
HBM4EU Chromates Study: Determinants of Exposure to Hexavalent Chromium in Plating, Welding and Other Occupational Settings

 ,
,  ,
, 
 , ,
, ,  ,
,  , ,
, ,  , , , , , , ,
, , , , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Recruitment
2.2. Sampling
2.2.1. Air Samples
2.2.2. Dermal Wipe Samples
2.2.3. Urine Samples
2.3. Contextual Data Collected
2.4. Data Management and Statistical Analysis
3. Results
3.1. Companies Involved in the Study
3.2. Study Population
3.3. Total Cr and Cr(VI) in Industrial Hygiene Samples (Air and Wipes)
3.4. Total Cr in Urine
3.5. Correlations between Different Exposure Metrics
3.6. Determinants of Exposure
4. Discussion
4.1. Workers Exposure
4.2. Relevance of U-Cr and BM for the Exposure Assessment to Cr(VI)
4.3. Exposure Determinants
4.3.1. Use of RPE and Daily Fit Check
4.3.2. Use of Gloves
4.3.3. Availability of LEV
4.3.4. Storage Working Clothes and RPE
4.3.5. Training on OSH Issues
4.3.6. Previous Monitoring Actions
4.4. Strenghts and Limitations
5. Conclusions
- Collection of contextual data supports the interpretation of HBM and industrial hygiene data and the identification of exposure determinants;
- Both inhalation exposure and dermal exposure can be reflected as enhanced urinary chromium excretion;
