
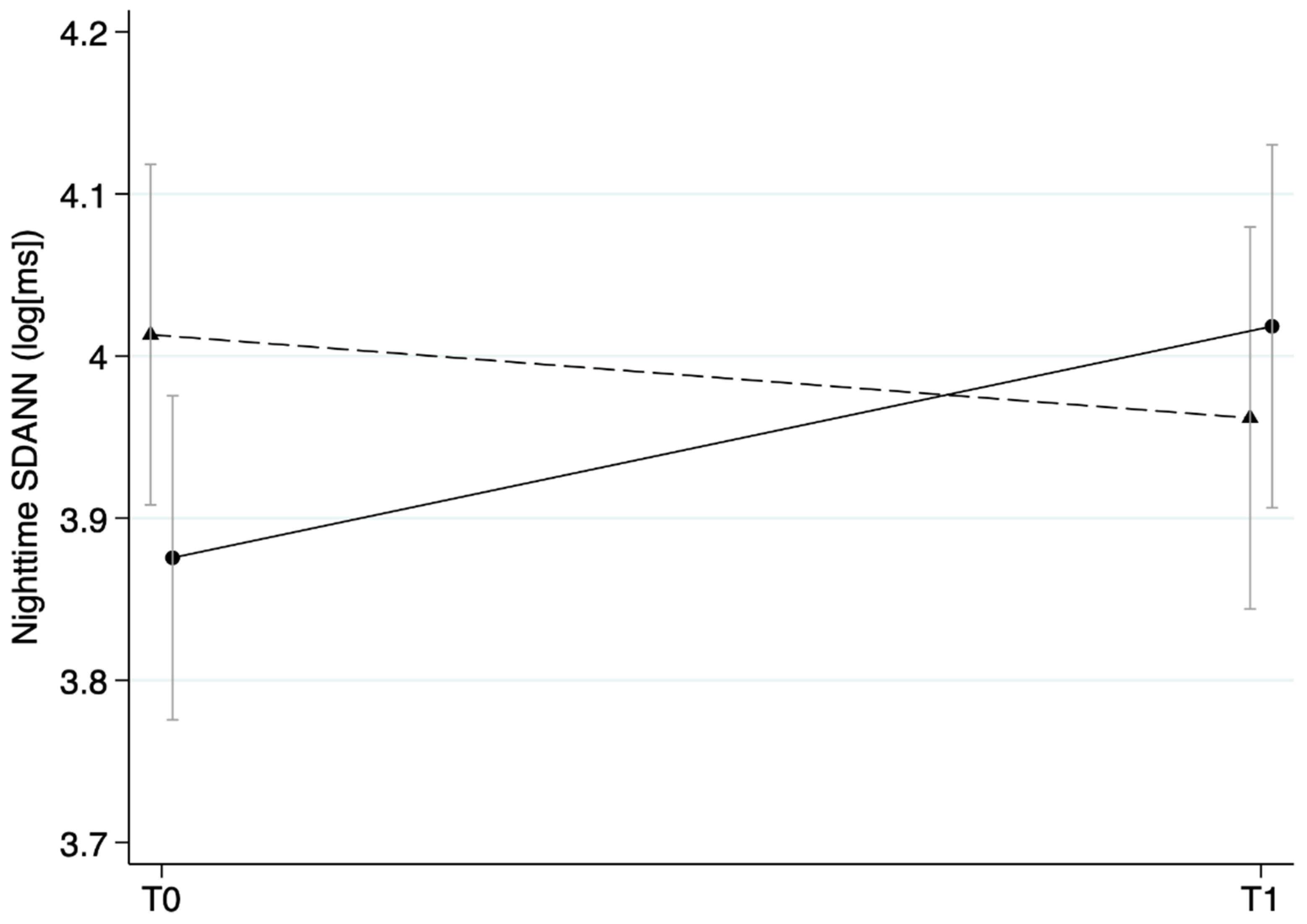
Stress Management Intervention for Leaders Increases Nighttime SDANN: Results from a Randomized Controlled Trial
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
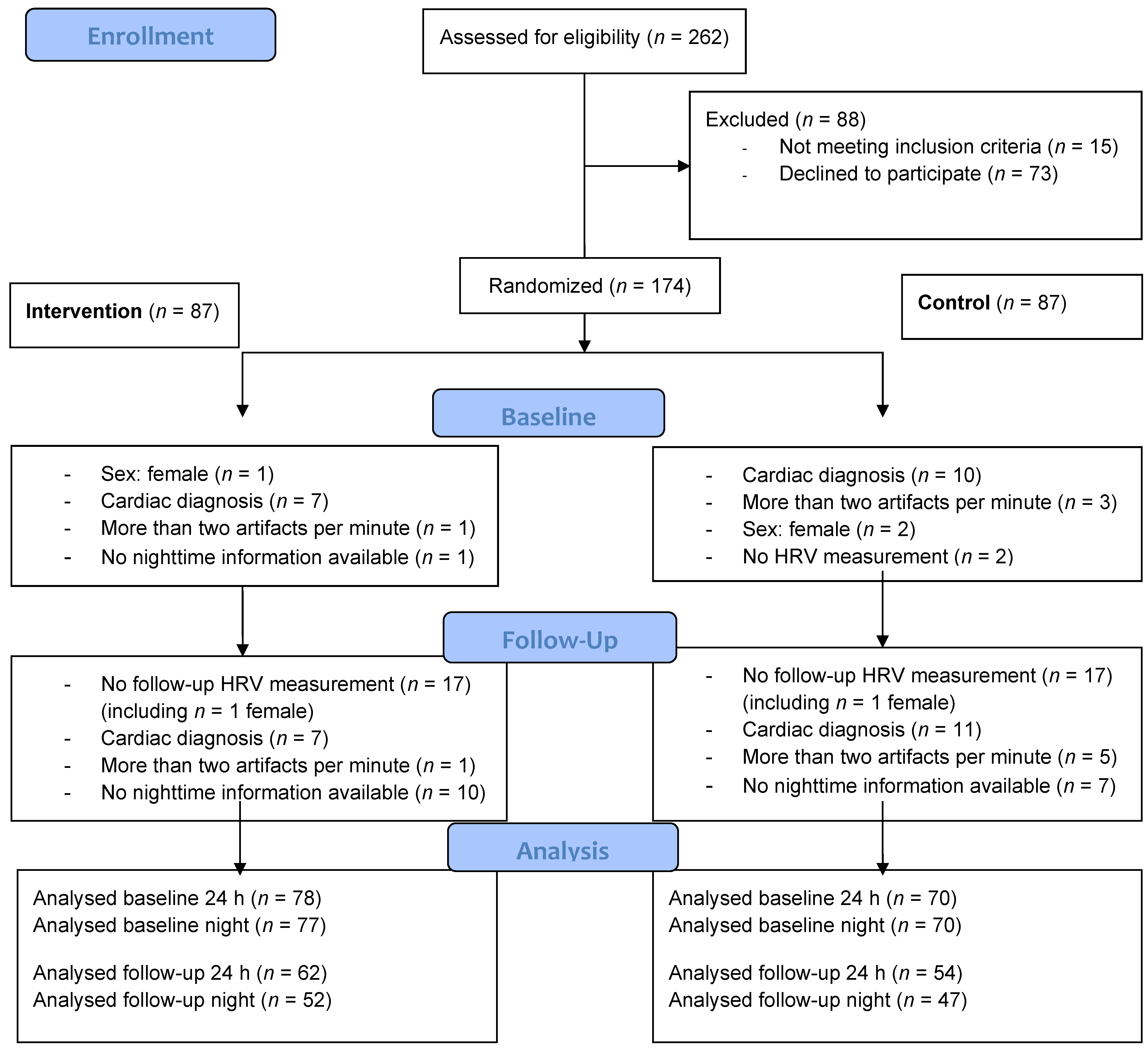
2.1. Participants and Procedures
2.2. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Urtasun, A.; Nuñez, I. Healthy Working Days: The (Positive) Effect of Work Effort on Occupational Health from a Human Capital Approach. Soc. Sci. Med. 2018, 202, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Sara, J.D.; Prasad, M.; Eleid, M.F.; Zhang, M.; Jay Widmer, R.; Lerman, A. Association between Work-Related Stress and Coronary Heart Disease: A Review of Prospective Studies through the Job Strain, Effort-Reward Balance, and Organizational Justice Models. J. Am. Heart Assoc. 2018, 7, 8073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivimäki, M.; Nyberg, S.T.; Batty, G.D.; Fransson, E.I.; Heikkilä, K.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; et al. Job Strain as a Risk Factor for Coronary Heart Disease: A Collaborative Meta-Analysis of Individual Participant Data. Lancet 2012, 380, 1491–1497. [Google Scholar] [CrossRef] [Green Version]
- Madsen, I.E.H.; Nyberg, S.T.; Magnusson Hanson, L.L.; Ferrie, J.E.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Job Strain as a Risk Factor for Clinical Depression: Systematic Review and Meta-Analysis with Additional Individual Participant Data. Psychol. Med. 2017, 47, 1342–1356. [Google Scholar] [CrossRef] [Green Version]
- Theorell, T.; Hammarström, A.; Aronsson, G.; Träskman Bendz, L.; Grape, T.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Hall, C. A Systematic Review Including Meta-Analysis of Work Environment and Depressive Symptoms. BMC Public Health 2015, 15, 738. [Google Scholar] [CrossRef] [Green Version]
- Harvey, S.B.; Sellahewa, D.A.; Wang, M.J.; Milligan-Saville, J.; Bryan, B.T.; Henderson, M.; Hatch, S.L.; Mykletun, A. The Role of Job Strain in Understanding Midlife Common Mental Disorder: A National Birth Cohort Study. Lancet Psychiatry 2018, 5, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Kivimäki, M.; Steptoe, A. Effects of Stress on the Development and Progression of Cardiovascular Disease. Nat. Rev. Cardiol. 2018, 15, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Pentti, J.; Ferrie, J.E.; Batty, G.D.; Nyberg, S.T.; Jokela, M.; Virtanen, M.; Alfredsson, L.; Dragano, N.; Fransson, E.I.; et al. Work Stress and Risk of Death in Men and Women with and without Cardiometabolic Disease: A Multicohort Study. Lancet Diabetes Endocrinol. 2018, 6, 705–713. [Google Scholar] [CrossRef]
