
Post-Hurricane Distress Scale (PHDS): Determination of General and Disorder-Specific Cutoff Scores

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Assessment Tools
2.2.1. PHDS Questionnaire
2.2.2. GAD-7 Questionnaire
2.2.3. K6 Questionnaire
2.2.4. PHQ-9 Questionnaire
2.2.5. PCL-5 Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
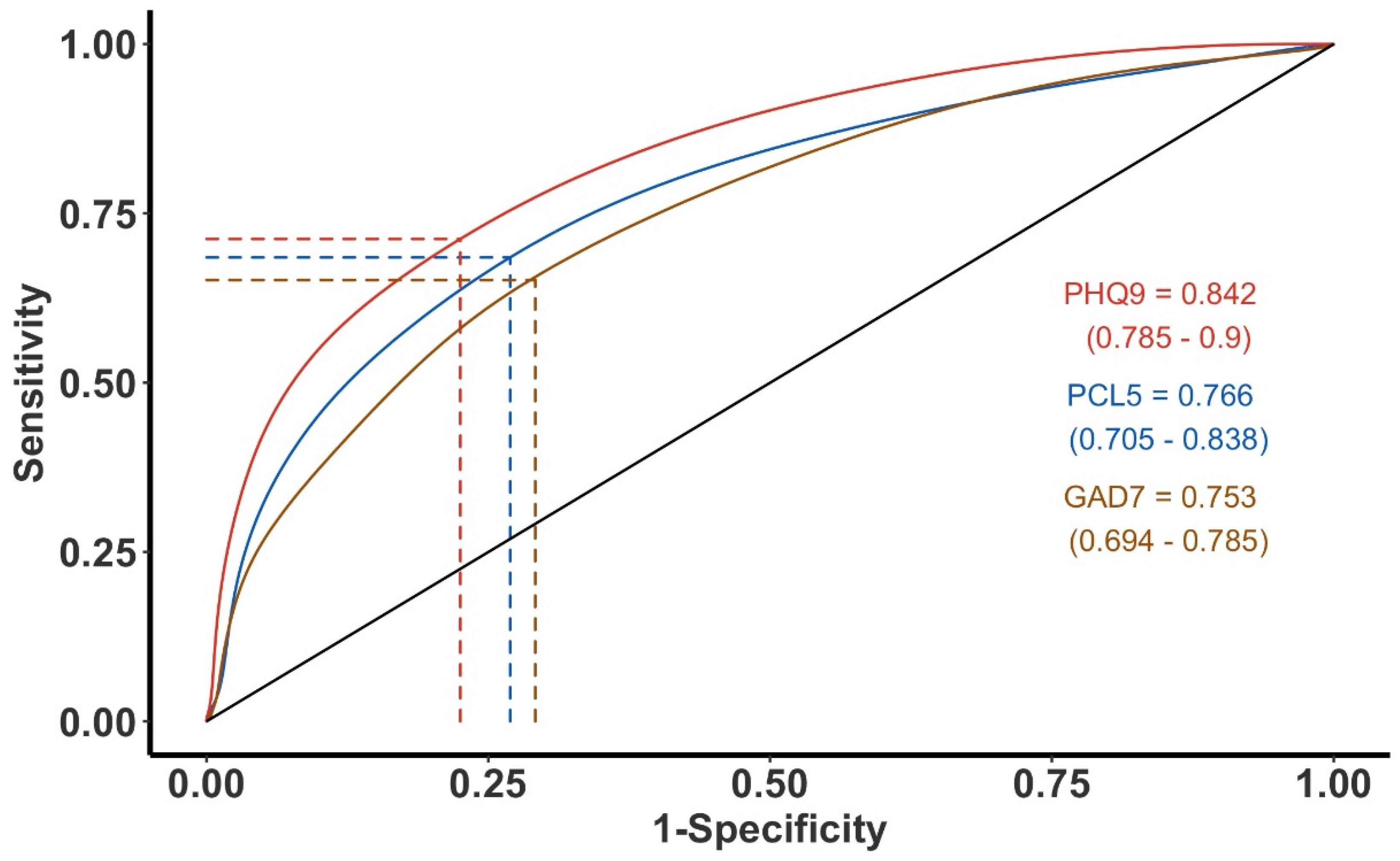
3.2. Predictive Accuracy of PHDS and Disorder Cutoffs Indices
3.3. Derivation of Both Disorder-Specific Cutoffs, as Well as a Single PHDS Cutoff Value
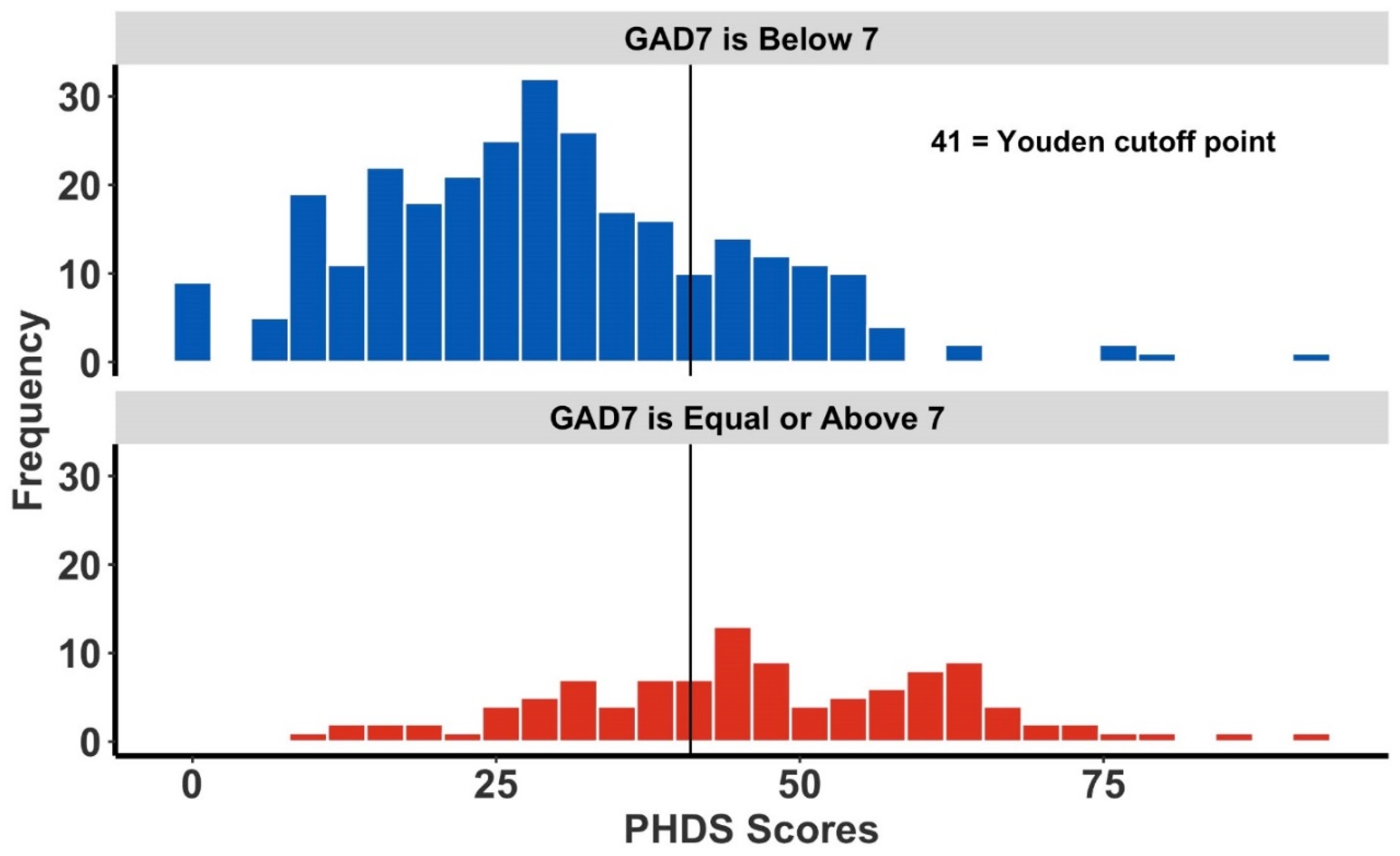
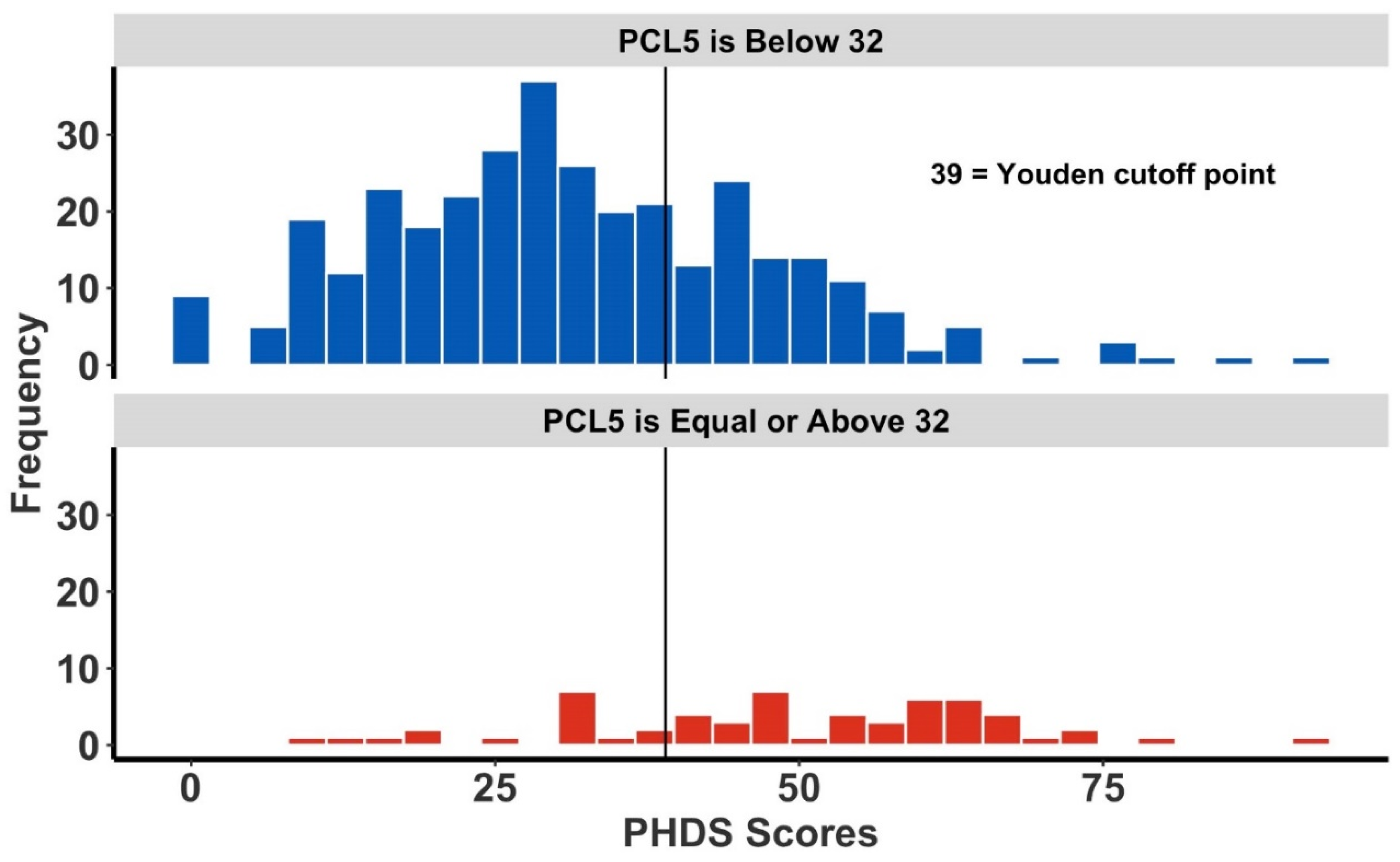
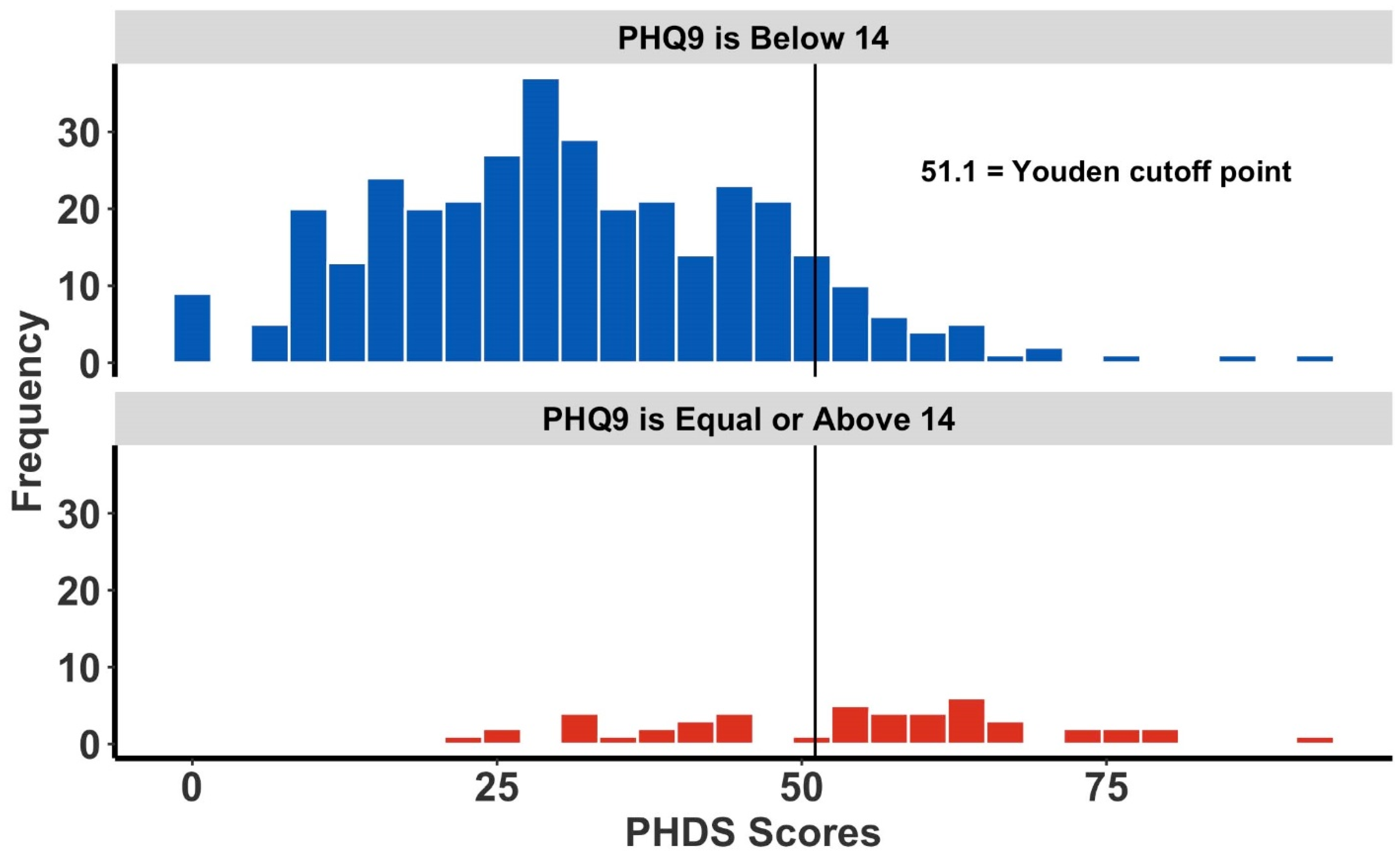
