
Sustainability of Hiking in Combination with Coaching in Cardiorespiratory Fitness and Quality of Life


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
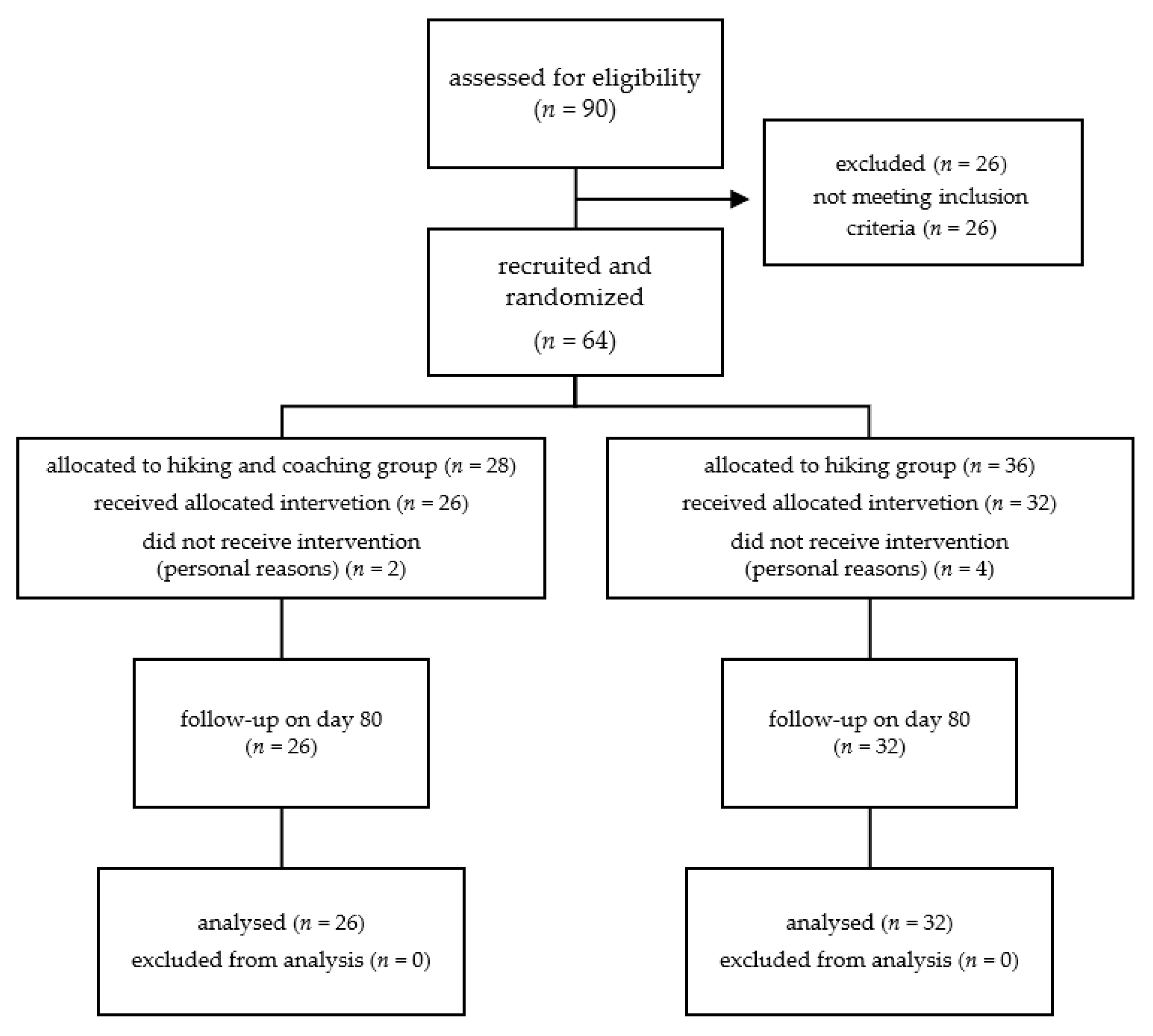
2.1. Study Design and Settings
2.2. Participants
2.3. Intervention
2.4. Data Collection and Outcomes
2.4.1. One-Mile Walking Test
2.4.2. Questionnaires for Health-Related Quality of Life
2.4.3. Spirometry
2.4.4. Coaching
2.4.5. Randomization and Sample Size
2.4.6. Statistical Analysis
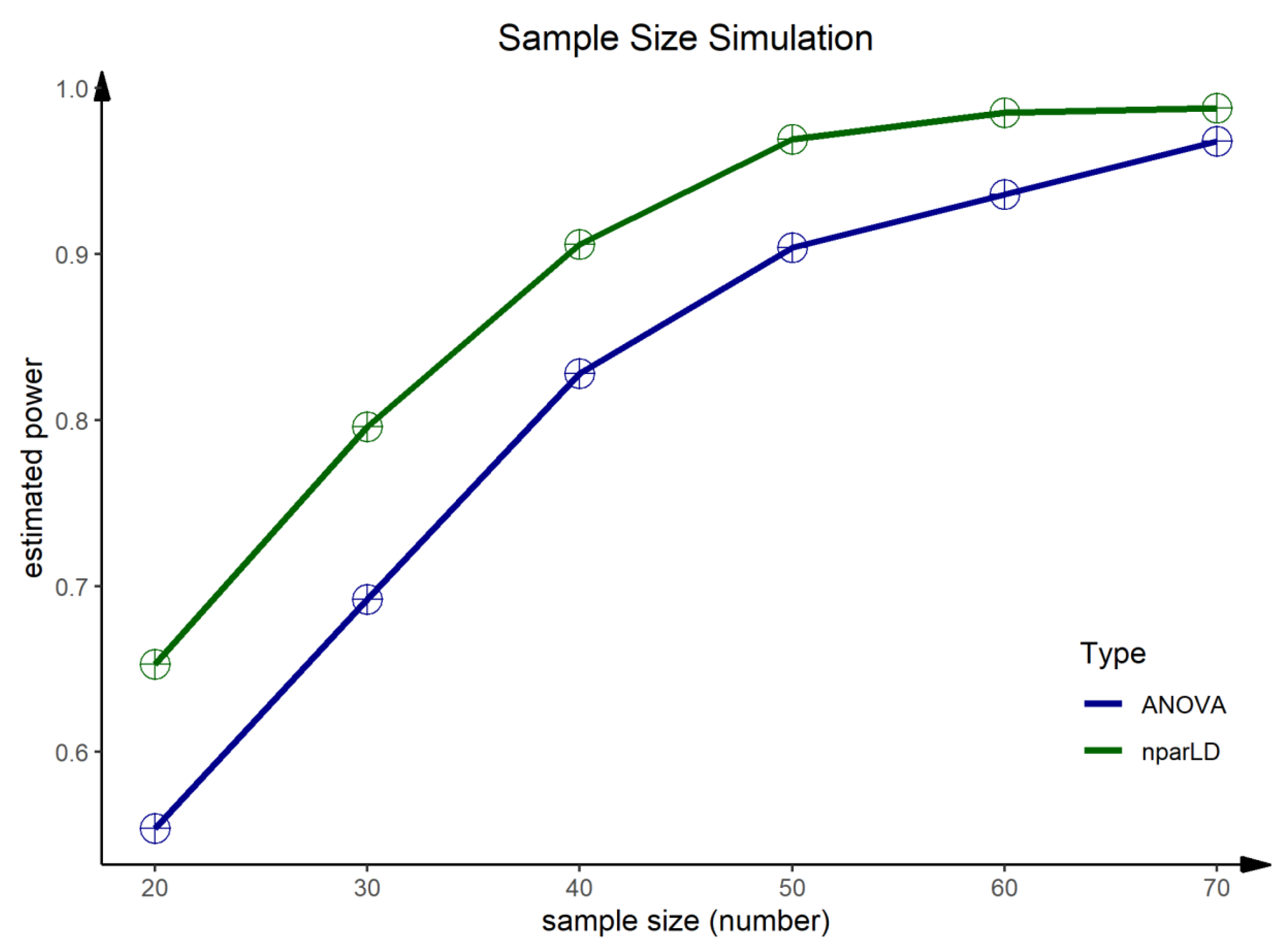
2.4.7. Sample Size Simulation
3. Results
3.1. Study Participants and Baseline Characteristics
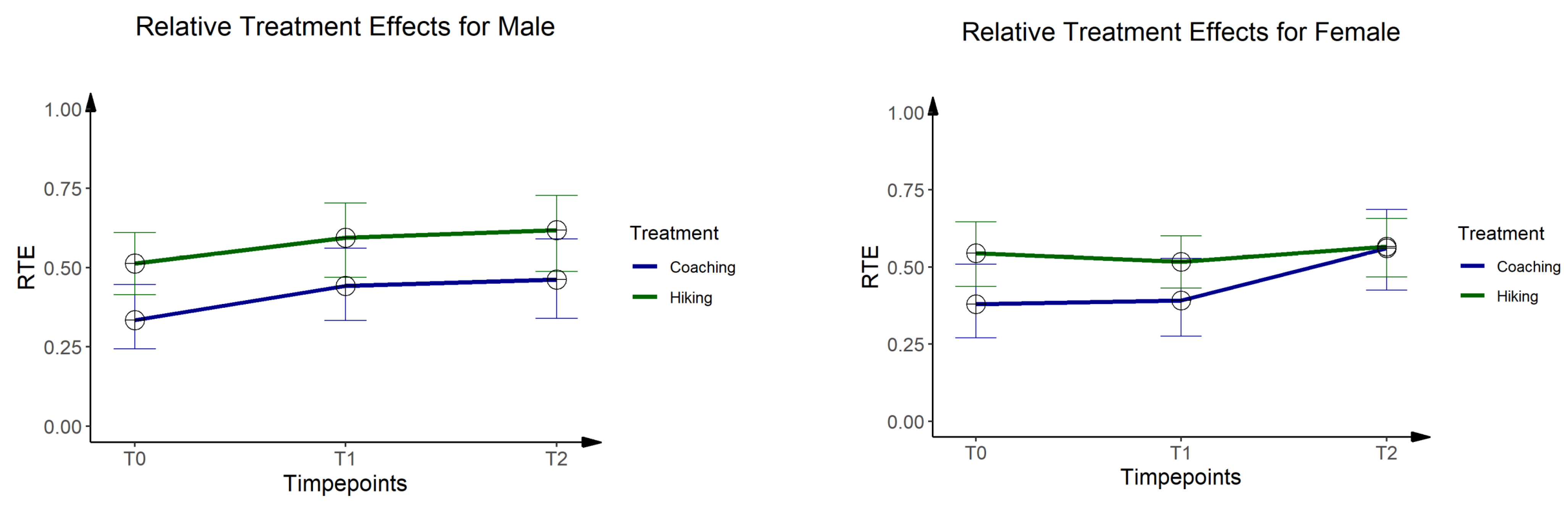
3.2. One-Mile Walking Test
3.3. EQ-5D-5L
3.4. SF-36
3.5. Spirometry
3.6. Sample Size Simulation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| ATS/ERS | American thoracic society/ European respiratory society |
| EQ-5D-5L | EuroQol health survey with 5 dimensions and 5 levels |
| FEV1 | Forced expiration volume in 1 s |
| FVC | Forced expiration volume |
| GE | Green exercise |
| HICO | Hiking and coaching |
| HR | Heart rate |
| ID | Identifier |
| IQR | Interquartile range |
| km | Kilometers |
| LOCF | Last outcome/observation carried forward |
| MET | Metabolic equivalent |
| NCDs | Non-communicable diseases |
| NOCB | Next outcome/observation carried backward |
| nparLD | Nonparametric longitudinal data analysis |
| PEF | Peak expiratory flow |
| RTE | Relative treatment effects |
| SD | Standard deviation |
| SF-36 | Short form health survey with 36 items |
| T0 | time of measurement/day 0 |
| T1 | time of measurement/day 7 |
| T2 | time of measurement/day 80 |
| VAS | Visual analogue scale |
| V(O2)max | Maximal oxygen consumption or aerobic capacity |
| WT | Weight in pounds |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hiking Group (n = 32) | Coaching Group (n = 26) | |||
|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | |
| Weight (kg) | 76.69 ± 15.64 | 75.85 ± 15.45 | 76.86 ± 16.04 | 71.70 ± 11.60 |
| BMI | 24.89 ± 4.24 | 24.64 ± 4.87 | 25.46 ± 4.06 | 24.98 ± 3.57 |
| FEV1 (%) | 103.07 ± 12.9 | 101.11 ± 18.25 | 101.72 ± 12.44 | 102.62 ± 17.50 |
| FVC (%) | 108.90 ± 13.24 | 109.50 ± 13.83 | 107.82 ± 12.90 | 107.71 ± 14.80 |
| PEF (%) | 100.92 ± 19.91 | 103.43 ± 27.39 | 109.51 ± 18.49 | 112.86 ± 25.15 |
| 48.29 ± 7.54 | 47.94 ± 8.98 | 45.62 ± 5.65 | 46.54 ± 8.95 | |
| (male) | 52.27 ± 7.04 | 52.04 ± 6.74 | 48.32 ± 5.81 | 48.68 ± 6.09 |
| (female) | 44.78 ± 6.24 | 45.55 ± 5.77 | 42.92 ± 4.10 | 42.46 ± 7.15 |
| EQ-5D-5L | ||||
| -VAS | 86.88 ± 9.31 | 90.00 ± 10.00 | 87.31 ± 7.78 | 90.00 ± 10.00 |
| -Score Index | 0.98 ± 0.04 | 1.00 ± 0.00 | 0.97 ± 0.04 | 1.00 ± 0.09 |
| SF-36 | ||||
| -Physical Functioning | 97.66 ± 5.53 | 100.00 ± 5.00 | 96.73 ± 3.73 | 97.50 ± 5.00 |
| -Role—Physical | 93.75 ± 16.80 | 100.00 ± 0.00 | 95.19 ± 14.18 | 100.00 ± 0.00 |
| -Bodily Pain | 83.78 ± 20.16 | 84.00 ± 26.00 | 81.12 ± 17.30 | 84.00 ± 26.00 |
| -General Health | 85.19 ± 12.39 | 84.50 ± 20.00 | 81.58 ± 10.47 | 82.00 ± 9.50 |
| -Vitality | 67.34 ± 15.40 | 67.50 ± 25.00 | 64.81 ± 12.53 | 65.00 ± 10.00 |
| -Social Functioning | 90.23 ± 14.10 | 100.00 ± 25.00 | 88.94 ± 16.33 | 100.00 ± 12.50 |
| -Role-Emotional | 94.79 ± 14.93 | 100.00 ± 0.00 | 93.59 ± 18.90 | 100.00 ± 0.00 |
| -Mental Health | 77.25 ± 12.50 | 78.00 ± 17.00 | 78.15 ± 11.82 | 80.00 ± 16.00 |
| -Physical Dimension | 85.54 ± 9.37 | 86.70 ± 9.15 | 83.88 ± 7.97 | 84.20 ± 8.35 |
| -Mental Dimension | 82.96 ± 8.44 | 84.30 ± 10.32 | 81.41 ± 11.16 | 84.25 ± 9.83 |
| -Total Score | 86.25 ± 7.77 | 86.73 ± 7.70 | 85.01 ± 8.81 | 86.56 ± 9.62 |
| Hiking Group (n = 32) | Coaching Group (n = 26) | |||
|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | |
| Weight (kg) | 76.36 ± 15.90 | 73.95 ± 16.05 | 75.82 ± 15.43 | 70.65 ± 12.40 |