- A high correlation between pre- and post-shift urinary chromium suggests that this biomarker reflects recent as well as past exposure;
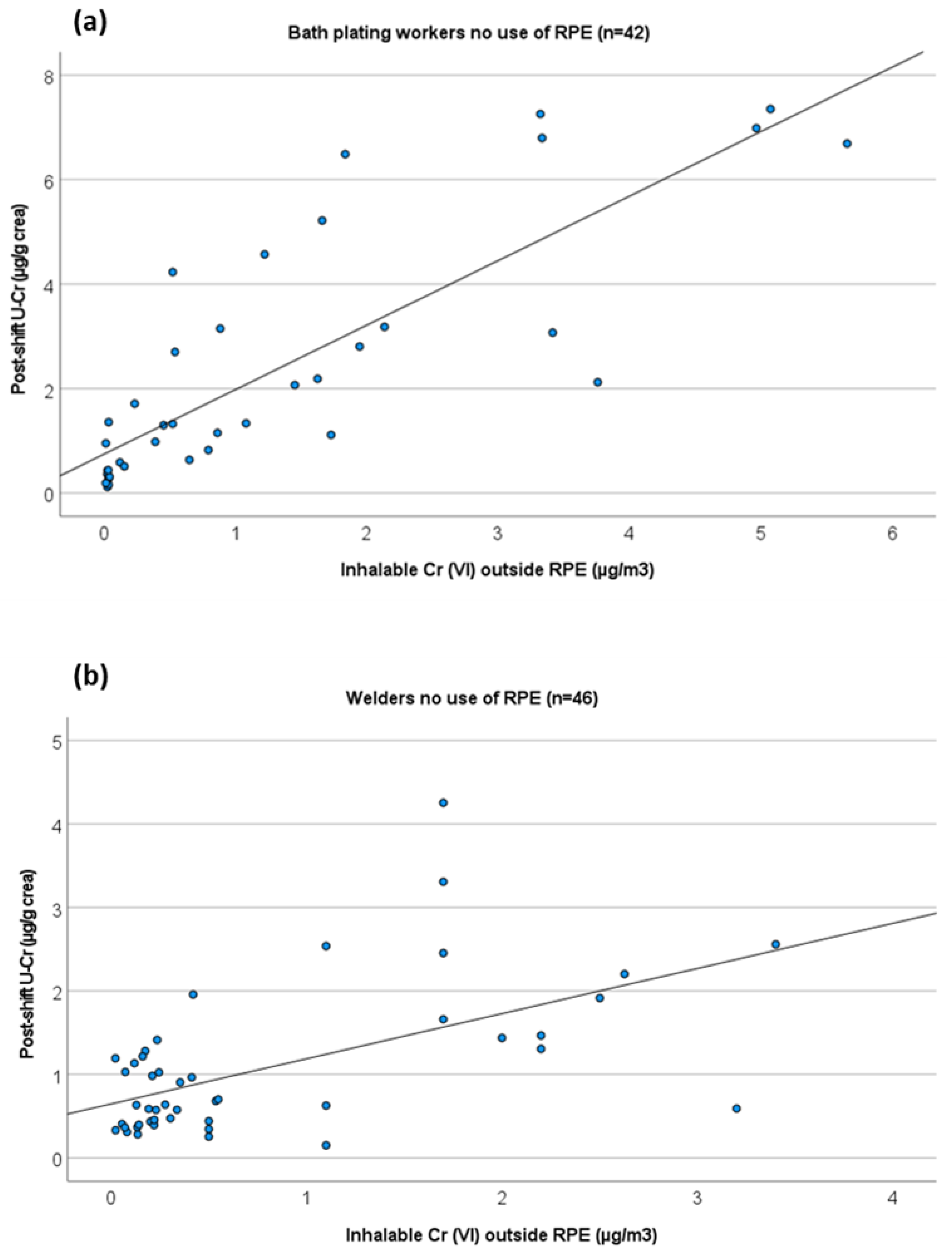
- The relationship between inhalable air Cr(VI) levels and urinary Cr levels in platers are consistent with earlier reported regression equations published by Chen et al. [37];
- Similar inhalation exposures translate into two-fold higher U-Cr levels in chrome platers as compared to welders suggesting differences in toxicokinetic (e.g., absorption and bioavailability) of Cr(VI) compounds related to the route of exposure;
- In some specific chrome applications, the use of RPE contributes to reduced exposures and risk;
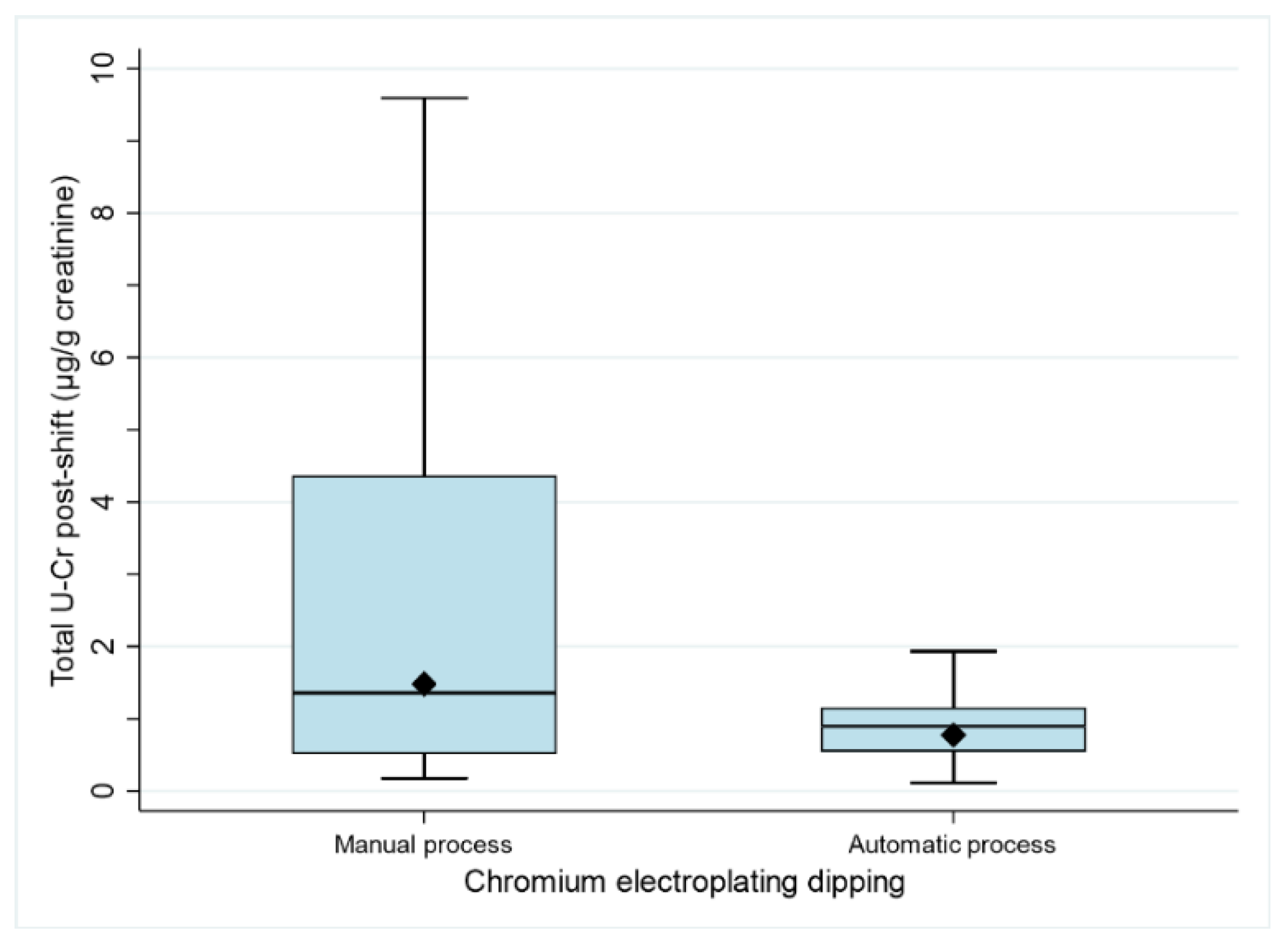
- Not all RMMs are equally effective in reducing exposure: automation of Cr electroplating dipping resulted in lower U-Cr levels; the use of RPE resulted in lower U-Cr in welding, bath plating and painting; LEV explains lower Cr exposure levels in welders;
- The existence of a dedicated place for storing working clothes might increase the exposure if not combined with clear procedures for washing/disposing of the working clothes/PPE and stringent housekeeping measures.
