
Factors Associated with the Risk of Major Adverse Cardiovascular Events in Patients with Ankylosing Spondylitis: A Nationwide, Population-Based Case—Control Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Source of Data and Study Population
2.3. Identification of MACE Cases and Non-MACE Matched Controls
2.4. Independent Variables
2.5. Patient and Public Involvement
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
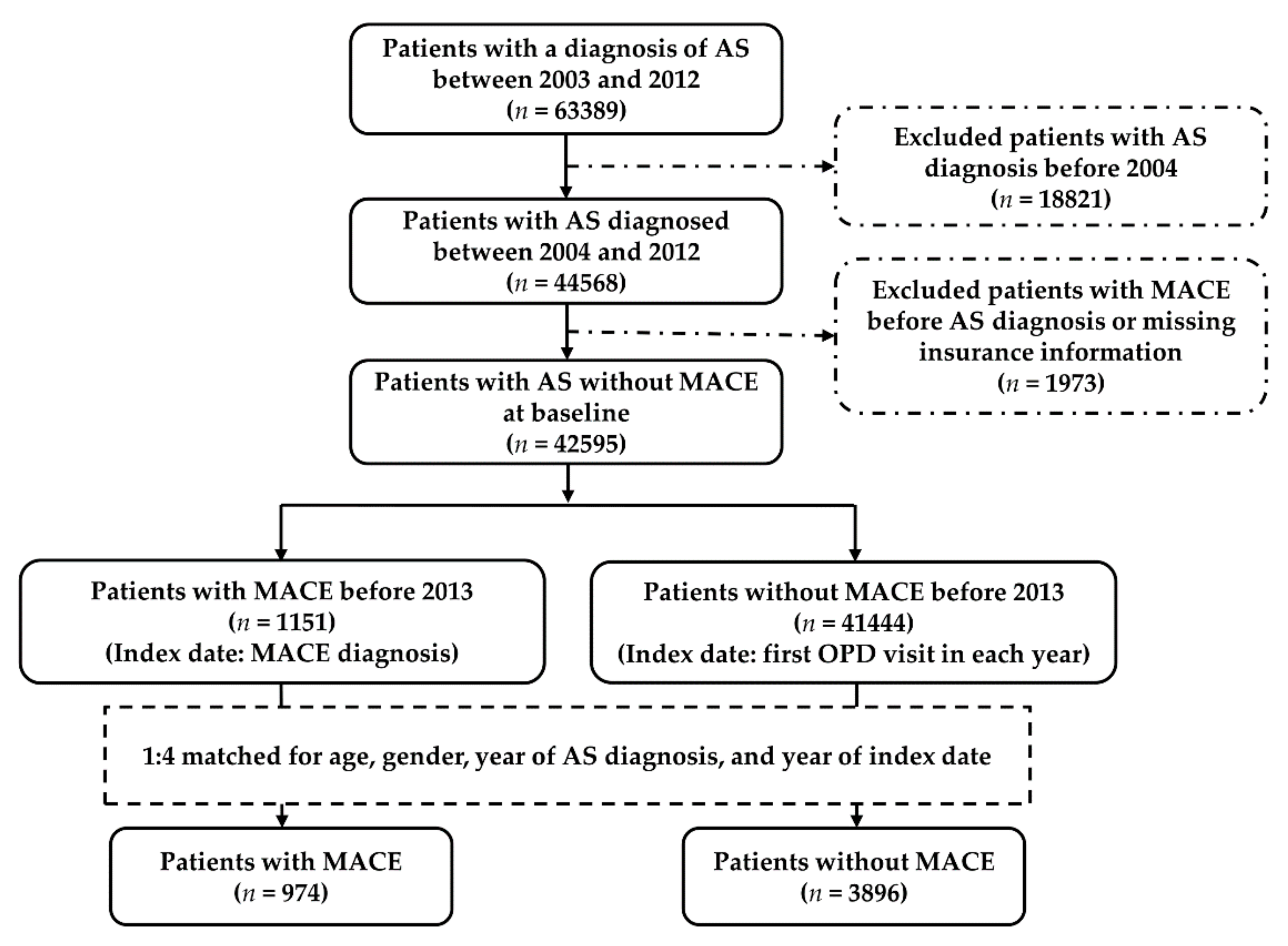
3.1. Selection and Grouping of Study Population and Prevalence and Incidence of MACE
3.2. Baseline Characteristics of the Study Population
3.3. Risk Factors of MACE Development in Patients with AS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, H.H.; Chen, T.J.; Chen, Y.M.; Ying-Ming, C.; Chen, D.Y. Gender differences in ankylosing spondylitis-associated cumulative healthcare utilization: A population-based cohort study. Clinics 2011, 66, 251–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.T.; Pei, L.; Chang, D.M.; Lee, C.F.; Schumacher, H.R.; Liang, M.H. Prevalence of rheumatic diseases in Taiwan: A population study of urban, suburban, rural differences. J. Rheumatol. 1994, 21, 302–306. [Google Scholar] [PubMed]
- Hsieh, M.-Y.; Kuo, C.-F. FRI0428 Epidemiology of Ankylosing Spondylitis in Taiwan: A Nationwide Population Study. Ann. Rheum. Dis. 2016, 75 (Suppl. S2), 590–591. [Google Scholar] [CrossRef]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; Landewe, R.; van der Heijde, D.; Listing, J.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Collantes-Estevez, E.; Davis, J.; Dijkmans, B.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part I): Classification of paper patients by expert opinion including uncertainty appraisal. Ann. Rheum. Dis. 2009, 68, 770–776. [Google Scholar] [CrossRef]
- Rudwaleit, M.; van der Heijde, D.; Landewe, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, J.C.; Liu, C.H.; Tseng, J.C.; Hsieh, L.F.; Chen, C.H.; Chen, H.H.; Chen, H.A.; Chen, Y.C.; Chou, C.T.; Liao, H.T.; et al. Taiwan Rheumatology Association consensus recommendations for the management of axial spondyloarthritis. Int. J. Rheum. Dis. 2020, 23, 7–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, S.S.; Robertson, S.; Reich, T.; Harrison, N.L.; Moots, R.J.; Goodson, N.J. Prevalence and impact of comorbidities in axial spondyloarthritis: Systematic review and meta-analysis. Rheumatology 2020, 59 (Suppl. S4), iv47–iv57. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.H.; Yeh, S.J.; Tsai, W.P.; Wang, C.M.; Chen, J.Y. Paroxysmal supraventricular tachycardia and Wolff-Parkinson-White syndrome in ankylosing spondylitis: A large cohort observation study and literature review. Semin. Arthritis Rheum. 2012, 42, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Roldan, C.A.; Chavez, J.; Wiest, P.W.; Qualls, C.R.; Crawford, M.H. Aortic root disease and valve disease associated with ankylosing spondylitis. J. Am. Coll. Cardiol. 