
Relationship between Cigarette Smoking and Cancer Characteristics and Survival among Breast Cancer Patients

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Characteristics
3.2. Tumor Pathology
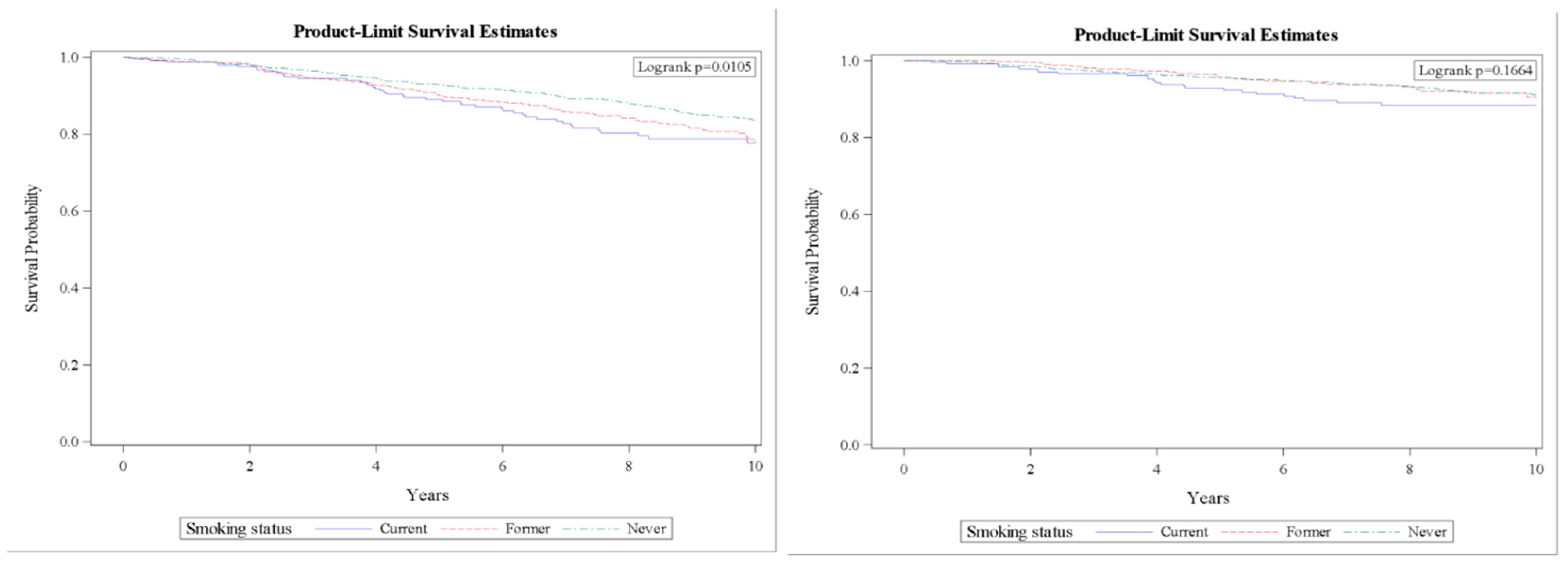
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014.
