
Sex-Specific Differences in Lower Body Fat Distribution and Association with Physical Performance among Healthy Community-Dwelling Older Adults: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Dual-Energy X-ray Absorptiometry
2.3. Magnetic Resonance Imaging
2.4. Proton Magnetic Resonance Spectroscopy
2.5. Muscle Strength and Physical Performance Measurement
2.6. Anthropometric Measurements
2.7. Blood Biochemical Analysis
2.8. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Subjects
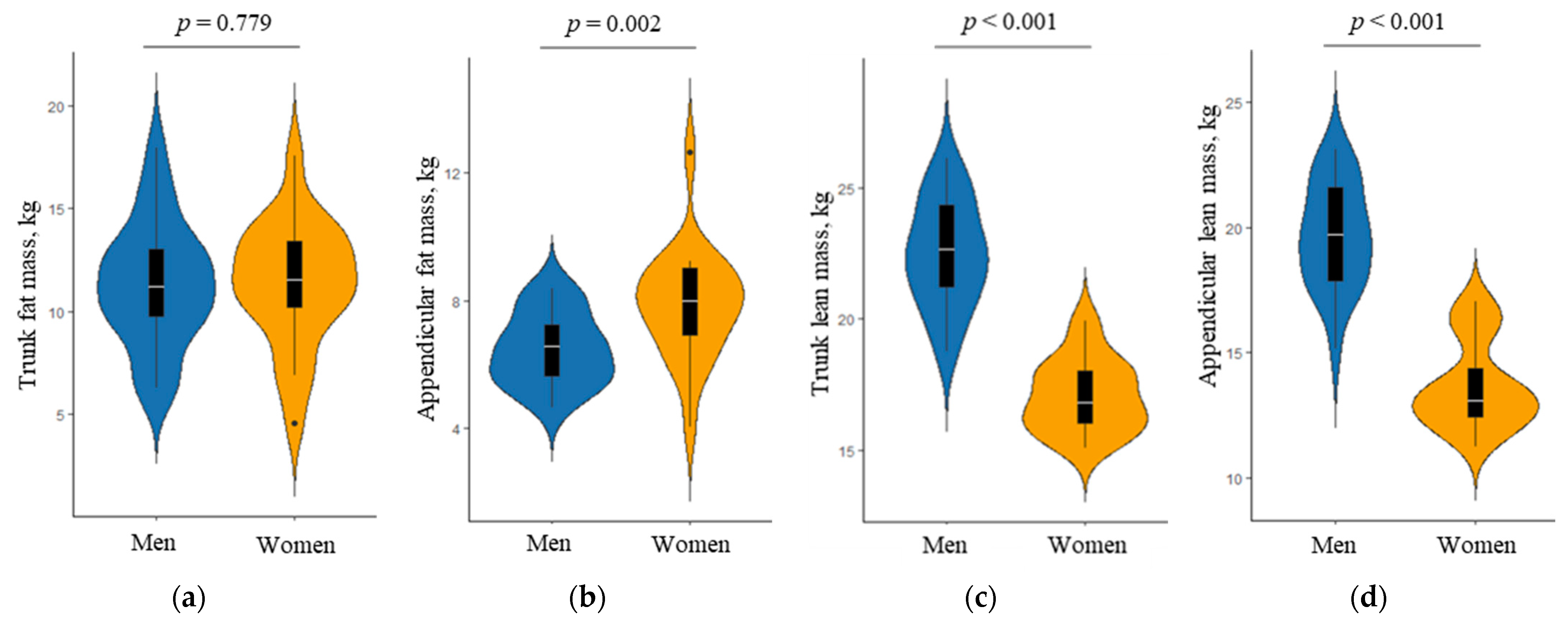
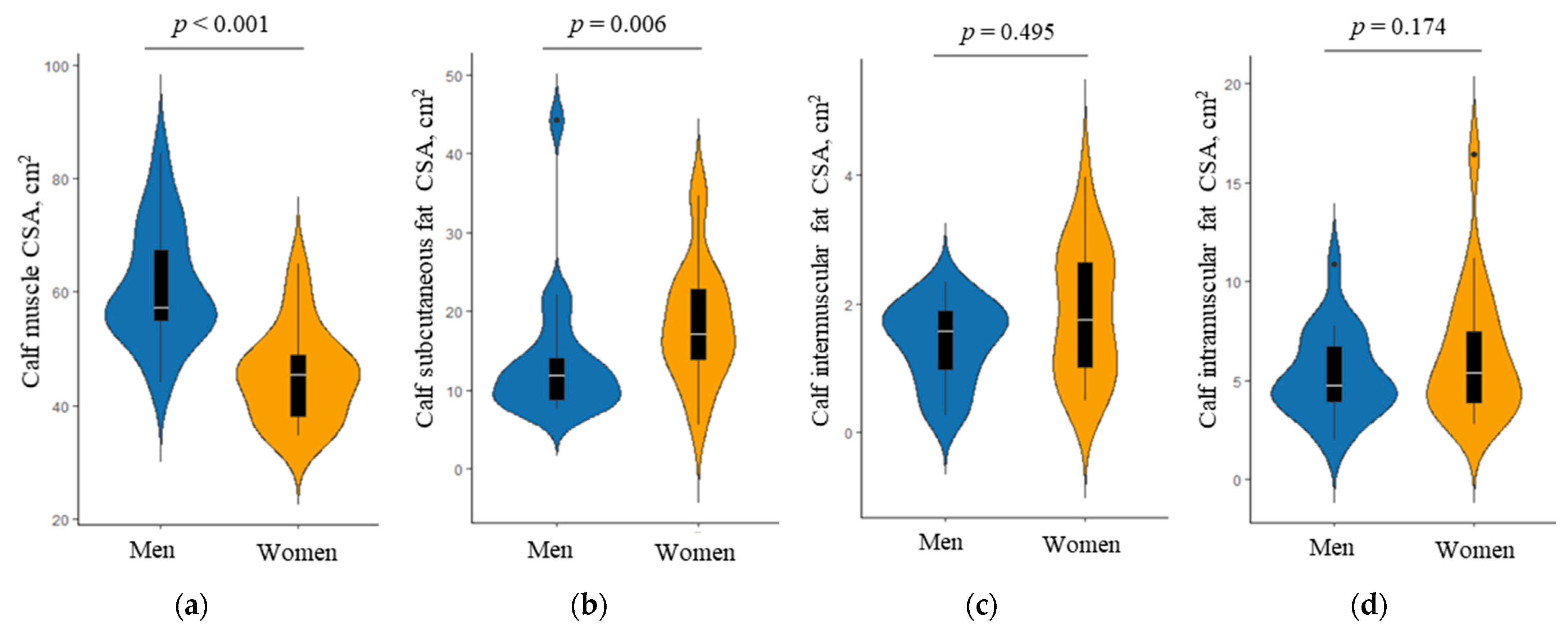
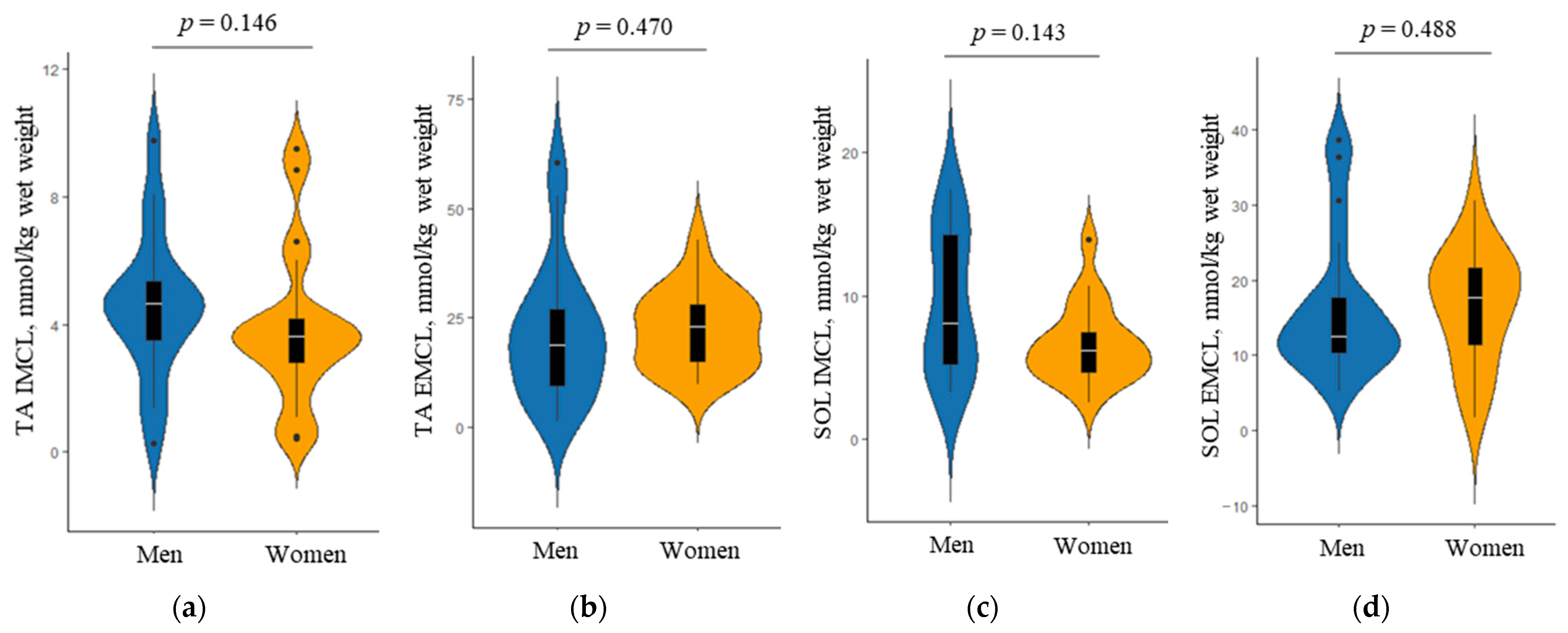
3.2. Sex-Specific Differences in Body Composition
3.3. Differences in the Association of Body Composition with Physical Performance between Men and Women
4. Discussion
5. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Studenski, S.; Perera, S.; Wallace, D.; Chandler, J.M.; Duncan, P.W.; Rooney, E.; Fox, M.; Guralnik, J.M. Physical performance measures in the clinical setting. J. Am. Geriatr. Soc. 2003, 51, 314–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Musich, S.; Wang, S.S.; Ruiz, J.; Hawkins, K.; Wicker, E. The impact of mobility limitations on health outcomes among older adults. Geriatr. Nurs. 2018, 39, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Pua, Y.H.; Matchar, D.B. Physical Performance Predictor Measures in Older Adults with Falls-Related Emergency Department Visits. J. Am. Med. Dir. Assoc. 2019, 20, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Choo, P.L.; Tou, N.X.; Jun Pang, B.W.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Chen, K.K.; Ng, T.P.; Wee, S.L. Timed Up and Go (TUG) Reference Values and Predictive Cutoffs for Fall Risk and Disability in Singaporean Community-Dwelling Adults: Yishun Cross-Sectional Study and Singapore Longitudinal Aging Study. J. Am. Med. Dir. Assoc. 2021, 22, 1640–1645. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Cawthon, P.M.; Stone, K.L.; Hillier, T.A.; Cauley, J.A.; Hochberg, M.C.; Rodondi, N.; et al. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch. Intern. Med. 2008, 168, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Ahmed, T.; Vafaei, A.; Auais, M.; Guralnik, J.; Zunzunegui, M.V. Gender Roles and Physical Function in Older Adults: Cross-Sectional Analysis of the International Mobility in Aging Study (IMIAS). PLoS ONE 2016, 11, e0156828. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Pérez-Sousa, M.A.; Venegas-Sanabria, L.C.; Cano-Gutierrez, C.A.; Hernández-Quiñonez, P.A.; Rincón-Pabón, D.; García-Hermoso, A.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Izquierdo, M. Normative Values for the Short Physical Performance Battery (SPPB) and Their Association With Anthropometric Variables in Older Colombian Adults. The SABE Study, 2015. Front. Med. 2020, 7, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tessier, A.J.; Wing, S.S.; Rahme, E.; Morais, J.A.; Chevalier, S. Physical function-derived cut-points for the diagnosis of sarcopenia and dynapenia from the