
Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea



Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey of Smoking Status and Tobacco Smoke Exposure Urinary Biomarker
2.2. Selection of Subjects
2.3. Analysis of Cigarette Smoke Composition and Inhalation Toxicity
2.4. Calculation of the Internal Estimated Daily Intake for Nicotine and Equivalent Smoked Cigarettes per Day
2.5. Inhalation Exposure and Risk Assessment
2.6. Data Analysis
3. Results
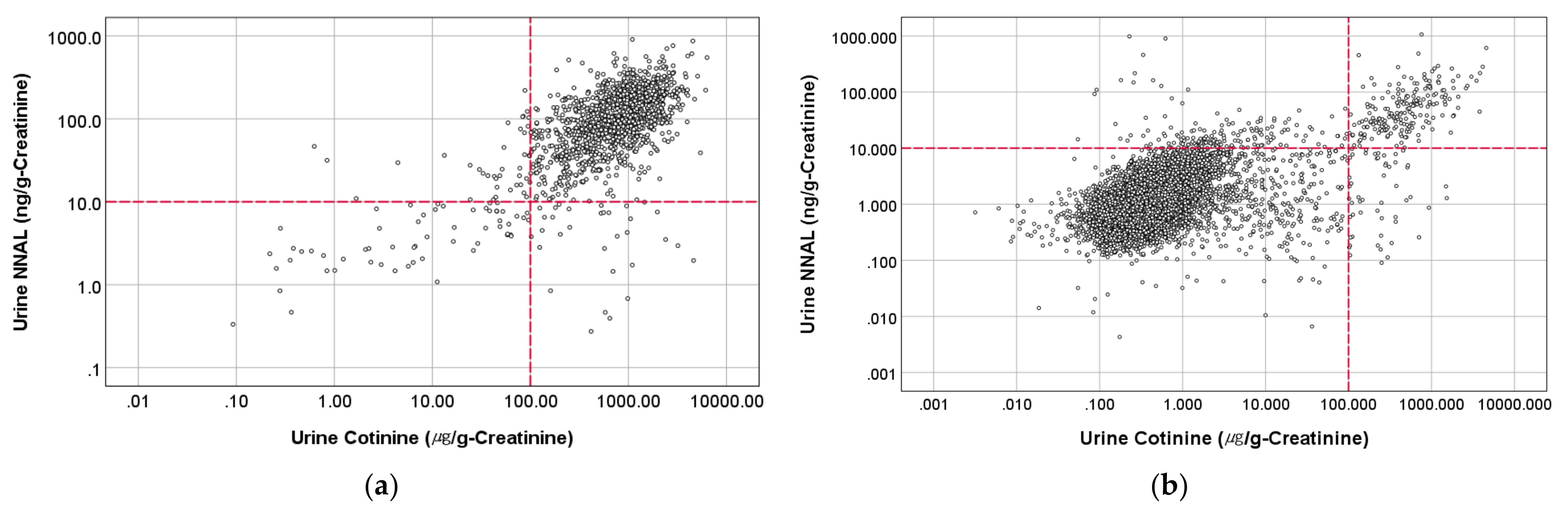
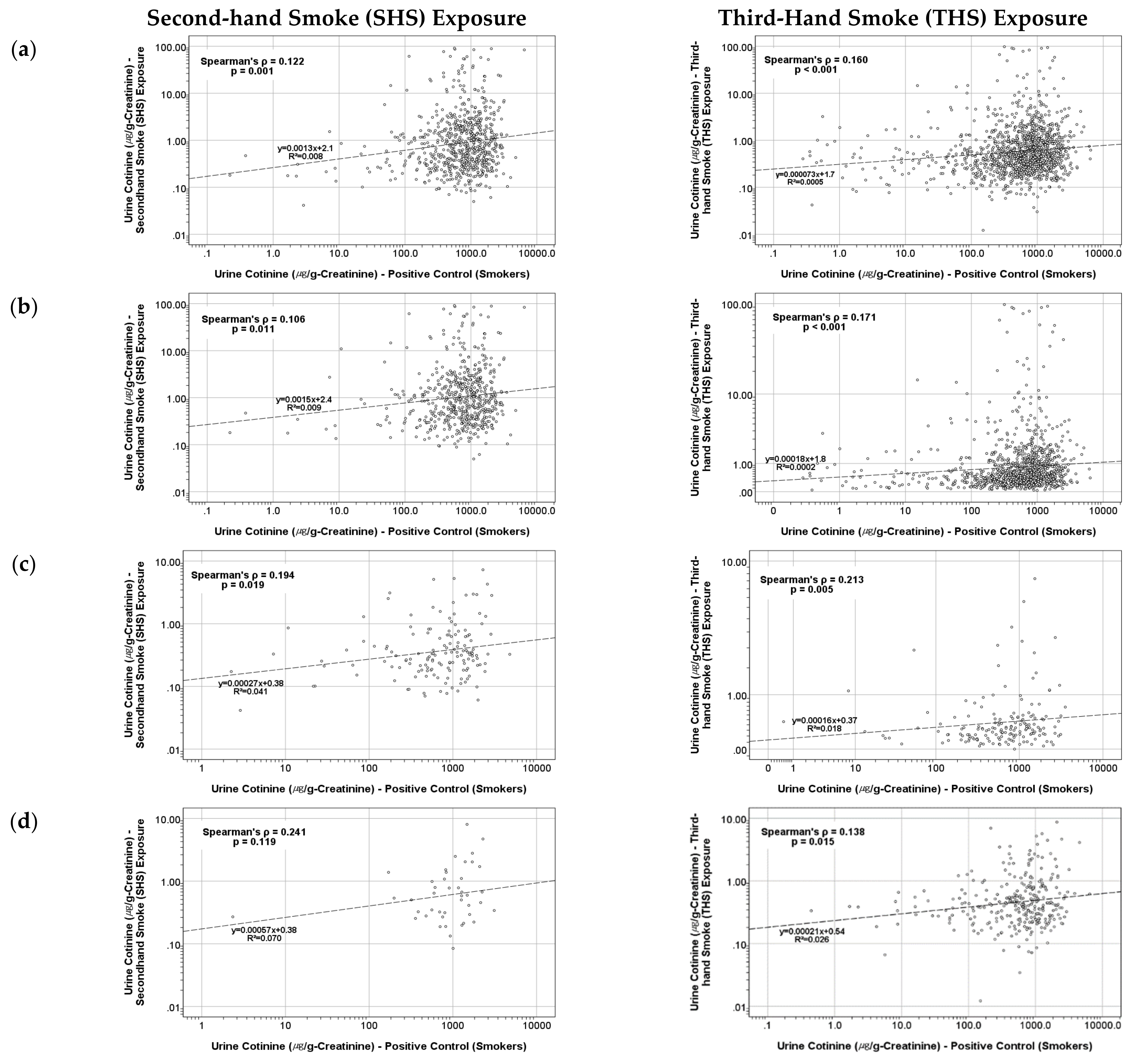
3.1. Correlation between the Urinary Smoking Exposure Biomarker of Active and Passive Smokers Living in the Same Family
3.2. Results of I-EDI for Nicotine and Equivalent Smoked Cigarettes per Day in Passive ETS Exposure Subjects
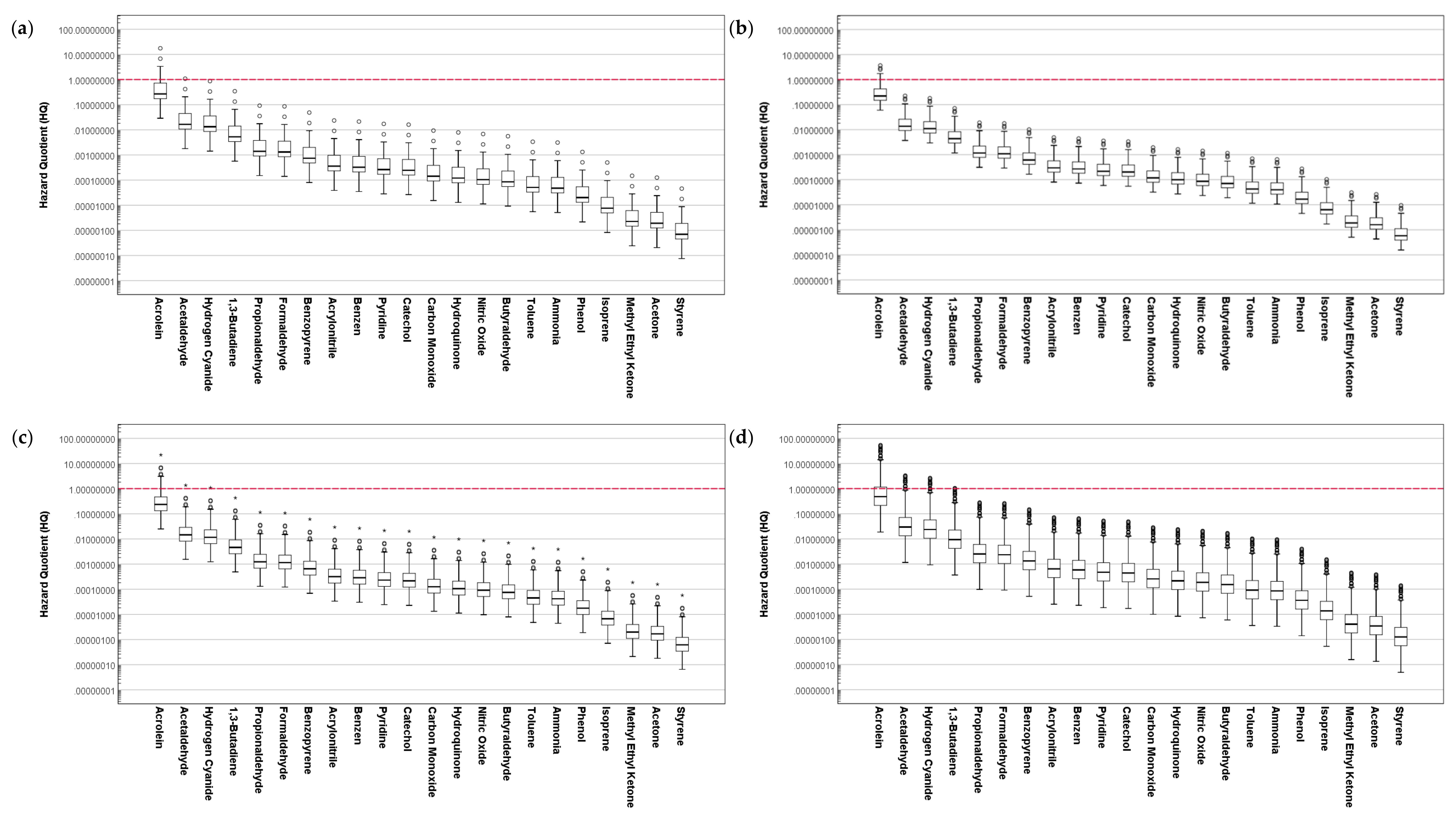
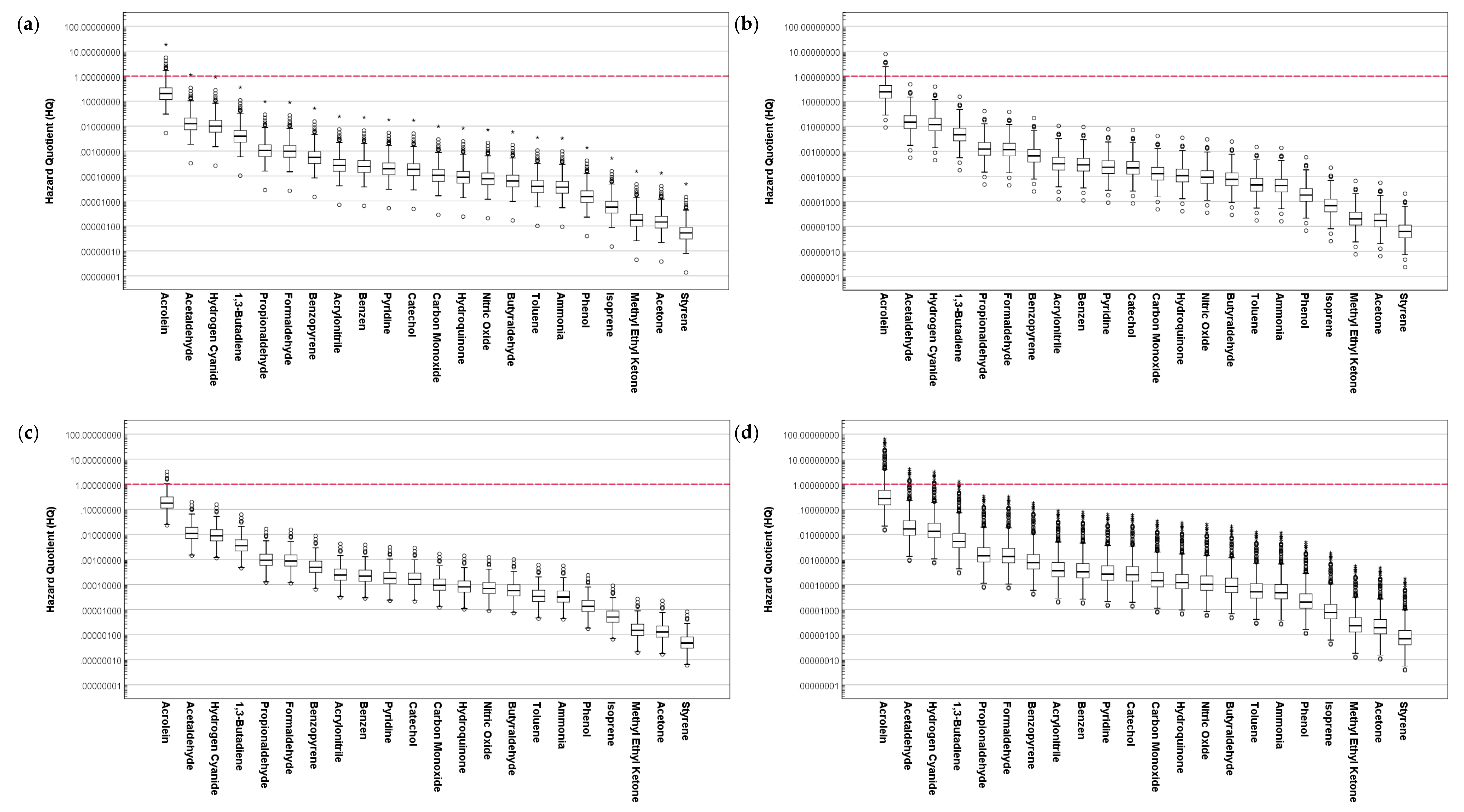
3.3. Results of Hazard Quotient Assessment for the Composition of Cigarette Smoke
