
Trimethoprim-Sulfamethoxazole (Bactrim) Dose Optimization in Pneumocystis jirovecii Pneumonia (PCP) Management: A Systematic Review

 ,
,  , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
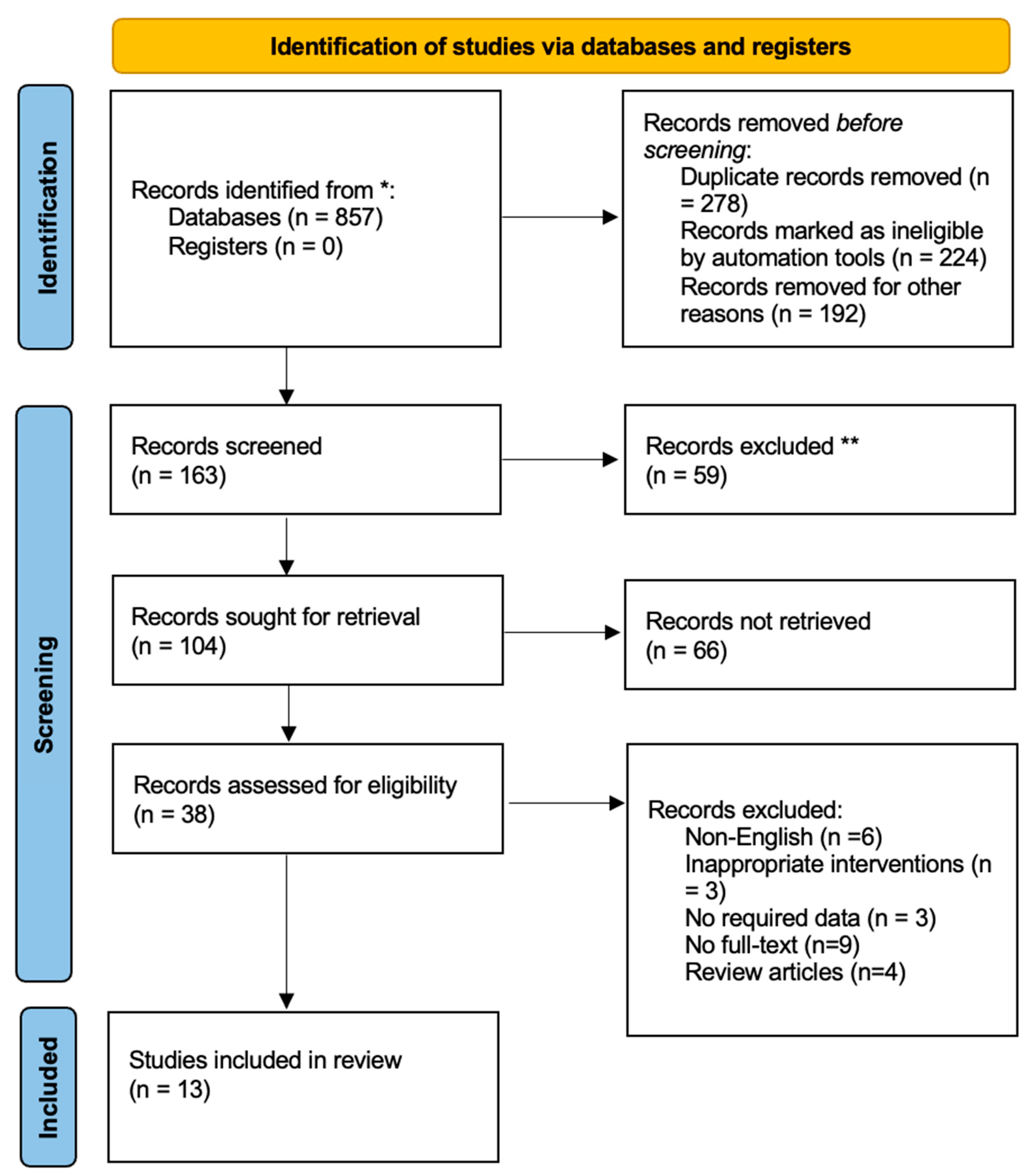
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Selection Criteria and Procedure
2.3. Data Extraction
2.4. Article Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Quality Assessment of Studies
3.3. Dosing Strategy of TMP-SMX in Selected Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, L.; Cattamanchi, A.; Davis, J.L.; den Boon, S.; Kovacs, J.; Meshnick, S.; Miller, R.F.; Walzer, P.D.; Worodria, W.; Masur, H. HIV-associated Pneumocystis pneumonia. Proc. Am. Thorac. Soc. 2011, 8, 294–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, C.F., Jr.; Limper, A.H. Pneumocystis pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef] [PubMed]
- Utsunomiya, M.; Dobashi, H.; Odani, T.; Saito, K.; Yokogawa, N.; Nagasaka, K.; Takenaka, K.; Soejima, M.; Sugihara, T.; Hagiyama, H. Optimal regimens of sulfamethoxazole-trimethoprim for chemoprophylaxis of Pneumocystis pneumonia in patients with systemic rheumatic diseases: Results from a non-blinded, randomized controlled trial. Arthirits Res. Ther. 2017, 19, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Huh, K.H.; Joo, D.J.; Kim, M.S.; Kim, S.I.; Lee, J.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; et al. Risk factors for Pneumocystis jirovecii pneumonia (PJP) in kidney transplantation recipients. Sci. Rep. 2017, 7, 1571. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Tang, Z.; Liu, F.; Yang, M. Efficacy and safety of trimethoprim-sulfamethoxazole for the prevention of Pneumocystis pneumonia in human immunodeficiency virus-negative immunodeficient patients: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0248524. [Google Scholar] [CrossRef]
- White, P.L.; Price, J.S.; Backx, M. Therapy and management of Pneumocystis jirovecii infection. J. Fungi 2018, 4, 127. [Google Scholar] [CrossRef] [Green Version]
- Autmizguine, J.; Melloni, C.; Hornik, C.P.; Dallefeld, S.; Harper, B.; Yogev, R.; Sullivan, J.E.; Atz, A.M.; Al-Uzri, A.; Mendley, S.; et al. Population Pharmacokinetics of Trimethoprim-Sulfamethoxazole in Infants and Children. Antimicrob. Agents Chemother. 2017, 62, e01813-17. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W.; Curtis, J.R.; Moon, J.; Song, Y.W.; Kim, S.; Lee, E.B. Prophylactic effect of trimethoprim-sulfamethoxazole for Pneumocystis pneumonia in patients with rheumatic diseases exposed to prolonged high-dose glucocorticoids. Ann. Rheum. Dis. 2018, 77, 644–649. [Google Scholar] [CrossRef]
- Hughes, W.T.; Feldman, S.; Aur, R.J.; Verzosa, M.S.; Hustu, H.O. Intensity of immunosuppressive therapy and the incidence of Pneumocystis carinii pneumonitis. Cancer 1975, 36, 2004–2009. [Google Scholar] [CrossRef]
- Nazir, H.F.; Elshinawy, M.; AlRawas, A.; Khater, D.; Zadjaly, S.; Wali, Y. Efficacy and Safety of Dapsone Versus Trimethoprim/Sulfamethoxazol for Pneumocystis jirovecii Prophylaxis in Children with Acute Lymphoblastic Leukemia with a Background of Ethnic Neutropenia. J. Pediatr. Hematol. Oncol. 2017, 39, 203–208. [Google Scholar] [CrossRef]
