
The Benefits of Physical Activity for People with Obesity, Independent of Weight Loss: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
3. Results
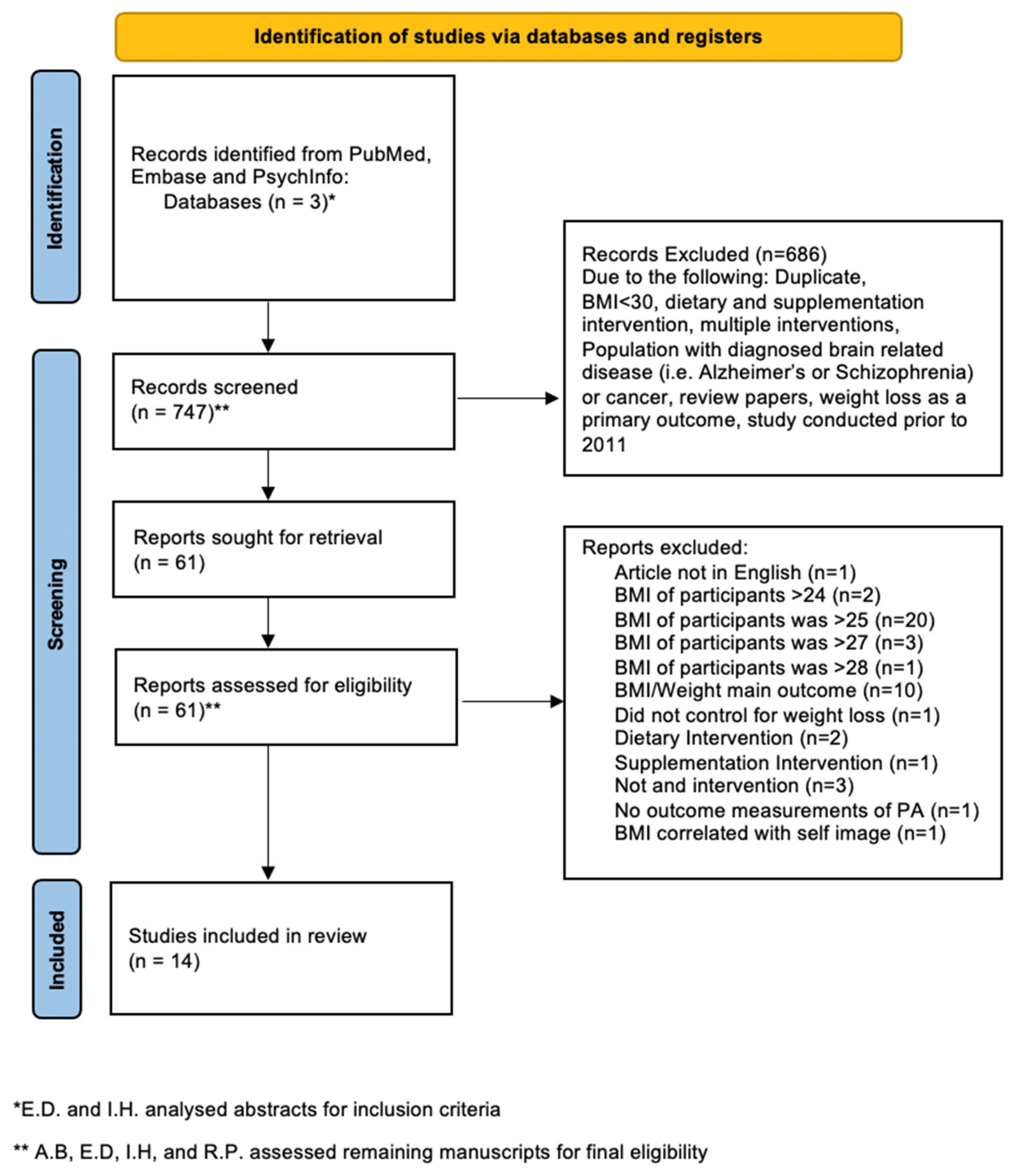
3.1. Included Articles
3.2. Cellular Outcomes
3.3. Metabolic and Cardiovascular Outcomes
3.4. Systemic Outcomes
3.5. Brain Health Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adult Obesity Facts. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 21 January 2022).
