
A Robot-Mediated Activity Using the Nao Robot to Promote COVID-19 Precautionary Measures among Older Adults in Geriatric Facilities


 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Material
2.2.1. Nao Robot
2.2.2. The Informational Robot-Mediated Scenario
- Introduction. The robot Nao presents itself as an assistant helping the hospital professionals and says that it will describe five ways to protect oneself from the COVID-19;
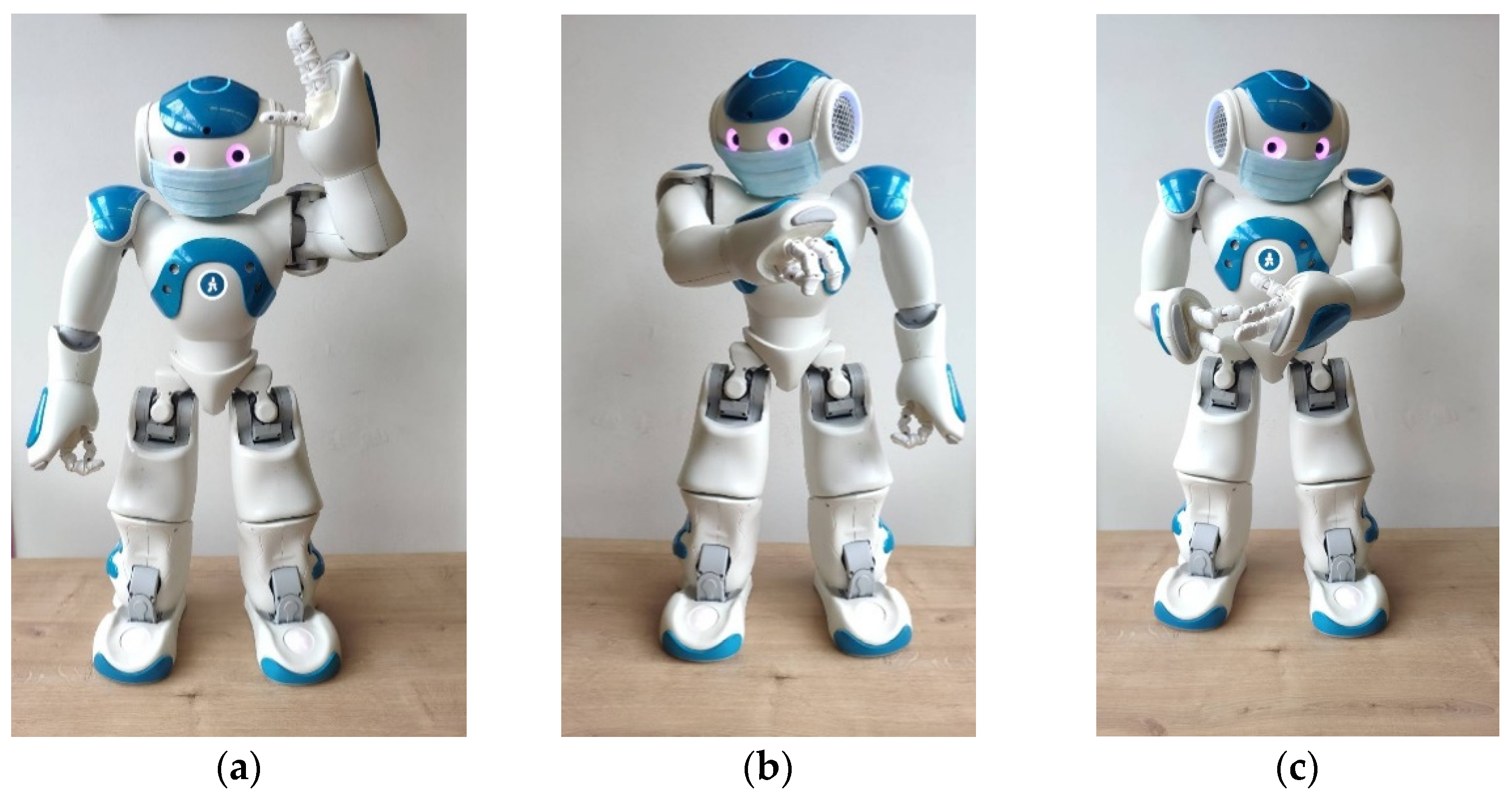
- Presentation of five precautionary measures. The robot describes five actions to prevent the transmission of COVID-19. Each explanation is associated to a corresponding gesture. Measures include the following:
- Correctly wearing a mask;
- Greeting other people without any physical touch;
- Maintaining a distance of at least 1.50 m from other people;
- Sneezing or coughing into the elbow;
- Cleaning hands frequently (with soap or hydroalcoholic gel);
- Summary. To help participants remember better the precautionary measures, the robot gives a short reminder of the five measures previously presented. Nao asks the participants if they have understood everything or if they want the robot to remind them of certain information. A variable amount of time is then set aside for discussion with the participants;
- Conclusion. The robot Nao concludes the presentation by wishing the participants a pleasant day.