- Occupational health and safety training has a beneficial effect on exposure levels in welders.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- NIOSH. Occupational Exposure to Hexavalent Chromium; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Washington, DC, USA, 2013. Available online: https://www.cdc.gov/niosh/docs/2013128/pdfs/2013_128.pdf?id=0.26616/NIOSHPUB2013128 (accessed on 11 February 2022).
- Beattie, H.; Keen, C.; Coldwell, M.; Tan, E.; Morton, J.; McAlinden, J.; Smith, P. The use of bio-monitoring to assess exposure in the electroplating industry. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viegas, S.; Jeddi, M.Z.; Hopf, N.B.; Bessems, J.; Palmen, N.; Galea, K.; Jones, K.; Kujath, P.; Duca, R.C.; Verhagen, H.; et al. Biomonitoring as an underused exposure assessment tool in Occupational Safety and Health context–Challenges and way forward! Int. J. Environ. Res. Public Health 2020, 17, 5884. [Google Scholar] [CrossRef] [PubMed]
- Saha, R.; Nandi, R.; Saha, B. Sources and toxicity of hexavalent chromium. J. Coord. Chem. 2011, 64, 1782–1806. [Google Scholar] [CrossRef]
- Chen, Q.Y.; DesMarais, T.; Costa, M. Metals and mechanisms of carcinogenesis. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 537–554. [Google Scholar] [CrossRef]
- OSHA. Health Effects of Hexavalent Chromium; Occupational Safety & Health Administration, United States Department of Labor: Washington, DC, USA, 2006. Available online: https://www.osha.gov/OshDoc/data_General_Facts/hexavalent_chromium.pdf (accessed on 11 February 2022).
- IARC. Chromium (VI) compounds. In IARC Monographs—Volume 100C, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer: Lyon, France, 2012; pp. 147–167. Available online: https://monographs.iarc.fr/wp-content/uploads/2018/06/mono100C-9.pdf (accessed on 11 February 2022).
- den Braver-Sewradj, S.P.; van Benthem, J.; Staal, Y.C.M.; Ezendam, J.; Piersma, A.H.; Hessel, E.V.S. Occupational exposure to hexavalent chromium. Part II. Hazard assessment of carcinogenic effects. Regul. Toxicol. Pharmacol. 2021, 126, 105045. [Google Scholar] [CrossRef]
- European Union. Regulation (EC) No 1907/2006 of the European Parliament and of the Council of 18 December 2006 concerning the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH); European Union: Brussels, Belgium, 2006. [Google Scholar]
- EU-OSHA. Directive 2004/37/EC—Carcinogens or Mutagens at Work; European Agency for Safety and Health at Work: Bilbao, Spain, 2004; Available online: https://osha.europa.eu/en/legislation/directives/directive-2004-37-ec-carcinogens-ormutagens-at-work (accessed on 11 February 2022).
- The Netherlands Ministerie van Sociale Zaken en Werkgelegenheid. Regeling van de Minister van Sociale Zaken en Werkgelegenheid van 18 Oktober 2016, 2016-0000222216, tot Wijziging van de Arbeidsomstandighedenregeling in Verband de Wijziging van Twee Wettelijke Grenswaarden in Bijlage XIII (Bisfenol A en Chroom (VI)-Verbindingen); Ministerie van Sociale Zaken en Werkgelegenheid: Den Haag, The Netherlands, 2016. Available online: https://zoek.officielebekendmakingen.nl/stcrt-2016-57792.html?grootte=2 (accessed on 11 February 2022).
- ANSES. Valeurs Limites D’exposition en Milieu Professionnel: Évaluation des Indicateurs Biologiques D’exposition et Recommandation de Valeurs Biologiques Pour le Chrome VI et ses Composés: Avis de l’Anses: Rapport D’expertise Collective; Agence Nationale de Sécurité Sanitaire de l’Alimentation, de l’Environnement et du Travail: Maisons-Alfort, France, 2017.
- Verdonck, J.; Duca, R.-C.; Galea, K.S.; Iavicoli, I.; Poels, K.; Toreyi, Z.N.; Vanoirbeek, J.; Godderis, L. Systematic review of biomonitoring data on occupational exposure to hexavalent chromium. Int. J. Hyg. Environ. Health 2021, 236, 113799. [Google Scholar] [CrossRef]
- STM. HTP-Arvot 2020: Haitallisiksi Tunnetut Pitoisuudet, Sosiaali-ja Terveysministeriön Julkaisuja 2020:24; Sosiaali-ja Terveysministeriö: Helsinki, Finland, 2020; ISBN 978-952-00-5658-2. Available online: http://urn.fi/ (accessed on 11 February 2022).