- Magnusson Hanson, L.L.; Westerlund, H.; Goldberg, M.; Zins, M.; Vahtera, J.; Hulvej Rod, N.; Stenholm, S.; Steptoe, A.; Kivimäki, M. Work Stress, Anthropometry, Lung Function, Blood Pressure, and Blood-Based Biomarkers: A Cross-Sectional Study of 43,593 French Men and Women. Sci. Rep. 2017, 7, 9282. [Google Scholar] [CrossRef]
- Albus, C.; Waller, C.; Fritzsche, K.; Gunold, H.; Haass, M.; Hamann, B.; Kindermann, I.; Köllner, V.; Leithäuser, B.; Marx, N.; et al. Significance of Psychosocial Factors in Cardiology: Update 2018: Position Paper of the German Cardiac Society. Clin. Res. Cardiol. 2019, 108, 1175–1196. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical PracticeDeveloped by the Task Force for Cardiovascular Disease Prevention in Clinical Practice with Representatives of the European Society of Cardiology and 12 Medical Societies With the Special Contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [PubMed]
- Zänkert, S.; Bellingrath, S.; Wüst, S.; Kudielka, B.M. HPA Axis Responses to Psychological Challenge Linking Stress and Disease: What Do We Know on Sources of Intra- and Interindividual Variability? Psychoneuroendocrinology 2019, 105, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Mather, M.; Koenig, J. Stress and Aging: A Neurovisceral Integration Perspective. Psychophysiology 2021, 58, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Benarroch, E.E. Central Autonomic Network. In Autonomic Neurology; Oxford University Press: Oxford, UK, 2014; pp. 3–14. [Google Scholar]
- Thayer, J.F.; Åhs, F.; Fredrikson, M.; Sollers, J.J.; Wager, T.D. A Meta-Analysis of Heart Rate Variability and Neuroimaging Studies: Implications for Heart Rate Variability as a Marker of Stress and Health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Thayer, J.F.; Vedhara, K. Stress and Health: A Review of Psychobiological Processes. Annu. Rev. Psychol. 2021, 72, 663–688. [Google Scholar] [CrossRef]
- Makovac, E.; Thayer, J.F.; Ottaviani, C. A Meta-Analysis of Non-Invasive Brain Stimulation and Autonomic Functioning: Implications for Brain-Heart Pathways to Cardiovascular Disease. Neurosci. Biobehav. Rev. 2017, 74, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Wulsin, L.; Herman, J.; Thayer, J.F. Stress, Autonomic Imbalance, and the Prediction of Metabolic Risk: A Model and a Proposal for Research. Neurosci. Biobehav. Rev. 2018, 86, 12–20. [Google Scholar] [CrossRef]
- Jarczok, M.N.; Li, J.; Mauss, D.; Fischer, J.E.; Thayer, J.F. Heart Rate Variability Is Associated with Glycemic Status after Controlling for Components of the Metabolic Syndrome. Int. J. Cardiol. 2013, 167, 855–861. [Google Scholar] [CrossRef]