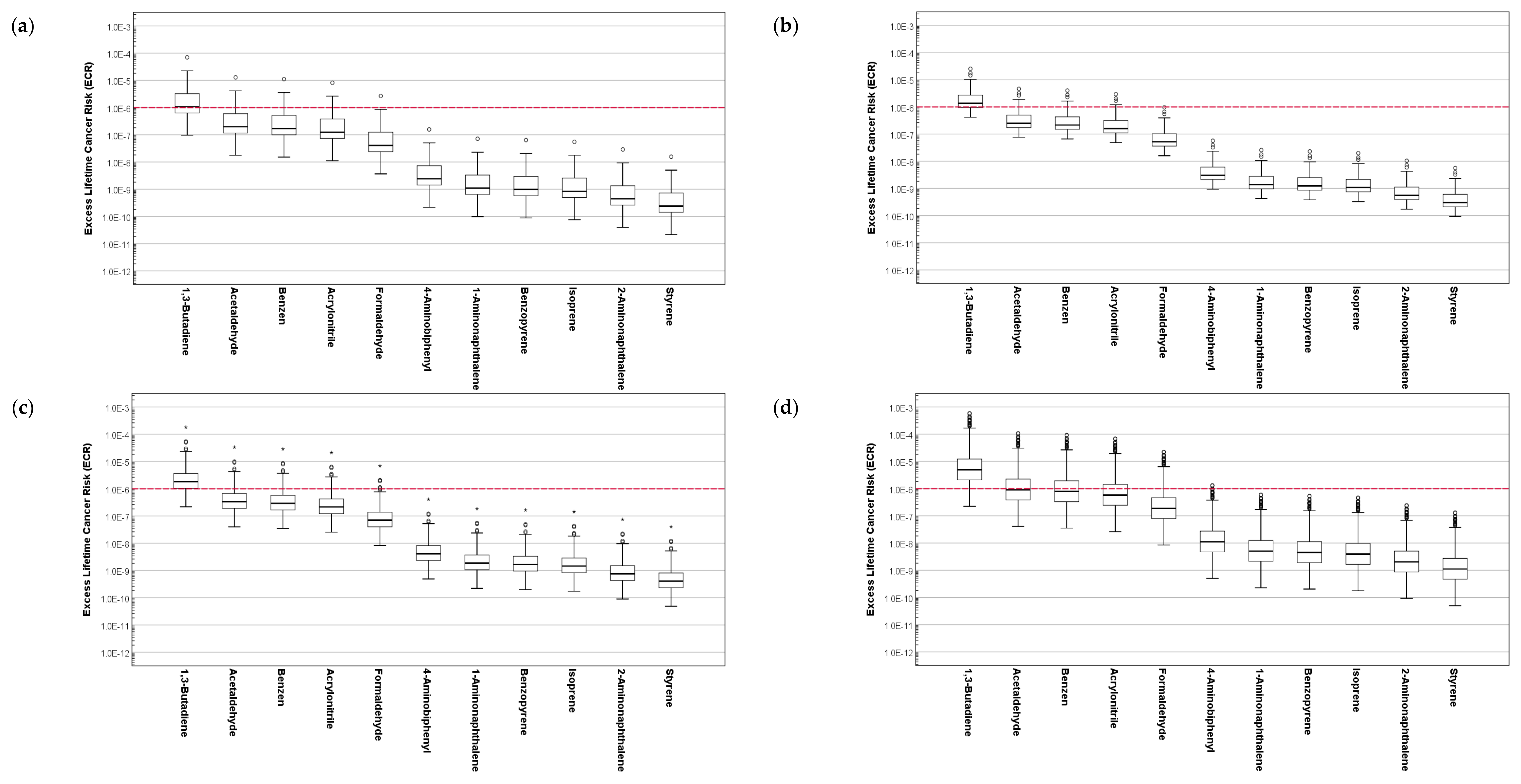
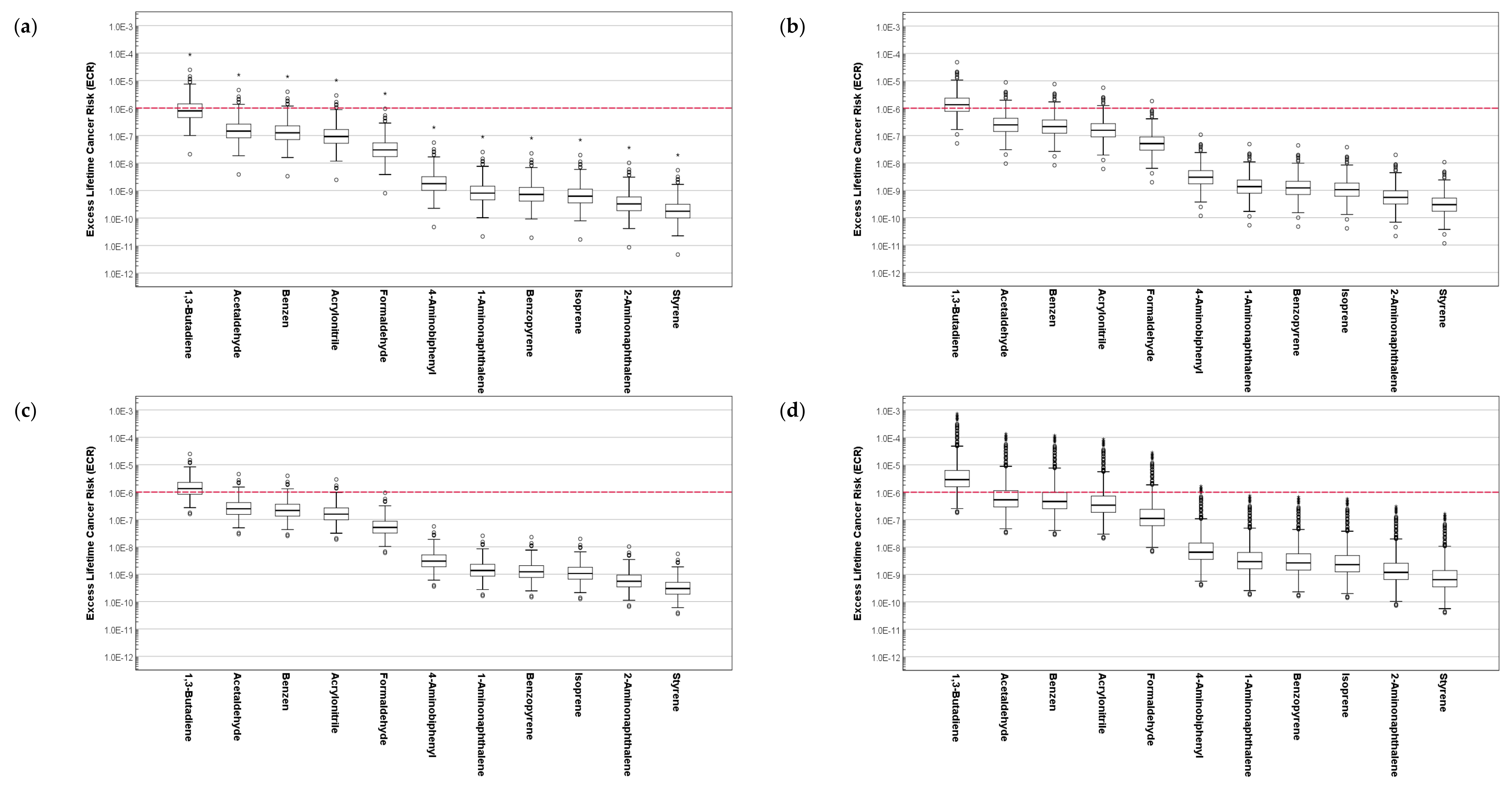
3.4. Results of Excess Lifetime Cancer Risk Assessment for the Composition of Cigarette Smoke
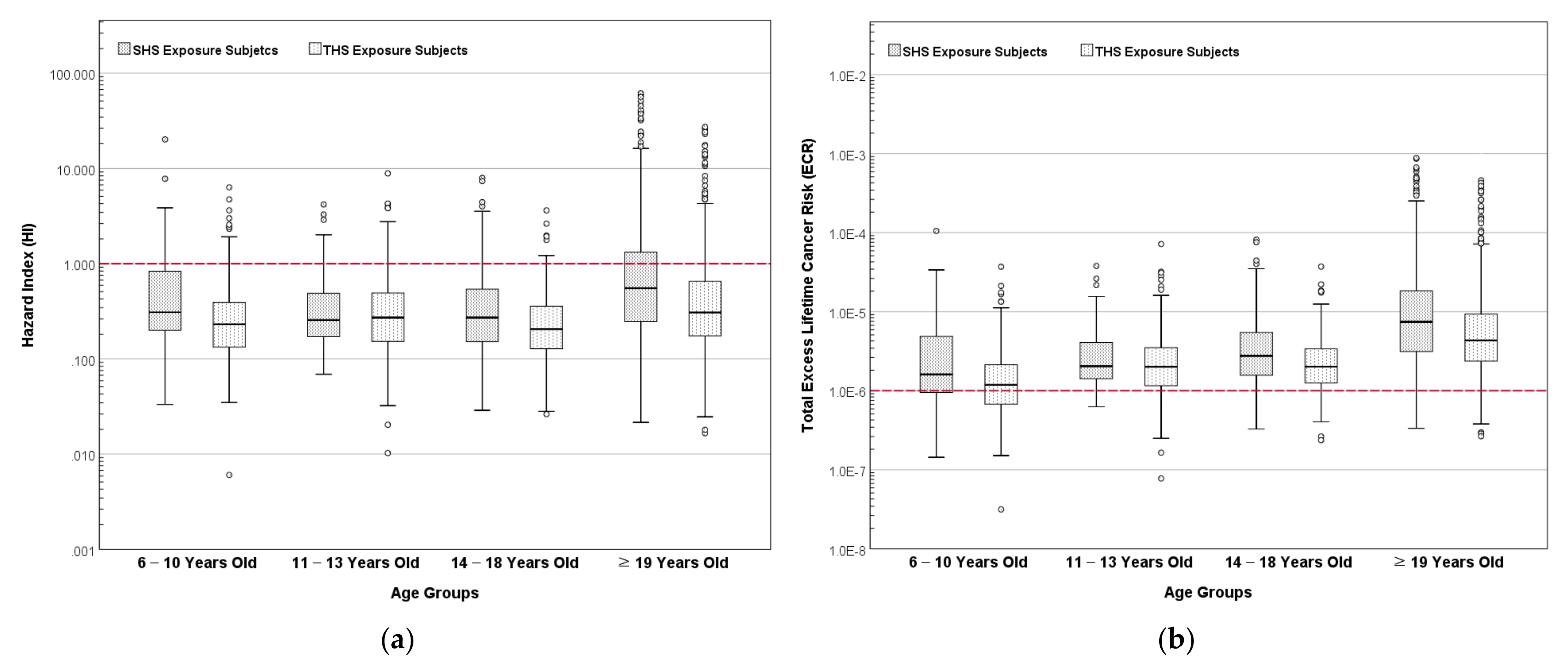
3.5. Results of Hazard Index and Total Excess Lifetime Cancer Risk for ETS Exposure Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| Abs | Absorption Rate |
| ADAF | Age-Dependent Adjustments Factor |
| ADD | Average Daily Dose |
| AT | Averaging Exposure Time |
| CPD | Cigarette per Day |
| ECR | Excess Lifetime Cancer Risk |
| ED | Exposure Duration |
| EF | Exposure Frequency |
| ETS | Exposure to Environmental Tobacco Smoke |
| FCTC | Framework Convention on Tobacco Control |
| HC | Health Canada |
| HI | Hazard Index |
| HPLC MS/MS | High-Performance Liquid Chromatography-Tandem Mass Spectroscopy |
| HQ | Hazard Quotient |