- Cornelius, M.E.; Wang, T.W.; Jamal, A.; Loretan, C.G.; Neff, L.J. Tobacco Product Use Among Adults—United States, 2019. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1736–1742. [Google Scholar] [CrossRef] [PubMed]
- Conway, K.; Edmiston, S.N.; Cui, L.; Drouin, S.S.; Pang, J.; He, M.; Tse, C.-K.; Geradts, J.; Dressler, L.; Liu, E.T.; et al. Prevalence and spectrum of p53 mutations associated with smoking in breast cancer. Cancer Res. 2002, 62, 1987–1995. [Google Scholar] [PubMed]
- The Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Baron, J.A.; La Vecchia, C.; Levi, F. The antiestrogenic effect of cigarette smoking in women. Am. J. Obstet. Gynecol. 1990, 162, 502–514. [Google Scholar] [CrossRef]
- Dasgupta, P.; Rizwani, W.; Pillai, S.; Kinkade, R.; Kovacs, M.; Rastogi, S.; Banerjee, S.; Carless, M.; Kim, E.; Coppola, D.; et al. Nicotine induces cell proliferation, invasion and epithelial-mesenchymal transition in a variety of human cancer cell lines. Int. J. Cancer 2009, 124, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Hortobagyi, G.N.; Edge, S.B.; Giuliano, A. New and Important Changes in the TNM Staging System for Breast Cancer. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 457–467. [Google Scholar] [CrossRef]
- Bloom, H.J.; Richardson, W.W. Histological grading and prognosis in breast cancer; a study of 1409 cases of which 359 have been followed for 15 years. Br. J. Cancer 1957, 11, 359–377. [Google Scholar] [CrossRef] [Green Version]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Hammond, M.E.H.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [Green Version]
- Hecht, S.S. Tobacco smoke carcinogens and breast cancer. Environ. Mol. Mutagen. 2002, 39, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Petrakis, N.L.; Gruenke, L.D.; Beelen, T.C.; Castagnoli, N., Jr.; Craig, J.C. Nicotine in breast fluid of nonlactating women. Science 1978, 199, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Eng, V.A.; David, S.P.; Li, S.; Ally, M.S.; Stefanick, M.; Tang, J.Y. The association between cigarette smoking, cancer screening, and cancer stage: A prospective study of the women’s health initiative observational cohort. BMJ Open 2020, 10, e037945. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, M.M.; Gapstur, S.M.; Sun, J.; Diver, W.R.; Hannan, L.M.; Thun, M.J. Active smoking and breast cancer risk: Original cohort data and meta-analysis. J. Natl. Cancer Inst. 2013, 105, 515–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gram, I.T.; Park, S.Y.; Maskarinec, G.; Wilkens, L.R.; Haiman, C.A.; Le Marchand, L. Smoking and breast cancer risk by race/ethnicity and oestrogen and progesterone receptor status: The Multiethnic Cohort (MEC) study. Int. J. Epidemiol. 2019, 48, 501–511. [Google Scholar] [CrossRef]
- Dossus, L.; Boutron-Ruault, M.C.; Kaaks, R.; Gram, I.T.; Vilier, A.; Fervers, B.; Manjer, J.; Tjonneland, A.; Olsen, A.; Overva, K.; et al. Active and passive cigarette smoking and breast cancer risk: Results from the EPIC cohort. Int. J. Cancer 2014, 134, 1871–1888. [Google Scholar] [CrossRef] [Green Version]