3.4. Histograms and Distribution Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hussain, A.; Weisaeth, L.; Heir, T. Psychiatric disorders and functional impairment among disaster victims after exposure to a natural disaster: A population based study. J. Affect. Disord. 2011, 128, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Math, S.B.; Nirmala, M.C.; Moirangthem, S.; Kumar, N.C. Disaster Management: Mental Health Perspective. Indian J. Psychol. Med. 2015, 37, 261–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galea, S.; Nandi, A.; Vlahov, D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol. Rev. 2005, 27, 78–91. [Google Scholar] [CrossRef] [Green Version]
- Kopala-Sibley, D.C.; Kotov, R.; Bromet, E.J.; Carlson, G.A.; Danzig, A.P.; Black, S.R.; Klein, D.N. Personality diatheses and Hurricane Sandy: Effects on post-disaster depression. Psychol. Med. 2016, 46, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.S.; Rhodes, J.E. Measuring exposure in Hurricane Katrina: A meta-analysis and an integrative data analysis. PLoS ONE 2014, 9, e92899. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Udomratn, P. Mental health and the psychosocial consequences of natural disasters in Asia. Int. Rev. Psychiatry 2008, 20, 441–444. [Google Scholar] [CrossRef]
- Beaglehole, B.; Mulder, R.T.; Frampton, C.M.; Boden, J.M.; Newton-Howes, G.; Bell, C.J. Psychological distress and psychiatric disorder after natural disasters: Systematic review and meta-analysis. Br. J. Psychiatry 2018, 213, 716–722. [Google Scholar] [CrossRef] [Green Version]
- Fullerton, C.S.; Ursano, R.J.; Liu, X.; McKibben, J.B.; Wang, L.; Reissman, D.B. Depressive Symptom Severity and Community Collective Efficacy following the 2004 Florida Hurricanes. PLoS ONE 2015, 10, e0130863. [Google Scholar] [CrossRef]
- Robert, L.S.J.; Kroenke, K. Patient Health Questionnaire Screeners. Available online: https://www.phqscreeners.com/select-screener/31 (accessed on 21 February 2022).