| I-EDI | Internal Estimated Daily Intake |
| IR | Inhalation Ratio |
| ISO | International Organization for Standardization |
| IUR | Inhalation Unit Risk |
| KNHANES | Korea National Health and Nutrition Examination Survey |
| LADD | Lifetime Average Daily Dose |
| NNAL | 4-(Methylnitrosamino)-1-(3-Pyridyl)-1-Butanol |
| RfC | Reference Concentration |
| SHS | Second-hand Smoke |
| THS | Third-hand Smoke |
| TSNAs | Tobacco-specific Nitrosamines |
| WHO | World Health Organization |
References
- Torres, S.; Merino, C.; Paton, B.; Correig, X.; Ramírez, N. Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives. Int. J. Environ. Res. Public Health 2018, 15, 2693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Tobacco. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 12 October 2021).
- Yousuf, H.; Hofstra, M.; Tijssen, J.; Leenen, B.; Lindemans, J.W.; van Rossum, A.; Narula, J.; Hofstra, L. Estimated Worldwide Mortality Attributed to Secondhand Tobacco Smoke Exposure, 1990–2016. JAMA Netw. Open 2020, 3, e201177. [Google Scholar] [CrossRef] [PubMed]
- Sadreameli, S.C.; Kopp, B.T.; Creary, S.E.; Eakin, M.N.; McGrath-Morrow, S.; Strouse, J.J. Secondhand Smoke Is an Important Modifiable Risk Factor in Sickle Cell Disease: A Review of the Current Literature and Areas for Future Research. Int. J. Environ. Res. Public Health 2016, 13, 1131. [Google Scholar] [CrossRef] [PubMed]
- Kopp, B.T.; Ortega-García, J.A.; Sadreameli, S.C.; Wellmerling, J.; Cormet-Boyaka, E.; Thompson, R.; McGrath-Morrow, S.; Groner, J.A. The Impact of Secondhand Smoke Exposure on Children with Cystic Fibrosis: A Review. Int. J. Environ. Res. Public Health 2016, 13, 1003. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.-S.; Ko, H.-J.; Kwon, J.-H.; Lee, J.-M. Exposure to Secondhand Smoke and Risk of Cancer in Never Smokers: A Meta-Analysis of Epidemiologic Studies. Int. J. Environ. Res. Public Health 2018, 15, 1981. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2003; ISBN 9789241591010. [Google Scholar]
- Woo, B.L.; Lim, M.K.; Park, E.Y.; Park, J.; Ryu, H.; Jung, D.; Ramirez, M.J.; Yang, W. Characteristics of Non-Smokers’ Exposure Using Indirect Smoking Indicators and Time Activity Patterns. Sustainability 2020, 12, 9099. [Google Scholar] [CrossRef]
- Hashemi, S. Sustainable Integrated Clean Environment for Human & Nature; MDPI: Basel, Switzerland, 2021; ISBN 9783036518817. [Google Scholar]
- Hashemi, S. Perspectives on Sustainable Integrated Clean Environment for Human and Nature. Sustainability 2021, 13, 4150. [Google Scholar] [CrossRef]
- United Nations. Goal 3 | Ensure Healthy Lives and Promote Well-Being for All at All Ages. Available online: https://sdgs.un.org/goals/goal3 (accessed on 8 January 2021).