| BMI | 24.79 ± 4.37 | 24.44 ± 5.13 | 25.12 ± 3.91 | 24.98 ± 3.15 |
| FEV1 (%) | 103.50 ± 12.77 | 101.58 ± 17.14 | 102.03 ± 11.45 | 103.93 ± 9.86 |
| FVC (%) | 109.22 ± 13.86 | 109.84 ± 14.36 | 109.54 ± 12.49 | 109.37 ± 15.01 |
| PEF (%) | 100.83 ± 16.40 | 97.57 ± 22.26 | 105.36 ± 14.32 | 106.44 ± 21.59 |
| 48.87 ± 7.75 | 49.47 ± 9.33 | 48.06 ± 7.56 | 47.03 ± 7.31 | |
| (male) | 51.85 ± 7.26 | 52.92 ± 8.22 | 50.31 ± 9.08 | 49.52 ± 5.70 |
| (female) | 46.24 ± 7.39 | 45.21 ± 8.85 | 45.81 ± 5.06 | 45.83 ± 7.55 |
| EQ-5D-5L | ||||
| -VAS | 83.12 ± 12.30 | 80.00 ± 10.00 | 82.69 ± 10.79 | 80.00 ± 10.00 |
| -Score Index | 0.98 ± 0.04 | 1.00 ± 0.00 | 0.98 ± 0.04 | 1.00 ± 0.07 |
| SF-36 | ||||
| -Physical Functioning | 98.44 ± 4.66 | 100.00 ± 0.00 | 96.92 ± 4.26 | 100.00 ± 5.00 |
| -Role—Physical | 96.88 ± 17.68 | 100.00 ± 0.00 | 95.19 ± 12.29 | 100.00 ± 0.00 |
| -Bodily Pain | 86.50 ± 18.35 | 100.00 ± 26.00 | 79.12 ± 20.36 | 84.00 ± 35.00 |
| -General Health | 84.44 ± 11.16 | 87.00 ± 15.75 | 81.38 ± 12.02 | 82.00 ± 16.00 |
| -Vitality | 65.47 ± 19.97 | 67.50 ± 36.25 | 66.15 ± 16.14 | 70.00 ± 15.00 |
| -Social Functioning | 88.28 ± 19.03 | 100.00 ± 12.50 | 88.94 ± 19.47 | 100.00 ± 12.50 |
| -Role-Emotional | 100.00 ± 0.00 | 100.00 ± 0.00 | 96.15 ± 10.86 | 100.00 ± 0.00 |
| -Mental Health | 77.38 ± 18.36 | 80.00 ± 14.00 | 78.77 ± 12.12 | 84.00 ± 13.00 |
| -Physical Dimension | 86.34 ± 9.32 | 86.90 ± 10.25 | 83.75 ± 9.42 | 86.50 ± 12.00 |
| -Mental Dimension | 83.11 ± 10.12 | 84.65 ± 10.45 | 82.28 ± 10.92 | 86.20 ± 11.20 |
| -Total Score | 87.17 ± 7.73 | 87.16 ± 8.95 | 85.33 ± 9.45 | 88.94 ± 12.83 |
| Number | Estimated Power | |
|---|---|---|
| ANOVA | F1-LD-F1 | |
| 20 | 0.55 | 0.65 |
| 30 | 0.69 | 0.80 |
| 40 | 0.83 | 0.91 |
| 50 | 0.90 | 0.97 |
| 60 | 0.94 | 0.99 |
| 70 | 0.97 | 0.99 |
References
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of Physical Inactivity on Major Non-Communicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Saunders, T.J.; McIsaac, T.; Douillette, K.; Gaulton, N.; Hunter, S.; Rhodes, R.E.; Prince, S.A.; Carson, V.; Chaput, J.-P.; Chastin, S.; et al. Sedentary Behaviour and Health in Adults: An Overview of Systematic Reviews. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2020, 45, S197–S217. [Google Scholar] [CrossRef] [PubMed]
- Sedentary Behaviour Research Network. Letter to the Editor: Standardized Use of the Terms “Sedentary” and “Sedentary Behaviours”. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.P.; Hewson, D.J.; Champion, R.B.; Sayegh, S.M. Sitting Time and Risk of Cardiovascular Disease and Diabetes: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2019, 57, 408–416. [Google Scholar] [CrossRef]
- Beunza, J.J.; Martínez-González, M.Á.; Ebrahim, S.; Bes-Rastrollo, M.; Núñez, J.; Martínez, J.A.; Alonso, Á. Sedentary Behaviors and the Risk of Incident Hypertension: The SUN Cohort. Am. J. Hypertens. 2007, 20, 1156–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [Green Version]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical Activity, Obesity and Sedentary Behavior in Cancer Etiology: Epidemiologic Evidence and Biologic Mechanisms. Mol. Oncol. 2021, 15, 790–800. [Google Scholar] [CrossRef]
- Healy, G.N.; Wijndaele, K.; Dunstan, D.W.; Shaw, J.E.; Salmon, J.; Zimmet, P.Z.; Owen, N. Objectively Measured Sedentary Time, Physical Activity, and Metabolic Risk: The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care 2008, 31, 369–371. [Google Scholar] [CrossRef] [Green Version]
- Ohlsson, C.; Gidestrand, E.; Bellman, J.; Larsson, C.; Palsdottir, V.; Hägg, D.; Jansson, P.-A.; Jansson, J.-O. Increased Weight Loading Reduces Body Weight and Body Fat in Obese Subjects—A Proof of Concept Randomized Clinical Trial. EClinicalMedicine 2020, 22, 100338. [Google Scholar] [CrossRef]