- Ganzleben, C.; Antignac, J.P.; Barouki, R.; Castaño, A.; Fiddicke, U.; Klánová, J.; Lebret, E.; Olea, N.; Sarigiannis, D.; Schoeters, G.R.; et al. Human biomonitoring as a tool to support chemicals regulation in the European Union. Int. J. Hyg. Environ. Health 2017, 220, 94–97. [Google Scholar] [CrossRef]
- Santonen, T.; Alimonti, A.; Bocca, B.; Duca, R.C.; Galea, K.S.; Godderis, L.; Göen, T.; Gomes, B.; Hanser, O.; Iavicoli, I.; et al. Setting up a collaborative European human biological monitoring study on occupational exposure to hexavalent chromium. Environ. Res. 2019, 177, 108583. [Google Scholar] [CrossRef]
- Santonen, T.; Porras, S.P.; Bocca, B.; Bousoumah, R.; Duca, R.C.; Galea, K.S.; Godderis, L.; Göen, T.; Hardy, E.; Iavicoli, I.; et al. HBM4EU chromates study—Overall results and recommendations for the biomonitoring of occupational exposure to hexavalent chromium. Environ. Res. 2022, 204 Pt A, 111984. [Google Scholar] [CrossRef]
- Galea, K.S.; Porras, S.P.; Viegas, S.; Bocca, B.; Bousoumah, R.; Duca, R.C.; Godderis, L.; Iavicoli, I.; Janasik, B.; Jones, K.; et al. HBM4EU chromates study—Reflection and lessons learnt from designing and undertaking a collaborative European biomonitoring study on occupational exposure to hexavalent chromium. Int. J. Hyg. Environ. Health 2021, 234, 113725. [Google Scholar] [CrossRef]
- OSHA. Metal and Metalloid Particulates in Workplace Atmospheres (ICP Analysis); Occupational Safety & Health Administration, United States Department of Labor: Washington, DC, USA, 2002. Available online: https://www.osha.gov/dts/sltc/methods/inorganic/id125g/id125g.pdf (accessed on 11 February 2022).
- ISO. ISO 16740:2005; Workplace Air–Determination of Hexavalent Chromium in Airborne Particulate Matter–Method by Ion Chromatography and Spectrophotometric Measurement Using Diphenyl Carbazide. International Standard Organization: Geneva, Switzerland, 2005. Available online: https://www.iso.org/standard/30432.html (accessed on 11 February 2022).
- NIOSH. Elements on wipes: NIOSH method 9102. In NIOSH Manual of Analytical Methods (NMAM), 4th ed.; Schlecht, P.C., O’Connor, P.F., Eds.; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Washington, DC, USA, 2003. Available online: https://www.cdc.gov/niosh/docs/2003-154/pdfs/9102.pdf (accessed on 11 February 2022).
- U.S. EPA. Exposure Factors Handbook: 2011 Edition: Final Report; EPA/600/R-09/052F; U.S. Environmental Protection Agency: Washington, DC, USA, 2011. Available online: https://www.epa.gov/sites/production/files/2015-09/documents/techoverview_efh-complete.pdf (accessed on 11 February 2022).
- Aitio, A. Quality Assurance. In Biological Monitoring of Chemical Exposure in the Workplace; World Health Organization: Geneva, Switzerland, 1996; Volume 1, pp. 20–51. [Google Scholar]
- Cocker, J.; Mason, H.J.; Warren, N.D.; Cotton, R.J. Creatinine adjustment of biological monitoring results. Occup. Med. 2011, 61, 349–353. [Google Scholar] [CrossRef] [Green Version]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Remy, A.M.; Robert, A.; Jacoby, N.; Wild, P. Is urinary chromium specific to hexavalent chromium exposure in the presence of Co-exposure to other chromium compounds? A biomonitoring study in the electroplating industry. Ann. Work. Expo. Health 2021, 65, 332–345. [Google Scholar] [CrossRef]
- Pesch, B.; Lehnert, M.; Weiss, T.; Kendzia, B.; Menne, E.; Lotz, A.; Heinze, E.; Behrens, T.; Gabriel, S.; Schneider, W.; et al. Exposure to hexavalent chromium in welders: Results of the WELDOX II field study. Ann. Work. Expo. Health 2018, 62, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Scheepers, P.T.; Heussen, G.A.; Peer, P.G.M.; Verbist, K.; Anzion, R.; Willemset, K. Characterisation of exposure to total and hexavalent chromium of welders using biological monitoring. Toxicol. Lett. 2008, 178, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Von Emmerling, G.; Zschiesche, W.; Schaller, K.H.; Weltle, D. Arbeitsmedizische Belastungs-und Beanspruchungsuntersuchungen von Edelstahlschweissen; Institut für Arbeits- und Sozialmedizin und der Poliklinik für Berufskrankheiten der Universität Erlangen-Nürnberg: Erlangen, Deutshland, 1989. [Google Scholar]
- ACGIH. Threshold Limit Values (TLVs) and Biological Exposure Indices (BEIs); American Conference of Govern-mental Industrial Hygienists: Cincinnati, OH, USA, 2021. [Google Scholar]
- Persoons, R.; Arnoux, D.; Monssu, T.; Culié, O.; Roche, G.; Duffaud, B.; Chalaye, D.; Maitre, A. Determinants of occupational exposure to metals by gas metal arc welding and risk management measures: A biomonitoring study. Toxicol. Lett. 2014, 231, 135–141. [Google Scholar] [CrossRef]
- Lehnert, M.; Weiss, T.; Pesch, B.; Lotz, A.; Zilch-Schöneweis, S.; Heinze, E.; Van Gelder, R.; Hahn, J.U.; Brüning, T. Reduction in welding fume and metal exposure of stainless steel welders: An example from the WELDOX study. Int. Arch. Occup. Environ. Health 2014, 87, 483–492. [Google Scholar] [CrossRef]
- Keen, C.; Tan, E.; McAlinden, J.; Woolgar, P.; Smith, P. Exposure to Hexavalent Chromium, Nickel and Cadmium Compounds in the Electroplating Industry: Prepared by the Health and Safety Laboratory for the Health and Safety Executive 2013; RR963 Research Report; Health and Safety Executive: London, UK, 2013.