- Brown, G.R. Cotrimoxazole—Optimal dosing in the critically ill. Ann. Intensive Care 2014, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhifany, A.A.; Alqurashi, A.F.; Al-Agamy, M.H.; Alkhushaym, N.; Alhomoud, F.; Alhomoud, F.K.; Almangour, T.A. Employment of mapping technology in antimicrobial resistance reporting in Saudi Arabia. Geospatial Health 2020, 15, 1. [Google Scholar] [CrossRef]
- Creemers-Schild, D.; Kroon, F.P.; Kuijper, E.J.; de Boer, M.G.J. Treatment of Pneumocystis pneumonia with intermediate-dose and step-down to low-dose trimethoprim-sulfamethoxazole: Lessons from an observational cohort study. Infection 2016, 44, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Sattler, F.R.; Cowan, R.; Nielsen, D.M.; Ruskin, J. Trimethoprim-sulfamethoxazole compared with pentamidine for treatment of Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome: A prospective, noncrossover study. Ann. Intern. Med. 1988, 109, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Medina, I.; Mills, J.; Leoung, G.; Hopewell, P.C.; Lee, B.; Modin, G.; Benowitz, N.; Wofsy, C.B. Oral therapy for Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome: A controlled trial of trimethoprim—Sulfamethoxazole versus trimethoprim—Dapsone. N. Eng. J. Med. 1990, 323, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.C.; Duncanson, F.P.; Lenox, T.H.; Forszpaniak, C.; Sherer, C.B.; Quentzel, H.; Nunez, M.; Suarez, M.; Kawwaff, O.; Pitta-Alvarez, A. Trimethoprim-sulfamethoxazole versus pentamidine for Pneumocystis carinii pneumonia in AIDS patients: Results of a large prospective randomized treatment trial. AIDS 1992, 6, 301–305. [Google Scholar] [CrossRef]
- Safrin, S.; Finkelstein, D.M.; Feinberg, J.; Frame, P.; Simpson, G.; Wu, A.; Cheung, T.; Soiero, R.; Hojczyk, P.; Black, J.R. Comparison of three regimens for treatment of mild to moderate Pneumocystis carinii pneumonia in patients with AIDS: A double-blind, randomized trial of oral trimethoprim-sulfamethoxazole, dapsone-trimethoprim, and clindamycin-primaquine. Ann. Intern. Med. 1996, 124, 792–802. [Google Scholar] [CrossRef]
- Chang, H.-M.; Tsai, H.-C.; Lee, S.S.-J.; Kunin, C.; Lin, P.-C.; Wann, S.-R.; Chen, Y.-S. High daily doses of trimethoprim/sulfamethoxazole are an independent risk factor for adverse reactions in patients with Pneumocystis pneumonia and AIDS. J. Chin. Med. Assoc. 2016, 79, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Haseeb, A.; Faidah, H.S.; Alghamdi, S.; Alotaibi, A.F.; Elrggal, M.E.; Mahrous, A.J.; Almarzoky Abuhussain, S.S.; Obaid, N.A.; Algethamy, M.; AlQarni, A. Dose Optimization of Colistin: A Systematic Review. Antibiotics 2021, 10, 1454. [Google Scholar] [CrossRef]
- Haseeb, A.; Faidah, H.S.; Al-Gethamy, M.; Iqbal, M.S.; Alhifany, A.A.; Ali, M.; Abuhussain, S.S.A.; Elrggal, M.E.; Almalki, W.H.; Alghamdi, S. Evaluation of Antimicrobial Stewardship Programs (ASPs) and their perceived level of success at Makkah region hospitals, Kingdom of Saudi Arabia. Saudi Pharm. J. 2020, 28, 1166–1171. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Connell, D.; Peterson, J.; Welch, V.; Losos, M. Newcastle-Ottawa Quality Assessment Scale Cohort Studies; University of Ottawa: Ottawa, ON, Canada, 2014; Volume 18, pp. 205–228. [Google Scholar]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. Cohrane Database Syst. Rev. 2019, 205–228. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Dao, B.D.; Barreto, J.N.; Wolf, R.C.; Dierkhising, R.A.; Plevak, M.F.; Tosh, P.K. Serum peak sulfamethoxazole concentrations demonstrate difficulty in achieving a target range: A retrospective cohort study. Curr. Ther. Res. 2014, 76, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Ohmura, S.-I.; Naniwa, T.; Tamechika, S.-Y.; Miyamoto, T.; Shichi, D.; Kazawa, N.; Iwagaitsu, S.; Maeda, S.; Wada, J.-I.; Niimi, A. Effectiveness and safety of lower dose sulfamethoxazole/trimethoprim therapy for Pneumocystis jirovecii pneumonia in patients with systemic rheumatic diseases: A retrospective multicenter study. BMC Infect. Dis. 2019, 25, 253–261. [Google Scholar] [CrossRef]
- Yamashita, K.; Shimomura, Y.; Ikesue, H.; Muroi, N.; Yoshimoto, A.; Hashida, T. Safety and efficacy evaluation of low-dose trimethoprim-sulfamethoxazole for prophylaxis of Pneumocystis pneumonia in HIV uninfected patients undergoing hemodialysis: A retrospective observational study. J. Infect. Chemother. 2021, 21, 664. [Google Scholar] [CrossRef]
- Kosaka, M.; Ushiki, A.; Ikuyama, Y.; Hirai, K.; Matsuo, A.; Hachiya, T.; Hanaoka, M. A four-center retrospective study of the efficacy and toxicity of low-dose trimethoprim-sulfamethoxazole for the treatment of Pneumocystis pneumonia in patients without HIV infection. Antimicrob. Agents Chemother. 2017, 61, e01173-17. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, K.; Aoshima, M.; Nakashita, T.; Hara, M.; Otsuki, A.; Noma, S.; Misawa, M.; Otsuka, Y.; Motojima, S. Low-dose trimethoprim-sulfamethoxazole treatment for Pneumocystis pneumonia in non-human immunodeficiency virus-infected immunocompromised patients: A single-center retrospective observational cohort study. J. Microb. Immunol. Infect. 2018, 51, 810–820. [Google Scholar] [CrossRef]
- Prasad, G.R.; Beckley, J.; Mathur, M.; Gunasekaran, M.; Nash, M.M.; Rapi, L.; Huang, M.; Zaltzman, J.S. Safety and efficacy of prophylaxis for Pneumocystis jirovecii pneumonia involving trimethoprim-sulfamethoxazole dose reduction in kidney transplantation. BMC Infect. Dis. 2019, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Rehman, U.; Farhan, K.; Shahnawaz, W.; Khalid, M.Z.; Neupane, K.J.C. A Rare Case of Pneumocystis Pneumonia in HIV Patient on Glucocorticoid. Cureus 2021, 13, e14445. [Google Scholar] [CrossRef]
- Lu, Y.-W.; Chen, T.-C. Use of trimethoprim-sulfamethoxazole in a patient with G6PD deficiency for treating Pneumocystis jirovecii pneumonia without haemolysis: Case report and literature review. J. Clin. Pharm. Ther. 2020, 45, 1483–1485. [Google Scholar] [CrossRef]
- Utsunomiya, M.; Dobashi, H.; Odani, T.; Saito, K.; Yokogawa, N.; Nagasaka, K.; Takenaka, K.; Soejima, M.; Sugihara, T.; Hagiyama, H. An open-label, randomized controlled trial of sulfamethoxazole–trimethoprim for Pneumocystis prophylaxis: Results of 52-week follow-up. Rheumatol. Adv. Pract. 2020, 4, rkaa029. [Google Scholar] [CrossRef] [PubMed]