1998, 32, 1397–1404. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Chung, H.Y.; Zhao, C.T.; Wong, A.; Zhen, Z.; Tsang, H.H.; Lau, C.S.; Tse, H.F.; Yiu, K.H. Left ventricular myocardial dysfunction and premature atherosclerosis in patients with axial spondyloarthritis. Rheumatology 2015, 54, 292–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.H.; Lin, M.C.; Peng, C.L.; Wu, Y.C.; Sung, F.C.; Kao, C.H.; Liu, S.H. A nationwide population-based retrospective cohort study: Increased risk of acute coronary syndrome in patients with ankylosing spondylitis. Scand. J. Rheumatol. 2014, 43, 132–136. [Google Scholar] [CrossRef]
- Szabo, S.M.; Levy, A.R.; Rao, S.R.; Kirbach, S.E.; Lacaille, D.; Cifaldi, M.; Maksymowych, W.P. Increased risk of cardiovascular and cerebrovascular diseases in individuals with ankylosing spondylitis: A population-based study. Arthritis Rheum. 2011, 63, 3294–3304. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Yeh, S.Y.; Chen, H.Y.; Lin, C.L.; Sung, F.C.; Kao, C.H. Ankylosing spondylitis and other inflammatory spondyloarthritis increase the risk of developing type 2 diabetes in an Asian population. Rheumatol. Int. 2014, 34, 265–270. [Google Scholar] [CrossRef] [PubMed]
- van Halm, V.P.; van Denderen, J.C.; Peters, M.J.; Twisk, J.W.; van der Paardt, M.; van der Horst-Bruinsma, I.E.; van de Stadt, R.J.; de Koning, M.H.; Dijkmans, B.A.; Nurmohamed, M.T. Increased disease activity is associated with a deteriorated lipid profile in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2006, 65, 1473–1477. [Google Scholar] [CrossRef]
- Maas, F.; Arends, S.; van der Veer, E.; Wink, F.; Efde, M.; Bootsma, H.; Brouwer, E.; Spoorenberg, A. Obesity Is Common in Axial Spondyloarthritis and Is Associated with Poor Clinical Outcome. J. Rheumatol. 2016, 43, 383–387. [Google Scholar] [CrossRef]
- Bakland, G.; Gran, J.T.; Nossent, J.C. Increased mortality in ankylosing spondylitis is related to disease activity. Ann. Rheum. Dis. 2011, 70, 1921–1925. [Google Scholar] [CrossRef] [PubMed]
- Rueda-Gotor, J.; Genre, F.; Corrales, A.; Blanco, R.; Fuentevilla, P.; Portilla, V.; Exposito, R.; Arnaiz, C.M.; Pina, T.; Gonzalez-Juanatey, C.; et al. Relative Risk Chart Score for the Assessment of the Cardiovascular Risk in Young Patients with Ankylosing Spondylitis. Int. J. Rheumatol. 2018, 2018, 1847894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, K.A.; Tcheng, J.E.; Bozkurt, B.; Chaitman, B.R.; Cutlip, D.E.; Farb, A.; Fonarow, G.C.; Jacobs, J.P.; Jaff, M.R.; Lichtman, J.H.; et al. 2014 ACC/AHA Key Data Elements and Definitions for Cardiovascular Endpoint Events in Clinical Trials: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Cardiovascular Endpoints Data Standards). J. Am. Coll. Cardiol. 2015, 66, 403–469. [Google Scholar] [PubMed] [Green Version]
