
The Analysis of Patterns of Two COVID-19 Outbreak Clusters in China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Estimation of the Effective Reproduction Number
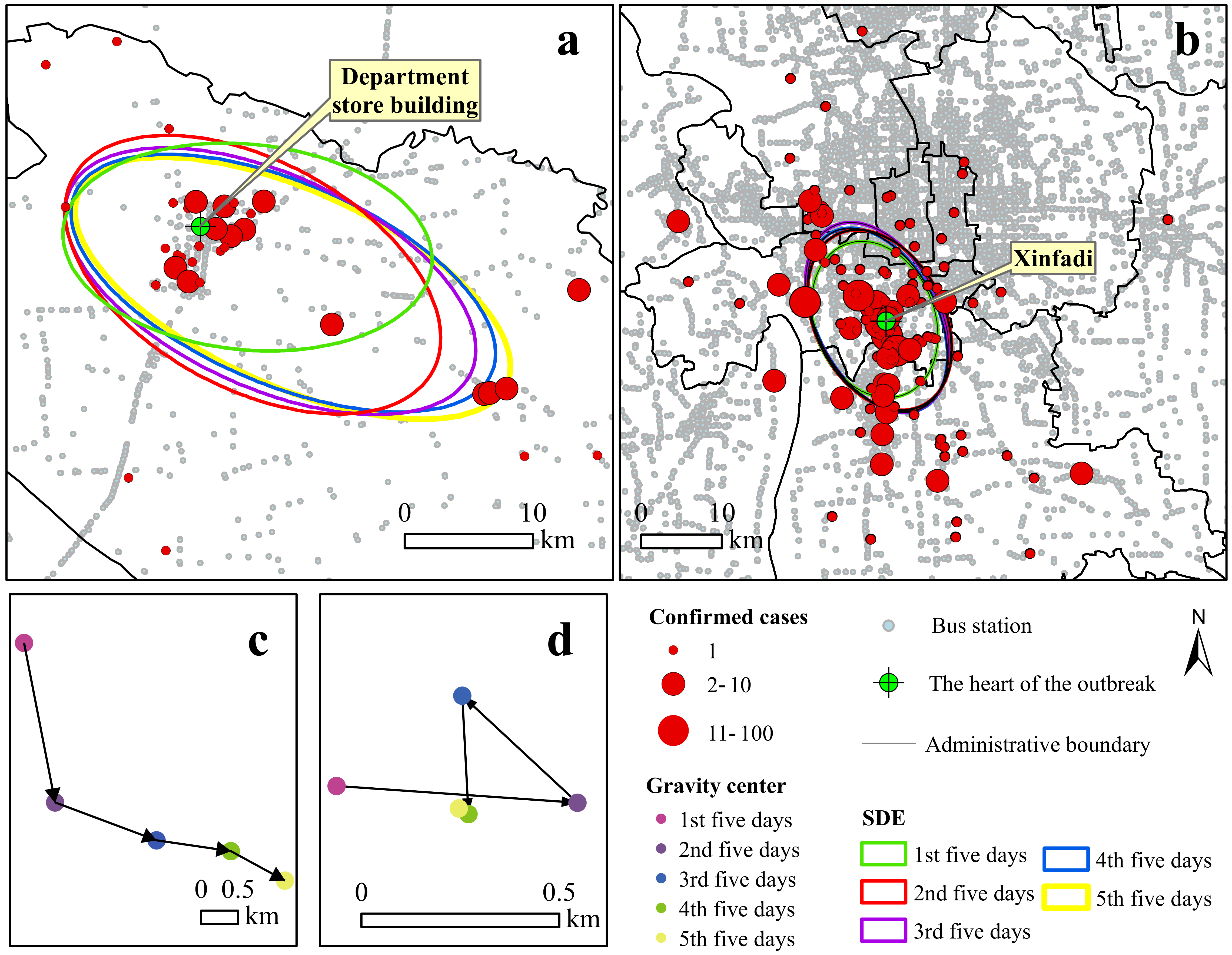
2.3. Spatiotemporal Analysis
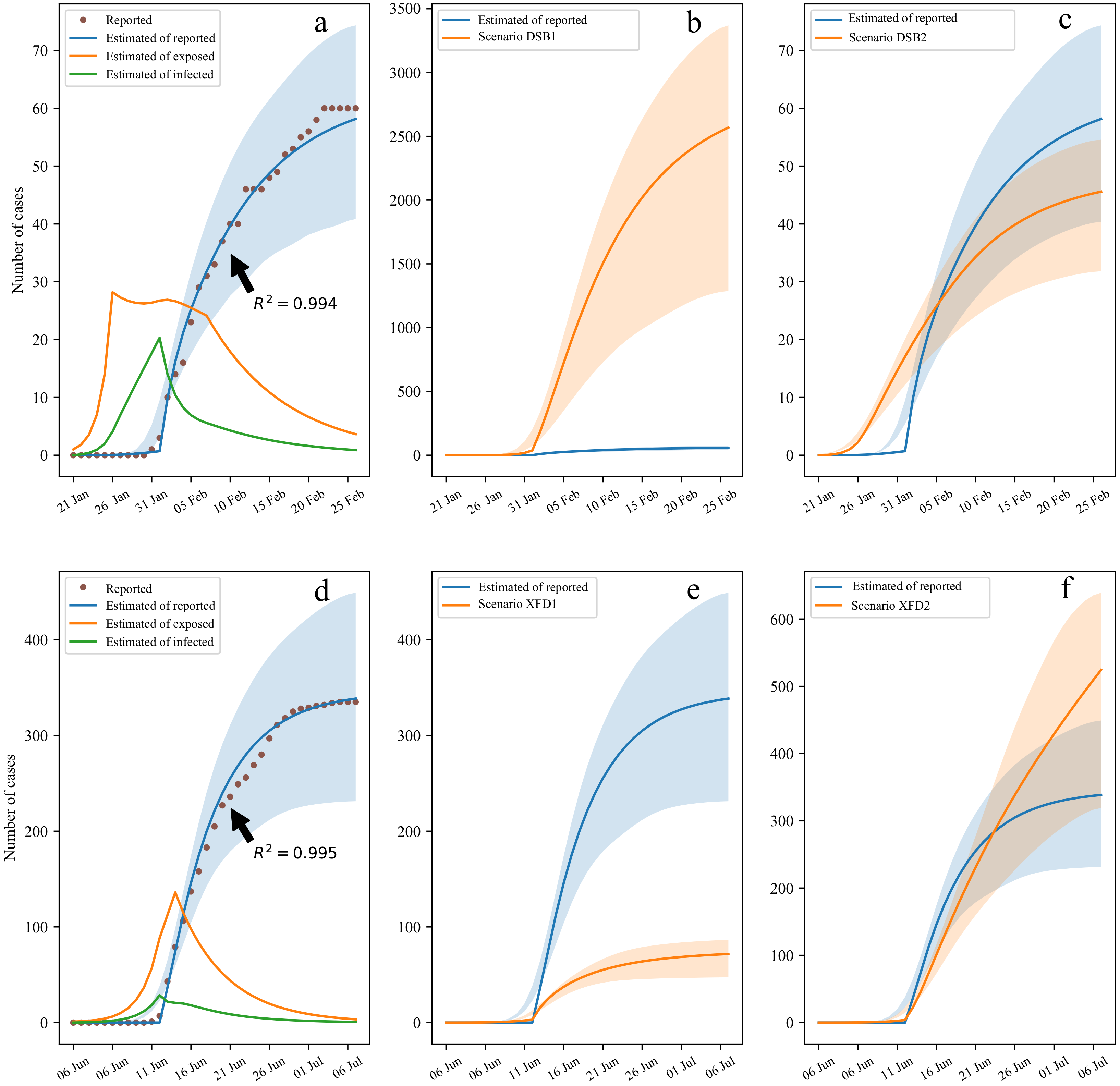
2.4. Modified Dynamic Model
3. Results
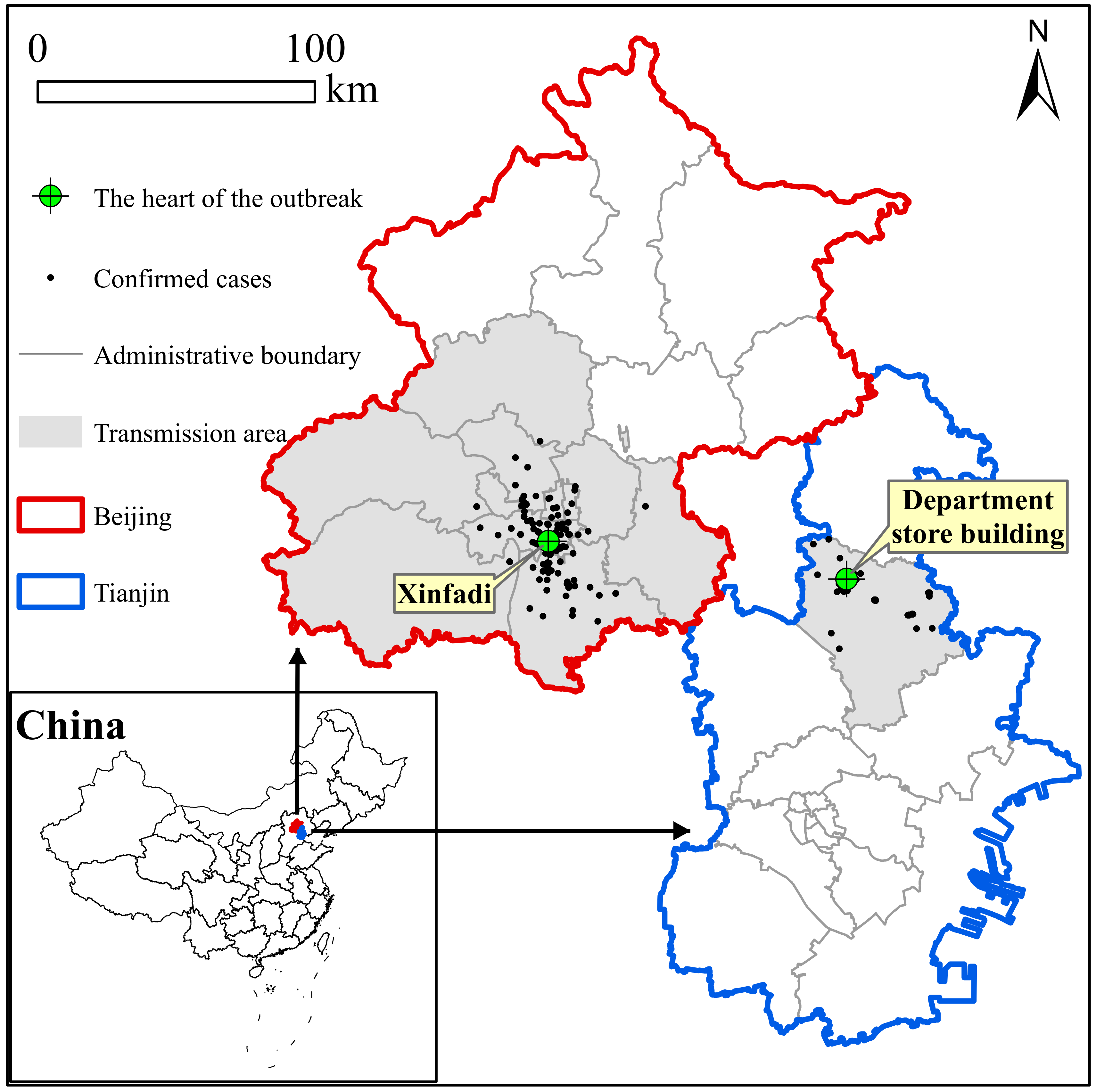
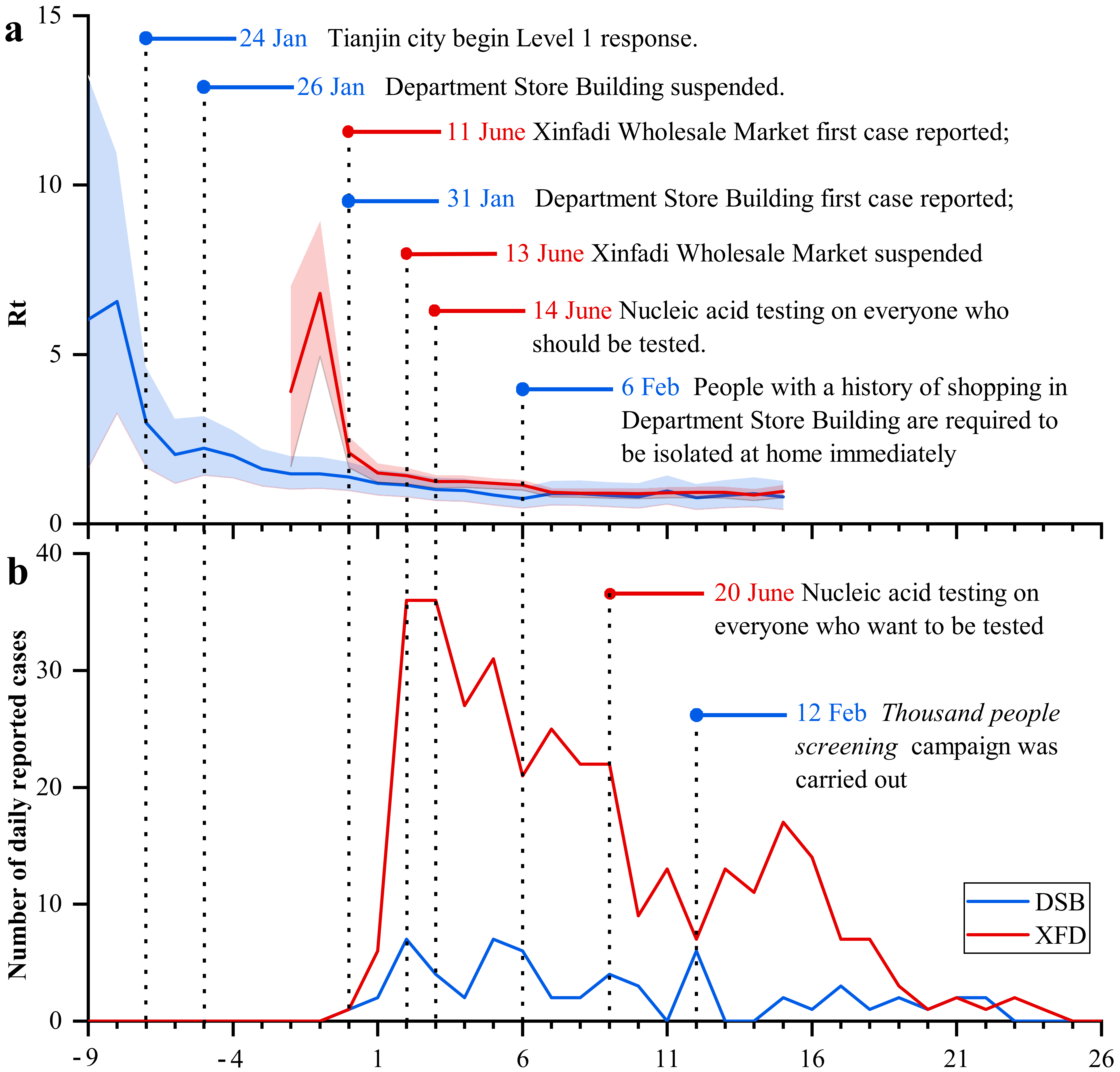
3.1. General Characteristics
3.2. Spatiotemporal Distributions
3.3. Sensitivity Analysis of Different Control Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duy, C.; Nong, V.M.; Van Ngo, A.; Doan, T.T.; Nguyen, T.Q.; Truong, P.T.; Olson, L.; Larsson, M. Nosocomial Coronavirus Disease Outbreak Containment, Hanoi, Vietnam, March–April 2020. Emerg. Infect. Dis. 2021, 27, 10. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.T.; Liu, Z.D.; Fan, Z.W.; Zhao, L.; Cao, W.C. Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study. Int. J. Environ. Res. Public Health 2020, 17, 7149. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Wuhan seafood market may not be source of novel virus spreading globally. Science 2020. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Chowell, G. Effect of a wet market on coronavirus disease (COVID-19) transmission dynamics in China, 2019–2020. Int. J. Infect. Dis. 2020, 97, 96–101. [Google Scholar] [CrossRef]
- Zhang, Y.; Pan, Y.; Zhao, X.; Shi, W.; Chen, Z.; Zhang, S.; Liu, P.; Xiao, J.; Tan, W.; Wang, D.; et al. Genomic characterization of SARS-CoV-2 identified in a reemerging COVID-19 outbreak in Beijing’s Xinfadi market in 2020. Biosaf. Health 2020, 2, 202–205. [Google Scholar] [CrossRef]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China, 2020. Emerg. Infect. Dis. 2020, 26, 1343–1345. [Google Scholar] [CrossRef]
- Liu, Y.F.; Li, J.M.; Zhou, P.H.; Liu, J.; Dong, X.C.; Lyu, J.; Zhang, Y. Analysis on cluster cases of COVID-19 in Tianjin. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 653–656. [Google Scholar]
- Cao, C.; Li, Y.; Liu, S.; Fan, H.; Hao, L. Epidemiological characteristics of 58 cluster cases of novel coronavirus disease in Baodi district of Tianjin city. Chin. J. Public Health 2020, 36, 289–292. [Google Scholar]
- Bae, S.; Kim, H.; Jung, T.Y.; Lim, J.A.; Jo, D.H.; Kang, G.S.; Jeong, S.H.; Choi, D.K.; Kim, H.J.; Cheon, Y.H.; et al. Epidemiological Characteristics of COVID-19 Outbreak at Fitness Centers in Cheonan, Korea. J. Korean Med. Sci. 2020, 35, e288. [Google Scholar] [CrossRef]
- Currie, D.W.; Moreno, G.K.; Delahoy, M.J.; Pray, I.W.; Jovaag, A.; Braun, K.M.; Cole, D.; Shechter, T.; Fajardo, G.C.; Griggs, C.; et al. Interventions to Disrupt Coronavirus Disease Transmission at a University, Wisconsin, USA. Emerg. Infect. Dis. 2021, 27, 11. [Google Scholar] [CrossRef]