- Butler, E.N.; Tse, C.K.; Bell, M.E.; Conway, K.; Olshan, A.F.; Troester, M.A. Active smoking and risk of Luminal and Basal-like breast cancer subtypes in the Carolina Breast Cancer Study. Cancer Causes Control 2016, 27, 775–786. [Google Scholar] [CrossRef] [Green Version]
- Baglia, M.L.; Cook, L.S.; Mei-Tzu, C.; Wiggins, C.; Hill, D.; Porter, P.; Li, C.I. Alcohol, smoking, and risk of Her2-overexpressing and triple-negative breast cancer relative to estrogen receptor-positive breast cancer. Int. J. Cancer 2018, 143, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Goldvaser, H.; Gal, O.; Rizel, S.; Hendler, D.; Neiman, V.; Shochat, T.; Sulkes, A.; Brenner, B.; Yerushalmi, R. The association between smoking and breast cancer characteristics and outcome. BMC Cancer 2017, 17, 624. [Google Scholar] [CrossRef] [Green Version]
- Holmes, M.D.; Murin, S.; Chen, W.Y.; Kroenke, C.H.; Spiegelman, D.; Colditz, G.A. Smoking and survival after breast cancer diagnosis. Int. J. Cancer 2007, 120, 2672–2677. [Google Scholar] [CrossRef]
- Kakugawa, Y.; Kawai, M.; Nishino, Y.; Fukamachi, K.; Ishida, T.; Ohuchi, N.; Minami, Y. Smoking and survival after breast cancer diagnosis in Japanese women: A prospective cohort study. Cancer Sci. 2015, 106, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Simonsson, M.; Markkula, A.; Rose, C.; Ingvar, C.; Jernstrom, H. Impacts of smoking on endocrine treatment response in a prospective breast cancer cohort. Br. J. Cancer 2016, 115, 382–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagiv, S.K.; Gaudet, M.M.; Eng, S.M.; Abrahamson, P.E.; Shantakumar, S.; Teitelbaum, S.L.; Britton, J.A.; Bell, P.; Thomas, J.A.; Neugut, A.I.; et al. Active and passive cigarette smoke and breast cancer survival. Ann. Epidemiol. 2007, 17, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Li, F.; Zhang, X.; Li, Z.; Li, H. Smoking increases risks of all-cause and breast cancer specific mortality in breast cancer individuals: A dose-response meta-analysis of prospective cohort studies involving 39725 breast cancer cases. Oncotarget 2016, 7, 83134–83147. [Google Scholar] [CrossRef] [Green Version]
- Duan, W.; Li, S.; Meng, X.; Sun, Y.; Jia, C. Smoking and survival of breast cancer patients: A meta-analysis of cohort studies. Breast 2017, 33, 117–124. [Google Scholar] [CrossRef]
- Braithwaite, D.; Izano, M.; Moore, D.H.; Kwan, M.L.; Tammemagi, M.C.; Hiatt, R.A.; Kerlikowske, K.; Kroenke, C.H.; Sweeney, C.; Habel, L.; et al. Smoking and survival after breast cancer diagnosis: A prospective observational study and systematic review. Breast Cancer Res. Treat. 2012, 136, 521–533. [Google Scholar] [CrossRef] [Green Version]
- Sollie, M.; Bille, C. Smoking and mortality in women diagnosed with breast cancer-a systematic review with meta-analysis based on 400,944 breast cancer cases. Gland Surg. 2017, 6, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Pierce, J.P.; Patterson, R.E.; Senger, C.M.; Flatt, S.W.; Caan, B.; Natarajan, L.; Nechuta, S.; Poole, E.M.; Shu, X.-O.; Chen, W.Y. Lifetime cigarette smoking and breast cancer prognosis in the After Breast Cancer Pooling Project. J. Natl. Cancer Inst. 2014, 106, djt359. [Google Scholar] [CrossRef] [Green Version]