- Kemp, A.H.; Brunoni, A.R.; Santos, I.S.; Nunes, M.A.; Dantas, E.M.; Carvalho de Figueiredo, R.; Pereira, A.C.; Ribeiro, A.L.P.; Mill, J.G.; Andreão, R.V.; et al. Effects of Depression, Anxiety, Comorbidity, and Antidepressants on Resting-State Heart Rate and Its Variability: An ELSA-Brasil Cohort Baseline Study. Am. J. Psychiatry 2014, 171, 1328–1334. [Google Scholar] [CrossRef] [Green Version]
- Kemp, A.H.; Koenig, J.; Thayer, J.F. From Psychological Moments to Mortality: A Multidisciplinary Synthesis on Heart Rate Variability Spanning the Continuum of Time. Neurosci. Biobehav. Rev. 2017, 83, 547–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarczok, M.N.; Koenig, J.; Fischer, J.E.; Hoffmann, K.; Schmidt, B.; Mauss, D.; Thayer, J.F. Circadian Variation of Cardiac Autonomic Modulation in a Rigorously Healthy Working Population: Results from the MICS-Cohort. Psychosom. Med. 2015, 77, 1. [Google Scholar]
- Jarczok, M.N.; Guendel, H.; McGrath, J.J.; Balint, E.M. Circadian Rhythms of the Autonomic Nervous System: Scientific Implication and Practical Implementation. In Chronobiology—The Science of Biological Time Structure; Pavol, S., Ed.; IntechOpen: London, UK, 2019. [Google Scholar]
- Ntougou Assoumou, H.G.; Pichot, V.; Barthelemy, J.C.; Dauphinot, V.; Celle, S.; Gosse, P.; Kossovsky, M.; Gaspoz, J.M.; Roche, F. Metabolic Syndrome and Short-Term and Long-Term Heart Rate Variability in Elderly Free of Clinical Cardiovascular Disease: The PROOF Study. Rejuvenation Res. 2010, 13, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Binici, Z.; Mouridsen, M.R.; Køber, L.; Sajadieh, A. Decreased Nighttime Heart Rate Variability Is Associated with Increased Stroke Risk. Stroke 2011, 42, 3196–3201. [Google Scholar] [CrossRef] [Green Version]
- Siegrist, J.; Li, J. Work Stress and Altered Biomarkers: A Synthesis of Findings Based on the Effort-Reward Imbalance Model. Int. J. Environ. Res. Public Health 2017, 14, 1373. [Google Scholar] [CrossRef] [Green Version]
- Jarczok, M.N.; Jarczok, M.; Mauss, D.; Koenig, J.; Li, J.; Herr, R.M.; Thayer, J.F. Autonomic Nervous System Activity and Workplace Stressors—A Systematic Review. Neurosci. Biobehav. Rev. 2013, 37, 1810–1823. [Google Scholar] [CrossRef]
- Jarczok, M.N.; Jarczok, M.; Thayer, J.F. Work Stress and Autonomic Nervous System Activity. In Handbook of Socioeconomic Determinants of Occupational Health—From Macro-Level to Micro-Level Evidence; Töres, T., Ed.; Springer International Publishing: Basel, Switzerland, 2020; p. 690. [Google Scholar]
- Theorell, T. (Ed.) Handbook of Socioeconomic Determinants of Occupational Health; Handbook Series in Occupational Health Sciences; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar]
- Kröll, C.; Doebler, P.; Nüesch, S. Meta-Analytic Evidence of the Effectiveness of Stress Management at Work. Eur. J. Work Organ. Psychol. 2017, 26, 677–693. [Google Scholar] [CrossRef]