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 January 2022).
- Gaesser, G.A.; Angadi, S.S. Obesity treatment: Weight loss versus increasing fitness and physical activity for reducing health risks. iScience 2021, 24, 102995. [Google Scholar] [CrossRef] [PubMed]
- Barry, V.W.; Baruth, M.; Beets, M.W.; Durstine, J.L.; Liu, J.; Blair, S.N. Fitness vs. Fatness on All-Cause Mortality: A Meta-Analysis. Prog. Cardiovasc. Dis. 2014, 56, 382–390. [Google Scholar] [CrossRef]
- Carbone, S.; Kirkman, D.L.; Garten, R.S.; Rodriguez-Miguelez, P.; Artero, E.G.; Lee, D.-C.; Lavie, C.J. Muscular Strength and Cardiovascular Disease: An updated state-of-the-art narrative review. J. Cardiopulm. Rehabil. Prev. 2020, 40, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Cash, R.E.; Bower, J.K.; Focht, B.C.; Paskett, E.D. Physical activity and risk of cardiovascular disease by weight status among U.S adults. PLoS ONE 2020, 15, e0232893. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Lee, D.-C.; Katzmarzyk, P.T.; Ruiz, J.R.; Sui, X.; Church, T.S.; Blair, S.N. The intriguing metabolically healthy but obese phenotype: Cardiovascular prognosis and role of fitness. Eur. Heart J. 2013, 34, 389–397. [Google Scholar] [CrossRef]
- Pucci, G.C.M.F.; Rech, C.R.; Fermino, R.C.; Reis, R.S. Association between physical activity and quality of life in adults. Rev. Saude Publica 2012, 46, 166–179. [Google Scholar] [CrossRef] [Green Version]
- Halloway, S.; Wilbur, J.; Schoeny, M.E.; Arfanakis, K. Effects of Endurance-Focused Physical Activity Interventions on Brain Health: A Systematic Review. Biol. Res. Nurs. 2017, 19, 53–64. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.; Sherwood, A. Aerobic Exercise and Neurocognitive Performance: A Meta-Analytic Review of Randomized Controlled Trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef]
- Roig, M.; Nordbrandt, S.; Geertsen, S.S.; Nielsen, J.B. The effects of cardiovascular exercise on human memory: A review with meta-analysis. Neurosci. Biobehav. Rev. 2013, 37, 1645–1666. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1364387. [Google Scholar]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. The Effects of Resistance Exercise Training on Anxiety: A Meta-Analysis and Meta-Regression Analysis of Randomized Controlled Trials. Sports Med. 2017, 47, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Mayoral, L.P.C.; Andrade, G.M.; Mayoral, E.P.C.; Huerta, T.H.; Canseco, S.P.; Canales, F.J.R.; Cabrera-Fuentes, H.A.; Cruz, M.M.; Santiago, A.D.P.; Alpuche, J.J.; et al. Obesity subtypes, related biomarkers & heterogeneity. Indian J. Med Res. 2020, 151, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biddle, M.G.; Vincent, G.; McCambridge, A.; Britton, G.; Dewes, O.; Elley, C.R.; Moyes, S.; Edge, J. Randomised controlled trial of informal team sports for cardiorespiratory fitness and health benefit in Pacific adults. J. Prim. Health Care 2011, 3, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Brandao, C.F.C.; Nonino, C.B.; De Carvalho, F.G.; Nicoletti, C.F.; Noronha, N.Y.; San Martin, R.; De Freitas, E.C.; Junqueira-Franco, M.V.M.; Marchini, J.S. The effects of short-term combined exercise training on telomere length in obese women: A prospective, interventional study. Sports Med. Open 2020, 6, 5. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2004065437&from=exportU2-L2004065437 (accessed on 21 January 2022). [CrossRef] [Green Version]
- Cocks, M.; Shaw, C.S.; Shepherd, S.O.; Fisher, J.P.; Ranasinghe, A.; Barker, T.A.; Wagenmakers, A.J. Sprint interval and moderate-intensity continuous training have equal benefits on aerobic capacity, insulin sensitivity, muscle capillarisation and endothelial eNOS/NAD (P) Hoxidase protein ratio in obese men. J. Physiol. 2016, 594, 2307–2321. [Google Scholar] [CrossRef]
