
Young Adult Carers during the Pandemic: The Effects of Parental Illness and Other Ill Family Members on COVID-19-Related and General Mental Health Outcomes





Abstract
:1. Introduction
The Present Study
2. Materials and Methods
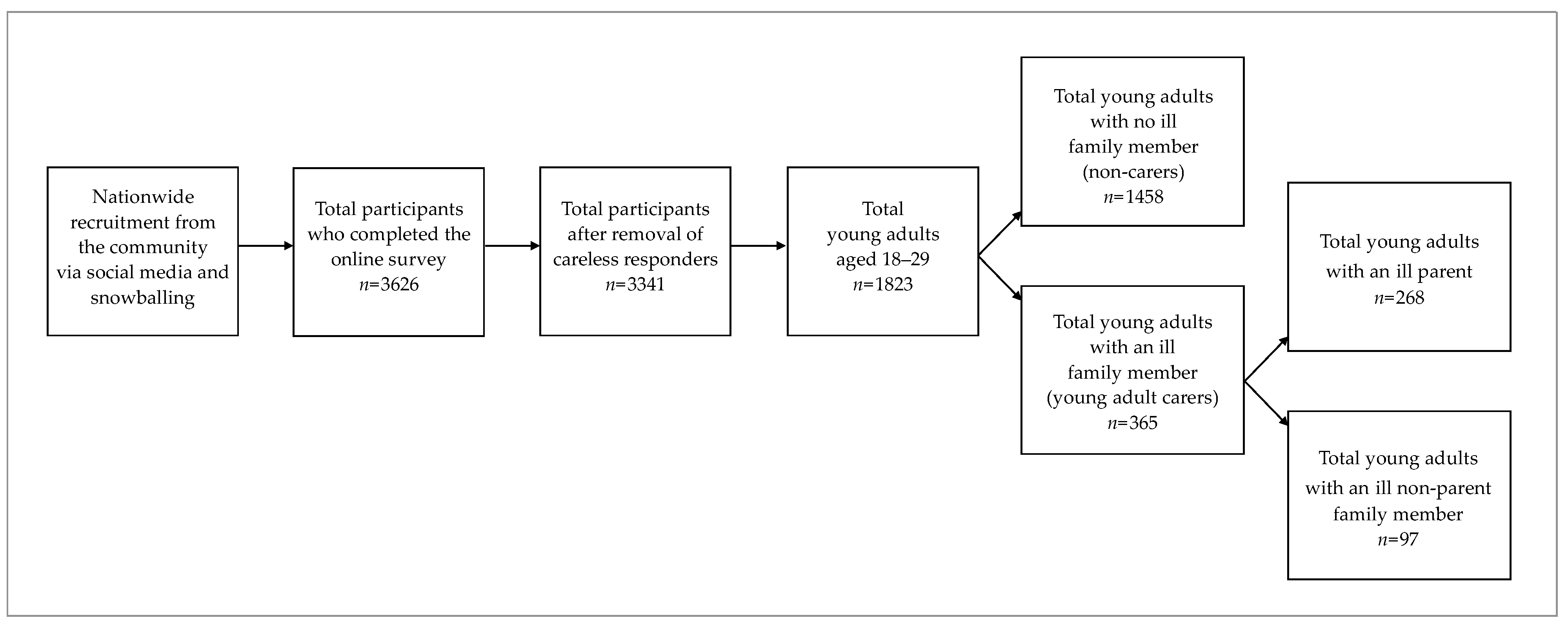
2.1. Participants and Recruitment Procedure
2.2. Measures
2.2.1. Socio-Demographics
2.2.2. Family Caregiving Status
2.2.3. COVID-19 and Lockdown Context Variables
2.2.4. COVID-19-Related Mental Health Outcomes
Risky Health Behaviors
Loneliness
Increase in Home Violence
Fear of COVID-19
2.2.5. General Mental Health Outcomes
Anxiety
Depression
Wellbeing
2.3. Data Analysis Approach
3. Results
3.1. Preliminary Analyses
3.1.1. Sample Characteristics
3.1.2. Mental Health Descriptive Data
3.2. Correlations between COVID-19 Context Variables and Mental Health Outcomes
3.3. Differences in Mental Health Outcomes among Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dharampal, R.; Ani, C. The emotional and mental health needs of young carers: What psychiatry can do. BJPsych Bull. 2020, 44, 112–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sieh, D.S.; Meijer, A.M.; Oort, F.J.; Visser-Meily, J.M.A.; Van der Leij, D.A.V. Problem behavior in children of chronically ill parents: A meta-analysis. Clin. Child Fam. Psychol. Rev. 2010, 13, 384–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, G.; Andreozzi, M.S.; Pakenham, K.I.; Grandi, S.; Tossani, E. Psychosocial adjustment of young offspring in the context of parental type 1 and type 2 diabetes: A systematic review. Diabet. Med. 2020, 37, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Duzen, A.; Patterson, P.; McDonald, F.E.J.; Crocetti, E.; Grandi, S.; Tossani, E. Illness unpredictability and psychosocial adjustment of adolescent and young adults impacted by parental cancer: The dediating role of unmet needs. Support. Care Cancer 2022, 30, 145–155. [Google Scholar] [CrossRef]
- van der Werf, H.M.; Luttik, M.L.A.; de Boer, A.; Roodbol, P.F.; Paans, W. Growing up with a chronically ill family member—The impact on and support needs of young adult carers: A scoping review. Int. J. Environ. Res. Public. Health 2022, 19, 855. [Google Scholar] [CrossRef]
- Arnett, J.J.; Žukauskienė, R.; Sugimura, K. The new life stage of emerging adulthood at ages 18–29 years: Implications for mental health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef]
- Ali, L.; Ahlström, B.H.; Krevers, B.; Skärsäter, I. Daily life for young adults who care for a person with mental illness: A qualitative study. J. Psychiatr. Ment. Health Nurs. 2012, 19, 610–617. [Google Scholar] [CrossRef]
- Haugland, B.S.M.; Hysing, M.; Sivertsen, B. The burden of care: A national survey on the prevalence, demographic characteristics and health problems among young adult carers attending higher education in Norway. Front. Psychol. 2020, 10, 2859. [Google Scholar] [CrossRef] [Green Version]
- Moberg, J.Y.; Larsen, D.; Brødsgaard, A. Striving for balance between caring and restraint: Young adults’ experiences with parental multiple sclerosis. J. Clin. Nurs. 2017, 26, 1363–1374. [Google Scholar] [CrossRef]