- Holman, D.; Johnson, S.; O’Connor, E. Stress Management Interventions: Improving Subjective Psychological Well-Being in the Workplace Stress Management Interventions: A Typology and Description. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, USA, 2018; pp. 1–14. [Google Scholar]
- Bishop, G.D.; Kaur, D.; Tan, V.L.M.; Chua, Y.-L.; Liew, S.-M.; Mak, K.-H. Effects of a Psychosocial Skills Training Workshop on Psychophysiological and Psychosocial Risk in Patients Undergoing Coronary Artery Bypass Grafting. Am. Heart J. 2005, 150, 602–609. [Google Scholar] [CrossRef]
- Jarczok, M.N.; Kleber, M.E.; Koenig, J.; Loerbroks, A.; Herr, R.M.; Hoffmann, K.; Fischer, J.E.; Benyamini, Y.; Thayer, J.F. Investigating the Associations of Self-Rated Health: Heart Rate Variability Is More Strongly Associated than Inflammatory and Other Frequently Used Biomarkers in a Cross Sectional Occupational Sample. PLoS ONE 2015, 10, e0117196. [Google Scholar] [CrossRef]
- Oyeleye, M.; Chen, T.; Titarenko, S.; Antoniou, G. A Predictive Analysis of Heart Rates Using Machine Learning Techniques. Int. J. Environ. Res. Public Health 2022, 19, 2417. [Google Scholar] [CrossRef]
- Staffini, A.; Svensson, T.; Chung, U.I.; Svensson, A.K. Heart Rate Modeling and Prediction Using Autoregressive Models and Deep Learning. Sensors 2021, 22, 34. [Google Scholar] [CrossRef] [PubMed]
- Massaro, A.; Maritati, V.; Savino, N.; Galiano, A. Neural Networks for Automated Smart Health Platforms Oriented on Heart Predictive Diagnostic Big Data Systems. In Proceedings of the 2018 AEIT International Annual Conference, Bari, Italy, 3–5 October 2018. [Google Scholar]
- Massaro, A.; Ricci, G.; Selicato, S.; Raminelli, S.; Galiano, A. Decisional Support System with Artificial Intelligence Oriented on Health Prediction Using a Wearable Device and Big Data. In Proceedings of the 2020 IEEE International Workshop on Metrology for Industry 4.0 & IoT, Roma, Italy, 3–5 June 2020; pp. 718–723. [Google Scholar]
- Ni, A.; Azarang, A.; Kehtarnavaz, N. A Review of Deep Learning-Based Contactless Heart Rate Measurement Methods. Sensors 2021, 21, 3719. [Google Scholar] [CrossRef]
- Cheng, C.H.; Wong, K.L.; Chin, J.W.; Chan, T.T.; So, R.H.Y. Deep Learning Methods for Remote Heart Rate Measurement: A Review and Future Research Agenda. Sensors 2021, 21, 6296. [Google Scholar] [CrossRef] [PubMed]
- Bonsaksen, T.; Thørrisen, M.M.; Skogen, J.C.; Aas, R.W. Who Reported Having a High-Strain Job, Low-Strain Job, Active Job and Passive Job? The WIRUS Screening Study. PLoS ONE 2019, 14, e0227336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hambrick, D.C.; Finkelstein, S.; Mooney, A.C. Executive Job Demands: New Insights for Explaining Strategic Decisions and Leader Behaviors. Acad. Manag. Rev. 2005, 30, 472–491. [Google Scholar] [CrossRef] [Green Version]