- Yang, J.; Hashemi, S.; Han, W.; Lee, C.; Song, Y.; Lim, Y. Study on the daily Ad Libitum smoking habits of active Korean smokers and their effect on urinary smoking exposure and impact biomarkers. Biomarkers 2021, 26, 691–702. [Google Scholar] [CrossRef]
- Stratton, K.; Shetty, P.; Wallace, R.; Bondurant, S. Clearing the Smoke: Assessing the Science Base for Tobacco Harm Reduction; National Academy Press: Washington, DC, USA, 2001; ISBN 9780309072823. [Google Scholar]
- U.S. Department of Health and Human Services. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010; ISBN 9780160840784. [Google Scholar]
- Repace, J.L.; Lowrey, A.H. Risk Assessment Methodologies for Passive Smoking-Induced Lung Cancer. Risk Anal. 1990, 10, 27–37. [Google Scholar] [CrossRef]
- Thomas, C.E.; Wang, R.; Adams-Haduch, J.; Murphy, S.E.; Ueland, P.M.; Midttun, Ø.; Brennan, P.; Johansson, M.; Gao, Y.-T.; Yuan, J.-M. Urinary Cotinine Is as Good a Biomarker as Serum Cotinine for Cigarette Smoking Exposure and Lung Cancer Risk Prediction. Cancer Epidemiol. Biomark. Prev. 2020, 29, 127–132. [Google Scholar] [CrossRef]
- Yang, J.; Hashemi, S.; Han, W.; Lee, C.; Kang, Y.; Lim, Y. Korean male active smokers: Quantifying their smoking habits and the transformation factor among biomarkers in urine and blood. Biomarkers 2020, 25, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Lee, I.S.; Kim, S.B.; Moon, C.S.; Jung, J.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; et al. Urine Cotinine for Assessing Tobacco Smoke Exposure in Korean: Analysis of the Korea National Health and Nutrition Examination Survey (KNHANES). Tuberc. Respir. Dis. 2012, 73, 210. [Google Scholar] [CrossRef]
- Benowitz, N.L.; St. Helen, G.; Nardone, N.; Cox, L.S.; Jacob, P. Urine Metabolites for Estimating Daily Intake of Nicotine From Cigarette Smoking. Nicotine Tob. Res. 2020, 22, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Marano, K.M.; Liu, C.; Fuller, W.; Gentry, P.R. Quantitative risk assessment of tobacco products: A potentially useful component of substantial equivalence evaluations. Regul. Toxicol. Pharmacol. 2018, 95, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data Resource Profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Disease Control and Prevention Agency. The Seventh Korea National Health and Nutrition Examination Survey (KNHANES VII). Available online: https://knhanes.kdca.go.kr/knhanes/main.do (accessed on 22 October 2021).
- Kim, S. Overview of Cotinine Cutoff Values for Smoking Status Classification. Int. J. Environ. Res. Public Health 2016, 13, 1236. [Google Scholar] [CrossRef]
- Ministry of Food and Drug Safety. Ministry of Food and Drug Safety Announces the Content of Harmful Ingredients in Cigarettes and E-Cigarettes at the Government Level. Available online: https://www.mfds.go.kr/brd/m_99/view.do?seq=36783 (accessed on 19 July 2021).
- National Institute of Food and Drug Safety. Evaluation Tobacco Analysis Method, Tobacco Mainstream Smoke Component Analysis Method—45 Components Including Nicotine and Benzopyrene. Available online: https://mfds.go.kr/brd/m_218/down.do?brd_id=data0013&seq=33257&data_tp=A&file_seq=1 (accessed on 17 June 2021).
- ISO 8243:2013 Cigarettes—Sampling; International Organization for Standardization: Geneva, Switzerland, 2013.
- California Environmental Protection Agency. Toxicity Criteria on Chemicals Evaluated by OEHHA. Available online: http://oehha.ca.gov/chemicals (accessed on 22 October 2021).
- US Environmental Protection Agency. US EPA Integrated Risk Information System (IRIS). Available online: https://www.epa.gov/iris (accessed on 14 October 2020).
- Agency for Toxic Substances and Disease Registry. Minimal Risk Levels (MRLs) for Hazardous Substances. Available online: https://wwwn.cdc.gov/TSP/MRLS/mrlsListing.aspx (accessed on 22 October 2021).
- Texas Commission on Environmental Quality. TRRP Protective Concentration Levels. Available online: https://www.tceq.texas.gov/remediation/trrp/trrppcls.html (accessed on 22 October 2021).
- Baars, A.J.; Theelen, R.M.C.; Janssen, P.; Hesse, J.M.; Van Apeldoorn, M.E.; Meijerink, M.C.M.; Verdam, L.; Zeilmaker, M.J. Re-Evaluation of Human-Toxicological Maximum Permissible Risk Levels; RIVM Report 711701 025; National Institute for Public Health and the Environment (RIVM): Bilthoven, The Netherlands, 2001. [Google Scholar]
- Michigan Department of Environmental Quality. Cleanup Criteria and Screening Levels Development and Application; Michigan Department of Environmental Quality, Remediation and Redevelopment Division: Lansing, MI, USA, 2016. [Google Scholar]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P., III. Nicotine Chemistry, Metabolism, Kinetics and Biomarkers. In Handbook of Experimental Pharmacology; Henningfield, J.E., London, E.D., Pogun, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 29–60. ISBN 9783540692461. [Google Scholar]