Canadian longitudinal study on aging. J. Cachexia Sarcopenia Muscle 2019, 10, 985–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Won, C.W. Prevalence of sarcopenia in community-dwelling older adults using the definition of the European Working Group on Sarcopenia in Older People 2: Findings from the Korean Frailty and Aging Cohort Study. Age Ageing 2019, 48, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Shinkai, S.; Fujiwara, Y.; Obuchi, S.; Yoshida, H.; Hirano, H.; Kim, H.K.; Ishizaki, T.; Takahashi, R.; Group, T.-L.R. Reference values and age and sex differences in physical performance measures for community-dwelling older Japanese: A pooled analysis of six cohort studies. PLoS ONE 2014, 9, e99487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, F.; Cohen, S.A.; Greaney, M.L.; Earp, J.E.; Delmonico, M.J. Longitudinal Sex-Specific Physical Function Trends by Age, Race/Ethnicity, and Weight Status. J. Am. Geriatr. Soc. 2020, 68, 2270–2278. [Google Scholar] [CrossRef]
- Reinders, I.; Murphy, R.A.; Koster, A.; Brouwer, I.A.; Visser, M.; Garcia, M.E.; Launer, L.J.; Siggeirsdottir, K.; Eiriksdottir, G.; Jonsson, P.V.; et al. Muscle Quality and Muscle Fat Infiltration in Relation to Incident Mobility Disability and Gait Speed Decline: The Age, Gene/Environment Susceptibility-Reykjavik Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 1030–1036. [Google Scholar] [CrossRef] [Green Version]
- Tseng, L.A.; Delmonico, M.J.; Visser, M.; Boudreau, R.M.; Goodpaster, B.H.; Schwartz, A.V.; Simonsick, E.M.; Satterfield, S.; Harris, T.; Newman, A.B. Body composition explains sex differential in physical performance among older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Visser, M.; Kritchevsky, S.B.; Goodpaster, B.H.; Newman, A.B.; Nevitt, M.; Stamm, E.; Harris, T.B. Leg muscle mass and composition in relation to lower extremity performance in men and women aged 70 to 79: The health, aging and body composition study. J. Am. Geriatr. Soc. 2002, 50, 897–904. [Google Scholar] [CrossRef]
- Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.; Newman, A.B.; Nevitt, M.; Rubin, S.M.; Simonsick, E.M.; Harris, T.B. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 324–333. [Google Scholar] [CrossRef]
- Sood, A. Sex differences: Implications for the obesity-asthma association. Exerc. Sport Sci. Rev. 2011, 39, 48–56. [Google Scholar] [CrossRef]
- Perseghin, G.; Scifo, P.; Pagliato, E.; Battezzati, A.; Benedini, S.; Soldini, L.; Testolin, G.; Del Maschio, A.; Luzi, L. Gender factors affect fatty acids-induced insulin resistance in nonobese humans: Effects of oral steroidal contraception. J. Clin. Endocrinol. Metab. 2001, 86, 3188–3196. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.H.; Pan, J.W.; Heydari, S.; Hetherington, H.P.; Stein, D.T. Regional differences in intramyocellular lipids in humans observed by in vivo 1H-MR spectroscopic imaging. J. Appl. Physiol. 