- Furuse, Y.; Sando, E.; Tsuchiya, N.; Miyahara, R.; Yasuda, I.; Ko, Y.K.; Saito, M.; Morimoto, K.; Imamura, T.; Shobugawa, Y.; et al. Clusters of Coronavirus Disease in Communities, Japan, January–April 2020. Emerg. Infect. Dis. 2020, 26, 2176–2179. [Google Scholar] [CrossRef] [PubMed]
- Haw, N.J.L.; Uy, J.; Sy, K.T.L.; Abrigo, M.R.M. Epidemiological profile and transmission dynamics of COVID-19 in the Philippines. Epidemiol. Infect. 2020, 48, e204. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.J.; Zhou, Y.; Zhang, X.B.; Lin, X.T.; Chen, L.; Ni, X.H.; Huang, S.C.; Ruan, F. A survey on the first clustering of coronavirus disease 2019 in Zhuhai city. Chin. J. Public Health 2020, 36, 273–276. [Google Scholar]
- Taylor, P.J.; Openshaw, S. Distance Decay in Spatial Interactions. In Concepts and Techniques in Modern Geography; Geo Abstracts Limited: Norwich, UK, 1975. [Google Scholar]
- Chen, Y. The Distance-Decay Function of Geographical Gravity Model: Power Law or Exponential Law? Chaos Solitons Fractals 2015, 77, 174–189. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Li, Y.; Feng, S.; Man, X.; Long, Y. Gravitational Scaling Analysis on Spatial Diffusion of COVID-19 in Hubei Province, China. PLoS ONE 2021, 16, e0252889. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-C.; Chi, W.-J.; Lin, Y.-T.; Lai, C.-Y. The Spatiotemporal Estimation of the Risk and the International Transmission of COVID-19: A Global Perspective. Sci. Rep. 2020, 10, 20021. [Google Scholar] [CrossRef]
- Han, S.; Cai, J.; Yang, J.; Zhang, J.; Wu, Q.; Zheng, W.; Shi, H.; Ajelli, M.; Zhou, X.H.; Yu, H. Time-varying optimization of COVID-19 vaccine prioritization in the context of limited vaccination capacity. Nat. Commun. 2021, 12, 4673. [Google Scholar] [CrossRef]
- National Health Commission of the PRC. COVID-19 Vaccination. 2021. Available online: http://www.gov.cn/xinwen/2022-04/08/content_5684088.htm (accessed on 7 April 2021).
- Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Malek, J.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. mRNA-1273 COVID-19 vaccine effectiveness against the B.1.1.7 and B.1.351 variants and severe COVID-19 disease in Qatar. Nat. Med. 2021, 27, 1614–1621. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Cauchemez, S. A New Framework and Software to Estimate Time-Varying Reproduction Numbers During Epidemics. Am. J. Epidemiol. 2013, 178, 1505–1512. [Google Scholar] [CrossRef] [Green Version]
- Fraser, C. Estimating Individual and Household Reproduction Numbers in an Emerging Epidemic. PLoS ONE 2007, 2, e758. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.N.; Stockwin, J.E.; van Gaalen, R.D.; Polonsky, J.A.; Kamvar, Z.N.; Demarsh, P.A.; Dahlqwist, E.; Li, S.; Miguel, E.; Jombart, T.; et al. Improved inference of time-varying reproduction numbers during infectious disease outbreaks. Epidemics 2019, 29, 100356. [Google Scholar] [CrossRef] [PubMed]
- Abbott, S.; Hellewell, J.; Thompson, R.N.; Sherratt, K.; Gibbs, H.P.; Bosse, N.I.; Munday, J.D.; Meakin, S.; Doughty, E.L.; Chun, J.Y.; et al. Estimating the time-varying reproduction number of SARS-CoV-2 using national and subnational case counts. Wellcome Open Res. 2020, 5, 112. [Google Scholar] [CrossRef]
- Lefever, D.W. Measuring Geographic Concentration by Means of the Standard Deviational Ellipse. Am. J. Sociol. 1926, 32, 88–94. [Google Scholar] [CrossRef]
- Mitchell, A. The ESRI Guide to GIS Analysis, Volume 2; ESRI Press: Redlands, CA, USA, 2005. [Google Scholar]
- Li, Y.; Gong, H.; Zhu, L.; Li, X. Measuring Spatiotemporal Features of Land Subsidence, Groundwater Drawdown, and Compressible Layer Thickness in Beijing Plain, China. Water 2017, 9, 64. [Google Scholar] [CrossRef]
- Cui, X.; Zhao, L.; Zhou, Y.; Lin, X.; Ye, R.; Ma, K.; Jiang, J.-F.; Jiang, B.; Xiong, Z.; Shi, H.; et al. Transmission Dynamics and the Effects of Non-Pharmaceutical Interventions in the COVID-19 Outbreak Resurged in Beijing, China: A Descriptive and Modelling Study. BMJ Open 2021, 11, e047227. [Google Scholar] [CrossRef]
- Weishen, W.; Yonggang, L.; Zhaofei, W.; Penghui, Z.; Likun, L.; Guoping, Z.; Ying, Z.; Haiyan, H.; Xiaoyan, L.; Lu, G.; et al. Investigation and analysis on characteristics of a cluster of COVID-19 associated with exposure in a department store in Tianjin. Chin. J. Epidemiol. 2020, 41, 489–493. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | DSB | XFD |
|---|---|---|
| Outbreak time | ||
| Notification time of the first confirmed case | 31 Jan 2020 | 11 Jun 2020 |
| Notification time of the last confirmed case | 22 Feb 2020 | 5 Jul 2020 |
| Time taken to detect all associated cases | 23 days | 25 days |
| Demographic Characteristics | ||
| Confirmed | 60 | 335 |
| Male | 25 (41.7%) | 187 (55.8%) |
| Female | 35 (58.3%) | 148 (44.2%) |
| Age (median (IQR 1)) | 50 (36~64) | 43 (31~52) |
| Incubation period: median (range) | 9.5 (6~12) | 5 (3~8) |
| Days from onset to confirmation: median (IQR 1) | 6 (3~9) | 2 (1~4) |
| Prevention and control measures | ||
| Market suspension | Y | Y |
| Home quarantine | Y | Y |
| Close contact tracing | Y | Y |
| Nucleic acid testing | Y | N |
| Vaccination | N | N |
| Lockdown | Y | N |
| Death status | ||
| Nondeath case | 59 | 335 |
| Death case | 1 | 0 |
| CFR (%) | 1.7 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, W.; Gong, J.; Zhou, J.; Fan, H.; Qin, C.; Gong, Y.; Hu, W. The Analysis of Patterns of Two COVID-19 Outbreak Clusters in China. Int. J. Environ. Res. Public Health 2022, 19, 4876. https://doi.org/10.3390/ijerph19084876
Li W, Gong J, Zhou J, Fan H, Qin C, Gong Y, Hu W. The Analysis of Patterns of Two COVID-19 Outbreak Clusters in China. International Journal of Environmental Research and Public Health. 2022; 19(8):4876. https://doi.org/10.3390/ijerph19084876
Chicago/Turabian StyleLi, Wenning, Jianhua Gong, Jieping Zhou, Hongkui Fan, Cheng Qin, Yujiang Gong, and Weidong Hu. 2022. "The Analysis of Patterns of Two COVID-19 Outbreak Clusters in China" International Journal of Environmental Research and Public Health 19, no. 8: 4876. https://doi.org/10.3390/ijerph19084876
APA StyleLi, W., Gong, J., Zhou, J., Fan, H., Qin, C., Gong, Y., & Hu, W. (2022). The Analysis of Patterns of Two COVID-19 Outbreak Clusters in China. International Journal of Environmental Research and Public Health, 19(8), 4876. https://doi.org/10.3390/ijerph19084876