- Jones, K. Human Biomonitoring in occupational health for exposure assessment. Port. J. Public Heath 2020, 38, 2–5. [Google Scholar] [CrossRef]
- Lindberg, E.; Vesterberg, O. Monitoring exposure to chromic acid in chrome plating by measuring chromium in urine. Scand. J. Work. Environ. Health 1983, 9, 333–340. [Google Scholar] [CrossRef]
- Chen, J.-L.; Guo, Y.-L.; Tsai, P.-J.; Su, L.-F. Use of inhalable Cr+6 exposures to characterize urinary chromium concentrations in plating industry workers. J. Occup. Health 2002, 44, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Wilbur, S.; Abadin, H.; Fay, M.; Yu, D.; Tencza, B.; Ingerman, L.; Klotzbach, J.; James, S. Toxicological Profile for Chromium; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2012.
- HSE. Respiratory Protective Equipment at Work: A Practical Guide; Health and Safety Executive: London, UK, 2013. Available online: https://www.hse.gov.uk/pubns/priced/hsg53.pdf (accessed on 11 February 2022).
- Picheansanthian, W.; Chotibang, J. Glove utilization in the prevention of cross transmission: A systematic review. JBI Database Syst. Rev. Implement Rep. 2015, 13, 188–230. [Google Scholar] [CrossRef]
- Viegas, C.; Twarużek, M.; Dias, M.; Almeida, B.; Carolino, E.; Kosicki, R.; Soszczyńska, E.; Grajewski, J.; Caetano, L.A.; Viegas, S. Assessment of the microbial contamination of mechanical protection gloves used on waste sorting industry: A contribution for the risk characterization. Environ. Res. 2020, 189, 109881. [Google Scholar] [CrossRef] [PubMed]
- Meeker, J.D.; Susi, P.; Flynn, M.R. Hexavalent chromium exposure and control in welding tasks. J. Occup. Environ. Hyg. 2010, 7, 607–615. [Google Scholar] [CrossRef] [PubMed]
- IARC. Welding, Molybdenum Trioxide, and Indium Tin Oxide. Available online: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Welding-Molybdenum-Trioxide-And-Indium-Tin-Oxide-2018 (accessed on 11 February 2022).
- European Commission. Third Study on Collecting Most Recent Information for a Certain Number of Substances with the View to Analyse the Health, Socio-Economic and Environmental Impacts in Connection with Possible Amendments of Directive 2004/37/EC (Ref: VC/2017/0011): Final Report for Chromium(VI) in Fumes from Welding, Plasma Cutting and Similar Processes; Publications Office of the European Union: Luxembourg, 2019; ISBN 978-92-76-07993-4. [Google Scholar]
- Cherrie, J.; Semple, S.; Christopher, Y.; Saleem, A.; Hughson, G.; Philips, A. How important is inadvertent ingestion of hazardous substances at work? Ann. Occup. Hyg. 2006, 50, 693–704. [Google Scholar]



{kind=link}
{kind=link}
| Questionnaire | Determinants of Exposure |
|---|---|
| 1 | Previous monitoring campaigns (environment and biomonitoring) |
| Previous training on OSH issues | |
| 2 | Availability of LEV |
| Use of gloves | |
| Use of RPE | |
| Daily fit check of RPE | |
| Existence of a dedicated place for storing working clothes and RPE | |
| Workers’ experience in their jobs | |
| Non-workplace exposure sources: smoking status, home location (urban or rural) and home traffic density |
| Total Cr (µg/m3) (Cr(VI) µg/m3) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | GM | Median | P75 | P95 | Range | OEL Cr(VI) (µg/m3) | ||
| Air samples (µg/m3) | Welding | ||||||||
| Inhalable—Outside RPE | 124 (107) | 111.0 (1.6) | 18.9 (0.5) | 16.1 (0.5) | 73.3 (1.1) | 481.0 (4.1) | 0.2–3670.0 (<LOQ–40.4) | 25.0 +; 5.0 * | |