2001, 90, 1267–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boesch, C.; Slotboom, J.; Hoppeler, H.; Kreis, R. In vivo determination of intra-myocellular lipids in human muscle by means of localized 1H-MR-spectroscopy. Magn. Reson. Med. 1997, 37, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-based differences in skeletal muscle kinetics and fiber-type composition. Physiology 2015, 30, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, S.; Reggiani, C. Fiber types in mammalian skeletal muscles. Physiol. Rev. 2011, 91, 1447–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punkt, K.; Mehlhorn, H.; Hilbig, H. Region- and age-dependent variations of muscle fibre properties. Acta Histochem. 1998, 100, 37–58. [Google Scholar] [CrossRef]
- Fournier, G.; Bernard, C.; Cievet-Bonfils, M.; Kenney, R.; Pingon, M.; Sappey-Marinier, E.; Chazaud, B.; Gondin, J.; Servien, E. Sex differences in semitendinosus muscle fiber-type composition. Scand. J. Med. Sci. Sports 2022, 32, 720–727. [Google Scholar] [CrossRef]
- Straight, C.R.; Voigt, T.B.; Jala, A.V.; Chase, J.D.; Ringham, O.R.; Ades, P.A.; Toth, M.J.; Miller, M.S. Quadriceps Lipid Content Has Sex-Specific Associations With Whole-Muscle, Cellular, and Molecular Contractile Function in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 1879–1886. [Google Scholar] [CrossRef]
- Won, C.W.; Lee, S.; Kim, J.; Chon, D.; Kim, S.; Kim, C.O.; Kim, M.K.; Cho, B.; Choi, K.M.; Roh, E.; et al. Korean frailty and aging cohort study (KFACS): Cohort profile. BMJ Open 2020, 10, e035573. [Google Scholar] [CrossRef] [Green Version]
- Cree, M.G.; Newcomer, B.R.; Katsanos, C.S.; Sheffield-Moore, M.; Chinkes, D.; Aarsland, A.; Urban, R.; Wolfe, R.R. Intramuscular and Liver Triglycerides Are Increased in the Elderly. J. Clin. Endocrinol. Metab. 2004, 89, 3864–3871. [Google Scholar] [CrossRef]
- Hioki, M.; Kanehira, N.; Koike, T.; Saito, A.; Takahashi, H.; Shimaoka, K.; Sakakibara, H.; Oshida, Y.; Akima, H. Associations of intramyocellular lipid in vastus lateralis and biceps femoris with blood free fatty acid and muscle strength differ between young and elderly adults. Clin. Physiol. Funct. Imaging 2016, 36, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, L.S.; Fabian, J.; Rospleszcz, S.; Lorbeer, R.; Machann, J.; Kraus, M.S.; Roemer, F.; Rathmann, W.; Meisinger, C.; Heier, M.; et al. Distribution patterns of intramyocellular and extramyocellular fat by magnetic resonance imaging in subjects with diabetes, prediabetes and normoglycaemic controls. Diabetes Obes. Metab. 2021, 23, 1868–1878. [Google Scholar] [CrossRef] [PubMed]
- White, L.J.; Ferguson, M.A.; McCoy, S.C.; Kim, H.W.; Castellano, V. Cardiovascular/non-insulin-dependent diabetes mellitus risk factors and intramyocellular lipid in healthy subjects: A sex comparison. Metabolism 2006, 55, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Schorr, M.; Dichtel, L.E.; Gerweck, A.V.; Valera, R.D.; Torriani, M.; Miller, K.K.; Bredella, M.A. Sex differences in body composition and association with cardiometabolic risk. Biol. Sex Differ. 2018, 9, 28. [Google Scholar] [CrossRef]