- Knopf, L.; Wazinski, K.; Wanka, A.; Hess, M. Caregiving students: A systematic literature review of an under-researched group. J. Furth. High. Educ. 2022, 1–14. [Google Scholar] [CrossRef]
- Greene, J.; Cohen, D.; Siskowski, C.; Toyinbo, P. The relationship between family caregiving and the mental health of emerging young adult caregivers. J. Behav. Health Serv. Res. 2017, 44, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Pakenham, K.I.; Boccolini, G.; Grandi, S.; Tossani, E. Health anxiety and mental health outcome during the COVID-19 lockdown in Italy: The mediating and moderating roles of psychological flexibility. Front. Psychol. 2020, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Landi, G.; Boccolini, G.; Furlani, A.; Grandi, S.; Tossani, E. The moderating roles of psychological flexibility and inflexibility on the mental health impacts of the COVID-19 pandemic and lockdown in Italy. J. Context. Behav. Sci. 2020, 17, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Grossman-Giron, A.; Bitan, D.T.; Mikulincer, M.; Grandi, S.; Tossani, E. Mental pain, psychological distress, and suicidal ideation during the COVID-19 emergency: The moderating role of tolerance for mental pain. Int. J. Ment. Health Addict. 2021, 1–12. [Google Scholar] [CrossRef]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.W.L.; Haines, J.; on behalf of the Guelph Family Health Study. The impact of COVID-19 on health behavior, stress, financial and food security among middle to high income Canadian families with young children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef]
- King, T.L. Young carers in the COVID-19 pandemic: Risks for mental health. Lancet Reg. Health West. Pac. 2021, 16, 100307. [Google Scholar] [CrossRef]
- Mak, H.W.; Fluharty, M.; Fancourt, D. Predictors and impact of arts engagement during the COVID-19 pandemic: Analyses of data from 19,384 adults in the COVID-19 Social Study. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Rodrigues, R.; Simmons, C.; Schmidt, A.E.; Steiber, N. Care in times of COVID-19: The impact of the pandemic on informal caregiving in Austria. Eur. J. Ageing 2021, 18, 195–205. [Google Scholar] [CrossRef]
- Blake-Holmes, K.; McGowan, A. ‘It’s Making His Bad Days into My Bad Days’: The impact of Coronavirus social distancing measures on young carers and young adult carers in the United Kingdom. Child Fam. Soc. Work 2022, 27, 22–29. [Google Scholar] [CrossRef]
- Becker, S. Global Perspectives on children’s unpaid caregiving in the family: Research and policy on ‘young carers’ in the UK, Australia, the USA and Sub-Saharan Africa. Glob. Soc. Policy 2007, 7, 23–50. [Google Scholar] [CrossRef] [Green Version]
- Hooper, L. Expanding the discussion regarding parentification and its varied outcomes: Implications for mental health research and practice. J. Ment. Health Couns. 2007, 29, 322–337. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Bursnall, S.; Chiu, J.; Cannon, T.; Okochi, M. The psychosocial impact of caregiving on young people who have a parent with an illness or disability: Comparisons between young caregivers and noncaregivers. Rehabil. Psychol. 2006, 51, 113–126. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Cox, S. The effects of parental illness and other ill family members on youth caregiving experiences. Psychol. Health 2015, 30, 857–878. [Google Scholar] [CrossRef] [Green Version]