- Colpitts, B.H.; Seaman, K.; Eadie, A.L.; Brunt, K.R.; Bouchard, D.R.; Sénéchal, M. Effects of sprint interval training on substrate oxidation in adults living with and without obesity: The i-FLEX study. Physiol. Rep. 2021, 9, e14916. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2012741791&from=exportU2-L2012741791 (accessed on 21 January 2022). [CrossRef]
- Dalleck, L.C.; Van Guilder, G.P.; Richardson, T.B.; Bredle, D.L.; Janot, J.M. A community-based exercise intervention transitions metabolically abnormal obese adults to a metabolically healthy obese phenotype. Diabetes, Metab. Syndr. Obes. Targets Ther. 2014, 7, 369–380. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Williams, G.; Kostner, K.; Brown, W.J. The Effect of Tai Chi on Quality of Life in Centrally Obese Adults with Depression. J. Altern. Complement. Med. 2019, 25, 1005–1008. [Google Scholar] [CrossRef]
- Lubans, D.R.; Plotnikoff, R.C.; Jung, M.; Eves, N.; Sigal, R. Testing mediator variables in a resistance training intervention for obese adults with type 2 diabetes. Psychol. Health 2012, 27, 1388–1404. [Google Scholar] [CrossRef]
- McNeilly, A.M.; McClean, C.; Murphy, M.; McEneny, J.; Trinick, T.; Burke, G.; Duly, E.; McLaughlin, J.; Davison, G. Exercise training and impaired glucose tolerance in obese humans. J. Sports Sci. 2012, 30, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Mendham, A.E.; Goedecke, J.H.; Fortuin-de Smidt, M.C.; Phiri, L.; Clamp, L.; Swart, J.; Lipinska, G.; Rae, D.E. Improved Sleep Quality and Depressive Symptoms With Exercise Training in Obese Women From a Low Socioeconomic Community: A Randomized Controlled Trial. J. Phys. Act. Health 2021, 18, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Mendham, A.E.; Goedecke, J.H.; Zeng, Y.; Larsen, S.; George, C.; Hauksson, J.; Smidt, M.C.F.-D.; Chibalin, A.V.; Olsson, T.; Chorell, E. Exercise training improves mitochondrial respiration and is associated with an altered intramuscular phospholipid signature in women with obesity. Diabetologia 2021, 64, 1642–1659. [Google Scholar] [CrossRef] [PubMed]
- Sabag, A.; Way, K.L.; Sultana, R.N.; Keating, S.E.; Gerofi, J.A.; Chuter, V.H.; Byrne, N.M.; Baker, M.K.; George, J.; Caterson, I.D.; et al. The Effect of a Novel Low-Volume Aerobic Exercise Intervention on Liver Fat in Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2020, 43, 2371–2378. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, B.; Tucker, W.J.; Bhammar, D.M.; Ryder, J.; Sweazea, K.; Gaesser, G.A. Effects of high-intensity interval training and moderate-intensity continuous training on endothelial function and cardiometabolic risk markers in obese adults. J. Appl. Physiol. 2016, 121, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Way, K.L.; Sabag, A.; Sultana, R.N.; Baker, M.K.; Keating, S.E.; Lanting, S.; Gerofi, J.; Chuter, V.H.; Caterson, I.D.; Twigg, S.M.; et al. The effect of low-volume high-intensity interval training on cardiovascular health outcomes in type 2 diabetes: A randomised controlled trial. Int. J. Cardiol. 2020, 320, 148–154. [Google Scholar] [CrossRef]
- Woudberg, N.J.; Mendham, A.E.; Katz, A.A.; Goedecke, J.H.; Lecour, S. Exercise intervention alters HDL subclass distribution and function in obese women. Lipids Health Dis. 2018, 17, 232. [Google Scholar] [CrossRef] [Green Version]
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. state-level prevalence of adult obesity and severe obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Gaesser, G.A.; Angadi, S.S.; Sawyer, B.J. Exercise and Diet, Independent of Weight Loss, Improve Cardiometabolic Risk Profile in Overweight and Obese Individuals. Physician Sportsmed. 2011, 39, 87–97. [Google Scholar] [CrossRef]
- Physical Activity Guidelines for Americans Scientific Report. 2018. Available online: https://health.gov/our-work/nutrition-physical-activity/physical-activity-guidelines/current-guidelines/scientific-report (accessed on 1 February 2022).