- Dehmer, G.J.; Badhwar, V.; Bermudez, E.A.; Cleveland, J.C., Jr.; Cohen, M.G.; D’Agostino, R.S.; Ferguson, T.B., Jr.; Hendel, R.C.; Isler, M.L.; Jacobs, J.P.; et al. 2020 AHA/ACC Key Data Elements and Definitions for Coronary Revascularization: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Coronary Revascularization). J. Am. Coll. Cardiol. 2020, 75, 1975–2088. [Google Scholar] [PubMed]
- Liu, C.H.; Hung, Y.T.; Chuang, Y.L.; Che, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating Development Stratification of Taiwan Townships into Sampling Design of Large Scale Health Interview Survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar]
- Cossman, J.S.; James, W.L.; Cosby, A.G.; Cossman, R.E. Underlying causes of the emerging nonmetropolitan mortality penalty. Am. J. Public Health 2010, 100, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.A.; Eldridge, G.; Graham, M.L.; Folta, S.C.; Nelson, M.E.; Strogatz, D. Strong Hearts, healthy communities: A rural community-based cardiovascular disease prevention program. BMC Public Health 2016, 16, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollick, R.J.; Stelfox, K.; Dean, L.E.; Shim, J.; Walker-Bone, K.; Macfarlane, G.J. Outcomes and treatment responses, including work productivity, among people with axial spondyloarthritis living in urban and rural areas: A mixed-methods study within a national register. Ann. Rheum. Dis. 2020, 79, 1055–1062. [Google Scholar] [CrossRef]
- Rueda-Gotor, J.; Corrales, A.; Blanco, R.; Fuentevilla, P.; Portilla, V.; Exposito, R.; Mata, C.; Pina, T.; Gonzalez-Juanatey, C.; Llorca, J.; et al. Atherosclerotic disease in axial spondyloarthritis: Increased frequency of carotid plaques. Clin. Exp. Rheumatol. 2015, 33, 315–320. [Google Scholar]
- Brophy, S.; Cooksey, R.; Atkinson, M.; Zhou, S.M.; Husain, M.J.; Macey, S.; Rahman, M.A.; Siebert, S. No increased rate of acute myocardial infarction or stroke among patients with ankylosing spondylitis-a retrospective cohort study using routine data. Semin. Arthritis Rheum. 2012, 42, 140–145. [Google Scholar] [CrossRef]
- Schieir, O.; Tosevski, C.; Glazier, R.H.; Hogg-Johnson, S.; Badley, E.M. Incident myocardial infarction associated with major types of arthritis in the general population: A systematic review and meta-analysis. Ann. Rheum. Dis. 2017, 76, 1396–1404. [Google Scholar] [CrossRef]
- Bai, R.; Zhang, Y.; Liu, W.; Ma, C.; Chen, X.; Yang, J.; Sun, D. The Relationship of Ankylosing Spondylitis and Subclinical Atherosclerosis: A Systemic Review and Meta-Analysis. Angiology 2019, 70, 492–500. [Google Scholar] [CrossRef]
- Arida, A.; Protogerou, A.D.; Konstantonis, G.; Konsta, M.; Delicha, E.M.; Kitas, G.D.; Sfikakis, P.P. Subclinical Atherosclerosis Is Not Accelerated in Patients with Ankylosing Spondylitis with Low Disease Activity: New Data and Metaanalysis of Published Studies. J. Rheumatol. 2015, 42, 2098–2105. [Google Scholar] [CrossRef]