- Zmarlicka, M.; Martin, S.T.; Cardwell, S.M.; Nailor, M.D. Tolerability of low-dose sulfamethoxazole/trimethoprim for Pneumocystis jirovecii pneumonia prophylaxis in kidney transplant recipients. Prog. Transplant. 2015, 25, 210–216. [Google Scholar] [CrossRef]
- Park, J.W.; Curtis, J.R.; Kim, M.J.; Lee, H.; Song, Y.W.; Lee, E.B. Pneumocystis pneumonia in patients with rheumatic diseases receiving prolonged, non-high-dose steroids—Clinical implication of primary prophylaxis using trimethoprim–sulfamethoxazole. Arthritis Resp. Ther. 2019, 21, 207. [Google Scholar] [CrossRef] [Green Version]
- Maschmeyer, G.; Helweg-Larsen, J.; Pagano, L.; Robin, C.; Cordonnier, C.; Schellongowski, P.; on behalf of the 6th European Conference on Infections in Leukemia (ECIL-6), a joint venture of The European Group for Blood and Marrow Transplantation (EBMT), The European Organization for Research and Treatment of Cancer (EORTC), the International Immunocompromised Host Society (ICHS) and The European LeukemiaNet (ELN). ECIL guidelines for treatment of Pneumocystis jirovecii pneumonia in non-HIV-infected haematology patients. J. Antimicrob. Chemother. 2016, 71, 2405–2413. [Google Scholar] [CrossRef]
- Schmajuk, G.; Jafri, K.; Evans, M.; Shiboski, S.; Gianfrancesco, M.; Izadi, Z.; Patterson, S.L.; Aggarwal, I.; Sarkar, U.; Dudley, R.A. Pneumocystis jirovecii pneumonia (PJP) prophylaxis patterns among patients with rheumatic diseases receiving high-risk immunosuppressant drugs. in Seminars in arthritis and rheumatism. Semin. Arthritis Rheum. 2019, 48, 1087–1092. [Google Scholar] [CrossRef]
- Di Cocco, P.; Orlando, G.; Bonanni, L.; D’Angelo, M.; Clemente, K.; Greco, S.; Gravante, G.; Madeddu, F.; Scelzo, C.; Famulari, A. A systematic review of two different trimetoprim–sulfamethoxazole regimens used to prevent Pneumocystis jirovecii and no prophylaxis at all in transplant recipients: Appraising the evidence. Transplant. Proc. 2009, 41, 1201–1203. [Google Scholar] [CrossRef]
- Sadiq, U.; Shrestha, U.; Guzman, N. Prevention of Opportunistic Infections in HIV; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Haseeb, A.; Faidah, H.S.; Algethamy, M.; Alghamdi, S.; Alhazmi, G.A.; Alshomrani, A.O.; Alqethami, B.R.; Alotibi, H.S.; Almutiri, M.Z.; Almuqati, K.S. Antimicrobial Usage and Resistance in Makkah Region Hospitals: A Regional Point Prevalence Survey of Public Hospitals. Int. J. Environ. Res. Public Health 2022, 19, 254. [Google Scholar] [CrossRef]
- Martin, S.; Fishman, J.; the AST Infectious Diseases Community of Practice. Pneumocystis pneumonia in solid organ transplantation. Am. J. Transplant. 2013, 13, 272–279. [Google Scholar] [CrossRef]
- Urbancic, K.F.; Ierino, F.; Phillips, E.; Mount, P.F.; Mahony, A.; Trubiano, J.A. Taking the challenge: A protocolized approach to optimize Pneumocystis pneumonia prophylaxis in renal transplant recipients. Am. J. Transplant. 2018, 18, 462–466. [Google Scholar] [CrossRef] [Green Version]
- Justin, R.; Hofmann, D. Prevention of Opportunistic Infections (OI) in Patients with HIV Infection. JAIDS J. Acquir. Immune Defic. Syndr. 2021, 12, 38–45. [Google Scholar]
- Rodriguez, M.; Fishman, J.A. Prevention of infection due to Pneumocystis spp. in human immunodeficiency virus-negative immunocompromised patients. Clin. Microbiol. Rev. 2004, 17, 770–782. [Google Scholar] [CrossRef] [Green Version]