| Inhalable—Inside RPE | 34 (10) | 15.3 (1.6) | 3.7 (1.0) | 3.2 (0.5) | 7.7 (1.1) | 124.0 (4.1) | 0.3–306.9 (0.1–44.3) | ||
| Respirable—Outside RPE | 32 (20) | 18.7 (2.3) | 1.8 (0.2) | 1.5 (0.1) | 4.0 (1.2) | 202.2 (22.3) | 0.1–266.6 (0.2–22.8) | ||
| Bath plating | |||||||||
| Inhalable—Outside RPE | 31 (57) | 41.1 (1.2) | 7.7 (0.3) | 9.9 (0.4) | 32.4 (1.7) | 359.0 (5.1) | 0.1–621.3 (<LOQ–9.1) | 10.0 +; 5.0 * | |
| Respirable—Outside RPE | 34 (54) | 7.8 (0.4) | 1.1 (0.1) | 0.7 (0.1) | 2.7 (0.5) | 59.3 (2.3) | 0.9–166.3 (<LOQ–3.1) | ||
| Painting | |||||||||
| Inhalable—Outside RPE | 4 (7) | 30.3 (29.3) | 7.6 (5.8) | 19.1 (5.6) | 70.8 (154) | 82.0 (154) | 1.0–82 (0.6–154.4) | ||
| Respirable—Outside RPE | 11 (<LOQ) | 2.5 | 1.2 | 1.0 | 3.0 | 9.5 | 0.3–9.4 | ||
| Machining | |||||||||
| Inhalable—Outside RPE | 8 (15) | 42.0 (0.2) | 11.0 (0.1) | 48.7 (0.1) | 70.2 (0.2) | 96.3 (<LOQ) | 0.3–96.3 (<LOQ–0.4) | ||
| Respirable—Outside RPE | 9 (10) | 1.5 (0.03) | 0.7 (0.03) | 0.6 (0.03) | 2.5 (0.04) | 6.2 (0.05) | 0.2–6.2 (<LOQ–0.05) | ||
| Steel production | |||||||||
| Inhalable—Outside RPE | 5 (<LOQ) | 4.9 | 3.3 | 2.4 | 9.6 | 13.9 | 1.5–13.9 | ||
| Respirable—Outside RPE | 5 (<LOQ) | 0.9 | 0.6 | 0.3 | 1.9 | 2.0 | 0.3–2.0 | ||
| Maintenance and laboratory work | |||||||||
| Inhalable—Outside RPE | 1 (3) | <LOQ | 9.9 (0.4) | <LOQ | <LOQ | <LOQ | 9.9 (0.3–0.8) | ||
| Respirable—Outside RPE | 2 (2) | 0.4 (0.2) | 0.4 (0.1) | <LOQ | <LOQ | <LOQ | 0.2–0.6 (<LOQ–0.3) | ||
| Thermal spraying | |||||||||
| Inhalable—Outside RPE | 5 (5) | 2566 (12.5) | 1050 (11.4) | 823 (9.6) | 5755 (18.8) | 8359 (21.0) | 192.5–8359.5 (6.4–21.0) | ||
| Respirable—Outside RPE | 5 (5) | 58.6 (0.07) | 23.0 (0.06) | 9.6 (0.06) | 136.0 (0.1) | 140.0 (0.1) | 5.5–140.0 (<LOQ–0.1) | ||
| Wipe samples Shift sum ** (µg/cm2) | Welding | 115 | 0.3 | 0.1 | 0.2 | 0.3 | 1.0 | <LOQ–1.8 | NA |
| Bath plating | 77 | 0.6 | 0.1 | 0.1 | 0.7 | 2.3 | <LOQ–8.4 | ||
| Painting | 32 | 0.1 | 0.1 | 0.0 | 0.1 | 0.3 | <LOQ–0.3 | ||
| Machining | 25 | 0.2 | 0.1 | 0.1 | 0.1 | 1.3 | <LOQ–1.4 | ||
| Steel production | 5 | <LOQ | <LOQ | <LOQ | <LOQ | <LOQ | <LOQ | ||
| Maintenance and laboratory work | 8 | 0.1 | <LOQ | <LOQ | 0.3 | 0.5 | <LOQ–0.5 | ||
| Thermal spraying | 5 | 18.5 | 13.9 | 13.8 | 32.7 | 46.6 | 6.6–46.6 | ||
| Total U-Cr (µg/g Creatinine) | Correlation Pre-Shift vs. Post-Shift | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | GM | Median | P75 | P95 | Range | rs | ||
| Pre-shift | Workers a,b,c,d | 399 | 0.9 | 0.6 | 0.5 | 1.0 | 3.1 | 0.0–8.3 | 0.795 |
| Welding a,b,c,d | 193 | 0.7 | 0.5 | 0.5 | 0.9 | 2.0 | 0.1–5.8 | 0.797 | |
| Bath plating a,b,c,d | 90 | 1.5 | 0.8 | 0.8 | 2.4 | 5.0 | 0.1–8.3 | 0.892 | |
| Painting a,b,c,d | 52 | 0.8 | 0.5 | 0.6 | 1.2 | 2.6 | 0.1–4.0 | 0.703 | |
| Machining a,b,c,d | 38 | 0.7 | 0.5 | 0.4 | 1.0 | 1.9 | 0.1–2.9 | 0.588 | |
| Steel production | 11 | 0.9 | 0.6 | 0.5 | 1.0 | 4.5 | 0.2–4.4 | - | |
| Maintenance and laboratory work | 8 | 0.4 | 0.3 | 0.2 | 0.7 | 1.1 | 0.1–1.1 | - | |
| Thermal spraying | 5 | 0.6 | 0.4 | 0.4 | 1.3 | 2.1 | 0.1–2.1 | - | |
| Controls * | 135 | 0.4 | 0.2 | 0.2 | 0.4 | 1.3 | 0.0–3.2 | - | |
| Within company controls e | 94 | 0.4 | 0.3 | 0.3 | 0.5 | 1.4 | 0.0–3.2 | - | |
| Outwith company controls e | 41 | 0.2 | 0.1 | 0.1 | 0.2 | 0.4 | 0.1–1.9 | - | |