- Kang, W.H.; Seo, G.H.; Lee, B.H.; Kim, B.; Lee, S.K.; Oh, D.J.; Huh, W.; Kim, Y.G.; Kim, D.J.; Oh, H.Y. Estimation of creatinine clearance with serum creatinine in Korean patients. Korean J. Nephrol. 1998, 17, 866–871. [Google Scholar]
- US Environmental Protection Agency. Risk Assessment Guidance for Superfund Volume 1 Human Health Evaluation Manual (Part F, Supplemental Guidance for Inhalation Risk Assessment); United States Environmental Protection Agency: Washington, DC, USA, 2009. [Google Scholar]
- National Institute of Environmental Research. Korean Exposure Factors Handbook; National Institute of Environmental Research: Incheon, Korea, 2019. [Google Scholar]
- National Institute of Environmental Research. Korean Exposure Factors Handbook for Children; National Institute of Environmental Research: Incheon, Korea, 2019. [Google Scholar]
- Jeong, S.H.; Jang, B.N.; Kang, S.H.; Joo, J.H.; Park, E.-C. Association between parents’ smoking status and tobacco exposure in school-age children: Assessment using major urine biomarkers. Sci. Rep. 2021, 11, 4536. [Google Scholar] [CrossRef]
- Mahabee-Gittens, E.M.; Matt, G.E.; Hoh, E.; Quintana, P.J.E.; Stone, L.; Geraci, M.A.; Wullenweber, C.A.; Koutsounadis, G.N.; Ruwe, A.G.; Meyers, G.T.; et al. Contribution of thirdhand smoke to overall tobacco smoke exposure in pediatric patients: Study protocol. BMC Public Health 2019, 19, 491. [Google Scholar] [CrossRef]
- Chan, S.S.; Lam, T.H.; Betson, C.L. Passive smoking exposure of sick children in Hong Kong. Hum. Exp. Toxicol. 1999, 18, 224–228. [Google Scholar] [CrossRef]
- Nadhiroh, S.; Djokosujono, K.; Utari, D.M. The association between secondhand smoke exposure and growth outcomes of children: A systematic literature review. Tob. Induc. Dis. 2020, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Parks, J.; McLean, K.E.; McCandless, L.; de Souza, R.J.; Brook, J.R.; Scott, J.; Turvey, S.E.; Mandhane, P.J.; Becker, A.B.; Azad, M.B.; et al. Assessing secondhand and thirdhand tobacco smoke exposure in Canadian infants using questionnaires, biomarkers, and machine learning. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Vitória, P.D.; Machado, J.C.; Araújo, A.C.; Ravara, S.B.; Samorinha, C.; Antunes, H.; Rosas, M.; Becoña, E.; Precioso, J. Children’s exposure to second hand smoke at home: A cross-sectional study in Portugal. Rev. Port. Pneumol. (English Ed.) 2015, 21, 178–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selection Step | Subjects Description | Number of Subjects | Level of Urinary Cotinine (μg/g-Creatinine) Mean ± SD (Min–Max) |
|---|---|---|---|
| 0 | Everyone with valid data in the KNHANES VII dataset | 17,686 | 189.7 ± 503.3 (0.0014~6446) |
| 1 | All non-smokers (including former smokers) in the KNHANES VII dataset | 14,333 | 27.5 ± 182.2 (0.0014~5324) |
| 2 | Non-smokers and former smokers who are living in a family, including at least one smoker | 3233 | 35.4 ± 222.2 (0.012~4571) |
| 3 | Excluding subjects with urinary cotinine levels above 100 μg/g-creatinine | 2736 | 1.86 ± 7.19 (0.012~93.8) |
| Items (Unit) | Positive Control (Active Smokers) | Passive ETS Exposure | |||||
|---|---|---|---|---|---|---|---|
| n | Value (% or Mean ± SD) | Second-Hand Smoke (SHS)Exposure | Third-Hand Smoke (THS)Exposure | ||||
| n | Value (% or Mean ± SD) | n | Value (% or Mean ± SD) | ||||
| Gender | Male | 2704 | 84.4% | 210 | 24.1% | 409 | 21.9% |
| Female | 499 | 15.6% | 660 | 75.9% | 1457 | 78.1% | |
| Age Range (Years) | 6–10 | - | - | 53 | 6.1% | 348 | 18.6% |
| 11–13 | - | - | 66 | 7.6% | 136 | 7.3% | |
| 14–18 | - | - | 117 | 13.4% | 115 | 6.2% | |
| ≥19 | 3203 | 100% | 634 | 72.9% | 1267 | 67.9% | |
| Body Weight (kg) | 3201 | 69.8 ± 13.1 | 870 | 58.8 ± 14.5 | 1866 | 53.5 ± 15.3 | |
| Body Mass Index (kg/m2) | 3198 | 24.2 ± 3.68 | 870 | 23.0 ± 4.25 | 1864 | 22.1 ± 4.42 | |
| Residence Region | Seoul | 554 | 17.3% | 116 | 13.3% | 354 | 19.0% |
| Busan | 207 | 6.5% | 67 | 7.7% | 106 | 5.7% | |
| Daegu | 148 | 4.6% | 44 | 5.1% | 78 | 4.2% | |
| Incheon | 184 | 5.7% | 55 | 6.3% | 122 | 6.5% | |
| Gwangju | 95 | 3.0% | 27 | 3.1% | 55 | 2.9% | |
| Daejeon | 109 | 3.4% | 33 | 3.8% | 67 | 3.6% | |
| Ulsan | 73 | 2.3% | 33 | 3.8% | 31 | 1.7% | |
| Sejong | 53 | 1.7% | 21 | 2.4% | 32 | 1.7% | |
| Gyeonggi-do | 814 | 25.4% | 188 | 21.6% | 498 | 26.7% | |
| Gangwon-do | 104 | 3.2% | 24 | 2.8% | 53 | 2.8% | |
| Chungcheongbuk-do | 96 | 3.0% | 24 | 2.8% | 46 | 2.5% | |
| Chungcheongnam-do | 122 | 3.5% | 34 | 3.9% | 55 | 2.9% | |
| Jeollabuk-do | 99 | 3.1% | 20 | 2.3% | 60 | 3.2% | |
| Jeollanam-do | 106 | 3.3% | 32 | 3.7% | 79 | 4.2% | |
| Gyeongsangbuk-do | 190 | 5.9% | 69 | 7.9% | 89 | 4.8% | |
| Gyeongsangnam-do | 177 | 5.5% | 60 | 6.9% | 91 | 4.9% | |
| Jeju Special Self-governing Province | 72 | 2.2% | 23 | 2.6% | 50 | 2.7% | |