- Landi, G.; Pakenham, K.I.; Crocetti, E.; Grandi, S.; Tossani, E. Examination of the tripartite model of youth caregiving in the context of parental illness. Psychol. Health 2022, 37, 397–418. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Cox, S. The effects of parental illness and other ill family members on the adjustment of children. Ann. Behav. Med. 2014, 48, 424–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boumans, N.P.G.; Dorant, E. A cross-sectional study on experiences of young adult carers compared to young adult noncarers: Parentification, coping and resilience. Scand. J. Caring Sci. 2018, 32, 1409–1417. [Google Scholar] [CrossRef]
- Landi, G.; Boccolini, G.; Giovagnoli, S.; Pakenham, K.I.; Grandi, S.; Tossani, E. Validation of the Italian Young Carer of Parents Inventory-Revised (YCOPI-R). Disabil. Rehabil. 2022, 44, 795–806. [Google Scholar] [CrossRef]
- Smriti, D.; Ambulkar, S.; Meng, Q.; Kaimal, G.; Ramotar, K.; Park, S.Y.; Huh-Yoo, J. Creative arts therapies for the mental health of emerging adults: A systematic review. Arts Psychother. 2022, 77, 101861. [Google Scholar] [CrossRef]
- Shamon, H.; Berning, C.C. Attention check items and instructions in online surveys with incentivized and non-incentivized samples: Boon or bane for data quality? Surv. Res. Methods 2020, 14, 55–77. [Google Scholar] [CrossRef]
- Fullana, M.A.; Hidalgo-Mazzei, D.; Vieta, E.; Radua, J. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. J. Affect. Disord. 2020, 275, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Bovo, C.; Sanchis-Gomar, F. Health risks and potential remedies during prolonged lockdowns for Coronavirus disease 2019 (COVID-19). Diagnosis 2020, 7, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Boffo, M. Exploratory structure equation Mmdeling of the UCLA Loneliness Scale: A contribution to the Italian adaptation. TPM-Test. Psychom. Methodol. Appl. Psychol. 2012, 345–363. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A short scale for measuring loneliness in large surveys. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–10. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L. Instruction Manual: Instructions for Patient Health Questionnaire (PHQ) and GAD-7 Measures. Available online: www.phqscreeners.com (accessed on 9 March 2020).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Mazzotti, E.; Fassone, G.; Picardi, A.; Sagoni, E.; Ramieri, L.; Lega, I.; Camaioni, D.; Abeni, D.; Pasquini, P. II Patient Health Questionnaire (PHQ) per lo screening dei disturbi psichiatrici: Uno studio di validazione nei confronti della Intervista Clinica Strutturata per il DSM-IV asse I (SCID-I). Ital. J. Psychopathol. 2003, 9, 235–242. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Can. Med. Assoc. J. 2012, 184, E191–E196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrillo, G.; Capone, V.; Caso, D.; Keyes, C.L.M. The Mental Health Continuum–Short Form (MHC–SF) as a measure of well-being in the Italian context. Soc. Indic. Res. 2015, 121, 291–312. [Google Scholar] [CrossRef]