- Passarelli, M.N.; Newcomb, P.A.; Hampton, J.M.; Trentham-Dietz, A.; Titus, L.J.; Egan, K.M.; Baron, J.A.; Willett, W.C. Cigarette Smoking before and after Breast Cancer Diagnosis: Mortality from Breast Cancer and Smoking-Related Diseases. J. Clin. Oncol. 2016, 34, 1315–1322. [Google Scholar] [CrossRef]
- Ordóñez-Mena, J.M.; Schöttker, B.; Mons, U.; Jenab, M.; Freisling, H.; Bueno-De-Mesquita, B.; O’Doherty, M.G.; Scott, A.; Kee, F.; Stricker, B.H.; et al. Quantification of the smoking-associated cancer risk with rate advancement periods: Meta-analysis of individual participant data from cohorts of the CHANCES consortium. BMC Med. 2016, 14, 62. [Google Scholar] [CrossRef]
- Parada, H., Jr.; Sun, X.; Tse, C.K.; Olshan, A.F.; Troester, M.A.; Conway, K. Active smoking and survival following breast cancer among African American and non-African American women in the Carolina Breast Cancer Study. Cancer Causes Control 2017, 28, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Caini, S.; Del Riccio, M.; Vettori, V.; Scotti, V.; Martinoli, C.; Raimondi, S.; Cammarata, G.; Palli, D.; Banini, M.; Masala, G.; et al. Quitting smoking at or around diagnosis improves the overall survival of lung cancer patients: A systematic review and meta-analysis. J. Thorac. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mizota, Y.I.T.; Ohashi, Y.; Mukai, H.; Yamamoto, S. The effects of smoking and smoking cessation on postmenopausal breast cancer recurrence—Results from the Cohort 05 of the Rainbow of KIBOU (ROK) study: A prospective breast cancer survivor cohort in Japan. Cancer Res. 2020, 80, nr P3-08-36. [Google Scholar]
- Passarelli, M.N.; Newcomb, P.A. Survival Benefits of Smoking Cessation after Breast Cancer Diagnosis. JNCI Cancer Spectr. 2017, 1, pkx005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parada, H., Jr.; Bradshaw, P.T.; Steck, S.E.; Engel, L.S.; Conway, K.; Teitelbaum, S.L.; Neugut, A.I.; Santella, R.M.; Gammon, M.D. Postdiagnosis Changes in Cigarette Smoking and Survival Following Breast Cancer. JNCI Cancer Spectr. 2017, 1, pkx001. [Google Scholar] [CrossRef] [PubMed]
- Strumylaite, L.; Kregzdyte, R.; Poskiene, L.; Bogusevicius, A.; Pranys, D.; Norkute, R. Association between lifetime exposure to passive smoking and risk of breast cancer subtypes defined by hormone receptor status among non-smoking Caucasian women. PLoS ONE 2017, 12, e0171198. [Google Scholar] [CrossRef] [Green Version]
- Parada, H., Jr.; Bradshaw, P.T.; Engel, L.S.; Conway, K.; Steck, S.E.; Teitelbaum, S.L.; Neugut, A.I.; Santella, R.M.; Gammon, M.D. Environmental Tobacco Smoke Exposure and Survival Following Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2017, 26, 278–280. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Never (n = 1330) | Former (n = 564) | Current (n = 259) | p-Value | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Age at Diagnosis | <0.0001 | ||||||