- Carl, Y.; Ortiz, E.R.; Cintron, M.; Vega, A.; Font, C.; Stukova, M.; Blundell, A.; Gutierrez, A.N.; Burgos, R.F. Post-Hurricane Distress Scale (PHDS): A Novel Tool for First Responders and Disaster Researchers. Disaster Med. Public Health Prep. 2019, 13, 82–89. [Google Scholar] [CrossRef]
- Elal, G.; Slade, P. Traumatic Exposure Severity Scale (TESS): A measure of exposure to major disasters. J. Trauma. Stress 2005, 18, 213–220. [Google Scholar] [CrossRef]
- Goldmann, E.; Galea, S. Mental Health Consequences of Disasters. Annu. Rev. Public Health 2013, 35, 169–183. [Google Scholar] [CrossRef]
- Lowe, S.R.; Tracy, M.; Cerda, M.; Norris, F.H.; Galea, S. Immediate and longer-term stressors and the mental health of Hurricane Ike survivors. J. Trauma. Stress 2013, 26, 753–761. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; McLaughlin, K.A.; Koenen, K.C.; Petukhova, M.; Hill, E.D.; WHO World Mental Health Survey Consortium. The importance of secondary trauma exposure for post-disaster mental disorder. Epidemiol. Psychiatr. Sci. 2012, 21, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.S.; Gruber, M.J.; Powers, R.E.; Schoenbaum, M.; Speier, A.H.; Wells, K.B.; Kessler, R.C. Disruption of existing mental health treatments and failure to initiate new treatment after Hurricane Katrina. Am. J. Psychiatry 2008, 165, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Cahill, S.P.; Pontoski, K. Post-traumatic stress disorder and acute stress disorder I: Their nature and assessment considerations. Psychiatry 2005, 2, 14–25. [Google Scholar]
- Keane, T.M.; Marshall, A.D.; Taft, C.T. Posttraumatic stress disorder: Etiology, epidemiology, and treatment outcome. Annu. Rev. Clin. Psychol. 2006, 2, 161–197. [Google Scholar] [CrossRef] [Green Version]
- Carl, Y.; Frias, R.L.; Kurtevski, S.; Gonzalez Copo, T.; Mustafa, A.R.; Font, C.M.; Blundell, A.R.; Rodriguez, E.C.; Sacasa, R. The Correlation of English Language Proficiency and Indices of Stress and Anxiety in Migrants from Puerto Rico after Hurricane Maria: A Preliminary Study. Disaster Med. Public Health Prep. 2020, 14, 23–27. [Google Scholar] [CrossRef]
- Chastang, F.; Rioux, P.; Dupont, I.; Baranger, E.; Kovess, V.; Zarifian, E. Suicide attempts and job insecurity: A complex association. Eur. Psychiatry 1998, 13, 359–364. [Google Scholar] [CrossRef]
- Libby, A.M.; Ghushchyan, V.; McQueen, R.B.; Slejko, J.F.; Bainbridge, J.L.; Campbell, J.D. Economic differences in direct and indirect costs between people with epilepsy and without epilepsy. Med. Care 2012, 50, 928–933. [Google Scholar] [CrossRef]
- Ranasinghe, S.; Ramesh, S.; Jacobsen, K.H. Hygiene and mental health among middle school students in India and 11 other countries. J. Infect. Public Health 2016, 9, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acquadro, C.; Conway, K.; Hareendran, A.; Aaronson, N.; European Regulatory Issues and Quality of Life Assessment (ERIQA) Group. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials. Value Health 2008, 11, 509–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.J.; Sung, H.Y.; Max, W.; Shi, Y.; Ong, M. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. CMAJ 2012, 184, E191–E196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Miles, J.N.; Marshall, G.N.; Schell, T.L. Spanish and English versions of the PTSD Checklist-Civilian version (PCL-C): Testing for differential item functioning. J. Trauma. Stress 2008, 21, 369–376. [Google Scholar] [CrossRef]