- Limm, H.; Gündel, H.; Heinmüller, M.; Marten-Mittag, B.; Nater, U.M.; Siegrist, J.; Angerer, P. Stress Management Interventions in the Workplace Improve Stress Reactivity: A Randomised Controlled Trial. Occup. Environ. Med. 2010, 68, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Wetzel, C.M.; George, A.; Hanna, G.B.; Athanasiou, T.; Black, S.A.; Kneebone, R.L.; Nestel, D.; Woloshynowych, M. Stress Management Training for Surgeons-a Randomized, Controlled, Intervention Study. Ann. Surg. 2011, 253, 488–494. [Google Scholar] [CrossRef]
- Herrmann-Lingen, C.; Buss, U.; Snaith, R. Hospital Anxiety and Depression Scale—Deutsche Version (HADS-D); Hogrefe, Ed.; 3. aktualisierte und neu normierte Auflage; Verlag Hans Huber: Bern, Switzerland, 2011. [Google Scholar]
- Rödel, A.; Siegrist, J.; Hessel, A.; Brähler, E. Fragebogen Zur Messung Beruflicher Gratifikationskrisen. Z. Differ. Diagn. Psychol. 2004, 25, 227–238. [Google Scholar] [CrossRef]
- Koenig, J.; Thayer, J.F. Sex Differences in Healthy Human Heart Rate Variability: A Meta-Analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef]
- Camm, A.; Malik, M.; Bigger, J.; Breithardt, G.; Cerutti, S.; Cohen, R.; Coumel, P.; Fallen, E.; Kennedy, H.; Kleiger, R.; et al. Heart Rate Variability. Standards of Measurement, Physiological Interpretation, and Clinical Use. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Roach, D.; Wilson, W.; Ritchie, D.; Sheldon, R. Dissection of Long-Range Heart Rate Variability. J. Am. Coll. Cardiol. 2004, 43, 2271–2277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Sen, A.; ó’Hartaigh, B.; Janszky, I.; Romundstad, P.R.; Tonstad, S.; Vatten, L.J. Resting Heart Rate and the Risk of Cardiovascular Disease, Total Cancer, and All-Cause Mortality—A Systematic Review and Dose–Response Meta-Analysis of Prospective Studies. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 504–517. [Google Scholar] [CrossRef] [PubMed]
- Sui, X.; Laditka, J.N.; Hardin, J.W.; Blair, S.N. Estimated Functional Capacity Predicts Mortality in Older Adults. J. Am. Geriatr. Soc. 2007, 55, 1940–1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palatini, P.; Reboldi, G.; Beilin, L.J.; Eguchi, K.; Imai, Y.; Kario, K.; Ohkubo, T.; Pierdomenico, S.D.; Saladini, F.; Schwartz, J.E.; et al. Predictive Value of Night-Time Heart Rate for Cardiovascular Events in Hypertension. The ABP-International Study. Int. J. Cardiol. 2013, 168, 1490–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cauter, E.; Spiegel, K.; Tasali, E.; Leproult, R. Metabolic Consequences of Sleep and Sleep Loss. Sleep Med. 2008, 9, S23–S28. [Google Scholar] [CrossRef] [Green Version]