2.2.3. Assessment Tools
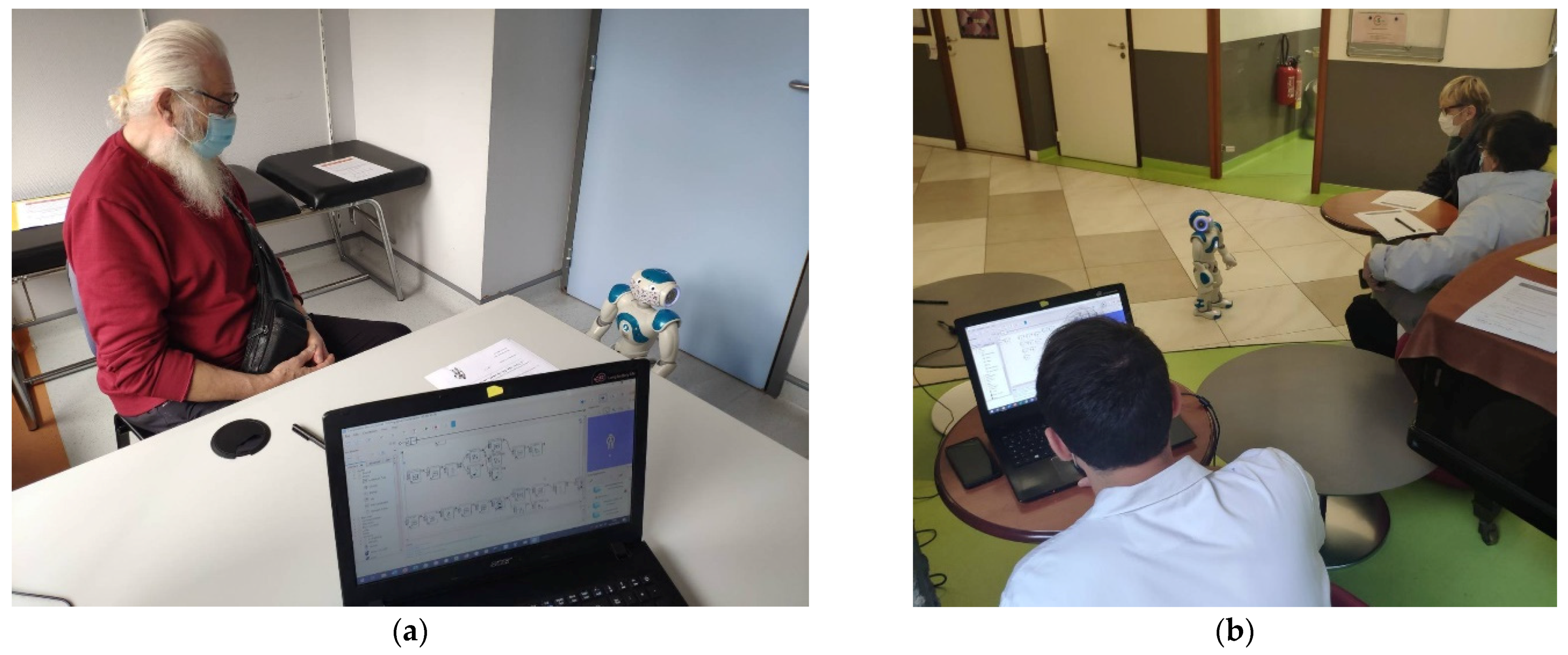
2.3. Procedure
3. Results
3.1. Socio-Demographic Data of Participants
3.2. Dimensions Addressed in the Evaluation
3.2.1. Self-Rated Knowledge of Precautionary Measures
3.2.2. Acceptability of the Robot
3.2.3. Overall Perception of the Activity: Duration and Content
3.2.4. Perceived Usefulness of the Activity
3.2.5. Analysis of the Videos of the NAO Intervention
3.2.6. Analysis of Key Barriers, Enablers, and Recommendations for the Implementation of the Intervention
- Making the robot available in a waiting room while waiting for test results to provide some distraction for patients and accompanying persons and reduce boredom;
- Offering various types of relaxation and leisure activities using the robot to help reduce anxiety and stress for patients and families who come to consult or visit;
- Organizing robotic mediated activities to deal with loneliness and isolation of patients in geriatric or paediatric departments;
- Using social robots to support healthcare workers and reduce their workload;
- Using social robots in the framework of rehabilitation therapies, (e.g., physical activity) or for monitoring vital functions;
- Integrating social robots into educational activities at school with younger audiences.
4. Discussion
4.1. The Feasibility of the Conception and Implementation of the Robot-Mediated Activity
4.2. The Acceptability of the Robot-Mediated Intervention