- Kim, G.; DeCoster, J.; Bryant, A.N.; Ford, K.L. Measurement Equivalence of the K6 Scale: The Effects of Race/Ethnicity and Language. Assessment 2016, 23, 758–768. [Google Scholar] [CrossRef]
- Munoz-Navarro, R.; Cano-Vindel, A.; Medrano, L.A.; Schmitz, F.; Ruiz-Rodriguez, P.; Abellan-Maeso, C.; Font-Payeras, M.A.; Hermosilla-Pasamar, A.M. Utility of the PHQ-9 to identify major depressive disorder in adult patients in Spanish primary care centres. BMC Psychiatry 2017, 17, 291. [Google Scholar] [CrossRef]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eekhout, I.; de Vet, H.C.; Twisk, J.W.; Brand, J.P.; de Boer, M.R.; Heymans, M.W. Missing data in a multi-item instrument were best handled by multiple imputation at the item score level. J. Clin. Epidemiol. 2014, 67, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Ratón, M.; Rodríguez-Álvarez, M.X.; Cadarso-Suárez, C.; Gude-Sampedro, F. OptimalCutpoints: An R Package for Selecting Optimal Cutpoints in Diagnostic Tests. J. Stat. Softw. 2014, 61, 36. [Google Scholar] [CrossRef] [Green Version]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Ruopp, M.D.; Perkins, N.J.; Whitcomb, B.W.; Schisterman, E.F. Youden Index and optimal cut-point estimated from observations affected by a lower limit of detection. Biom. J. 2008, 50, 419–430. [Google Scholar] [CrossRef] [Green Version]
- Rice, M.E.; Harris, G.T. Comparing effect sizes in follow-up studies: ROC Area, Cohen’s d, and r. Law Hum. Behav. 2005, 29, 615–620. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Lowe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Belk, R.A.; Pilling, M.; Rogers, K.D.; Lovell, K.; Young, A. The theoretical and practical determination of clinical cut-offs for the British Sign Language versions of PHQ-9 and GAD-7. BMC Psychiatry 2016, 16, 372. [Google Scholar] [CrossRef] [Green Version]
- Moriarty, A.S.; Gilbody, S.; McMillan, D.; Manea, L. Screening and case finding for major depressive disorder using the Patient Health Questionnaire (PHQ-9): A meta-analysis. Gen. Hosp. Psychiatry 2015, 37, 567–576. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Range (Median) | 18–94 (43.5) | ||||
| 18–25 | N 140 | (%) (21) | 35–49 | N 153 | (%) (23) |
| 26–34 | 100 (15) | 50+ | 271 | (40) | |
| Gender | |||||
| Female | 434 | (65) | Male | 221 | (33) |
| Civil Status a | |||||
| Never married | 247 | (37) | Previously Married | 224 | (33) |
| Married | 193 | (28) | |||
| Ethnicity | |||||
| Hispanic | 427 | (97) | Not Hispanic | 4 | (1) |
| Race | |||||
| White | 271 | (61) | African American | 37 | (8) |
| Native American | 28 | (6) | Asian | 9 | (2) |
| Hawaiian/Pacific islands | 3 | (1) | Other | 80 | (18) |
| Education Level | |||||
| Less than High School | 52 | (8) | Bachelor’s or associate degree | 247 | (36) |
| High School | 133 | (20) | Graduate or professional degree | 122 | (18) |
| Some college, no degree | 111 | (17) | |||
| Employment Status b | |||||
| Employed | 292 | (49) | Retired/pensioned | 87 | (15) |
| Unemployed | 176 | (30) | Incapacitated | 35 | (6) |
| Combined household income | |||||
| US $10,000 or less | 192 | (29) | US $26,000 to $49,999 | 126 | (53) |
| US $10,000 to $25,999 | 252 | (38) | US $50,000 or more | 50 | (7) |
| Current living location c | |||||