- Willert, M.V.; Thulstrup, A.M.; Hertz, J.; Bonde, J.P. Sleep and Cognitive Failures Improved by a Three-Month Stress Management Intervention. Int. J. Stress Manag. 2010, 17, 193–213. [Google Scholar] [CrossRef]
- Vargas, S.; Antoni, M.H.; Carver, C.S.; Lechner, S.C.; Wohlgemuth, W.; Llabre, M.; Blomberg, B.B.; Glück, S.; Derhagopian, R.P.; Vargas, S.; et al. Sleep Quality and Fatigue after a Stress Management Intervention for Women with Early-Stage Breast Cancer in Southern Florida. Int. J. Behav. Med. 2014, 21, 971–981. [Google Scholar] [CrossRef] [Green Version]
- Nolan, R.P.; Jong, P.; Barry-Bianchi, S.M.; Tanaka, T.H.; Floras, J.S. Effects of Drug, Biobehavioral and Exercise Therapies on Heart Rate Variability in Coronary Artery Disease: A Systematic Review. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 386–396. [Google Scholar] [CrossRef]
- Angelovski, A.; Sattel, H.; Henningsen, P.; Sack, M. Heart Rate Variability Predicts Therapy Outcome in Pain-Predominant Multisomatoform Disorder. J. Psychosom. Res. 2016, 83, 16–21. [Google Scholar] [CrossRef]
- Hayano, J.; Furukawa, Y.; Yuda, E.; Yoshida, Y. Association of 24-Hour Heart Rate Variability and Daytime Physical Activity: ALLSTAR Big Data Analysis. Int. J. Biosci. Biochem. Bioinform. 2018, 8, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Young, H.A.; Benton, D. Heart-Rate Variability: A Biomarker to Study the Influence of Nutrition on Physiological and Psychological Health? Behav. Pharmacol. 2018, 29, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, Y.T.; Steffen, P.R. Adding HRV Biofeedback to Psychotherapy Increases Heart Rate Variability and Improves the Treatment of Major Depressive Disorder. Int. J. Psychophysiol. 2018, 131, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The Measurement of Effort-Reward Imbalance at Work: European Comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Schienkiewitz, A.; Mensink, G.B.; Kuhnert, R.; Lange, C. Übergewicht Und Adipositas Bei Erwachsenen in Deutschland. J. Health Monit. 2017, 2, 21–28. [Google Scholar]
- Jahnsen, K.; Strube, H.; Starker, A. Hypertonie; Robert-Koch-Institut: Berlin, Germany, 2008. [Google Scholar]
- Jarczok, M.N.; Buckley, T.; Guendel, H.O.; Boeckelmann, I.; Mauss, D.; Thayer, J.F.; Balint, E.M. 24 H-Heart Rate Variability as a Communication Tool for a Personalized Psychosomatic Consultation in Occupational Health. Front. Neurosci. 2021, 15, 31. [Google Scholar] [CrossRef] [PubMed]
- Sammito, S.; Böckelmann, I. New Reference Values of Heart Rate Variability during Ordinary Daily Activity. Hear. Rhythm. 2017, 14, 304–307. [Google Scholar] [CrossRef]