- Pritchard, J.M.; Karampatos, S.; Beattie, K.A.; Giangregorio, L.M.; Ioannidis, G.; Atkinson, S.A.; Thabane, L.; Gerstein, H.; Punthakee, Z.; Adachi, J.D.; et al. The Relationship between Intramuscular Adipose Tissue, Functional Mobility, and Strength in Postmenopausal Women with and without Type 2 Diabetes. J. Aging Res. 2015, 2015, 872726. [Google Scholar] [CrossRef]
- Isobe, T.; Okamoto, Y.; Hirano, Y.; Ando, H.; Takada, K.; Sato, E.; Shinoda, K.; Tadano, K.; Takei, H.; Kamizawa, S.; et al. Effect of biological factors on successful measurements with skeletal-muscle (1)H-MRS. Ther. Clin. Risk Manag. 2016, 12, 1133–1137. [Google Scholar] [CrossRef] [Green Version]
- Weis, J.; Johansson, L.; Ortiz-Nieto, F.; Ahlström, H. Assessment of lipids in skeletal muscle by LCModel and AMARES. J. Magn. Reson. Imaging 2009, 30, 1124–1129. [Google Scholar] [CrossRef]
- Kim, M.; Won, C.W.; Kim, M. Muscular grip strength normative values for a Korean population from the Korea National Health and Nutrition Examination Survey, 2014–2015. PLoS ONE 2018, 13, e0201275. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Coen, P.M.; Goodpaster, B.H. Role of intramyocelluar lipids in human health. Trends Endocrino.l Metab. 2012, 23, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkland, J.L.; Tchkonia, T.; Pirtskhalava, T.; Han, J.; Karagiannides, I. Adipogenesis and aging: Does aging make fat go MAD? Exp. Gerontol. 2002, 37, 757–767. [Google Scholar] [CrossRef]
- Sepe, A.; Tchkonia, T.; Thomou, T.; Zamboni, M.; Kirkland, J.L. Aging and Regional Differences in Fat Cell Progenitors—A Mini-Review. Gerontology 2011, 57, 66–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perseghin, G.; Scifo, P.; De Cobelli, F.; Pagliato, E.; Battezzati, A.; Arcelloni, C.; Vanzulli, A.; Testolin, G.; Pozza, G.; Del Maschio, A.; et al. Intramyocellular triglyceride content is a determinant of in vivo insulin resistance in humans: A 1H-13C nuclear magnetic resonance spectroscopy assessment in offspring of type 2 diabetic parents. Diabetes 1999, 48, 1600–1606. [Google Scholar] [CrossRef]
- Petersen, K.F.; Befroy, D.; Dufour, S.; Dziura, J.; Ariyan, C.; Rothman, D.L.; DiPietro, L.; Cline, G.W.; Shulman, G.I. Mitochondrial dysfunction in the elderly: Possible role in insulin resistance. Science 2003, 300, 1140–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crane, J.D.; Devries, M.C.; Safdar, A.; Hamadeh, M.J.; Tarnopolsky, M.A. The effect of aging on human skeletal muscle mitochondrial and intramyocellular lipid ultrastructure. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65, 119–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Distefano, G.; Standley, R.A.; Zhang, X.; Carnero, E.A.; Yi, F.; Cornnell, H.H.; Coen, P.M. Physical activity unveils the relationship between mitochondrial energetics, muscle quality, and physical function in older adults. J. Cachexia Sarcopenia Muscle 2018, 9, 279–294. [Google Scholar] [CrossRef] [Green Version]