- Chastin, S.F.M.; Mandrichenko, O.; Helbostadt, J.L.; Skelton, D.A. Associations between Objectively-Measured Sedentary Behaviour and Physical Activity with Bone Mineral Density in Adults and Older Adults, the NHANES Study. Bone 2014, 64, 254–262. [Google Scholar] [CrossRef]
- Lee, S.-H.; Son, C.; Yeo, S.; Ha, I.-H. Cross-Sectional Analysis of Self-Reported Sedentary Behaviors and Chronic Knee Pain among South Korean Adults over 50 Years of Age in KNHANES 2013-2015. BMC Public Health 2019, 19, 1375. [Google Scholar] [CrossRef]
- Henson, J.; Yates, T.; Edwardson, C.L.; Khunti, K.; Talbot, D.; Gray, L.J.; Leigh, T.M.; Carter, P.; Davies, M.J. Sedentary Time and Markers of Chronic Low-Grade Inflammation in a High Risk Population. PLoS ONE 2013, 8, e78350. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. The Economic Burden of Physical Inactivity: A Global Analysis of Major Non-Communicable Diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Martins, L.C.G.; de Oliveira Lopes, M.V.; Diniz, C.M.; Guedes, N.G. The Factors Related to a Sedentary Lifestyle: A Meta-analysis Review. J. Adv. Nurs. 2021, 77, 1188–1205. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide Trends in Insufficient Physical Activity from 2001 to 2016: A Pooled Analysis of 358 Population-Based Surveys with 1·9 Million Participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting Time, Physical Activity, and Risk of Mortality in Adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Da Luz Scheffer, D.; Latini, A. Exercise-Induced Immune System Response: Anti-Inflammatory Status on Peripheral and Central Organs. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165823. [Google Scholar] [CrossRef] [PubMed]
- Turner, W.R.; Nakamura, T.; Dinetti, M. Global Urbanization and the Separation of Humans from Nature. BioScience 2004, 54, 585–590. [Google Scholar] [CrossRef] [Green Version]
- Flowers, E.P. A Cross-Sectional Study Examining Predictors of Visit Frequency to Local Green Space and the Impact This Has on Physical Activity Levels. BMC Public Health 2016, 16, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Keniger, L.E.; Gaston, K.J.; Irvine, K.N.; Fuller, R.A. What Are the Benefits of Interacting with Nature? Int. J. Environ. Res. Public Health 2013, 10, 913–935. [Google Scholar] [CrossRef] [Green Version]
- Thomsen, J.M.; Powell, R.B.; Monz, C. A Systematic Review of the Physical and Mental Health Benefits of Wildland Recreation. J. Park Recreat. Adm. 2018, 36, 123–148. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring Pathways Linking Greenspace to Health: Theoretical and Methodological Guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Elliott, L.R.; Gascon, M.; Roberts, B.; Fleming, L.E. Blue Space, Health and Well-Being: A Narrative Overview and Synthesis of Potential Benefits. Environ. Res. 2020, 191, 110169. [Google Scholar] [CrossRef] [PubMed]
- Holt, E.W.; Lombard, Q.K.; Best, N.; Smiley-Smith, S.; Quinn, J.E. Active and Passive Use of Green Space, Health, and Well-Being amongst University Students. Int. J. Environ. Res. Public Health 2019, 3, 424. [Google Scholar] [CrossRef] [Green Version]
- Gidlow, C.J.; Jones, M.V.; Hurst, G.; Masterson, D.; Clark-Carter, D.; Tarvainen, M.P.; Smith, G.; Nieuwenhuijsen, M. Where to Put Your Best Foot Forward: Psycho-Physiological Responses to Walking in Natural and Urban Environments. J. Environ. Psychol. 2016, 45, 22–29. [Google Scholar] [CrossRef]
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The Mental and Physical Health Outcomes of Green Exercise. Int. J. Environ. Health 2005, 15, 319–337. [Google Scholar] [CrossRef]