- Iriart, X.; Bouar, M.L.; Kamar, N.; Berry, A. Pneumocystis Pneumonia in Solid-Organ Transplant Recipients. J. Fungi 2015, 1, 293–331. [Google Scholar] [CrossRef] [Green Version]
- Butler-Laporte, G.; Smyth, E.; Amar-Zifkin, A.; Cheng, M.P.; McDonald, E.G.; Lee, T.C. Low-Dose TMP-SMX in the Treatment of Pneumocystis jirovecii Pneumonia: A Systematic Review and Meta-analysis. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Haseeb, A.; Faidah, H.S.; Al-Gethamy, M.; Iqbal, M.S.; Barnawi, A.M.; Elahe, S.S.; Bukhari, D.N. Evaluation of a Multidisciplinary Antimicrobial Stewardship Program in a Saudi Critical Care Unit: A Quasi-Experimental Study. Front. Pharmacol. 2021, 11, 2222. [Google Scholar] [CrossRef]
- Harigai, M.; Koike, R.; Miyasaka, M. Pneumocystis pneumonia associated with infliximab in Japan. N. Engl. J. Med. 2007, 357, 1874–1876. [Google Scholar] [CrossRef]
- Katsuyama, T.; Saito, K.; Kubo, S.; Nawata, M.; Tanaka, Y. Prophylaxis for Pneumocystis pneumonia in patients with rheumatoid arthritis treated with biologics, based on risk factors found in a retrospective study. Arthritis Res. Ther. 2014, 16, R43. [Google Scholar] [CrossRef] [Green Version]
- Lehman, J.S.; Gonzalez Santiago, T.M.; Wetter, D.A.; Kalaaji, A.N.; Limper, A.H. Weighing the risks and benefits of Pneumocystis pneumonia prophylaxis in iatrogenically immunosuppressed dermatology patients. Int. J. Dermatol. 2017, 56, e5–e6. [Google Scholar] [CrossRef]
- Wolfe, R.M.; Peacock, J.E., Jr. Pneumocystis Pneumonia and the Rheumatologist: Which Patients Are At Risk and How Can PCP Be Prevented? Curr. Rheumatol. Rep. 2017, 19, 35. [Google Scholar] [CrossRef]


{kind=link}
| Author and Year | Design | Sample Size | Characteristics of Patients | Dosing Regimen | Clinical Outcomes | Findings |
|---|---|---|---|---|---|---|
| Dao et al., 2014 [25] | Retrospective Cohort study | 305 | Patients with PCP infection | Group A received low-dose TMP-SMX regimen (TMP o15 mg/kg/day) while Group B received high-dose regimen (TMP 415 mg/kg/day) | In low-dose group, 32% of the patients were found to be within therapeutic range while in high-dose group, 22% of the patients were in therapeutic range | Furthers studies are required on large-scale to monitor plasma concentration of SMX and to evaluate the clinical outcomes. |
| Ohmura et al., 2018 [26] | Retrospective study | 81 | Patients with systemic rheumatoid diseases | Group A received low-dose SMX-TMP: ≤10 mg/kg/day; Group B received the intermediate dose, 10–15 mg/kg/day; Group C received high and conventional dose, 15–20 mg/kg/day for TMP dose. | The survival rate of Group A, B and C were 100%, 93.3%, and 96.7%, respectively. | Low-dose SMX/TMP treatment with ≤10 mg/kg/day for TMP was as safe and effective as high-dose regimen for occurrence and recurrence of PCP. |
| Yamashita et al., 2021 [27] | Retrospective study | 81 | Patients with HIV | Group A: standard-dose (≥6 SS (TMP-SMX 80 mg/400 mg tablets/week) Group B: low-dose groups (<6 SS tablets/week). | PCP was not developed in any patients during study period | Low-dose TMP-SMX is optimal treatment option to treat and prevent PCP |