- Edgerton, V.R.; Smith, J.L.; Simpson, D.R. Muscle fibre type populations of human leg muscles. Histochem. J. 1975, 7, 259–266. [Google Scholar] [CrossRef]
- De Stefano, M.A.; Ambrosio, R.; Porcelli, T.; Orlandino, G.; Salvatore, D.; Luongo, C. Thyroid Hormone Action in Muscle Atrophy. Metabolites 2021, 11, 730. [Google Scholar] [CrossRef]
- Bloise, F.F.; Cordeiro, A.; Ortiga-Carvalho, T.M. Role of thyroid hormone in skeletal muscle physiology. J. Endocrinol. 2018, 236, R57–R68. [Google Scholar] [CrossRef]
- McKeran, R.O.; Slavin, G.; Andrews, T.M.; Ward, P.; Mair, W.G. Muscle fibre type changes in hypothyroid myopathy. J. Clin. Pathol. 1975, 28, 659–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.S.; Yen, P.M.; Chin, W.W.; Pfaff, D.W. Estrogen and thyroid hormone interaction on regulation of gene expression. Proc. Natl. Acad. Sci. USA 1996, 93, 12587–12592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, R.; Wen, C.; Li, J.; Harris, M.B.; Liu, Y.Y.; Kuo, C.H. Lipid storage changes in human skeletal muscle during detraining. Front. Physiol. 2015, 6, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brechtel, K.; Niess, A.M.; Machann, J.; Rett, K.; Schick, F.; Claussen, C.D.; Dickhuth, H.H.; Haering, H.U.; Jacob, S. Utilisation of intramyocellular lipids (IMCLs) during exercise as assessed by proton magnetic resonance spectroscopy (1H-MRS). Horm. Metab. Res. 2001, 33, 63–66. [Google Scholar] [CrossRef]
- Frayn, K.N.; Karpe, F. Regulation of human subcutaneous adipose tissue blood flow. Int. J. Obes. 2014, 38, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Newton, C.J.; Samuel, D.L.; James, V.H. Aromatase activity and concentrations of cortisol, progesterone and testosterone in breast and abdominal adipose tissue. J. Steroid Biochem. 1986, 24, 1033–1039. [Google Scholar] [CrossRef]
- Szymczak, J.; Milewicz, A.; Thijssen, J.H.; Blankenstein, M.A.; Daroszewski, J. Concentration of sex steroids in adipose tissue after menopause. Steroids 1998, 63, 319–321. [Google Scholar] [CrossRef]
- Manolopoulos, K.N.; Karpe, F.; Frayn, K.N. Gluteofemoral body fat as a determinant of metabolic health. Int. J. Obes. 2010, 34, 949–959. [Google Scholar] [CrossRef] [Green Version]
- Hiol, A.N.; von Hurst, P.R.; Conlon, C.A.; Mugridge, O.; Beck, K.L. Body composition associations with muscle strength in older adults living in Auckland, New Zealand. PLoS ONE 2021, 16, e0250439. [Google Scholar] [CrossRef]
- Patiño-Villada, F.A.; González-Bernal, J.J.; González-Santos, J.; de Paz, J.A.; Jahouh, M.; Mielgo-Ayuso, J.; Romero-Pérez, E.M.; Soto-Cámara, R. Relationship of Body Composition with the Strength and Functional Capacity of People over 70 Years. Int. J. Environ. Res. Public Health 2020, 17, 7767. [Google Scholar] [CrossRef]