- Niedermeier, M.; Einwanger, J.; Hartl, A.; Kopp, M. Affective Responses in Mountain Hiking—A Randomized Crossover Trial Focusing on Differences between Indoor and Outdoor Activity. PLoS ONE 2017, 12, e0177719. [Google Scholar] [CrossRef]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The Effects of Green Exercise on Physical and Mental Wellbeing: A Systematic Review. Int. J. Environ. Res. Public. Health 2019, 16, 1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burtscher, M. Endurance Performance of the Elderly Mountaineer: Requirements, Limitations, Testing, and Training. Wien. Klin. Wochenschr. 2004, 116, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Faulhaber, M.; Pocecco, E.; Niedermeier, M.; Ruedl, G.; Walter, D.; Sterr, R.; Ebner, H.; Schobersberger, W.; Burtscher, M. Fall-Related Accidents among Hikers in the Austrian Alps: A 9-Year Retrospective Study. BMJ Open Sport Exerc. Med. 2017, 3, e000304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richins, H.; Hull, J.S. Mountain Tourism: Experiences, Communities, Environments and Sustainable Futures; CABI: Wallingford, UK, 2016. [Google Scholar]
- Kercher, V.M.; Kercher, K.; Bennion, T.; Yates, B.A.; Feito, Y.; Alexander, C.; Amaral, P.C.; Soares, W.; Li, Y.-M.; Han, J.; et al. Fitness Trends From Around the Globe. ACSMS Health Fit. J. 2021, 25, 20–31. [Google Scholar] [CrossRef]
- Batrakoulis, A. European Survey of Fitness Trends for 2020. ACSM Health Fit. J. 2019, 23, 28–35. [Google Scholar] [CrossRef]
- Palmer, S.; Tubbs, I.; Whybrow, A. Health Coaching to Facilitate the Promotion of Healthy Behaviour and Achievement of Health-Related Goals. Int. J. Health Promot. Educ. 2003, 41, 91–93. [Google Scholar] [CrossRef]
- Wolever, R.Q.; Simmons, L.A.; Sforzo, G.A.; Dill, D.; Kaye, M.; Bechard, E.M.; Southard, M.E.; Kennedy, M.; Vosloo, J.; Yang, N. A Systematic Review of the Literature on Health and Wellness Coaching: Defining a Key Behavioral Intervention in Healthcare. Glob. Adv. Health Med. 2013, 2, 38–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butterworth, S.W.; Linden, A.; McClay, W. Health Coaching as an Intervention in Health Management Programs. Dis. Manag. Health Outcomes 2007, 15, 299–307. [Google Scholar] [CrossRef]
- Greif, S. Mehrebenen-Coaching von Individuen, Gruppen und Organisationen. In Eine umfassende und genaue Definition von Coaching als Förderung der Selbstreflexion; Universität Osnabrück: Osnabrück, Germany, 2005. [Google Scholar]
- Kivelä, K.; Elo, S.; Kyngäs, H.; Kääriäinen, M. The Effects of Health Coaching on Adult Patients with Chronic Diseases: A Systematic Review. Patient Educ. Couns. 2014, 97, 147–157. [Google Scholar] [CrossRef]
- Butterworth, S.; Linden, A.; McClay, W.; Leo, M.C. Effect of Motivational Interviewing-Based Health Coaching on Employees’ Physical and Mental Health Status. J. Occup. Health Psychol. 2006, 11, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Wolever, R.Q.; Dreusicke, M.; Fikkan, J.; Hawkins, T.V.; Yeung, S.; Wakefield, J.; Duda, L.; Flowers, P.; Cook, C.; Skinner, E. Integrative Health Coaching for Patients With Type 2 Diabetes. Diabetes Educ. 2010, 36, 629–639. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B.; For Physical Activity Guidelines Advisory Committee. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sports Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef]
- Saidj, M.; Menai, M.; Charreire, H.; Weber, C.; Enaux, C.; Aadahl, M.; Kesse-Guyot, E.; Hercberg, S.; Simon, C.; Oppert, J.-M. Descriptive Study of Sedentary Behaviours in 35,444 French Working Adults: Cross-Sectional Findings from the ACTI-Cités Study. BMC Public Health 2015, 1, 379–389. [Google Scholar] [CrossRef]
- Johansson, G.; Westerterp, K.R. Assessment of the Physical Activity Level with Two Questions: Validation with Doubly Labeled Water. Int. J. Obes. 2008, 32, 1031–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, G.M.; Porcari, J.P.; Hintermeister, R.; Freedson, P.S.; Ward, A.; McCarron, R.F.; Ross, J.; Rippe, J.M. Estimation of VO2max from a One-Mile Track Walk, Gender, Age, and Body Weight. Med. Sci. Sports Exerc. 1987, 19, 253–259. [Google Scholar] [CrossRef]