| Schild et al., 2015 [13] | Observational Cohort study | 104 | Patients with PCPs in various immune dysfunctions | Patients received intermediate-dose TMP–SMX (TMP 10–15 mg/kg/day) and reduced to low-dose TMP–SMX (TMP 4–6 mg/kg/day) during therapy. | 23% of patients were switched to low-dose TMP–SMX in step-down group compared to intermediate dose group | A step-down strategy to low-dose TMP–SMX also reported to be effective and safe |
| Kosaka et al., 2017 [28] | Retrospective cohort study | 82 | Patients with non-HIV-PCP | Group A received conventional dose of TMP (15 to 20 mg/kg), Group B received a low dose of TMP <15 mg/kg | The mortality rates were 25.0% in conventional-dose group and 19.5% in low-dose groups | The low-dose regimen is well tolerated and results in fewer adverse effects |
| Nakashima et al., 2018 [29] | Retrospective cohort study | 24 | Patients with non-HIV-PCP | Patients received low-dose TMP-SMX (TMP, 4e10 mg/kg/day; SMX, 20–50 mg/kg/day and conventional dose TMP-SMX (TMP, 10–20 mg/kg/day; SMX, 50–100 mg/kg/day) was used as reference | The total adverse reaction rate was 58.3% and 72.4% in low-dose group and conventional-dose group | Low-dose TMP-SMX may be considered as better treatment option for patients with non-HIV PCP |
| Prasad et al., 2019 [30] | Retrospective study | 438 | Kidney transplant recipients | SS dose of TMP-SMX OD, thrice daily and twice daily | The dose was reduced in 84 patients who experienced hyperkalemia and 102 patients who experienced leukopenia | TMP-SMX dose reduction is frequent in the first post-transplant year, but PCP does not occur |
| Rehman et al., 2021 [31] | Case report | 01 | Patient with CAP | - | Respiratory condition improved on day 9 | Early diagnosis and management with TMP-SMX can lead to a better prognosis for patient |
| Lu et al., 2020 [32] | Case report | 01 | Patients with G6PD | TMP-SMZ (240/1200 mg) every 8 h, given IV. On day 16, PO (240/1200 mg) TID for 5 days | TMP-SMX reported to cause hemolysis in patients | Successfully treated with PCP with high dose of TMP-SMZ without any symptoms. |
| Park et al., 2021 [35] | Retrospective cohort study | 1092 | Patients with PCP and rheumatoid arthritis | one SS tablet of TMP-SMX (400/80 mg) per day for prophylaxis | TMP-SMX reduced 1 year PCP incidence and related mortality | TMP-SMX prophylaxis significantly decreased the incidence of the PCP with a favorable safety profile in a patient with RA taking steroids |
| Utsunomiya et al., 2017 [3] | RCT | 183 | Patients with systemic Rheumatoid diseases | SS group (SMX-TMP of 400/80 mg daily). HS group (200/40 mg/day) ES group (initiated with 40/8 mg/day, increasing to 200/40 mg/day) | No cases of PCP were reported up to week 24 | The daily HS regimen is deemed to be first-line treatment option for the prophylaxis of PCP in patients with rheumatic disorders |
| Utsunomiya et al., 2020 [33] | RCT | 183 | Patients with rheumatoid diseases | SS group (SMX-TMP 400/80 mg/day), HS group (200/40 mg/day) ES group (initiating at 40/8 mg/day) and increasing to 200/40 mg/day) | PCP did not develop in any of the patients by week 52 | SMX-TMP 200 mg/40 mg might provide a favourable benefit-risk balance in PCP prophylaxis. |