4.3. Usefulness of the Intervention
4.4. Ethical Issues
- The fact that everyone was free to participate or not in the activity;
- Each person who accepted to participate in the activity, could decide to interact with the robot at the level of involvement he or she wanted (e.g., only observing, responding verbally or non-verbally to the robot, initiating an interaction with the robot, etc.);
- The nature of the robotic tool and the presence of the Wizard of Oz person who handled the robot were clearly explained;
- A methodological limitation in that, overall, ethical issues were not explicitly addressed in the evaluation protocol.
4.5. Recommendations for Robot-Mediated Intervention for Health Prevention
- Define the target population as follows: Inclusion in this kind of activity must privilege older adults who are cognitively healthy or have mild or moderate cognitive impairment, according to the type of information to be provided and the objectives of the activity. The participation of persons with significant communication and/or comprehension impairments should be examined on a case-by-case basis;
- Identify audience needs as follows: Examine the needs of older adults in terms of health information (for instance, precautionary measures for COVID-19 infection) and prepare the contents of the message accordingly;
- Develop HRI scenarios as follows: Develop scenarios combining robot’s speech and gestures. Prepare short, precise, and simple key messages and associate them, if possible, with embodied cues (i.e., a set of gestures and other nonverbal behaviours that convey information and support the speech). Sound effects can be useful to encourage participants’ attention and motivation;
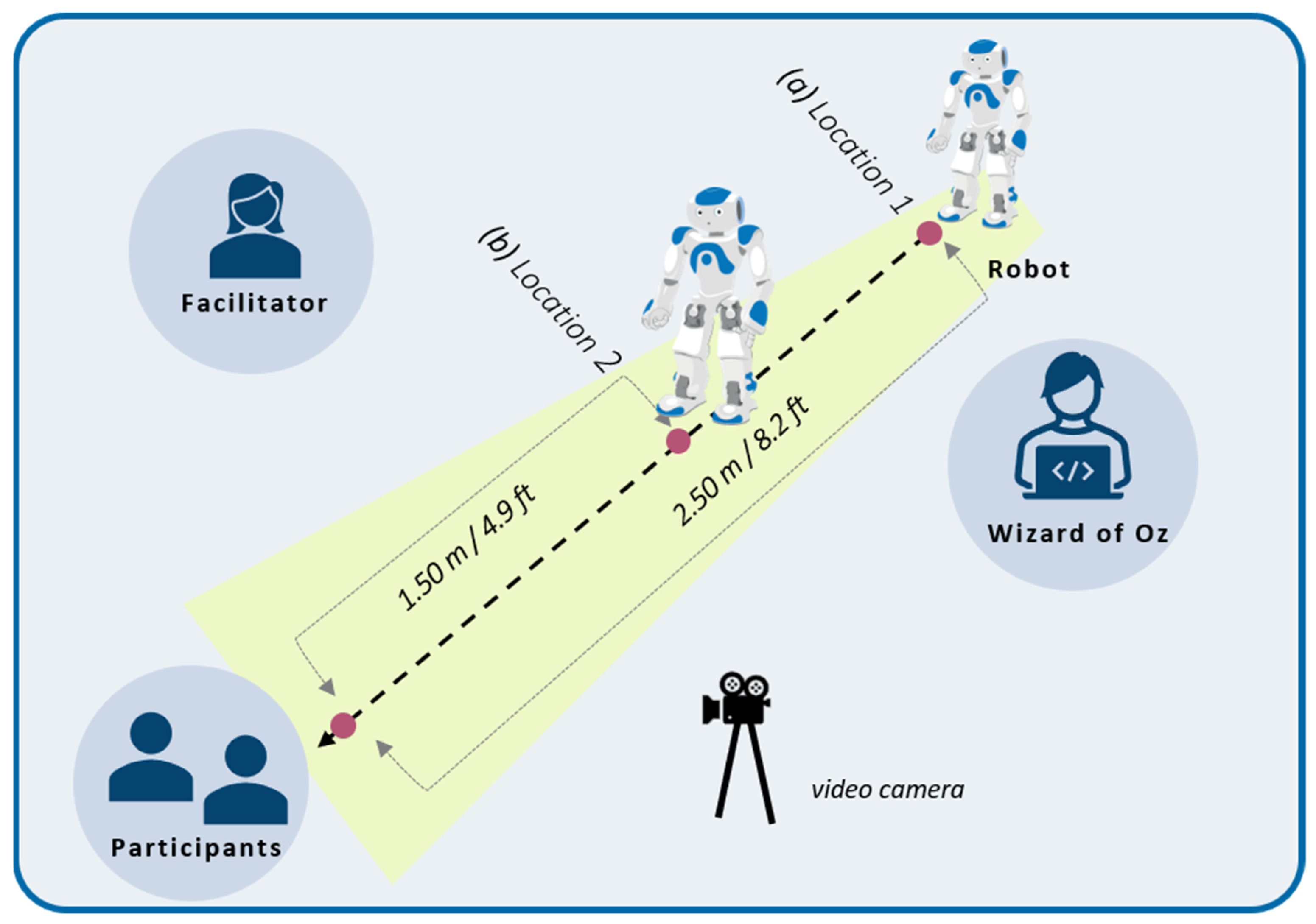
- Preparation of the robot as follows: Program the robot in advance and adapt its voice, speech, and volume for people with potential hearing loss. Make the objects that support the informational message visible and identifiable (for instance, the mask in the case of the COVID-19 precautionary measure scenario). Plan to start the activity with the robot located at 2.50 m away from the participant to allow for a gradual familiarisation with the robot’s presence. After introducing itself, the robot can approach the participant to facilitate visual access to the gestural explanations, up to 1.50 m. Before each activity session, verify the technical aspects that are necessary for the correct use of the robot (e.g., availability of up-to-date software, level of charge batteries, wifi connection, hygiene procedures, etc.);
- Feasibility/acceptability/usefulness testing as follows: Test the feasibility, acceptability, and usefulness of the scenarios with some older adults and implement necessary adaptations to the activity before proposing a large-scale deployment of the activity.