- Sparling, P.B. A Meta-Analysis of Studies Comparing Maximal Oxygen Uptake in Men and Women. Res. Q. Exerc. Sport 1980, 51, 542–552. [Google Scholar] [CrossRef]
- Kohrt, W.M.; Malley, M.T.; Coggan, A.R.; Spina, R.J.; Ogawa, T.; Ehsani, A.A.; Bourey, R.E.; Martin, W.H.; Holloszy, J.O. Effects of Gender, Age, and Fitness Level on Response of VO2max to Training in 60-71 Yr Olds. J. Appl. Physiol. 1991, 71, 2004–2011. [Google Scholar] [CrossRef]
- Ludwig, K.; Graf von der Schulenburg, J.-M.; Greiner, W. German Value Set for the EQ-5D-5L. PharmacoEconomics 2018, 36, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Stolk, E.; Ludwig, K.; Rand, K.; van Hout, B.; Ramos-Goñi, J.M. Overview, Update, and Lessons Learned From the International EQ-5D-5L Valuation Work: Version 2 of the EQ-5D-5L Valuation Protocol. Value Health 2019, 22, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullinger, M.; Kirchberger, I.; Ware, J. Der deutsche SF-36 Health Survey Übersetzung und psychometrische Testung eines krankheitsübergreifenden Instruments zur Erfassung der gesundheitsbezogenen Lebensqualität. J. Public Health 1995, 3, 21–36. [Google Scholar] [CrossRef]
- Miller, M.R. Standardisation of Spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Whitmore, J.; Gsänger, C.; Pyko, F.; Savelsberg, J.; Popp, M.; Whitmore, J. Coaching für die Praxis: Wesentliches für Jede Führungskraft; 2. Aufl. November 2009 der neu überarb. und erw. 3. Ausg.; Alles im Fluss-Verlag: Staufen im Breisgau, Germany, 2011. [Google Scholar]
- Hagemann, W.; Geuenich, K. Burnout-Screening-Skalen: BOSS, 2nd ed.; Hogrefe: Göttingen, Germany, 2009. [Google Scholar]
- Schulz, P.; Schlotz, W.; Becker, P. Trierer Inventar Zum Chronischen Stress TICS; Hogrefe: Göttingen, Germany, 2004. [Google Scholar]
- Erdmann, G.; Janke, W. Stressverarbeitungsfragebogen Mit SVF 120 Und SVF 78 (SVF), 3rd ed.; Hogrefe: Göttingen, Germany, 2004. [Google Scholar]
- Saghaei, M. Random Allocation Software for Parallel Group Randomized Trials. BMC Med. Res. Methodol. 2004, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. NparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Lunneborg, C.E. Bootstrap Applications for the Behavioral Sciences. Educ. Psychol. Meas. 1987, 47, 627–629. [Google Scholar] [CrossRef]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J. Fam. Med. 2020, 41, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Menz, V.; Marterer, N.; Amin, S.B.; Faulhaber, M.; Hansen, A.B.; Lawley, J.S. Functional Vs. Running Low-Volume High-Intensity Interval Training: Effects on VO2max and Muscular Endurance. J. Sports Sci. Med. 2019, 18, 497–504. [Google Scholar] [PubMed]
- Bumeder, I. Psychoonkologie: Diagnostik—Methoden—Therapieverfahren, 2nd ed.; Dorfmüller, M., Dietzfelbinger, H., Eds.; Urban & Fischer: München, Germany, 2013. [Google Scholar]
- Linnig, S.; Mache, S.; Strehler, V.; Ochsmann, E.; Preuß, G. Mitarbeiterzufriedenheit durch einen Gesundheitscoach und dessen Auswirkung auf körperliche Aktivität in einem Logistikunternehmen. Gesundheitswesen 2014, 76, A98. [Google Scholar] [CrossRef]
- Mannhardt, S.M.; de Haan, E.; Page, N. Greatest-Ever-Executive-Coaching-Outcome-Studie. In Coaching als Individuelle Antwort auf Gesellschaftliche Entwicklungen; Wegener, R., Deplazes, S., Hasenbein, M., Künzli, H., Ryter, A., Uebelhart, B., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2016; pp. 225–236. [Google Scholar]
- Wallace, A.M.; Bogard, M.T.; Zbikowski, S.M. Intrapersonal Variation in Goal Setting and Achievement in Health Coaching: Cross-Sectional Retrospective Analysis. J. Med. Internet Res. 2018, 20, e32. [Google Scholar] [CrossRef]