- Kim, S.; Leng, X.I.; Kritchevsky, S.B. Body Composition and Physical Function in Older Adults with Various Comorbidities. Innov. Aging 2017, 1, igx008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Lebon, J.; Barsalani, R.; Payette, H.; Brochu, M.; Dionne, I.J. Inflammation and Fat Mass as Determinants of Changes in Physical Capacity and Mobility in Older Adults Displaying A Large Variability in Body Composition: The NuAge Study. Exp. Aging Res. 2016, 42, 403–417. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Harris, T.B.; Langlois, J.; Hannan, M.T.; Roubenoff, R.; Felson, D.T.; Wilson, P.W.; Kiel, D.P. Body fat and skeletal muscle mass in relation to physical disability in very old men and women of the Framingham Heart Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1998, 53, M214–M221. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Men | Women | p Value | ||
|---|---|---|---|---|---|
| n = 20 | n = 20 | ||||
| Clinical characteristics | |||||
| Age, years | 78.0 | [76.0–80.4] | 76.6 | [72.7–78.5] | 0.072 |
| Height, cm | 163.3 | [161.6–165.0] | 150.3 | [147.6–155.0] | 0.000 |
| Weight, kg | 65.2 | [62.0–75.0] | 54.7 | [51.6–64.6] | 0.000 |
| Body mass index, kg/m2 | 24.1 | [22.9–27.2] | 24.2 | [21.9–28.0] | 0.841 |
| Waist circumference, cm | 86.0 | [82.5–91.5] | 79.0 | [75.0–84.4] | 0.005 |
| Hip circumference, cm | 91.0 | [88.8–95.7] | 90.5 | [87.9–92.4] | 0.414 |
| Waist-to-hip ratio | 0.94 | [0.91–0.98] | 0.89 | [0.83–0.93] | 0.002 |
| Thigh circumference, cm | 44.5 | [42.3–48.7] | 43.0 | [41.1–45.8] | 0.121 |
| Calf circumference, cm | 34.8 | [32.5–36.0] | 31.8 | [31.0–33.4] | 0.014 |
| Physical activity level (metabolic equivalent, minutes/week) | 2196 | [720–3900] | 940 | [420–2420] | 0.221 |
| Current smokers, % | 1 | (5.0) | 1 | (5.0) | 0.756 |
| Chronic health conditions | |||||
| Hypertension, % | 11 | (55.0) | 16 | (80.0) | 0.088 |
| Lung disease, % | 1 | (5.0) | 3 | (15.0) | 0.302 |
| Biochemical parameters in blood samples | |||||
| Total cholesterol, mg/dL | 165.5 | [154.0–203.0] | 170.0 | [157.5–210.0] | 0.620 |
| High-density lipoprotein cholesterol, mg/dL | 48.5 | [39.3–55.8] | 65.5 | [53.3–79.5] | 0.001 |
| Low-density lipoprotein cholesterol, mg/dL | 104.0 | [98.5–133.8] | 101.0 | [76.0–129.8] | 0.529 |
| Triglyceride, mg/dL | 113.5 | [80.3–183.5] | 101.0 | [86.8–124.5] | 0.341 |
| Fasting glucose, mg/dL | 99.0 | [94.3–103.0] | 106.5 | [93.0–103.0] | 0.495 |
| Fasting insulin, uU/mL | 7.7 | [4.4–12.8] | 7.0 | [5.9–9.3] | 0.883 |
| Glycosylated hemoglobin, % | 5.9 | [5.4–6.2] | 5.9 | [5.7–6.1] | 0.529 |
| Creatinine, mg/dL | 0.93 | [0.83–1.03] | 0.69 | [0.64–0.79] | 0.001 |
| Albumin, g/dL | 4.3 | [4.1–4.5] | 4.4 | [4.4–4.5] | 0.040 |
| High-sensitivity C-reactive protein, mg/L | 0.65 | [0.41–2.16] | 0.49 | [0.35–0.87] | 0.270 |
| 25-hydroxy vitamin D, ng/mL | 19.8 | [16.7–27.8] | 15.2 | [12.1–24.6] | 0.134 |
| Physical performance | |||||
| Grip strength, kg | 34.4 | [29.4–35.8] | 19.6 | [18.3–22.5] | 0.001 |
| 4-m usual gait speed, m/s | 1.13 | [1.04–1.28] | 1.11 | [1.01–1.19] | 0.301 |
| Five-times sit-to-stand test, s | 8.17 | [6.88–9.92] | 9.07 | [7.89–10.10] | 0.120 |
| Timed up-and-go test, s | 9.54 | [8.43–10.58] | 9.92 | [9.02–10.58] | 0.134 |
| Short Physical Performance Battery, score | 12.0 | [11.0–12.0] | 11.5 | [10.0–12.0] | 0.242 |