| Zamarlicha et al., 2015 [34] | Retrospective cohort study | 88 | Kidney transplant recipient | SMX-TMP dosed at 1 single-strength tablet thrice weekly | SMX-TMP therapy was discontinued in 10 patients while 11 patients received atovaquone. | A low-dose SMX-TMP regimen of 1 SS tablet thrice weekly is safe and effective. |
| Selection | Comparability | Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|
| Reference | Representative of Exposed Studies A | Selection of Non-Exposed B | Ascertainment of Exposure C | Demonstration of Outcome D | Comparability of Cohort Studies on Basis of Design E | Assessment of Outcomes F | Adequacy of Follow-up G | Quality Score |
| Dao et al., 2014 [25] | * | * | * | * | * | ** | * | 8 |
| Ohmura et al., 2018 [26] | * | * | * | * | * | * | * | 7 |
| Yamashita et al., 2021 [27] | * | * | * | * | * | * | * | 7 |
| Schild et al., 2016 [13] | * | * | * | * | * | * | - | 6 |
| Kosaka et al., 2017 [28] | * | * | * | * | * | ** | - | 7 |
| Nakashima et al., 2017 [29] | * | * | * | * | * | ** | - | 7 |
| Prasad et al., 2019 [30] | * | * | * | * | * | ** | * | 8 |
| Park et al., 2021 [35] | * | * | * | * | * | ** | * | 8 |
| Zmarlicha et al., 2015 [34] | * | * | * | * | * | ** | * | 8 |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Utsunomiya et al., 2017 [3] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Unclear |
| Utsunomiya et al., 2020 [33] | Low risk | Low risk | Low risk | Low risk | Unclear | Low risk | Unclear |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haseeb, A.; Abourehab, M.A.S.; Almalki, W.A.; Almontashri, A.M.; Bajawi, S.A.; Aljoaid, A.M.; Alsahabi, B.M.; Algethamy, M.; AlQarni, A.; Iqbal, M.S.; et al. Trimethoprim-Sulfamethoxazole (Bactrim) Dose Optimization in Pneumocystis jirovecii Pneumonia (PCP) Management: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 2833. https://doi.org/10.3390/ijerph19052833
Haseeb A, Abourehab MAS, Almalki WA, Almontashri AM, Bajawi SA, Aljoaid AM, Alsahabi BM, Algethamy M, AlQarni A, Iqbal MS, et al. Trimethoprim-Sulfamethoxazole (Bactrim) Dose Optimization in Pneumocystis jirovecii Pneumonia (PCP) Management: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(5):2833. https://doi.org/10.3390/ijerph19052833
Chicago/Turabian StyleHaseeb, Abdul, Mohammed A. S. Abourehab, Wesam Abdulghani Almalki, Abdulrahman Mohammed Almontashri, Sultan Ahmed Bajawi, Anas Mohammed Aljoaid, Bahni Mohammed Alsahabi, Manal Algethamy, Abdullmoin AlQarni, Muhammad Shahid Iqbal, and et al. 2022. "Trimethoprim-Sulfamethoxazole (Bactrim) Dose Optimization in Pneumocystis jirovecii Pneumonia (PCP) Management: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 5: 2833. https://doi.org/10.3390/ijerph19052833
APA StyleHaseeb, A., Abourehab, M. A. S., Almalki, W. A., Almontashri, A. M., Bajawi, S. A., Aljoaid, A. M., Alsahabi, B. M., Algethamy, M., AlQarni, A., Iqbal, M. S., Mutlaq, A., Alghamdi, S., Elrggal, M. E., Saleem, Z., Radwan, R. M., Mahrous, A. J., & Faidah, H. S. (2022). Trimethoprim-Sulfamethoxazole (Bactrim) Dose Optimization in Pneumocystis jirovecii Pneumonia (PCP) Management: A Systematic Review. International Journal of Environmental Research and Public Health, 19(5), 2833. https://doi.org/10.3390/ijerph19052833