- Mason, A.E.; Epel, E.S.; Aschbacher, K.; Lustig, R.H.; Acree, M.; Kristeller, J.; Cohn, M.; Dallman, M.; Moran, P.J.; Bacchetti, P.; et al. Reduced Reward-Driven Eating Accounts for the Impact of a Mindfulness-Based Diet and Exercise Intervention on Weight Loss: Data from the SHINE Randomized Controlled Trial. Appetite 2016, 100, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Hiking Group (n = 32) | Coaching Group (n = 26) | Baseline Test | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | p-Value | Test | |
| Gender | male n = 15 | female n = 17 | male n = 13 | female n = 13 | 1.00 | χ² Test |
| Smoking status | smoker n = 5 | no-smoker n = 27 | smoker n = 7 | no-smoker n = 19 | 0.47 | χ² Test |
| Age (years) | 36.59 ± 8.53 | 34.5 ± 12.75 | 42.19 ± 6.04 | 42.50 ± 6.50 | 0.01 * | T-Test |
| Height (m) | 175.28 ± 9.07 | 173.5 ± 12.35 | 173.35 ± 9.01 | 172.00 ± 14.75 | 0.42 | T-Test |
| Weight (kg) | 75.92 ± 15.87 | 73.75 ± 15.63 | 76.31 ± 15.95 | 71.45 ± 11.85 | 0.84 | U-Test |
| BMI (kg/m²) | 24.63 ± 4.26 | 24.59 ± 5.09 | 25.28 ± 4.09 | 24.63 ± 3.64 | 0.54 | U-Test |
| FEV1 (%) | 105.09 ± 14.32 | 104.26 ± 14.44 | 103.46 ± 13.04 | 102.85 ± 12.3 | 0.65 | T-Test |
| FVC (%) | 109.97 ± 15.72 | 108.84 ± 13.2 | 109.00 ± 15.00 | 109.00 ± 11.00 | 0.77 | T-Test |
| PEF (%) | 101.17 ± 17.21 | 99.68 ± 20.73 | 110.84 ± 21.56 | 109.25 ± 30.28 | 0.07 | T-Test |
| VO2max (mL/min/kg) | 47.83 ± 7.97 | 49.12 ± 7.26 | 43.16 ± 7.20 | 43.34 ± 9.56 | 0.02 * | T-Test |
| Male: VO2max | 49.89 ± 6.35 | 50.79 ± 4.39 | 44.04 ± 8.94 | 48.78 ± 9.93 | 0.06 | T-Test |
| Female: VO2max | 46.01 ± 8.96 | 45.80 ± 10.71 | 42.29 ± 5.15 | 42.77 ± 4.37 | 0.16 | T-Test |
| Hiking Group (n = 32) | Coaching Group (n = 26) | Baseline Test | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | p-Value | Test | |
| EQ-5D-5L | ||||||
| -VAS | 83.44 ± 9.71 | 90.00 ± 10.00 | 80.38 ± 15.09 | 80.00 ± 20.00 | 0.55 | U-Test |
| -Score Index | 0.97 ± 0.05 | 1.00 ± 0.08 | 0.97 ± 0.04 | 1.00 ± 0.09 | 0.93 | U-Test |
| SF-36 | ||||||
| -Physical Functioning | 97.66 ± 4.21 | 100.00 ± 5.00 | 95.77 ± 4.17 | 95.00 ± 5.00 | 0.03 | U-Test |
| -Role—Physical | 92.97 ± 18.22 | 100.00 ± 0.00 | 97.12 ± 10.79 | 100.00 ± 0.00 | 0.35 | U-Test |
| -Bodily Pain | 86.38 ± 18.13 | 100.00 ± 18.50 | 73.69 ± 21.40 | 82.00 ± 22.00 | 0.01 * | U-Test |
| -General Health | 81.09 ± 11.92 | 79.50 ± 18.50 | 76.81 ± 11.09 | 77.00 ± 20.00 | 0.23 | U-Test |
| -Vitality | 62.66 ± 15.40 | 62.50 ± 21.25 | 64.23 ± 12.86 | 65.00 ± 10.00 | 0.67 | T-Test |
| -Social Functioning | 88.28 ± 14.53 | 100.00 ± 25.00 | 85.58 ± 22.83 | 100.00 ± 25.00 | 0.83 | U-Test |
| -Role-Emotional | 89.58 ± 19.74 | 100.00 ± 8.33 | 89.74 ± 24.53 | 100.00 ± 0.00 | 0.68 | U-Test |
| -Mental Health | 76.62 ± 14.59 | 80.00 ± 16.00 | 77.08 ± 10.34 | 78.00 ± 14.00 | 0.76 | U-Test |
| -Physical Dimension | 84.15 ± 8.95 | 84.90 ± 8.15 | 81.52 ± 8.76 | 83.70 ± 9.15 | 0.18 | U-Test |
| -Mental Dimension | 79.65 ± 11.27 | 81.52 ± 13.55 | 78.69 ± 13.04 | 82.50 ± 16.12 | 0.96 | U-Test |
| -Total Score | 84.40 ± 8.92 | 86.62 ± 8.21 | 82.50 ± 10.32 | 85.94 ± 15.53 | 0.58 | U-Test |
| Parameter | F1-LD-F1 Model | Relative Treatment Effects (RTE) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F (df) | p-Value | Time | Coaching | Hiking | ||||||
| 1-mile walking test | ||||||||||
| Coaching | 0.43 | Hiking | 0.55 | |||||||
| Treat | 3.10 (1.00, ∞) | 0.08 | n.s. | T0 | 0.45 | Co × T0 | 0.36 | Hi × T0 | 0.54 | |
| Time | 6.47 (1.93, ∞) | 0.00 | *** | T1 | 0.49 | Co × T1 | 0.43 | Hi × T1 | 0.54 | |
| Treat × Time | 2.58 (1.93, ∞) | 0.08 | n.s. | T2 | 0.54 | Co × T2 | 0.51 | Hi × T2 | 0.58 | |
male | Coaching | 0.41 | Hiking | 0.58 | ||||||
| Treat | 3.00 (1.00, ∞) | 0.08 | n.s. | T0 | 0.42 | Co × T0 | 0.33 | Hi × T0 | 0.51 | |