| Variable | Grip Strength, kg | Usual Gait Speed, m/s | Five-Times Sit-to-Stand Test, s | Timed up-and-Go Test, s | SPPB, Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| rs | p Value | rs | p Value | rs | p Value | rs | p Value | rs | p Value | |
| Dual-energy X-ray absorptiometry parameters | ||||||||||
| Whole-body mass measurement | ||||||||||
| Fat mass, kg | −0.245 | 0.298 | 0.003 | 0.990 | 0.259 | 0.271 | 0.126 | 0.596 | −0.004 | 0.988 |
| Lean mass, kg | 0.498 | 0.026 * | 0.194 | 0.412 | −0.165 | 0.486 | −0.212 | 0.369 | 0.056 | 0.815 |
| Percentage of fat mass, % | −0.483 | 0.031 * | −0.100 | 0.675 | 0.269 | 0.251 | 0.192 | 0.416 | −0.030 | 0.901 |
| Segmental body mass measurement | ||||||||||
| Trunk fat mass, kg | −0.310 | 0.184 | −0.019 | 0.937 | 0.248 | 0.292 | 0.167 | 0.482 | 0.017 | 0.944 |
| Appendicular fat mass, kg | −0.146 | 0.539 | 0.111 | 0.642 | 0.081 | 0.734 | −0.072 | 0.762 | −0.097 | 0.684 |
| Right lean fat mass, kg | −0.146 | 0.539 | 0.134 | 0.573 | 0.111 | 0.640 | 0.003 | 0.990 | −0.142 | 0.944 |
| Trunk lean mass kg | 0.418 | 0.067 | 0.230 | 0.390 | −0.263 | 0.262 | −0.173 | 0.466 | 0.073 | 0.760 |
| Appendicular lean mass, kg | 0.586 | 0.007 ** | 0.144 | 0.546 | 0.009 | 0.970 | −0.180 | 0.446 | −0.037 | 0.876 |
| Right leg lean mass, kg | 0.532 | 0.016 * | 0.157 | 0.508 | 0.006 | 0.980 | −0.268 | 0.254 | −0.022 | 0.925 |
| Magnetic resonance imaging parameters | ||||||||||
| Calf muscle CSA, cm2 | 0.417 | 0.068 † | 0.287 | 0.219 | −0.253 | 0.283 | −0.415 | 0.069 † | 0.140 | 0.556 |
| Calf subcutaneous fat CSA, cm2 | −0.313 | 0.179 | 0.002 | 0.992 | 0.036 | 0.880 | 0.023 | 0.925 | −0.095 | 0.690 |
| Calf intermuscular fat CSA, cm2 | −0.041 | 0.865 | 0.337 | 0.146 | −0.553 | 0.011 * | −0.340 | 0.143 | 0.021 | 0.932 |
| Calf intramuscular fat CSA, cm2 | 0.081 | 0.734 | −0.311 | 0.182 | 0.552 | 0.012 * | 0.429 | 0.059 † | −0.500 | 0.025 * |
| Magnetic resonance spectroscopy parameters | ||||||||||
| TA IMCL, mmol/kg wet weight | −0.251 | 0.300 | −0.320 | 0.182 | 0.518 | 0.023 * | 0.367 | 0.123 | −0.168 | 0.492 |
| TA EMCL, mmol/kg wet weight | −0.202 | 0.408 | −0.227 | 0.351 | 0.344 | 0.149 | 0.284 | 0.238 | −0.125 | 0.610 |
| SOL IMCL, mmol/kg wet weight | 0.404 | 0.107 | −0.026 | 0.922 | 0.113 | 0.667 | 0.203 | 0.434 | −0.109 | 0.677 |
| SOL EMCL, mmol/kg wet weight | 0.033 | 0.892 | 0.038 | 0.878 | −0.018 | 0.943 | −0.040 | 0.870 | −0.033 | 0.894 |
| Variable | Grip Strength, kg | Usual Gait Speed, m/s | Five-Times Sit-to-Stand Test, s | Timed up-and-Go Test, s | SPPB, Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| rs | p Value | rs | p Value | rs | p Value | rs | p Value | rs | p Value | |
| Dual-energy X-ray absorptiometry parameters | ||||||||||
| Whole-body mass measurement | ||||||||||
| Fat mass, kg | 0.300 | 0.199 | 0.264 | 0.262 | −0.086 | 0.726 | −0.048 | 0.840 | 0.278 | 0.235 |
| Lean mass, kg | 0.467 | 0.038 * | −0.050 | 0.833 | −0.100 | 0.684 | 0.083 | 0.729 | −0.065 | 0.784 |
| Percentage of fat mass, % | 0.002 | 0.992 | 0.405 | 0.076 † | −0.200 | 0.412 | −0.266 | 0.257 | 0.470 | 0.036 * |