- Levy, A.R.; Szabo, S.M.; Rao, S.R.; Cifaldi, M.; Maksymowych, W.P. Estimating the occurrence of renal complications among persons with ankylosing spondylitis. Arthritis Care Res. 2014, 66, 440–445. [Google Scholar] [CrossRef]
- Siao, W.Z.; Liu, C.H.; Wang, Y.H.; Wei, J.C.; Jong, G.P. Increased risk of valvular heart disease in patients with ankylosing spondylitis: A nationwide population-based longitudinal cohort study. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211021676. [Google Scholar] [CrossRef] [PubMed]
- Sharif, K.; Watad, A.; Tiosano, S.; Yavne, Y.; Blokh Kerpel, A.; Comaneshter, D.; Cohen, A.D.; Amital, H. The link between COPD and ankylosing spondylitis: A population based study. Eur. J. Intern. Med. 2018, 53, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Diabetes, heart failure, and renal dysfunction: The vicious circles. Prog. Cardiovasc. Dis. 2019, 62, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Li, X.C.; Lu, L.; Cao, Y.; Sun, R.R.; Chen, S.; Zhang, P.Y. Cardiovascular disease and its relationship with chronic kidney disease. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 2918–2926. [Google Scholar]
- Urena-Torres, P.; D’Marco, L.; Raggi, P.; Garcia-Moll, X.; Brandenburg, V.; Mazzaferro, S.; Lieber, A.; Guirado, L.; Bover, J. Valvular heart disease and calcification in CKD: More common than appreciated. Nephrol. Dial. Transpl. 2020, 35, 2046–2053. [Google Scholar] [CrossRef]
- Elewaut, D.; Matucci-Cerinic, M. Treatment of ankylosing spondylitis and extra-articular manifestations in everyday rheumatology practice. Rheumatology 2009, 48, 1029–1035. [Google Scholar] [CrossRef] [Green Version]
- Fosslien, E. Cardiovascular complications of non-steroidal anti-inflammatory drugs. Ann. Clin. Lab. Sci. 2005, 35, 347–385. [Google Scholar]
- Ghosh, R.; Alajbegovic, A.; Gomes, A.V. NSAIDs and Cardiovascular Diseases: Role of Reactive Oxygen Species. Oxid. Med. Cell. Longev. 2015, 2015, 536962. [Google Scholar] [CrossRef] [Green Version]
- Karmacharya, P.; Shahukhal, R.; Crowson, C.S.; Murad, M.H.; Davis, J.M., 3rd; Shrestha, P.; Bekele, D.; Wright, K.; Chakradhar, R.; Dubreuil, M. Effects of Therapies on Cardiovascular Events in Ankylosing Spondylitis: A Systematic Review and Meta-Analysis. Rheumatol. Ther. 2020, 7, 993–1009. [Google Scholar] [CrossRef]
- Braun, J.; Baraliakos, X.; Westhoff, T. Nonsteroidal anti-inflammatory drugs and cardiovascular risk—A matter of indication. Semin. Arthritis Rheum. 2020, 50, 285–288. [Google Scholar] [CrossRef]
- Helin-Salmivaara, A.; Virtanen, A.; Vesalainen, R.; Gronroos, J.M.; Klaukka, T.; Idanpaan-Heikkila, J.E.; Huupponen, R. NSAID use and the risk of hospitalization for first myocardial infarction in the general population: A nationwide case-control study from Finland. Eur. Heart J. 2006, 27, 1657–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.C.; Leong, P.Y.; Yeo, K.J.; Li, T.Y.; Wang, Y.H.; Chiou, J.Y.; Wei, J.C. Celecoxib and sulfasalazine had negative association with coronary artery diseases in patients with ankylosing spondylitis: A nation-wide, population-based case-control study. Medicine 2016, 95, e4792. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.C.; Ou, T.T.; Yen, J.H.; Wu, C.C.; Tung, Y.C. Long-term frequent use of non-steroidal anti-inflammatory drugs might protect patients with ankylosing spondylitis from cardiovascular diseases: A nationwide case-control study. PLoS ONE 2015, 10, e0126347. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Lanes, S.; Triadafilopoulos, G. Risk of serious upper gastrointestinal and cardiovascular thromboembolic complications with meloxicam. Am. J. Med. 2004, 117, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Asghar, W.; Jamali, F. The effect of COX-2-selective meloxicam on the myocardial, vascular and renal risks: A systematic review. Inflammopharmacology 2015, 23, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Heslinga, S.C.; Van Sijl, A.M.; De Boer, K.; Van Halm, V.P.; Nurmohamed, M.T. Tumor necrosis factor blocking therapy and congestive heart failure in patients with inflammatory rheumatic disorders: A systematic review. Curr. Med. Chem. 2015, 22, 1892–1902. [Google Scholar] [CrossRef]
- Hokstad, I.; Deyab, G.; Wang Fagerland, M.; Lyberg, T.; Hjeltnes, G.; Forre, O.; Agewall, S.; Mollnes, T.E.; Hollan, I. Tumor necrosis factor inhibitors are associated with reduced complement activation in spondylarthropathies: An observational study. PLoS ONE 2019, 14, e0220079. [Google Scholar] [CrossRef] [Green Version]
- Atzeni, F.; Nucera, V.; Galloway, J.; Zoltan, S.; Nurmohamed, M. Cardiovascular risk in ankylosing spondylitis and the effect of anti-TNF drugs: A narrative review. Expert Opin. Biol. Ther. 2020, 20, 517–524. [Google Scholar] [CrossRef]
- Beringer, A.; Miossec, P. Systemic effects of IL-17 in inflammatory arthritis. Nat. Rev. Rheumatol. 2019, 15, 491–501. [Google Scholar] [CrossRef]
- Wei, C.Y.; Kung, W.M.; Chou, Y.S.; Wang, Y.C.; Tai, H.C.; Wei, J.C. Cardiac Autonomic Function in Patients with Ankylosing Spondylitis: A Case-Control Study. Medicine 2016, 95, e3749. [Google Scholar] [CrossRef]
- Wei, J.C.; Jan, M.S.; Yu, C.T.; Huang, Y.C.; Yang, C.C.; Tsou, H.K.; Lee, H.S.; Chou, C.T.; Tsay, G.; Chou, M.C. Plasma homocysteine status in patients with ankylosing spondylitis. Clin. Rheumatol. 2007, 26, 739–742. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Non-MACE (n = 3896) | MACE (n = 974) | p Value | |
|---|---|---|---|
| Age at diagnosis of AS, years | 59.3 ± 12.1 | 59.3 ± 12.1 | 1.000 |
| Age at diagnosis of MACE, years | 63.1 ± 12.0 | 63.1 ± 12.0 | 1.000 |
| Male, n (%) | 2604 (66.8) | 651 (66.8) | 1.000 |
| Urbanisation, n (%) | 0.449 | ||
| Urban | 1035 (26.6) | 240 (24.6) | |
| Suburban | 1647 (42.3) | 418 (42.9) | |
| Rural | 1213 (31.1) | 316 (32.4) | |
| Low income, n (%) 1 | 1777 (45.6) | 467 (47.9) | 0.191 |
| Comorbidities | |||
| Hypertension, n (%) | 1415 (36.3) | 709 (72.8) | <0.001 |