| Education Level | Elementary School or Lower | 373 | 11.6% | 264 | 30.3% | 744 | 39.9% |
| Middle School | 311 | 9.7% | 148 | 17.0% | 177 | 9.5% | |
| High School | 1243 | 38.8% | 25 | 2.9% | 446 | 23.9% | |
| College or Higher | 1127 | 35.2% | 178 | 20.5% | 459 | 24.6% | |
| No Answer (Unknown) | 149 | 4.7% | 255 | 29.3% | 40 | 2.1% | |
| Urinary Cotinine (μg/g-creatinine) | 3203 | 912.7 ± 772.2 | 870 | 2.82 ± 8.90 | 1866 | 1.42 ± 6.20 | |
| Compound | Concentration in Main Stream of Cigarette Smoke (μg/Cig) | Inhalation Toxicity Value | |||
|---|---|---|---|---|---|
| Mean ± SD | Range (Min–Max) | Reference Concentration (mg/m3) | Inhalation Unit Risk (per μg/m3) | Reference | |
| Nicotine | 470 ± 44.7 | 400–500 | - | - | - |
| 1-Aminonaphthalene | 0.0068 ± 0.002 | 0.0056–0.0095 | - | 5.14 × 10−4 | [20] |
| 1,3-Butadiene | 20.1 ± 4.75 | 15.0–26.1 | 0.002 | 0.00017 | [27] |
| 2-Aminonaphthalene | 0.0027 ± 0.001 | 0.0020–0.0043 | - | 5.14 × 10−4 | [20] |
| 4-Aminobiphenyl | 0.0013 ± 0.0002 | 0.0011–0.0016 | - | 0.006 | [27] |
| Acetaldehyde | 285.0 ± 44.1 | 224.7–327.2 | 0.009 | 2.20 × 10−6 | [28] |
| Acetone | 113.5 ± 11.0 | 104.5–127.4 | 30.9 | - | [29] |
| Acrolein | 10.3 ± 1.24 | 8.80–11.4 | 2.00 × 10−5 | - | [28] |
| Acrylonitrile | 1.38 ± 0.70 | 0.80–2.40 | 0.002 | 2.90 × 10−4 | [27] |
| Ammonia | 6.38 ± 1.0 | 5.30–7.80 | 0.07 | - | [29] |
| Benzene | 18.7 ± 4.31 | 13.0–23.8 | 0.03 | 2.90 × 10−5 | [27] |
| Benzopyrene | 0.003 ± 0.001 | 0.0017–0.0045 | 2.00 × 10−6 | 0.0011 | [28] |
| Butyraldehyde | 16.3 ± 2.81 | 13.8–19.5 | 0.1 | - | [30] |
| Carbon Monoxide | 6280 ± 1535.3 | 3700–7500 | 23 | - | [27] |
| Catechol | 65.8 ± 12.5 | 47.0–80.5 | 0.14 | - | [31] |
| Formaldehyde | 10.0 ± 2.62 | 8.20–14.3 | 0.004 | 1.30 × 10−5 | [28] |
| Hydrogen Cyanide | 20.3 ± 3.16 | 15.9–23.8 | 0.0008 | - | [28] |
| Hydroquinone | 20.2 ± 2.96 | 15.5–23.5 | 0.088 | - | [31] |
| Isoprene | 122.6 ± 26.0 | 91.7–158.3 | 8.4 | 2.20 × 10−8 | [30] |
| Methyl Ethyl Ketone | 21.6 ± 1.91 | 19.6–24.1 | 5 | - | [28] |
| Nitric Oxide | 93.7 ± 27.6 | 52.3–129.9 | 0.47 | - | [27] |
| Phenol | 7.32 ± 2.64 | 3.10–9.70 | 0.19 | - | [32] |
| Propionaldehyde | 21.5 ± 3.83 | 17.4–25.7 | 0.008 | - | [28] |
| Pyridine | 1.76 ± 0.47 | 1.00–2.20 | 0.0035 | - | [32] |
| Styrene | 1.34 ± 0.40 | 0.80–1.80 | 1 | 5.70 × 10−7 | [28,32] |
| Toluene | 29.4 ± 4.94 | 22.4–35.9 | 0.3 | - | [27] |
| i-Value | Age Range | ED (Years) | ADAF | IR (m3/day) | Reference | |
|---|---|---|---|---|---|---|
| Male | Female | |||||
| 1 | 0–2 | 2 | 10 | 9.80 | 9.25 | [36,37] |
| 2 | 3–5 | 3 | 3 | 10.96 | 9.62 | |
| 3 | 6–8 | 3 | 3 | 11.39 | 10.08 | |
| 4 | 9–11 | 3 | 3 | 12.49 | 11.65 | |
| 5 | 12–15 | 4 | 3 | 15.55 | 12.66 | |
| 6 | ≥16 | Current Age–16 | 1 | 16.43 | 13.64 | |
| Variable | Subjects | Groups | ||||||
|---|---|---|---|---|---|---|---|---|
| All | Gender | Age Range (Years) | ||||||
| Male | Female | 6–10 | 11–13 | 14–18 | ≥19 | |||
| Nicotine I-EDI (μg-nicotine/day) Mean ± SD (min–max) | SHS Exposure | 20.3 ± 61.6 (0.27–643.7) | 15.8 ± 37.1 (0.84–335.2) | 21.8 ± 67.5 (0.27–643.7) | 10.4 ± 27.1 (0.27–185.1) | 5.65 ± 8.44 (0.84–51.0) | 10.8 ± 34.0 (0.36–335.2) | 24.4 ± 69.7 (0.30–643.7) |
| THS Exposure | 9.77 ± 44.0 (0.06–718.7) | 7.41 ± 35.9 (0.06–678.4) | 10.4 ± 46.0 (0.11–718.7) | 4.1 ± 11.2 (0.06–187.3) | 5.94 ± 11.3 (0.11–100.4) | 4.01 ± 6.04 (0.28–48.6) | 12.3 ± 52.7 (0.17–718.7) | |
| Equivalent CPD (Cig/day) Mean ± SD (min–max) | SHS Exposure | 0.04 ± 0.13 (0.0006–1.37) | 0.03 ± 0.08 (0.002–0.71) | 0.05 ± 0.14 (0.0006–1.37) | 0.02 ± 0.06 (0.0006–0.40) | 0.01 ± 0.02 (0.002–0.11) | 0.02 ± 0.07 (0.001–0.71) | 0.05 ± 0.15 (0.0007–1.37) |
| THS Exposure | 0.02 ± 0.09 (0.0001–1.53) | 0.02 ± 0.08 (0.0001–1.44) | 0.02 ± 0.10 (0.0002–1.53) | 0.01 ± 0.02 (0.0001–0.40) | 0.01 ± 0.02 (0.0002–0.21) | 0.01 ± 0.01 (0.0006–0.10) | 0.03 ± 0.11 (0.0004–1.53) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Hashemi, S.; Han, W.; Song, Y.; Lim, Y. Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 3746. https://doi.org/10.3390/ijerph19063746
Yang J, Hashemi S, Han W, Song Y, Lim Y. Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea. International Journal of Environmental Research and Public Health. 2022; 19(6):3746. https://doi.org/10.3390/ijerph19063746
Chicago/Turabian StyleYang, Jiyeon, Shervin Hashemi, Wonseok Han, Yoojin Song, and Youngwook Lim. 2022. "Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea" International Journal of Environmental Research and Public Health 19, no. 6: 3746. https://doi.org/10.3390/ijerph19063746
APA StyleYang, J., Hashemi, S., Han, W., Song, Y., & Lim, Y. (2022). Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea. International Journal of Environmental Research and Public Health, 19(6), 3746. https://doi.org/10.3390/ijerph19063746