- Keyes, C.L.M.; Wissing, M.; Potgieter, J.P.; Temane, M.; Kruger, A.; van Rooy, S. Evaluation of the Mental Health Continuum–Short Form (MHC–SF) in Setswana-speaking South Africans. Clin. Psychol. Psychother. 2008, 15, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. The Mental Health Continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [Green Version]
- Lamers, S.M.A.; Westerhof, G.J.; Bohlmeijer, E.T.; ten Klooster, P.M.; Keyes, C.L.M. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (MHC-SF). J. Clin. Psychol. 2011, 67, 99–110. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017; pp. 1998–2018. [Google Scholar]
- Little, R.J.A. A Test of Missing Completely at Random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Bollen, K.A. Structural Equations with Latent Variables; John Wiley & Sons: Oxford, UK, 1989; pp. xiv, 514. ISBN 978-0-471-01171-2. [Google Scholar]
- Sheshkin, D.J. Handbook of Parametric and Nonparametric Statistical Procedures, 3rd ed.; Chapman & Hall/CRC: Boca Raton, FL, USA, 2004. [Google Scholar]
- Selya, A.S.; Rose, J.S.; Dierker, L.C.; Hedeker, D.; Mermelstein, R.J. A practical guide to calculating Cohen’s f2, a measure of local effect size, from PROC MIXED. Front. Psychol. 2012, 3, 111. [Google Scholar] [CrossRef] [Green Version]
- Ellis, P.D. The Essential Guide to Effect Sizes: Statistical Power, Meta-Analysis, and the Interpretation of Research Results; Cambridge University Press: New York, NY, USA, 2010; ISBN 978-1-139-48815-0. [Google Scholar]
- Sonino, N.; Fava, G.A. A simple instrument for assessing stress in clinical practice. Postgrad. Med. J. 1998, 74, 408–410. [Google Scholar] [CrossRef] [Green Version]
- Pakenham, K.I.; Cox, S. Effects of benefit finding, social support and caregiving on youth adjustment in a parental illness context. J. Child Fam. Stud. 2018, 27, 2491–2506. [Google Scholar] [CrossRef]
- Landi, G.; Pakenham, K.I.; Benassi, M.; Giovagnoli, S.; Tossani, E.; Grandi, S. A model of the effects of parental illness on youth adjustment and family functioning: The moderating effects of psychological flexibility on youth caregiving and stress. Int. J. Environ. Res. Public. Health 2021, 18, 4902. [Google Scholar] [CrossRef]
- Viskovich, S.; Pakenham, K.I. R Randomized Controlled Trial of a web-based Acceptance and Commitment Therapy (ACT) program to promote mental health in university students. J. Clin. Psychol. 2020, 76, 929–951. [Google Scholar] [CrossRef]
- Han, A.; Yuen, H.K.; Jenkins, J. Acceptance and Commitment Therapy for family caregivers: A systematic review and meta-analysis. J. Health Psychol. 2021, 26, 82–102. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Giovannetti, A.M.; Quintas, R.; Tramacere, I.; Giordano, A.; Confalonieri, P.; Messmer Uccelli, M.; Solari, A.; Pakenham, K.I. A Resilience group training program for people with Multiple Sclerosis: Results of a pilot single-blind Randomized Controlled Trial and nested qualitative study. PLoS ONE 2020, 15, e0231380. [Google Scholar] [CrossRef] [Green Version]