| Time | 3.83 (1.50, ∞) | 0.03 | * | T1 | 0.52 | Co × T1 | 0.44 | Hi × T1 | 0.59 | |
| Treat × Time | 0.05 (1.50, ∞) | 0.91 | n.s. | T2 | 0.54 | Co × T2 | 0.46 | Hi × T2 | 0.62 | |
female | Coaching | 0.44 | Hiking | 0.54 | ||||||
| Treat | 1.11 (1.00, ∞) | 0.29 | n.s. | T0 | 0.46 | Co × T0 | 0.38 | Hi × T0 | 0.54 | |
| Time | 4.82 (1.87, ∞) | 0.01 | ** | T1 | 0.45 | Co × T1 | 0.39 | Hi × T1 | 0.52 | |
| Treat × Time | 2.26 (1.87, ∞) | 0.11 | n.s. | T2 | 0.56 | Co × T2 | 0.56 | Hi × T2 | 0.57 | |
| Time T1 | 0.02 (1.00, ∞) | 0.90 | n.s. | |||||||
| Time T2 | 8.65 (1.00, ∞) | 0.01 | ** | |||||||
| Treat × T1 | 0.11 (1.00, ∞) | 0.75 | n.s. | |||||||
| Treat × T2 | 5.97 (1.00, ∞) | 0.03 | * | |||||||
| Spirometry | ||||||||||
| FVC % | Coaching | 0.50 | Hiking | 0.50 | ||||||
| Treat | 0.01 (1.00, ∞) | 0.92 | n.s. | T0 | 0.51 | Co × T0 | 0.51 | Hi × T0 | 0.51 | |
| Time | 0.77 (1.75, ∞) | 0.45 | n.s. | T1 | 0.48 | Co × T1 | 0.47 | Hi × T1 | 0.50 | |
| Treat × Time | 0.37 (1.75, ∞) | 0.66 | n.s. | T2 | 0.51 | Co × T2 | 0.51 | Hi × T2 | 0.50 | |
| FEV1 % | Coaching | 0.49 | Hiking | 0.51 | ||||||
| Treat | 0.07 (1.00, ∞) | 0.80 | n.s. | T0 | 0.52 | Co × T0 | 0.52 | Hi × T0 | 0.53 | |
| Time | 2.82 (2.00, ∞) | 0.06 | n.s. | T1 | 0.48 | Co × T1 | 0.47 | Hi × T1 | 0.49 | |
| Treat × Time | 0.00 (2.00, ∞) | 1.00 | n.s. | T2 | 0.49 | Co × T2 | 0.48 | Hi × T2 | 0.50 | |
| PEF % | Coaching | 0.57 | Hiking | 0.44 | ||||||
| Treat | 3.28 (1.00, ∞) | 0.07 | n.s. | T0 | 0.52 | Co × T0 | 0.60 | Hi × T0 | 0.44 | |
| Time | 2.10 (1.88, ∞) | 0.13 | n.s. | T1 | 0.52 | Co × T1 | 0.59 | Hi × T1 | 0.46 | |
| Treat × Time | 0.77 (1.88, ∞) | 0.46 | n.s. | T2 | 0.47 | Co × T2 | 0.52 | Hi × T2 | 0.43 | |
| Parameter | F1-LD-F1 Model | Relative Treatment Effects (RTE) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F (df) | p-Value | Time | Coaching | Hiking | ||||||
| EQ-5D-5L | ||||||||||
| VAS | Coaching | 0.49 | Hiking | 0.51 | ||||||
| Treat | 0.10 (1.00, ∞) | 0.76 | n.s. | T0 | 0.46 | Co × T0 | 0.44 | Hi × T0 | 0.48 | |
| Time | 5.52 (1.73, ∞) | 0.01 | ** | T1 | 0.57 | Co × T1 | 0.57 | Hi × T1 | 0.57 | |
| Treat × Time | 0.22 (1.73, ∞) | 0.77 | n.s. | T2 | 0.47 | Co × T2 | 0.46 | Hi × T2 | 0.48 | |
| Score | Coaching | 0.48 | Hiking | 0.52 | ||||||
| Treat | 0.48 (1.00, ∞) | 0.49 | n.s. | T0 | 0.46 | Co × T0 | 0.46 | Hi × T0 | 0.47 | |
| Time | 2.95 (2.00, ∞) | 0.05 | n.s. | T1 | 0.5 | Co × T1 | 0.46 | Hi × T1 | 0.54 | |
| Treat × Time | 0.84 (2.00, ∞) | 0.43 | n.s. | T2 | 0.53 | Co × T2 | 0.51 | Hi × T2 | 0.55 | |
| SF-36 | ||||||||||
| Physical Functioning | Coaching | 0.43 | Hiking | 0.56 | ||||||
| Treat | 6.27 (1.00, ∞) | 0.01 | * | T0 | 0.45 | Co × T0 | 0.38 | Hi × T0 | 0.53 | |
| Time | 2.63 (1.98, ∞) | 0.07 | n.s. | T1 | 0.49 | Co × T1 | 0.44 | Hi × T1 | 0.54 | |
| Treat × Time | 0.24 (1.98, ∞) | 0.78 | n.s. | T2 | 0.54 | Co × T2 | 0.47 | Hi × T2 | 0.60 | |
| Role—Physical | Coaching | 0.50 | Hiking | 0.50 | ||||||
| Treat | 0.00 (1.00, ∞) | 0.97 | n.s. | T0 | 0.5 | Co × T0 | 0.52 | Hi × T0 | 0.48 | |
| Time | 0.39 (1.80, ∞) | 0.65 | n.s. | T1 | 0.49 | Co × T1 | 0.50 | Hi × T1 | 0.48 | |
| Treat × Time | 2.15 (1.80, ∞) | 0.12 | n.s. | T2 | 0.51 | Co × T2 | 0.48 | Hi × T2 | 0.54 | |
| Bodily Pain | Coaching | 0.43 | Hiking | 0.55 | ||||||
| Treat | 3.95 (1.00, ∞) | 0.05 | * | T0 | 0.47 | Co × T0 | 0.38 | Hi × T0 | 0.57 | |
| Time | 0.74 (1.99, ∞) | 0.48 | n.s. | T1 | 0.5 | Co × T1 | 0.47 | Hi × T1 | 0.53 | |
| Treat × Time | 1.88 (1.99, ∞) | 0.15 | n.s. | T2 | 0.51 | Co × T2 | 0.46 | Hi × T2 | 0.57 | |
| General Health | Coaching | 0.45 | Hiking | 0.54 | ||||||
| Treat | 2.09 (1.00, ∞) | 0.15 | n.s. | T0 | 0.42 | Co × T0 | 0.37 | Hi × T0 | 0.37 | |
| Time | 6.51 (1.82, ∞) | 0.01 | ** | T1 | 0.54 | Co × T1 | 0.49 | Hi × T1 | 0.49 | |