| P.R: Eastern region | 206 | (31) | P.R: Northern region | 24 | (4) |
| P.R: Southern region | 178 | (26) | P.R: Western region | 20 | (3) |
| P.R: Central region | 145 | (22) | USA (emigrated participants) | 18 | (3) |
| P.R: Metropolitan region | 73 | (11) | |||
| Household Ownership | |||||
| Homeowner | 329 | (65) | Living with friend or family member (not paying rent) | 48 | (9) |
| Rent | 108 | (21) | Government paid home | 6 | (1) |
| Hotel/Motel | 3 | (1) | Homeless | 1 | (0) |
| Stayed in Puerto Rico During Hurricane Maria | Left Puerto Ricoafter Hurricane Maria | ||||
| Yes | 647 | (96) | Yes | 61 | (9) |
| No | 23 | (3) | No | 526 | (78) |
| Female Participants | Male Participants | |||
|---|---|---|---|---|
| Valid Number of Participants | Mean Score ± SD | Valid Number of Participants | Mean Score ± SD | |
| PHDS (N = 655) | 648 (66%) | 34.40 ± 16.92 | 333 (34%) | 32.19 ± 16.23 |
| K6 (N = 426) | 270 (63%) | 7.32 ± 6.29 | 156 (37%) | 5.73 ± 5.79 |
| GAD-7 (N = 644) | 425 (66%) | 6.05 ± 5.80 | 219 (34%) | 4.73 ± 5.12 |
| PHQ-9 (N = 425) | 270 (64%) | 6.38 ± 6.00 | 155 (37%) | 5.21 ± 5.80 |
| PCL-5 (N = 422) | 270 (64%) | 16.54 ± 16.90 | 152 (36%) | 12.63 ± 17.51 |
| GAD7 | K6 | PHQ-9 | PCL-5 | Hybrid Multi-Index Cutoff | ||
|---|---|---|---|---|---|---|
| Youden (Maximising) | Cut-off | 41 | 46 | 51 | 39 | 41 |
| sens, spec | 0.593, 0.791 | 0.576, 0.821 | 0.632, 0.901 | 0.746, 0.701 | 0.560, 0.801 | |
| LR+ | 2.800 | 3.212 | 6.395 | 2.495 | 2.84 | |
| FPR FP TN | 0.210 96 362 | 0.179 64 293 | 0.099 37 337 | 0.299 104 244 | 0.200 88 353 | |
| FNR TP FN | 0.407 105 72 | 0.424 38 28 | 0.367 31 18 | 0.250 44 15 | 0.440 116 91 | |
| AUC (95% CI) | 0.753 (0.694–0.785) | 0.744 (0.675–0.819) | 0.842 (0.785–0.900) | 0.766 (0.705–0.838) | 0.739 (0.698–0.780) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carl, Y.; Vega, A.; Cardona-Acevedo, G.; Stukova, M.; Matos-Rivera, M.; Torres-Sanchez, A.; Milián-Rodríguez, M.; Torres-Mercado, B.; Burgos, G.; Tremblay, R.L. Post-Hurricane Distress Scale (PHDS): Determination of General and Disorder-Specific Cutoff Scores. Int. J. Environ. Res. Public Health 2022, 19, 5204. https://doi.org/10.3390/ijerph19095204
Carl Y, Vega A, Cardona-Acevedo G, Stukova M, Matos-Rivera M, Torres-Sanchez A, Milián-Rodríguez M, Torres-Mercado B, Burgos G, Tremblay RL. Post-Hurricane Distress Scale (PHDS): Determination of General and Disorder-Specific Cutoff Scores. International Journal of Environmental Research and Public Health. 2022; 19(9):5204. https://doi.org/10.3390/ijerph19095204
Chicago/Turabian StyleCarl, Yonatan, Andy Vega, Gina Cardona-Acevedo, Marina Stukova, Melissa Matos-Rivera, Anamaris Torres-Sanchez, Melissa Milián-Rodríguez, Brian Torres-Mercado, Grisel Burgos, and Raymond L. Tremblay. 2022. "Post-Hurricane Distress Scale (PHDS): Determination of General and Disorder-Specific Cutoff Scores" International Journal of Environmental Research and Public Health 19, no. 9: 5204. https://doi.org/10.3390/ijerph19095204
APA StyleCarl, Y., Vega, A., Cardona-Acevedo, G., Stukova, M., Matos-Rivera, M., Torres-Sanchez, A., Milián-Rodríguez, M., Torres-Mercado, B., Burgos, G., & Tremblay, R. L. (2022). Post-Hurricane Distress Scale (PHDS): Determination of General and Disorder-Specific Cutoff Scores. International Journal of Environmental Research and Public Health, 19(9), 5204. https://doi.org/10.3390/ijerph19095204