- Levin, M.E.; Haeger, J.; Pierce, B.; Cruz, R.A. Evaluating an adjunctive mobile app to enhance psychological flexibility in Acceptance and Commitment Therapy. Behav. Modif. 2017, 41, 846–867. [Google Scholar] [CrossRef] [PubMed]
- Dunér, A.; Olin, E. Personal assistance from family members as an unwanted situation, an optimal solution or an additional good? The Swedish example. Disabil. Soc. 2018, 33, 1–19. [Google Scholar] [CrossRef]
- Järkestig Berggren, U.; Bergman, A. Whether disabled parents receive personal assistance for parenting and the consequences for children—An interview study. Int. J. Environ. Res. Public. Health. 2022, 19, 3330. [Google Scholar] [CrossRef]


{kind=link}
| PI (n = 268) | OIFM (n = 97) | Non-Carers (n = 1458) | ||||
|---|---|---|---|---|---|---|
| Variable | % | M (SD) | % | M (SD) | % | M (SD) |
| Socio-demographics | ||||||
| Gender: female | 74.25 | 72.16 | 71.26 | |||
| Age years | 24.03 (2.72) | 24.02 (2.80) | 24.50 (2.86) | |||
| Education | ||||||
| Primary school | 2.24 | 3.09 | 4.05 | |||
| Secondary school | 47.01 | 47.42 | 42.03 | |||
| Bachelor’s degree | 46.64 | 44.33 | 49.93 | |||
| Postgraduate course | 4.10 | 5.15 | 3.98 | |||
| Single | 96.27 | 92.78 | 86.97 | |||
| Married or living with a partner | 3.73 | 7.22 | 12.83 | |||
| Currently studying | 65.67 | 62.89 | 56.24 | |||
| Currently working | 25.00 | 28.87 | 37.72 | |||
| Not in education, employment, or training | 10.82 | 11.34 | 9.19 | |||
| Socio-economic status | ||||||
| <€15,000 | 19.78 | 15.46 | 16.60 | |||
| €15,001–€36,000 | 42.16 | 42.27 | 42.94 | |||
| €36,000–€70.000 | 29.85 | 32.99 | 29.29 | |||
| >€70.000 | 5.22 | 5.15 | 7.89 | |||
| Italian nationality | 98.51 | 98.97 | 97.74 | |||
| Presence of a physical health condition | 10.82 | 14.43 | 8.30 | |||
| Family caregiving context variables | ||||||
| Ill mother | 61.94 | |||||
| Ill father | 54.48 | |||||
| Ill siblings | 59.79 | |||||
| Ill grandparents | 43.30 | |||||
| Physical illness | 66.04 | 57.73 | ||||
| Mental illness | 46.64 | 52.58 | ||||
| Insufficient home dimension a | 1.44 (1.02) | 1.45 (1.12) | 1.41 (1.02) | |||
| Working or studying from home a | 2.55 (1.84) | 2.38 (1.84) | 2.30 (1.86) | |||
| Currently in red zone | 10.45 | 9.28 | 9.05 | |||
| COVID-19 infected | 15.21 | 8.25 | 14.18 | |||
| COVID-19 hospitalized | 0.00 | 0.00 | 0.00 | |||
| Family member infected | 27.00 | 17.53 | 24.53 | |||
| Family member hospitalized | 5.22 | 3.09 | 4.18 | |||
| Family member death | 3.00 | 4.12 | 4.18 | |||
| Lost work | 5.22 | 1.03 | 3.02 | |||
| Redundancy payment | 1.49 | 3.09 | 1.99 | |||
| Substantial income reduction | 4.85 | 3.09 | 4.12 | |||
| PI (n = 268) | OIFM (n = 97) | Non-Carers (n = 1458) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M (SD) or % | Range | α | M (SD) or % | Range | α | M (SD) or % | Range | α | |
| COVID-19-related mental health outcomes | |||||||||
| Risky health behaviors a | 1.03 (0.53) | 0–2.50 | − | 1.04 (0.61) | 0–2.25 | − | 0.94 (0.50) | 0–3 | − |
| Loneliness | 1.70 (0.86) | 0–3 | 0.84 | 1.58 (0.89) | 0–3 | 0.87 | 1.48 (0.90) | 0–3 | 0.87 |
| Increased home violence a | 0.64 (0.93) | 0–4 | − | 0.53 (0.82) | 0–4 | − | 0.31 (0.64) | 0–4 | − |