| Hyperlipidaemia receiving lipid-lowering agents, n (%) | 761 (19.5) | 619 (61.3) | <0.001 |
| Diabetes mellitus, n (%) | 546 (14.0) | 349 (35.8) | <0.001 |
| Chronic kidney disease, n (%) | 96 (2.5) | 95 (9.8) | <0.001 |
| Heart failure, n (%) | 75 (1.9) | 114 (11.7) | <0.001 |
| Valvular heart disease, n (%) | 77 (2.0) | 69 (7.1) | <0.001 |
| COPD, n (%) | 327 (8.4) | 114 (11.7) | 0.001 |
| Extra-articular manifestations | |||
| Acute anterior uveitis, n (%) | 321 (8.2) | 80 (8.2) | 0.979 |
| Psoriasis, n (%) | 91 (2.3) | 25 (2.6) | 0.672 |
| Inflammatory bowel disease, n (%) | 23 (0.6) | 4 (0.4) | 0.499 |
| Antiplatelet agents, n (%) | 825 (21.2) | 913 (93.7) | <0.001 |
| Anticoagulation agents, n (%) | 86 (2.2) | 456 (46.8) | <0.001 |
| Biologics, n (%) | 35 (0.9) | 7 (0.7) | 0.588 |
| Methotrexate, n (%) | 139 (3.6) | 30 (3.1) | 0.457 |
| Sulfasalazine, n (%) | 676 (17.4) | 165 (16.9) | 0.762 |
| Steroid use, n (%) | 1282 (32.9) | 473 (48.6) | <0.001 |
| No use | 2614 (67.1) | 501 (51.4) | |
| <5 mg/day | 1081 (27.7) | 296 (30.4) | |
| ≥5 mg/day | 201 (5.2) | 177 (18.2) | |
| NSAIDs, n (%) | 3372 (86.6) | 890 (91.4) | <0.001 |
| NSAIDs, cDDD | 79.7 ± 104.4 | 97.5 ± 117.5 | <0.001 |
| None | 524 (13.4) | 86 (8.6) | <0.001 |
| 0 < cDDD ≤ 18.75 | 856 (22.0) | 213 (21.9) | |
| 18.75 < cDDD ≤ 56 | 872 (22.4) | 197 (20.2) | |
| 56 < cDDD ≤ 131.25 | 831 (21.3) | 228 (23.4) | |
| 131.25 < cDDD | 813 (20.9) | 252 (25.9) | |
| Traditional NSAIDs, n (%) | 2974 (76.3) | 815 (83.7) | <0.001 |
| Traditional NSAIDs, cDDD | 33.5 ± 58.0 | 42.3 ± 68.2 | <0.001 |
| None | 922 (23.7) | 159 (16.3) | <0.001 |
| 0 < cDDD ≤ 7.75 | 768 (19.7) | 188 (19.3) | |
| 7.75 < cDDD ≤ 21 | 759 (19.5) | 209 (21.5) | |
| 21 < cDDD ≤ 56.17 | 726 (18.6) | 192 (19.7) | |
| 56.17 < cDDD | 721 (18.5) | 226 (23.2) | |
| Selective COX-2 inhibitors, n (%) | 1014 (26.0) | 313 (32.1) | <0.001 |
| Selective COX-2 inhibitors, cDDD | 26.6 ± 75.3 | 32.9 ± 80.2 | 0.028 |
| None | 2882 (74.0) | 661 (67.9) | 0.005 |
| 0 < cDDD ≤ 28 | 327 (8.4) | 104 (10.7) | |
| 28 < cDDD ≤ 56 | 185 (4.7) | 56 (5.7) | |
| 56 < cDDD ≤ 132 | 250 (6.4) | 74 (7.6) | |
| 132 < cDDD | 252 (6.5) | 79 (8.1) | |
| Preferential COX-2 inhibitors, n (%) | 1339 (34.4) | 355 (36.4) | 0.223 |
| Preferential COX-2 inhibitors, cDDD | 19.6 ± 48.3 | 22.3 ± 52.3 | 0.142 |
| None | 2557 (65.6) | 619 (63.6) | 0.645 |
| 0 < cDDD ≤ 14 | 390 (10.0) | 99 (10.2) | |
| 14 < cDDD ≤ 30 | 284 (7.3) | 80 (8.2) | |
| 30 < cDDD ≤ 77 | 343 (8.8) | 85 (8.7) | |
| 77 < cDDD | 322 (8.3) | 91 (9.3) |
| Univariable Analysis | Multivariable Analysis (Model 1—Adjustment of NSAIDs in General) | Multivariable Analysis (Model 2—Adjustment of Three NSAIDs Categories) | ||||
|---|---|---|---|---|---|---|
| Independent Variable: MACE | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p |
| Urbanisation | ||||||