| Segmental body mass measurement | ||||||||||
| Trunk fat mass, kg | 0.163 | 0.493 | 0.178 | 0.452 | −0.019 | 0.937 | 0.045 | 0.850 | 0.180 | 0.447 |
| Appendicular fat mass, kg | 0.371 | 0.107 | 0.276 | 0.238 | −0.296 | 0.218 | −0.343 | 0.139 | 0.500 | 0.025 * |
| Right leg fat mass, kg | 0.437 | 0.054 † | 0.250 | 0.288 | −0.275 | 0.218 | −0.338 | 0.145 | 0.462 | 0.040 * |
| Trunk lean mass, kg | 0.406 | 0.076 † | −0.248 | 0.291 | 0.111 | 0.652 | 0.245 | 0.298 | −0.335 | 0.149 |
| Appendicular lean mass, kg | 0.505 | 0.023 * | 0.166 | 0.485 | −0.267 | 0.270 | −0.048 | 0.840 | 0.190 | 0.423 |
| Right leg lean mass, kg | 0.388 | 0.091 | 0.239 | 0.311 | −0.289 | 0.229 | −0.104 | 0.663 | 0.237 | 0.315 |
| Magnetic resonance imaging parameters | ||||||||||
| Calf muscle CSA, cm2 | 0.267 | 0.255 | −0.194 | 0.412 | −0.046 | 0.853 | 0.141 | 0.552 | 0.091 | 0.704 |
| Calf subcutaneous fat CSA, cm2 | 0.150 | 0.528 | 0.447 | 0.048 * | −0.411 | 0.081 † | −0.394 | 0.086 † | 0.439 | 0.053 † |
| Calf intermuscular fat CSA, cm2 | 0.272 | 0.182 | −0.010 | 0.967 | −0.207 | 0.395 | −0.248 | 0.292 | 0.352 | 0.128 |
| Calf intramuscular fat CSA, cm2 | 0.167 | 0.481 | 0.161 | 0.497 | −0.053 | 0.831 | 0.021 | 0.930 | −0.048 | 0.839 |
| Magnetic resonance spectroscopy parameters | ||||||||||
| TA IMCL, mmol/kg wet weight | 0.264 | 0.276 | 0.001 | 0.997 | −0.044 | 0.861 | −0.039 | 0.875 | −0.022 | 0.929 |
| TA EMCL, mmol/kg wet weight | 0.433 | 0.064 † | −0.068 | 0.783 | 0.100 | 0.693 | 0.072 | 0.770 | −0.192 | 0.431 |
| SOL IMCL, mmol/kg wet weight | 0.160 | 0.525 | 0.231 | 0.356 | 0.132 | 0.613 | 0.472 | 0.048 * | 0.079 | 0.756 |
| SOL EMCL, mmol/kg wet weight | 0.129 | 0.598 | −0.031 | 0.901 | −0.488 | 0.040 * | −0.337 | 0.158 | −0.180 | 0.461 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Oh, J.-H.; Won, C.W. Sex-Specific Differences in Lower Body Fat Distribution and Association with Physical Performance among Healthy Community-Dwelling Older Adults: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 4201. https://doi.org/10.3390/ijerph19074201
Kim M, Oh J-H, Won CW. Sex-Specific Differences in Lower Body Fat Distribution and Association with Physical Performance among Healthy Community-Dwelling Older Adults: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(7):4201. https://doi.org/10.3390/ijerph19074201
Chicago/Turabian StyleKim, Miji, Jang-Hoon Oh, and Chang Won Won. 2022. "Sex-Specific Differences in Lower Body Fat Distribution and Association with Physical Performance among Healthy Community-Dwelling Older Adults: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 7: 4201. https://doi.org/10.3390/ijerph19074201
APA StyleKim, M., Oh, J. -H., & Won, C. W. (2022). Sex-Specific Differences in Lower Body Fat Distribution and Association with Physical Performance among Healthy Community-Dwelling Older Adults: A Pilot Study. International Journal of Environmental Research and Public Health, 19(7), 4201. https://doi.org/10.3390/ijerph19074201