| Fear of COVID-19 | 12.30 (4.63) | 7–35 | 0.85 | 12.23 (4.79) | 7–27 | 0.85 | 11.41 (4.02) | 7–32 | 0.82 |
| General mental health outcomes | |||||||||
| Anxiety ¥ | 9.23 (4.95) | 0–21 | 0.88 | 8.99 (5.34) | 0–21 | 0.90 | 7.35 (4.90) | 0–21 | 0.90 |
| Normal | 18.01% | 22.11% | 32.43% | ||||||
| Mild | 37.55% | 36.84% | 38.54% | ||||||
| Moderate | 27.20% | 22.10% | 17.89% | ||||||
| Severe | 17.24% | 18.95% | 11.14% | ||||||
| Depression ¥ | 11.46 (5.93) | 0–27 | 0.88 | 11.24 (6.35) | 0–27 | 0.89 | 9.03 (5.65) | 0–27 | 0.88 |
| Normal | 9.96% | 15.79% | 21.65% | ||||||
| Mild | 33.33% | 30.53% | 40.52% | ||||||
| Moderate | 26.82% | 26.31% | 20.51% | ||||||
| Severe | 29.89% | 27.37% | 17.32% | ||||||
| Wellbeing ¥ | 31.15 (13.22) | 2–61 | 0.91 | 31.59 (13.83) | 0–60 | 0.91 | 35.12 (12.94) | 0–70 | 0.90 |
| Flourishing | 27.64% | 30.85% | 18.28% | ||||||
| Moderate | 54.07% | 50.00% | 56.68% | ||||||
| Languishing | 18.29% | 19.15% | 25.04% | ||||||
| COVID-19-Related Mental Health Outcomes | ||||||||||||
| Risky Health Behaviors | Loneliness | Increased Home Violence | Fear of COVID-19 | |||||||||
| PI | OIFM | Non-Carers | PI | OIFM | Non- Carers | PI | OIFM | Non- Carers | PI | OIFM | Non-Carers | |
| Insufficient home dimension | 0.018 | 0.222 * | 0.008 | 0.021 | 0.216 * | 0.099 *** | 0.113 | 0.204 * | 0.102 *** | 0.031 | 0.317 **† | −0.003 † |
| Working or studying from home | 0.094 | 0.044 | 0.080 ** | −0.045 | 0.123 | 0.104 *** | −0.108 | 0.170 | 0.028 | 0.003 | −0.115 | 0.079 ** |
| Currently in red zone b | −0.117 | 0.033 | 0.006 | −0.077 | 0.041 | 0.049 | −0.105 | 0.103 | 0.002 | −0.101 | 0.027 | 0.027 |
| COVID-19 infected b | 0.045 | −0.017 | 0.043 | 0.103 | 0.170 * | 0.036 | −0.041 | 0.015 | 0.027 | −0.029 | 0.151 | 0.014 |
| Family member infected b | −0.051 | 0.027 | 0.027 | 0.171 ** | 0.088 | 0.015 | −0.009 | −0.035 | 0.03 | −0.018 | 0.126 | 0.011 |
| Family member hospitalized b | −0.024 | 0.043 | −0.007 | −0.042 | −0.017 | 0.033 | −0.047 | −0.026 | 0.000 | 0.009 | 0.037 | 0.014 |
| Family member death b | 0.078 | 0.119 | 0.017 | 0.043 | 0.020 | 0.042 | 0.007 | −0.152 | −0.021 | 0.053 | 0.228 * | 0.034 |
| Reduced family income b | 0.035 | 0.099 | 0.027 | 0.130 * | 0.190 | 0.036 | 0.033 | −0.064 | −0.001 | 0.057 | 0.114 | 0.041 |
| COVID-19 Context Index | 0.003 | 0.248 * | 0.037 | 0.111 | 0.294 ** | 0.113 *** | 0.069 | 0.174 | 0.095 *** | −0.010 | 0.417 ***† | 0.018 † |
| General Mental Health Outcomes | ||||||||||||
| Anxiety | Depression | Wellbeing | ||||||||||
| PI | OIFM | Non- carers | PI | OIFM | Non- carers | PI | OIFM | Non- carers | ||||
| Insufficient home dimension | −0.033 | 0.278 ** | 0.079 ** | −0.046 | 0.178 | 0.085 ** | −0.119 | −0.210 * | −0.122 *** | |||
| Working or studying from home | 0.121 | 0.062 | 0.174 *** | 0.075 | 0.127 | 0.203 *** | −0.104 | −0.139 | −0.171 *** | |||
| Currently in red zone b | −0.163 **† | 0.113 | 0.082 **† | −0.078 † | 0.028 | 0.103 ***† | 0.120 † | −0.063 | −0.080 **† | |||
| COVID-19 infected b | −0.028 | 0.137 | 0.017 | −0.008 | 0.178 | 0.004 | 0.006 | −0.085 | −0.002 | |||