| <45 | 243 | 18.3 | 50 | 8.9 | 38 | 14.7 | |
| 45–54 | 359 | 27.0 | 126 | 22.3 | 96 | 37.1 | |
| 55–64 | 340 | 25.6 | 165 | 29.3 | 75 | 29.0 | |
| 65–74 | 253 | 19.0 | 152 | 27.0 | 39 | 15.1 | |
| 75+ | 135 | 10.2 | 71 | 12.6 | 11 | 4.3 | |
| Race/Ethnicity | 0.0005 b | ||||||
| NHW | 997 | 75.0 | 470 | 83.3 | 216 | 83.4 | |
| NHB | 252 | 19.0 | 77 | 13.7 | 28 | 10.8 | |
| Asian | 43 | 3.2 | 7 | 1.2 | 7 | 2.7 | |
| Hispanic | 23 | 1.7 | 9 | 1.6 | 6 | 2.3 | |
| Other/Unknown | 15 | 1.1 | 1 | 0.2 | 2 | 0.8 | |
| Education | <0.0001 b | ||||||
| Less than 4 Year College a | 617 | 46.4 | 333 | 59.0 | 182 | 70.3 | |
| 4 Year College or Beyond | 578 | 43.5 | 209 | 37.1 | 58 | 22.4 | |
| Unknown | 135 | 10.2 | 22 | 3.9 | 19 | 7.3 | |
| Marital Status | 0.2223 b | ||||||
| Not Married | 389 | 29.3 | 184 | 32.6 | 92 | 35.5 | |
| Married | 932 | 70.1 | 377 | 66.8 | 165 | 63.7 | |
| Unknown | 9 | 0.7 | 3 | 0.5 | 2 | 0.8 | |
| BMI | 0.1654 c | ||||||
| Less than 25 | 430 | 32.3 | 158 | 28.0 | 97 | 37.5 | |
| 25–29.9 | 410 | 30.8 | 191 | 33.9 | 79 | 30.5 | |
| 30 or Greater | 487 | 36.6 | 213 | 37.8 | 83 | 32.1 | |
| Unknown | 3 | 0.23 | 2 | 0.35 | 0 | 0.0 | |
| CCI | <0.0001 | ||||||
| 0 | 370 | 27.8 | 99 | 17.6 | 67 | 25.9 | |
| 1 | 312 | 23.5 | 121 | 21.5 | 77 | 29.7 | |
| 2 | 291 | 21.9 | 147 | 26.1 | 59 | 22.8 | |
| 3+ | 357 | 26.8 | 196 | 34.8 | 55 | 21.2 | |
| Unknown | 0 | 0.0 | 1 | 0.2 | 1 | 0.4 | |
| Site of enrollment | <0.0001 | ||||||
| AAMC | 627 | 47.1 | 361 | 64.0 | 140 | 54.1 | |
| JMBCC | 175 | 13.2 | 60 | 10.6 | 62 | 23.9 | |
| WR | 528 | 39.7 | 143 | 25.4 | 57 | 22.0 | |
| Characteristic | Never (n = 1330) | Former (n = 564) | Current (n = 259) | p-Value | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| AJCC Pathological Stage | 0.0027 | ||||||
| Stage I | 684 | 51.4 | 340 | 60.3 | 118 | 45.6 | |
| Stage II | 446 | 33.5 | 161 | 28.5 | 93 | 35.9 | |
| Stage III/IV a | 180 | 13.6 | 53 | 9.4 | 43 | 16.6 | |
| Unknown | 20 | 1.5 | 10 | 1.8 | 5 | 1.9 | |
| Tumor Type | 0.9031 | ||||||
| IDCA | 1013 | 76.2 | 432 | 76.6 | 202 | 78.0 | |
| ILCA | 157 | 11.8 | 61 | 10.8 | 29 | 11.2 | |
| Other | 140 | 10.5 | 65 | 11.5 | 26 | 10.0 | |
| Unknown | 20 | 1.5 | 6 | 1.1 | 2 | 0.8 | |
| Tumor Grade | 0.3289 | ||||||
| Well Differentiated | 331 | 24.9 | 149 | 26.4 | 52 | 20.1 | |
| Moderately Differentiated | 502 | 37.7 | 204 | 36.2 | 114 | 44.0 | |
| Poorly Differentiated | 450 | 33.8 | 191 | 33.9 | 87 | 33.6 | |
| Unknown | 47 | 3.5 | 20 | 3.6 | 6 | 2.3 | |
| Tumor Size | 0.0185 | ||||||
| T1 | 836 | 62.9 | 382 | 67.7 | 143 | 55.2 | |
| T2 | 377 | 28.4 | 145 | 25.7 | 87 | 33.6 | |
| T3/T4 | 82 | 6.2 | 23 | 4.1 | 17 | 6.6 | |
| Unknown | 35 | 2.6 | 14 | 2.5 | 12 | 4.6 | |
| ER Status | 0.0530 b | ||||||
| Negative | 236 | 17.7 | 86 | 15.3 | 55 | 21.2 | |
| Positive | 1091 | 82.0 | 478 | 84.8 | 202 | 78.0 | |
| Unknown | 3 | 0.2 | 0 | 0.0 | 2 | 0.8 | |
| PR Status | 0.0972 b | ||||||
| Negative | 420 | 31.6 | 158 | 28.0 | 87 | 33.6 | |
| Positive | 905 | 68.1 | 406 | 72.0 | 170 | 65.6 | |