| Urban | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| Suburban | 1.09 (0.92–1.30) | 0.315 | 1.22 (0.98–1.52) | 0.076 | 1.22 (0.98–1.52) | 0.082 |
| Rural | 1.13 (0.93–1.36) | 0.218 | 1.32 (1.03–1.69) | 0.026 | 1.32 (1.03–1.69) | 0.028 |
| Low income 1 | 1.17 (1.01–1.35) | 0.041 | 1.14 (0.94–1.38) | 0.177 | 1.13 (0.94–1.37) | 0.206 |
| Comorbidities | ||||||
| Hypertension | 5.42 (4.58–6.43) | <0.001 | 3.12 (2.57–3.80) | <0.001 | 3.12 (2.57–3.80) | <0.001 |
| Hyperlipidaemia | 7.45 (6.31–8.78) | <0.001 | 4.93 (4.09–5.95) | <0.001 | 5.00 (4.14–6.03) | <0.001 |
| Diabetes mellitus | 3.63 (3.07–4.29) | <0.001 | 1.71 (1.39–2.09) | <0.001 | 1.69 (1.37–2.07) | <0.001 |
| Chronic kidney disease | 4.29 (3.19–5.77) | <0.001 | 1.97 (1.34–2.88) | 0.001 | 1.98 (1.35–2.90) | 0.001 |
| Heart failure | 6.77 (4.98–9.20) | <0.001 | 4.04 (2.74–5.94) | <0.001 | 4.04 (2.74–5.94) | <0.001 |
| Valvular heart disease | 3.91 (2.78–5.50) | <0.001 | 2.10 (1.36–3.26) | 0.001 | 2.06 (1.33–3.20) | 0.001 |
| COPD | 1.47 (1.16–1.84) | 0.001 | 0.92 (0.68–1.23) | 0.565 | 0.92 (0.68–1.23) | 0.563 |
| Extra-articular manifestations | ||||||
| Acute anterior uveitis | 1.00 (0.77–1.29) | 0.979 | 1.03 (0.74–1.44) | 0.849 | 1.01 (0.73–1.41) | 0.952 |
| Psoriasis | 1.10 (0.70–1.74) | 0.669 | 1.10 (0.61–1.98) | 0.750 | 1.13 (0.62–2.04) | 0.694 |
| Inflammatory bowel disease | 0.70 (0.24–2.01) | 0.503 | 0.82 (0.23–2.95) | 0.757 | 0.77 (0.21–2.83) | 0.694 |
| Biologics | 0.80 (0.36–1.80) | 0.590 | 0.41 (0.14–1.20) | 0.103 | 0.37 (0.13–1.11) | 0.076 |
| Methotrexate | 0.86 (0.57–1.28) | 0.454 | 0.72 (0.42–1.26) | 0.250 | 0.70 (0.40–1.22) | 0.204 |
| Sulfasalazine | 0.97 (0.80–1.18) | 0.750 | 0.93 (0.72–1.19) | 0.553 | 0.87 (0.67–1.12) | 0.278 |
| Steroid | ||||||
| None | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| <5 mg/day | 1.45 (1.23–1.70) | <0.001 | 1.29 (1.06–1.58) | 0.013 | 1.25 (1.02–1.54) | 0.028 |
| ≥5 mg/day | 4.80 (3.81–6.06) | <0.001 | 4.85 (3.58–6.55) | <0.001 | 4.75 (3.51–6.43) | <0.001 |
| NSAIDs | 1.67 (1.31–2.13) | <0.001 | 1.27 (0.94–1.71) | 0.118 | ||
| Traditional NSAIDs | 1.61 (1.34–1.95) | <0.001 | 1.29 (1.02–1.63) | 0.031 | ||
| Selective COX-2 inhibitors | 1.37 (1.17–1.60) | <0.001 | 1.38 (1.13–1.69) | 0.002 | ||
| Preferential COX-2 inhibitors | 1.11 (0.95–1.29) | 0.198 | 0.91 (0.75–1.10) | 0.320 | ||
| Univariable Analysis | Multivariable Analysis (Model 1—Adjustment of NSAIDs in General) | Multivariable Analysis (Model 2—Adjustment of Three NSAIDs Categories) | ||||
|---|---|---|---|---|---|---|
| Independent Variable: MACE | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p |
| NSAIDs | 1.67 (1.31–2.13) | <0.001 | ||||
| None | 1 (Reference) | 1 (Reference) | ||||
| 0 < cDDD ≤ 18.75 | 1.56 (1.18–2.05) | 0.002 | 1.33 (0.96–1.85) | 0.090 | ||
| 18.75 < cDDD ≤ 56 | 1.44 (1.09–1.91) | 0.011 | 1.13 (0.81–1.58) | 0.480 | ||
| 56 < cDDD ≤ 131.25 | 1.77 (1.34–2.34) | <0.001 | 1.25 (0.89–1.76) | 0.199 | ||