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.-P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Nelson, V.R.; Masocol, R.V.; Ewing, J.A.; Johnston, S.; Hale, A.; Wiederman, M.; Asif, I.M. Association Between a Physical Activity Vital Sign and Cardiometabolic Disease in High-Risk Patients. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2020, 30, 348–352. [Google Scholar] [CrossRef]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2016, 22, 842–884. Available online: https://www.aace.com/publications/guidelines (accessed on 21 January 2022).
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129 (Suppl. S2), S102–S138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pojednic, R.; Stoutenberg, M. Key Steps to Implementing Physical Activity into Health Professional Training Programs. Curr. Sports Med. Rep. 2020, 19, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Segar, M.L.; Guérin, E.; Phillips, E.; Fortier, M. From a Vital Sign to Vitality: Selling Exercise So Patients Want to Buy It. Curr. Sports Med. Rep. 2016, 15, 276–281. [Google Scholar] [CrossRef]
- Bergeron, C.D.; Tanner, A.H.; Friedman, D.B.; Zheng, Y.; Schrock, C.S.; Bornstein, D.B.; Segar, M.; Swift, N. Physical Activity Communication: A Scoping Review of the Literature. Health Promot. Pract. 2019, 20, 344–353. [Google Scholar] [CrossRef]
- Montani, J.-P.; Schutz, Y.; Dulloo, A. Dieting and weight cycling as risk factors for cardiometabolic diseases: Who is really at risk? Obes. Rev. 2015, 16 (Suppl. S1), 7–18. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Database | Search Terms Used |
|---|---|
| Embase | intervention AND obes# AND ‘physical activity’ AND fitness AND physical AND exercise NOT ‘body weight loss’ NOT (weight AND reduction) NOT ‘weight management’ NOT (lose AND weight) NOT (body AND composition AND assessment) AND [2011–2021]/py AND ([adult]/lim OR [aged]/lim) |
| PsychInfo | Intervention AND obes* AND physical activity or exercise or fitness or physical exercise NOT weight loss NOT weight reduction NOT weight management NOT lose weight NOT body composition assessment; Adults 18–64, 65+; PY 2011–2021 |
| Pubmed | (body mass index OR “obes *” or “obesity paradox” OR “obesity treatment”) AND (“physical activity” or “exercise” or “fitness”) AND (reducing health risks) AND (weight neutral) |
| Pubmed | (body mass index) AND (humans) AND (life style) AND (“adult *”) OR (“obes *”) AND (“physical activity” or “exercise”) AND (health benefits independent of weight status) |
| Pubmed | (body mass index OR “obes *” or “obesity paradox”) AND (“physical activity” or “exercise”) AND (Cardiorespiratory fitness) AND (“fitness and fatness”) |
| Pubmed | (adult) OR (aged) OR (middle aged) AND (body mass index) AND (humans) AND (life style) AND (mortality / trends) OR (obesity/mortality) OR (overweight/mortality) AND (united states/epidemiology) AND (risk reduction behavior) |
| Pubmed | (body mass index OR “obes *” or “obesity paradox” OR “obesity treatment”) AND (“physical activity” or “exercise” or “fitness”) AND (“CRF”) AND (“fitness and fatness”) AND (reducing health risks) |
| Author | Year Published | Country | Outcome Category | Physical Activity Modality | Subjects a | Intervention Duration and Frequency | Primary Outcome | Results | BMI (kg/m2) |
|---|---|---|---|---|---|---|---|---|---|
| Biddle, M.G. et al. [16] | 2011 | New Zealand | Systemic | Sports Games | Sedentary Pacific Adults from age 16–65; n = 9 INT, n = 11 CON | 45 min per day, 3 times per week, for 4 weeks | Cardiorespiratory fitness and leg strength | Increase in VO2 peak (p = 0.003), leg strength (p = 0.04) and HDL (p = 0.02) were greater within the intervention versus control group | 36.3 |