- Mulfinger, N.; Sander, A.; Stuber, F.; Brinster, R.; Junne, F.; Limprecht, R.; Jarczok, M.N.; Seifried-Dübon, T.; Rieger, M.A.; Zipfel, S.; et al. Cluster-Randomised Trial Evaluating a Complex Intervention to Improve Mental Health and Well-Being of Employees Working in Hospital—A Protocol for the SEEGEN Trial. BMC Public Health 2019, 19, 1694. [Google Scholar] [CrossRef]
- LaMontagne, A.D.; Martin, A.; Page, K.M.; Reavley, N.J.; Noblet, A.J.; Milner, A.J.; Keegel, T.; Smith, P.M. Workplace Mental Health: Developing an Integrated Intervention Approach. BMC Psychiatry 2014, 14, 131. [Google Scholar] [CrossRef] [Green Version]
- Michaelis, M.; Balint, E.M.; Junne, F.; Zipfel, S.; Gündel, H.; Lange, R.; Rieger, M.A.; Rothermund, E. Who Should Play a Key Role in Preventing Common Mental Disorders That Affect Employees in the Workplace? Results of a Survey with Occupational Health Physicians, Primary Care Physicians, Psychotherapists, and Human Resource Managers. Int. J. Environ. Res. Public Health 2019, 16, 1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing Occupational Stress in Healthcare Workers. Cochrane Database Syst. Rev. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, J.A.M.; Schwarz, E.; Azad, Z.R.; Gritzka, S.; Diebig, M.; Gast, M.; Kilian, R.; Nater, U.; Jarczok, M.; Kessemeier, F.; et al. Effectiveness and Cost Effectiveness of a Stress Management Training for Leaders of Small and Medium Sized Enterprises—Study Protocol for a Randomized Controlled-Trial. BMC Public Health 2021, 21, 468. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention Group N = 87 | Control Group N = 87 | ||||||
|---|---|---|---|---|---|---|---|
| Variable | 25th Quartile (N) | Median (%) | 75th Quartile (N) | 25th Quartile (N) | Median (%) | 75th Quartile (N) | p-Value |
| Age (years) | 35 | 41 | 47 | 35 | 41 | 48 | 0.922 |
| Sex (female) | 1 | 1 | 2 | 2 | 1.000 | ||
| Smoker | 22 | 25 | 29 | 33 | 0.318 | ||
| BMI (kg/m2) | 25.3 | 27.8 | 30.7 | 25.3 | 27.5 | 29.5 | 0.217 |
| Resting systolic blood pressure (mmHg) | 124 | 134 | 141 | 125 | 133 | 142 | 0.945 |
| Resting diastolic blood pressure (mmHg) | 81 | 90 | 94 | 82 | 88 | 94 | 0.789 |
| Resting heart rate (bpm) | 70.2 | 75.1 | 82.2 | 70.9 | 77.1 | 82.5 | 0.823 |
| Weekly working hours: | 0.743 | ||||||
| <40 | 17 | 20 | 20 | 23 | |||
| 41–45 | 44 | 51 | 40 | 46 | |||
| 46–50 | 21 | 24 | 19 | 22 | |||
| >50 | 5 | 6 | 8 | 9 | |||
| Sick leave during the last 12 months: More than 10 days | 11 | 13 | 11 | 13 | 1.000 | ||
| HADS anxious symptoms | 4 | 5 | 8 | 3 | 6 | 9 | 0.614 |
| HADS depressive symptoms | 2 | 4 | 7 | 2 | 4 | 6 | 0.189 |
| ERI effort | 14 | 16 | 19 | 14 | 16 | 18 | 0.757 |
| ERI reward | 38 | 43 | 49 | 43 | 47 | 51 | 0.003 |