| Post-shift | Workers a,b,d | 399 | 1.4 | 0.8 | 0.9 | 1.7 | 5.1 | 0.1–13.6 | - |
| Welding d,e | 189 | 1.1 | 0.7 | 0.7 | 1.4 | 3.4 | 0.1–5.8 | - | |
| Bath plating a,b,d | 90 | 2.3 | 1.2 | 1.1 | 2.4 | 7.7 | 0.1–13.6 | - | |
| Painting d | 45 | 1.4 | 0.7 | 0.9 | 1.8 | 3.6 | 0.1–12.3 | - | |
| Machining a,b,d | 36 | 1.5 | 1.0 | 1.0 | 1.7 | 6.7 | 0.1–7.7 | - | |
| Steel production | 10 | 1.2 | 1.1 | 1.3 | 1.7 | 2.0 | 0.3–2.0 | - | |
| Maintenance and laboratory work | 8 | 0.5 | 0.4 | 0.3 | 1.0 | 1.5 | 0.1–1.5 | - | |
| Thermal spraying | 5 | 0.7 | 0.4 | 0.4 | 1.4 | 2.4 | 0.1–2.4 | - | |
| Urine: Total Cr (Post Shift) (µg/g Creatinine) | Air: Inhalable Total Cr Outside RPE (µg/m3) | Air: Inhalable Total Cr Inside RPE (µg/m3) | Air: Inhalable Cr(VI) Outside RPE (µg/m3) | Air: Inhalable Cr(VI) Inside RPE (µg/m3) | Air: Respirable Total Cr Outside RPE (µg/m3) | Air: Respirable Cr(VI) Outside RPE (µg/m3) | Wipe: Total Cr Shift Sum (µg/m2) | ||
|---|---|---|---|---|---|---|---|---|---|
| Urine: Total Cr (Pre-shift) (µg/g creatinine) | rs | 0.795 | 0.165 | 0.476 | 0.412 | 0.369 | 0.677 | 0.394 | |
| Sig. | <0.001 | 0.047 | <0.001 | 0.005 | <0.001 | <0.001 | <0.001 | ||
| N | 382 | 145 | 161 | 44 | 98 | 91 | 266 | ||
| Urine: Total Cr (End shift) (µg/g creatinine) | rs | 0.461 | 0.514 | 0.329 | 0.694 | 0.403 | |||
| Sig. | <0.001 | <0.001 | 0.001 | <0.001 | 0.001 | ||||
| N | 193 | 44 | 96 | 90 | 260 | ||||
| Air: Inhalable Total Cr Outside RPE (µg/m3) | rs | 0.609 | 0.800 | 0.457 | 0.606 | ||||
| Sig. | <0.001 | <0.001 | 0.005 | <0.001 | |||||
| N | 88 | 84 | 36 | 90 | |||||
| Air: Inhalable Total Cr Inside RPE (µg/m3) | rs | 0.435 | |||||||
| Sig. | 0.007 | ||||||||
| N | 37 | ||||||||
| Air: Inhalable Cr(VI) Outside RPE (µg/m3) | rs | 0.654 | 0.791 | 0.495 | |||||
| Sig. | <0.001 | <0.001 | <0.001 | ||||||
| N | 48 | 88 | 143 | ||||||
| Air: Inhalable Cr(VI) Inside RPE (µg/m3) | rs | ||||||||
| Sig. | |||||||||
| N | |||||||||
| Air: Respirable Total Cr Outside RPE (µg/m3) | rs | 0.587 | 0.479 | ||||||
| Sig. | <0.001 | <0.001 | |||||||
| N | 34 | 97 | |||||||
| Air: Respirable Cr(VI) Outside RPE (µg/m3) | rs | 0.639 | |||||||
| Sig. | <0.001 | ||||||||
| N | 91 | ||||||||
| Activity | RMM | Urine Total Cr | Air Inha out-RPE Total Cr | Air Inha out-RPE Cr(VI) | Air Inha in-RPE Cr(VI) | Air Resp out-RPE Cr(VI) | Hand Wipe Total Cr |
|---|---|---|---|---|---|---|---|
| Welding (n = 195) | Use of RPE | Yes (p = 0.004) | ------ | ------ | ------ | ------ | ------ |
| Daily fit check of RPE | No | ------ | ------ | ------ | ------ | ------ | |
| Use of gloves | No | ------ | ------ | ------ | ------ | No | |
| Availability of LEV | Yes (p = 0.001) | Yes (p = 0.015) | Yes (p < 0.001) | No | No | No | |
| Dedicated place for storing work clothes | No | ------ | ------ | ------ | ------ | No | |
| Dedicated place for storing RPE | No | ------ | ------ | ------ | ------ | No | |
| Previous training | Yes (p = 0.010) | ------ | ------ | ------ | ------ | Yes (p = 0.005) | |
| Previous monitoring campaigns | Yes (p < 0.001) a | No | Yes (p < 0.001) b | Yes (p = 0.001) b | No | No | |
| Bath plating (n = 90) | Use of RPE | Yes (p = 0.002) | ------ | ------ | ------ | ------ | ------ |
| Daily fit check of RPE | No | ------ | ------ | ------ | ------ | ------ | |
| Use of gloves | No | ------ | ------ | ------ | ------ | No | |
| Availability of LEV | No | No | No | ND | No | No | |