| Treat × Time | 0.09 (1.82, ∞) | 0.90 | n.s. | T2 | 0.53 | Co × T2 | 0.49 | Hi × T2 | 0.49 | |
| Vitality | Coaching | 0.50 | Hiking | 0.50 | ||||||
| Treat | 0.00 (1.00, ∞) | 0.96 | n.s. | T0 | 0.47 | Co × T0 | 0.48 | Hi × T0 | 0.45 | |
| Time | 1.49 (1.63, ∞) | 0.23 | n.s. | T1 | 0.51 | Co × T1 | 0.49 | Hi × T1 | 0.54 | |
| Treat × Time | 0.76 (1.63, ∞) | 0.44 | n.s. | T2 | 0.52 | Co × T2 | 0.53 | Hi × T2 | 0.51 | |
| Social Functioning | Coaching | 0.50 | Hiking | 0.50 | ||||||
| Treat | 0.01 (1.00, ∞) | 0.91 | n.s. | T0 | 0.48 | Co × T0 | 0.49 | Hi × T0 | 0.47 | |
| Time | 0.69 (1.93, ∞) | 0.49 | n.s. | T1 | 0.5 | Co × T1 | 0.49 | Hi × T1 | 0.51 | |
| Treat × Time | 0.28 (1.93, ∞) | 0.75 | n.s. | T2 | 0.52 | Co × T2 | 0.53 | Hi × T2 | 0.51 | |
| Role—Emotional | Coaching | 0.49 | Hiking | 0.50 | ||||||
| Treat | 0.06 (1.00, ∞) | 0.80 | n.s. | T0 | 0.46 | Co × T0 | 0.47 | Hi × T0 | 0.44 | |
| Time | 6.64 (1.88, ∞) | 0.01 | ** | T1 | 0.5 | Co × T1 | 0.51 | Hi × T1 | 0.50 | |
| Treat × Time | 1.65 (1.88, ∞) | 0.19 | n.s. | T2 | 0.54 | Co × T2 | 0.51 | Hi × T2 | 0.57 | |
| Mental Health | Coaching | 0.50 | Hiking | 0.50 | ||||||
| Treat | 0.00 (1.00, ∞) | 0.95 | n.s. | T0 | 0.47 | Co × T0 | 0.46 | Hi × T0 | 0.49 | |
| Time | 1.27 (1.71, ∞) | 0.28 | n.s. | T1 | 0.49 | Co × T1 | 0.50 | Hi × T1 | 0.49 | |
| Treat × Time | 0.19 (1.71, ∞) | 0.79 | n.s. | T2 | 0.53 | Co × T2 | 0.54 | Hi × T2 | 0.53 | |
| Physical Dimension | Coaching | 0.45 | Hiking | 0.54 | ||||||
| Treat | 1.66 (1.00, ∞) | 0.20 | n.s. | T0 | 0.45 | Co × T0 | 0.40 | Hi × T0 | 0.50 | |
| Time | 3.22 (1.93, ∞) | 0.04 | * | T1 | 0.51 | Co × T1 | 0.47 | Hi × T1 | 0.55 | |
| Treat × Time | 0.06 (1.93, ∞) | 0.94 | n.s. | T2 | 0.53 | Co × T2 | 0.49 | Hi × T2 | 0.57 | |
| Mental Dimension | Coaching | 0.50 | Hiking | 0.50 | ||||||
| Treat | 0.00 (1.00, ∞) | 0.94 | n.s. | T0 | 0.45 | Co × T0 | 0.45 | Hi × T0 | 0.45 | |
| Time | 3.65 (1.70, ∞) | 0.03 | * | T1 | 0.51 | Co × T1 | 0.50 | Hi × T1 | 0.52 | |
| Treat × Time | 0.13 (1.70, ∞) | 0.84 | n.s. | T2 | 0.54 | Co × T2 | 0.54 | Hi × T2 | 0.53 | |
| Total Score | Coaching | 0.48 | Hiking | 0.51 | ||||||
| Treat | 0.20 (1.00, ∞) | 0.65 | n.s. | T0 | 0.45 | Co × T0 | 0.43 | Hi × T0 | 0.47 | |
| Time | 3.73 (1.76, ∞) | 0.03 | * | T1 | 0.51 | Co × T1 | 0.49 | Hi × T1 | 0.52 | |
| Treat × Time | 0.09 (1.76, ∞) | 0.89 | n.s. | T2 | 0.54 | Co × T2 | 0.53 | Hi × T2 | 0.55 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huber, D.; Mayr, M.; Hartl, A.; Sittenthaler, S.; Traut-Mattausch, E.; Weisböck-Erdheim, R.; Freidl, J. Sustainability of Hiking in Combination with Coaching in Cardiorespiratory Fitness and Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 3848. https://doi.org/10.3390/ijerph19073848
Huber D, Mayr M, Hartl A, Sittenthaler S, Traut-Mattausch E, Weisböck-Erdheim R, Freidl J. Sustainability of Hiking in Combination with Coaching in Cardiorespiratory Fitness and Quality of Life. International Journal of Environmental Research and Public Health. 2022; 19(7):3848. https://doi.org/10.3390/ijerph19073848
Chicago/Turabian StyleHuber, Daniela, Michaela Mayr, Arnulf Hartl, Sandra Sittenthaler, Eva Traut-Mattausch, Renate Weisböck-Erdheim, and Johanna Freidl. 2022. "Sustainability of Hiking in Combination with Coaching in Cardiorespiratory Fitness and Quality of Life" International Journal of Environmental Research and Public Health 19, no. 7: 3848. https://doi.org/10.3390/ijerph19073848
APA StyleHuber, D., Mayr, M., Hartl, A., Sittenthaler, S., Traut-Mattausch, E., Weisböck-Erdheim, R., & Freidl, J. (2022). Sustainability of Hiking in Combination with Coaching in Cardiorespiratory Fitness and Quality of Life. International Journal of Environmental Research and Public Health, 19(7), 3848. https://doi.org/10.3390/ijerph19073848