| Brandao, C.F.C. et al. [17] | 2020 | Brazil | Cellular | Combined Aerobic and Resistance Training | Sedentary Females from age 20–40; n = 20 (No CON) | 55 min per day, 3 times per week, for 8 weeks | Telomere length | Increased telomere length, fat-free mass and VO2 max. Inverse relationship between telomere length and waist circumference (p < 0.05) | 34 |
| Cocks, M. et al. [18] | 2016 | United Kingdom | Cellular | SIT or MICT using a cycle ergometer | Sedentary Young Men; n = 8 INT; n = 8 CON | SIT: 4–7 constant workload intervals of 200% Wmax 3 times per week; MICT: 40–60 min cycling at 65% VO2 peak, 5 times per week, for 4 weeks | Skeletal muscle microvascular density and microvascular filtration capacity | SIT and MICT have equal benefits on aerobic capacity, insulin sensitivity, muscle capillarization and endothelial protein ratio men with obesity (p < 0.05) | 34.8 |
| Colpitts, B.H. et al. [19] | 2021 | Canada | Metabolic and Cardiovascular | SIT using a cycle ergometer | Inactive adults between age 16–60 years; n = 12 with obesity, n = 18 without obesity | 30 s Wingate cycling with 4 min of active recovery, 3 times per week, for 4 weeks | Substrate oxidation at rest and at submaximal exercise | Significant increase in fat oxidation during exercise for adults living obesity (p = 0.001) | 34.1 |
| Dalleck, L.C. et al. [20] | 2014 | USA | Systemic | Supervised community-based exercise program | Healthy Adults aged 22–88 years; n = 55 MAO, n = 37 MHO, n = 200 MH not obese; n = 24 MA not obese | Personalized time periods, 3 times per week, for 14 weeks | Metabolic Phenotype | 40% of metabolically abnormally obese (MAO) individuals transitioned to a metabolically healthy but obese (MHO) phenotype (p < 0.05) | 34.1 |
| Liu, Xin et al. [21] | 2019 | Australia | Brain Health | Tai Chi | Adults with a diagnosis of depression; n = 106 INT n = 107 CON | 1.5 h sessions, 3 times per week, for 24 weeks | Quality of life and emotional health | Improvement of physical functioning, role in physical health and role in emotional health (p < 0.05) | >30 |
| Lubans, D.R. et al. [22] | 2012 | Canada | Systemic | Supervised Resistance Training | Sedentary adults with Type 2 Diabetes; n = 27 INT; n = 21 CON | 3 times per week, for 16 weeks | Muscular strength and resistance training behavior | Increased muscle strength and resistance training behavior (p < 0.05) | 36 |
| McNeilly, A.M. et al. [23] | 2012 | United Kingdom | Metabolic and Cardiovascular | Treadmill Walking | Adults with impaired glucose tolerance; n = 11 (no CON) | 30 min walking at 65% maximum heart rate, 5 times a week, for 12 weeks | Arterial stiffness | Improvement in Pulse wave velocity, systolic blood pressure, triglycerides and lipid hydroperoxides (p < 0.05) | 32.4 |
| Mendham, A.E. et al. [24] | 2021 | South Africa | Brain Health | Combined Aerobic and Resistance Training | Low Income adults women aged 20–35 years; n = 20 INT; n = 15 CON | 40–60 min at a moderate-vigorous intensity, 4 days per week for 12 weeks | Depressive Symptoms and Sleep quality | Depressive symptoms improved with peak oxygen consumption (p < 0.001) while sleep improvement was correlated with reduced sedentary time (p = 0.018). | 30–40 |