| Family member infected b | 0.043 | 0.008 | 0.038 | 0.136 * | 0.133 | 0.033 | −0.030 | −0.077 | 0.031 | |||
| Family member hospitalized b | 0.007 | 0.033 | 0.024 | 0.011 | 0.035 | 0.008 | 0.030 | −0.042 | −0.002 | |||
| Family member death b | 0.039 | −0.034 | 0.056 * | 0.056 | 0.025 | 0.041 | 0.078 | 0.045 | −0.008 | |||
| Reduced family income b | 0.078 | 0.252 * | 0.043 | 0.080 | 0.250 * | 0.062 * | −0.072 | −0.185 | −0.066 * | |||
| COVID-19 Context Index | −0.030 | 0.324 ** | 0.109 *** | 0.012 | 0.281 ** | 0.117 *** | −0.080 | −0.262 * | −0.118 *** | |||
| COVID-19-Related Mental Health Outcomes | GeneralMental Health Outcomes | ||||||
|---|---|---|---|---|---|---|---|
| Risky Health Behaviors | Loneliness | Increased Home Violence | Fear of COVID-19 | Anxiety | Depression | Wellbeing | |
| β (ƒ2) | β (ƒ2) | β (ƒ2) | β (ƒ2) | β (ƒ2) | β (ƒ2) | β (ƒ2) | |
| Family caregiving status | |||||||
| PI † | 0.052 * (0.003) | 0.073 ** (0.005) |
0.161 *** (0.027) |
0.067 ** (0.005) |
0.114 *** (0.013) |
0.125 *** (0.016) | −0.085 *** (0.007) |
| OIFM † | 0.042 (0.002) |
0.019 (0.000) | 0.070 ** (0.005) | 0.042 (0.002) |
0.068 ** (0.005) |
0.078 ** (0.006) | −0.052 * (0.003) |
| Confounders | |||||||
| COVID-19 Context Index | 0.058 * (0.003) | 0.136 *** (0.019) | 0.096 *** (0.009) | 0.043 (0.002) | 0.118 *** (0.014) | 0.130 *** (0.017) | −0.134 *** (0.018) |
| Age | −0.100 *** (0.010) | −0.087 ** (0.008) | −0.030 (0.001) | −0.024 (0.001) | −0.039 (0.002) | −0.078 ** (0.006) |
0.041 (0.002) |
| Currently studying b |
0.064 (0.004) | −0.018 (0.000) |
0.030 (0.001) | −0.026 (0.001) | 0.062 (0.004) |
0.020 (0.000) |
0.034 (0.001) |
| Currently working b | 0.027 (0.001) | −0.113 ** (0.013) |
0.021 (0.000) | −0.077 * (0.006) | −0.122 ** (0.015) | −0.158 *** (0.026) |
0.204 *** (0.043) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landi, G.; Pakenham, K.I.; Grandi, S.; Tossani, E. Young Adult Carers during the Pandemic: The Effects of Parental Illness and Other Ill Family Members on COVID-19-Related and General Mental Health Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 3391. https://doi.org/10.3390/ijerph19063391
Landi G, Pakenham KI, Grandi S, Tossani E. Young Adult Carers during the Pandemic: The Effects of Parental Illness and Other Ill Family Members on COVID-19-Related and General Mental Health Outcomes. International Journal of Environmental Research and Public Health. 2022; 19(6):3391. https://doi.org/10.3390/ijerph19063391
Chicago/Turabian StyleLandi, Giulia, Kenneth I. Pakenham, Silvana Grandi, and Eliana Tossani. 2022. "Young Adult Carers during the Pandemic: The Effects of Parental Illness and Other Ill Family Members on COVID-19-Related and General Mental Health Outcomes" International Journal of Environmental Research and Public Health 19, no. 6: 3391. https://doi.org/10.3390/ijerph19063391
APA StyleLandi, G., Pakenham, K. I., Grandi, S., & Tossani, E. (2022). Young Adult Carers during the Pandemic: The Effects of Parental Illness and Other Ill Family Members on COVID-19-Related and General Mental Health Outcomes. International Journal of Environmental Research and Public Health, 19(6), 3391. https://doi.org/10.3390/ijerph19063391