| Parameter | Group | Baseline | Follow-Up | Baseline | Follow-Up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Night | Night | 24 h | 24 h | ||||||||||
| N | Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | ||
| SDANN | CG | 70 | 61.4 | 32.1 | 47 | 56.8 | 23.4 | 70 | 126.0 | 36.8 | 54 | 122.0 | 31.7 |
| SDANN | IG | 77 | 53.5 | 25.6 | 52 | 62.5 | 29.4 | 78 | 131.0 | 34.5 | 62 | 125.0 | 35.5 |
| SDNN | CG | 70 | 102.0 | 34.4 | 47 | 101.0 | 33.2 | 70 | 142.0 | 34.3 | 54 | 143.0 | 35.0 |
| SDNN | IG | 77 | 99.4 | 29.7 | 52 | 107.0 | 30.8 | 78 | 150.0 | 36.4 | 62 | 145.0 | 35.3 |
| RMSSD | CG | 70 | 36.4 | 16.5 | 47 | 36.9 | 15.8 | 70 | 26.9 | 9.4 | 54 | 28.1 | 10.1 |
| RMSSD | IG | 77 | 38.4 | 17.2 | 52 | 39.9 | 17.9 | 78 | 29.0 | 10.4 | 62 | 29.7 | 11.5 |
| HR | CG | 70 | 64.5 | 8.5 | 47 | 63.4 | 10.1 | 70 | 77.5 | 8.5 | 54 | 75.9 | 9.7 |
| HR | IG | 77 | 63.0 | 8,2 | 52 | 62.2 | 7.2 | 78 | 76.4 | 8.8 | 62 | 76.0 | 9.2 |
| Dependent Variables | Group ×Time | Group | Time | |||||
|---|---|---|---|---|---|---|---|---|
| N | z | p-Value | z | p-Value | z | p-Value | ||
| SDANN | Nighttime | 149 | 2.04 | 0.041 * | −1.86 | 0.063 | −0.75 | 0.455 |
| SDANN | 24 h | 150 | −0.13 | 0.898 | 0.88 | 0.378 | −1.38 | 0.166 |
| SDNN | Nighttime | 149 | 1.23 | 0.218 | −0.49 | 0.623 | −0.38 | 0.701 |
| SDNN | 24 h | 150 | −0.48 | 0.631 | 1.37 | 0.170 | −0.83 | 0.405 |
| RMSSD | Nighttime | 149 | 0.22 | 0.825 | 0.98 | 0.329 | −0.38 | 0.703 |
| RMSSD | 24 h | 150 | −0.53 | 0.594 | 1.41 | 0.157 | 0.69 | 0.487 |
| HR | Nighttime | 149 | −0.25 | 0.799 | 1.13 | 0.259 | 0.26 | 0.796 |
| HR | 24 h | 150 | 0.83 | 0.409 | −0.75 | 0.453 | −0.82 | 0.412 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balint, E.M.; Angerer, P.; Guendel, H.; Marten-Mittag, B.; Jarczok, M.N. Stress Management Intervention for Leaders Increases Nighttime SDANN: Results from a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 3841. https://doi.org/10.3390/ijerph19073841
Balint EM, Angerer P, Guendel H, Marten-Mittag B, Jarczok MN. Stress Management Intervention for Leaders Increases Nighttime SDANN: Results from a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(7):3841. https://doi.org/10.3390/ijerph19073841
Chicago/Turabian StyleBalint, Elisabeth Maria, Peter Angerer, Harald Guendel, Birgitt Marten-Mittag, and Marc N. Jarczok. 2022. "Stress Management Intervention for Leaders Increases Nighttime SDANN: Results from a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 7: 3841. https://doi.org/10.3390/ijerph19073841
APA StyleBalint, E. M., Angerer, P., Guendel, H., Marten-Mittag, B., & Jarczok, M. N. (2022). Stress Management Intervention for Leaders Increases Nighttime SDANN: Results from a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(7), 3841. https://doi.org/10.3390/ijerph19073841