| 131.25 < cDDD | 2.00 (1.52–2.64) | <0.001 | 1.38 (0.97–1.95) | 0.072 | ||
| Traditional NSAIDs | 1.61 (1.34–1.95) | <0.001 | ||||
| None | 1 (Reference) | 1 (Reference) | ||||
| 0 < cDDD ≤ 7.75 | 1.43 (1.13–1.80) | 0.003 | 1.28 (0.96–1.70) | 0.095 | ||
| 7.75 < cDDD ≤ 21 | 1.63 (1.29–2.05) | <0.001 | 1.39 (1.05–1.85) | 0.023 | ||
| 21 < cDDD ≤ 56.17 | 1.57 (1.24–1.99) | <0.001 | 1.25 (0.93–1.67) | 0.140 | ||
| 56.17 < cDDD | 1.87 (1.49–2.36) | <0.001 | 1.28 (0.96–1.72) | 0.095 | ||
| Selective COX-2 inhibitors | 1.37 (1.17–1.60) | <0.001 | ||||
| None | 1 (Reference) | 1 (Reference) | ||||
| 0< cDDD ≤ 28 | 1.41 (1.11–1.80) | 0.005 | 1.37 (1.02–1.85) | 0.036 | ||
| 28 < cDDD ≤ 56 | 1.34 (0.98–1.83) | 0.064 | 1.43 (0.96–2.12) | 0.077 | ||
| 56 < cDDD ≤ 132 | 1.32 (0.99–1.73) | 0.051 | 1.20 (0.85–1.71) | 0.300 | ||
| 132 < cDDD | 1.38 (1.06–1.81) | 0.019 | 1.61 (1.12–2.32) | 0.011 | ||
| Preferential COX-2 inhibitors | 1.11 (0.95–1.29) | 0.198 | ||||
| None | 1 (Reference) | 1 (Reference) | ||||
| 0 < cDDD ≤ 14 | 1.06 (0.83–1.35) | 0.654 | 0.83 (0.62–1.11) | 0.213 | ||
| 14 < cDDD ≤ 30 | 1.17 (0.90–1.53) | 0.237 | 1.00 (0.71–1.40) | 0.996 | ||
| 30 < cDDD ≤ 77 | 1.04 (0.80–1.35) | 0.778 | 0.88 (0.64–1.22) | 0.445 | ||
| 77 < cDDD | 1.18 (0.92–1.53) | 0.198 | 0.98 (0.71–1.35) | 0.899 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, C.-M.; Wang, J.-S.; Ho, W.-L.; Ko, T.-M.; Chen, H.-M.; Lin, C.-H.; Huang, W.-N.; Chen, Y.-H.; Chen, H.-H. Factors Associated with the Risk of Major Adverse Cardiovascular Events in Patients with Ankylosing Spondylitis: A Nationwide, Population-Based Case—Control Study. Int. J. Environ. Res. Public Health 2022, 19, 4098. https://doi.org/10.3390/ijerph19074098
Kao C-M, Wang J-S, Ho W-L, Ko T-M, Chen H-M, Lin C-H, Huang W-N, Chen Y-H, Chen H-H. Factors Associated with the Risk of Major Adverse Cardiovascular Events in Patients with Ankylosing Spondylitis: A Nationwide, Population-Based Case—Control Study. International Journal of Environmental Research and Public Health. 2022; 19(7):4098. https://doi.org/10.3390/ijerph19074098
Chicago/Turabian StyleKao, Chung-Mao, Jun-Sing Wang, Wei-Li Ho, Tai-Ming Ko, Hsian-Min Chen, Ching-Heng Lin, Wen-Nan Huang, Yi-Hsing Chen, and Hsin-Hua Chen. 2022. "Factors Associated with the Risk of Major Adverse Cardiovascular Events in Patients with Ankylosing Spondylitis: A Nationwide, Population-Based Case—Control Study" International Journal of Environmental Research and Public Health 19, no. 7: 4098. https://doi.org/10.3390/ijerph19074098
APA StyleKao, C. -M., Wang, J. -S., Ho, W. -L., Ko, T. -M., Chen, H. -M., Lin, C. -H., Huang, W. -N., Chen, Y. -H., & Chen, H. -H. (2022). Factors Associated with the Risk of Major Adverse Cardiovascular Events in Patients with Ankylosing Spondylitis: A Nationwide, Population-Based Case—Control Study. International Journal of Environmental Research and Public Health, 19(7), 4098. https://doi.org/10.3390/ijerph19074098