| Dedicated place for storing work clothes | Yes (p = 0.008) ** | ------ | ------ | ------ | ------ | Yes (p = 0.024) ** | |
| Dedicated place for storing RPE | Yes (p = 0.013) | ------ | ------ | ------ | ------ | Yes (p = 0.002) | |
| Previous training | No | ------ | ------ | ------ | ------ | No | |
| Previous monitoring campaigns | Yes (p < 0.001) b | No | Yes (p = 0.014) b | ND | Yes (p = 0.014) b | Yes (p = 0.014) b | |
| Painting (n = 52) | Use of RPE | Yes (p = 0.026) | ------ | ------ | ------ | ------ | ------ |
| Daily fit check of RPE | No | ------ | ------ | ------ | ------ | * | |
| Use of gloves | No | ------ | ------ | ------ | ------ | No | |
| Availability of LEV | No | * | * | ND | * | Yes (p = 0.022) | |
| Dedicated place for storing work clothes | Yes (p = 0.007) ** | ------ | ------ | ------ | ------ | No | |
| Dedicated place for storing RPE | No | ------ | ------ | ------ | ------ | No | |
| Previous training | * | ------ | ------ | ------ | ------ | * | |
| Previous monitoring campaigns | * | * | * | ND | * | * | |
| Machining (n = 38) | Use of RPE | No | ------ | ------ | ------ | ------ | ------ |
| Daily fit check of RPE | No | ------ | ------ | ------ | ------ | ------ | |
| Use of gloves | Yes (p = 0.003) | ------ | ------ | ------ | ------ | No | |
| Availability of LEV | No | No | No | ND | No | No | |
| Dedicated place for storing work clothes | No | ------ | ------ | ------ | ------ | No | |
| Dedicated place for storing RPE | No | ------ | ------ | ------ | ------ | No | |
| Previous training | No | ------ | ------ | ------ | ------ | No | |
| Previous monitoring campaigns | * | * | * | ND | * | * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viegas, S.; Martins, C.; Bocca, B.; Bousoumah, R.; Duca, R.C.; Galea, K.S.; Godderis, L.; Iavicoli, I.; Janasik, B.; Jones, K.; et al. HBM4EU Chromates Study: Determinants of Exposure to Hexavalent Chromium in Plating, Welding and Other Occupational Settings. Int. J. Environ. Res. Public Health 2022, 19, 3683. https://doi.org/10.3390/ijerph19063683
Viegas S, Martins C, Bocca B, Bousoumah R, Duca RC, Galea KS, Godderis L, Iavicoli I, Janasik B, Jones K, et al. HBM4EU Chromates Study: Determinants of Exposure to Hexavalent Chromium in Plating, Welding and Other Occupational Settings. International Journal of Environmental Research and Public Health. 2022; 19(6):3683. https://doi.org/10.3390/ijerph19063683
Chicago/Turabian StyleViegas, Susana, Carla Martins, Beatrice Bocca, Radia Bousoumah, Radu Corneliu Duca, Karen S. Galea, Lode Godderis, Ivo Iavicoli, Beata Janasik, Kate Jones, and et al. 2022. "HBM4EU Chromates Study: Determinants of Exposure to Hexavalent Chromium in Plating, Welding and Other Occupational Settings" International Journal of Environmental Research and Public Health 19, no. 6: 3683. https://doi.org/10.3390/ijerph19063683
APA StyleViegas, S., Martins, C., Bocca, B., Bousoumah, R., Duca, R. C., Galea, K. S., Godderis, L., Iavicoli, I., Janasik, B., Jones, K., Leese, E., Leso, V., Ndaw, S., van Nieuwenhuyse, A., Poels, K., Porras, S. P., Ruggieri, F., Silva, M. J., Verdonck, J., ... HBM4EU Chromates Study Team. (2022). HBM4EU Chromates Study: Determinants of Exposure to Hexavalent Chromium in Plating, Welding and Other Occupational Settings. International Journal of Environmental Research and Public Health, 19(6), 3683. https://doi.org/10.3390/ijerph19063683