.13) | 46.67 | (2.69) | 39.83 | (3.97) | 0.005 |
| Physical fitness | |||||||
| General fitness | 2.55 | (0.69) | 2.75 | (0.46) | 2.00 | (1.00) | 0.109 |
| Cardiorespiratory fitness | 2.27 | (0.90) | 2.50 | (0.76) | 1.67 | (1.15) | 0.186 |
| Muscular strength | 2.46 | (0.52) | 2.50 | (0.53) | 2.33 | (0.58) | 0.662 |
| Speed/Agility | 2.36 | (0.81) | 2.38 | (0.52) | 2.33 | (1.53) | 0.967 |
| Flexibility | 1.73 | (0.90) | 1.38 | (0.52) | 2.67 | (1.15) | 0.185 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zúñiga-Moreno, D.; Amaro-Gahete, F.J.; Chillón, P. Bicycle Touring 480 km in Seven Days: Effects on Body Composition and Physical Fitness—A Case Study. Int. J. Environ. Res. Public Health 2022, 19, 2550. https://doi.org/10.3390/ijerph19052550
Zúñiga-Moreno D, Amaro-Gahete FJ, Chillón P. Bicycle Touring 480 km in Seven Days: Effects on Body Composition and Physical Fitness—A Case Study. International Journal of Environmental Research and Public Health. 2022; 19(5):2550. https://doi.org/10.3390/ijerph19052550
Chicago/Turabian StyleZúñiga-Moreno, David, Francisco J. Amaro-Gahete, and Palma Chillón. 2022. "Bicycle Touring 480 km in Seven Days: Effects on Body Composition and Physical Fitness—A Case Study" International Journal of Environmental Research and Public Health 19, no. 5: 2550. https://doi.org/10.3390/ijerph19052550
APA StyleZúñiga-Moreno, D., Amaro-Gahete, F. J., & Chillón, P. (2022). Bicycle Touring 480 km in Seven Days: Effects on Body Composition and Physical Fitness—A Case Study. International Journal of Environmental Research and Public Health, 19(5), 2550. https://doi.org/10.3390/ijerph19052550