| Mendham, A.E. et al. [25] | 2021 | South Africa | Metabolic and Cardiovascular | Combined Aerobic and Resistance Training | Low Income Black adult women aged 20–35 years; n = 20 INT; n = 15 CON | 40–60 min at a moderate-vigorous intensity, 4 days per week for 12 weeks | Mitochondrial respiration and the association with altered intramuscular phospholipid signature in women with obesity | Exercise training significantly altered the skeletal muscle lipid profile and increased content driven mitochondrial metabolism (p < 0.05) | 30–40 |
| Sabag, A. et al. [26] | 2020 | Australia | Metabolic and Cardiovascular | HIIT training/cycling MICT training/cycling or CON | Inactive Adults with Type 2 Diabetes; n = 12 MICT; n = 12 HIIT; n = 11 CON | HIIT: 19 total minutes of intervals designed to elicit 90% VO2 peak; MICT: 45 min at 60% VO2 peak, 3 days per week, for 12 weeks | Liver fat, glucose metabolism, cardiorespiratory fitness | Decreased liver fat (p = 0.046), HbA1C (p = 0.014) and improved cardiorespiratory fitness (p = 0.006) in MICT/HIIT but not placebo | 35.9 |
| Sawyer B.J et al. [27] | 2016 | USA | Metabolic and Cardiovascular | HIIT training/cycling MICT training/cycling | Healthy adults aged 18–55 years; n = 11 HIIT; n = 11 MICT | HIIT: 10 × 1 min intervals at 90–95% maximum heart rate; MICT: 30 min at 70–75% maximum heart rate, 3 sessions per week, for 8 weeks (3 sessions/wk) of either | Endothelial function and maximum oxygen uptake | HIIT improved brachial artery flow-mediated dilation (p = 0.02) and MICT increased resting artery diameter (p = 0.02).HIIT and MICT both enhanced low flow-mediated constriction (p = 0.03) and VO2 max in both groups (p < 0.01) | |
| Way, K.L. et al. [28] | 2020 | Australia | Systemic | HIIT training/cycling MICT training/cycling or CON | Inactive Adults with Type 2 Diabetes; n = 12 MICT; n = 12 HIIT; n = 11 CON | HIIT: 19 total minutes of intervals designed to elicit 90% VO2 peak; MICT: 45 min at 60% VO2 peak, 3 days per week, for 12 weeks | Central arterial stiffness and hemodynamic responses | Significant reduction in pulse wave velocity (p = 0.03) HbA1c (p = 0.03), systolic blood pressure (p = 0.01) and waist circumference (p = 0.03), | 36.1 |
| Woudberg N.J. et al. [29] | 2018 | South Africa | Metabolic and Cardiovascular | Combined Aerobic and Resistance Training | Low Income Black adult women aged 20–35 years; n = 20 INT; n = 15 CON | 40–60 min at a moderate-vigorous intensity, 4 days per week for 12 weeks | Lipid profile and HDL functionality | Decreased BMI (p = 0.01), increased antioxidant capacity (p = 0.02) and anti-thrombotic function (p = 0.002) | 30–40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pojednic, R.; D'Arpino, E.; Halliday, I.; Bantham, A. The Benefits of Physical Activity for People with Obesity, Independent of Weight Loss: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 4981. https://doi.org/10.3390/ijerph19094981
Pojednic R, D'Arpino E, Halliday I, Bantham A. The Benefits of Physical Activity for People with Obesity, Independent of Weight Loss: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(9):4981. https://doi.org/10.3390/ijerph19094981
Chicago/Turabian StylePojednic, Rachele, Emma D'Arpino, Ian Halliday, and Amy Bantham. 2022. "The Benefits of Physical Activity for People with Obesity, Independent of Weight Loss: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 9: 4981. https://doi.org/10.3390/ijerph19094981
APA StylePojednic, R., D'Arpino, E., Halliday, I., & Bantham, A. (2022). The Benefits of Physical Activity for People with Obesity, Independent of Weight Loss: A Systematic Review. International Journal of Environmental Research and Public Health, 19(9), 4981. https://doi.org/10.3390/ijerph19094981