| Unknown | 5 | 0.4 | 0 | 0.0 | 2 | 0.8 | |
| HER2 Status | 0.4435 | ||||||
| Negative | 1114 | 83.8 | 476 | 84.4 | 206 | 79.5 | |
| Positive | 193 | 14.5 | 79 | 14.0 | 46 | 17.8 | |
| Unknown | 23 | 1.7 | 9 | 1.6 | 7 | 2.7 | |
| Node Status | 0.0005 | ||||||
| Negative | 853 | 64.1 | 409 | 72.5 | 153 | 59.1 | |
| Positive | 445 | 33.5 | 141 | 25.0 | 101 | 39.0 | |
| Unknown | 32 | 2.4 | 14 | 2.5 | 5 | 1.9 | |
| Adjusted OR for Smoker vs. Never Smoked | |||
|---|---|---|---|
| Response Variable | Smoking Status | ||
| Current Smoker | Former Smoker | ||
| Tumor stage | Stage I | Reference | Reference |
| Stage II | 1.247 (0.895, 1.739) | 0.795 (0.624, 1.012) | |
| Stage III | 1.260 (0.771, 2.059) | 0.832 (0.565, 1.224) | |
| Stage IV | 2.675 (0.998, 7.170) | 0.278 (0.063, 1.233) | |
| Tumor type | IDCA | Reference | Reference |
| ILCA | 1.055 (0.654, 1.701) | 0.876 (0.623, 1.233) | |
| Other | 0.969 (0.580, 1.619) | 1.002 (0.698, 1.438) | |
| Tumor grade | Well-differentiated (grade 1) | Reference | Reference |
| Moderately differentiated (grade 2) | 1.460 (0.971, 2.193) | 0.890 (0.675, 1.172) | |
| Poorly differentiated (grade 3) | 1.207 (0.784, 1.857) | 1.031 (0.775, 1.371) | |
| Tumor size | T1 | Reference | Reference |
| T2 | 1.337 (0.963, 1.856) | 0.957 (0.748, 1.224) | |
| T3/4 | 1.386 (0.755, 2.545) | 0.755 (0.443, 1.287) | |
| ER | Negative | Reference | Reference |
| Positive | 0.777 (0.527, 1.147) | 1.031 (0.756, 1.406) | |
| PR | Negative | Reference | Reference |
| Positive | 0.889 (0.643, 1.230) | 1.166 (0.914, 1.488) | |
| HER2 | Negative | Reference | Reference |
| Positive | 1.209 (0.807, 1.812) | 0.940 (0.680, 1.299) | |
| Node | Negative | Reference | Reference |
| Positive | 1.235 (0.904, 1.688) | 0.759 (0.595, 0.967) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darmon, S.; Park, A.; Lovejoy, L.A.; Shriver, C.D.; Zhu, K.; Ellsworth, R.E. Relationship between Cigarette Smoking and Cancer Characteristics and Survival among Breast Cancer Patients. Int. J. Environ. Res. Public Health 2022, 19, 4084. https://doi.org/10.3390/ijerph19074084
Darmon S, Park A, Lovejoy LA, Shriver CD, Zhu K, Ellsworth RE. Relationship between Cigarette Smoking and Cancer Characteristics and Survival among Breast Cancer Patients. International Journal of Environmental Research and Public Health. 2022; 19(7):4084. https://doi.org/10.3390/ijerph19074084
Chicago/Turabian StyleDarmon, Sarah, Amie Park, Leann A. Lovejoy, Craig D. Shriver, Kangmin Zhu, and Rachel E. Ellsworth. 2022. "Relationship between Cigarette Smoking and Cancer Characteristics and Survival among Breast Cancer Patients" International Journal of Environmental Research and Public Health 19, no. 7: 4084. https://doi.org/10.3390/ijerph19074084
APA StyleDarmon, S., Park, A., Lovejoy, L. A., Shriver, C. D., Zhu, K., & Ellsworth, R. E. (2022). Relationship between Cigarette Smoking and Cancer Characteristics and Survival among Breast Cancer Patients. International Journal of Environmental Research and Public Health, 19(7), 4084. https://doi.org/10.3390/ijerph19074084