- Create a positive context as follows: Create a pleasant atmosphere between the participant, the facilitator, the Wizard of Oz (if available), and the robot.
- Check consent as follows: Before starting the activity, explain the context and objectives of the session, make sure that participants feel at ease with the robot, and verify that they agree to take part in the activity at its beginning and throughout its course;
- Facilitate understanding and learning as follows: The facilitator plays a key role in promoting participation in the activity session. To favour participants’ understanding and learning, the facilitator should articulate well and observe a sufficiently slow rhythm, check participants’ reactions to verify understanding throughout the session, and rephrase or imitate what the robot says or does when needed. A few simple questions addressed to participants can be integrated throughout the presentation to keep their attention and to encourage the retention of the message;
- Assess pre-and post-learning as follows: in cognitively fit older adults who appreciate challenges, assess knowledge in the health domain before and after the robot activity.
4.6. Limitations of the Study and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lekamwasam, R.; Lekamwasam, S. Effects of COVID-19 Pandemic on Health and Wellbeing of Older People: A Comprehensive Review. Ann. Geriatr. Med. Res. 2020, 24, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Kumar, P.; Singh, S.; Saha, S.; Dey, A.B. Clinical features and outcomes of COVID-19 in older adults: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 321. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef] [PubMed]
- Moline, H.L.; Whitaker, M.; Deng, L.; Rhodes, J.C.; Milucky, J.; Pham, H.; Patel, K.; Anglin, O.; Reingold, A.; Chai, S.J.; et al. Effectiveness of COVID-19 Vaccines in Preventing Hospitalization Among Adults Aged ≥65 Years—COVID-NET, 13 States, February–April 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1088–1093. [Google Scholar] [CrossRef]
- World Health Organization. Considerations for Implementing and Adjusting Public Health and Social Measures in the Context of COVID-19. Interim Guidance 4 November 2020. Available online: https://www.who.int/publications/i/item/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance (accessed on 10 January 2022).
- D’Cruz, M.; Banerjee, D. Caring for Persons Living with Dementia during the COVID-19 Pandemic: Advocacy Perspectives from India. Front. Psychiatry 2020, 11, 603231. [Google Scholar] [CrossRef]
- Elashri, N.I.E.; Elfadawy, H.A.M.; Alam, R.R. Effect of COVID-19 Educational Bag on Knowledge, Attitude and Precautionary Practices of Institutionalized Elderly Persons. Egypt. J. Health Care 2021, 12, 176–194. [Google Scholar] [CrossRef]
- Muruganandam, P.; Neelamegam, S.; Menon, V.; Alexander, J.; Chaturvedi, S.K. COVID-19 and Severe Mental Illness: Impact on patients and its relation with their awareness about COVID-19. Psychiatry Res. 2020, 291, 113265. [Google Scholar] [CrossRef]
- Mazereel, V.; Van Assche, K.; Detraux, J.; De Hert, M. COVID-19 vaccination for people with severe mental illness: Why, what, and how? Lancet Psychiatry 2021, 8, 444–450. [Google Scholar] [CrossRef]
- Lin, T.; Harris, E.A.; Heemskerk, A.; Van Bavel, J.J.; Ebner, N.C. A multi-national test on self-reported compliance with COVID-19 public health measures: The role of individual age and gender demographics and countries’ developmental status. Soc. Sci. Med. 2021, 286, 114335. [Google Scholar] [CrossRef]
- Bearth, A.; Luchsinger, L.; Siegrist, M. Reactions of older Swiss adults to the COVID-19 pandemic: A longitudinal survey on the acceptance of and adherence to public health measures. Soc. Sci. Med. 2021, 280, 114039. [Google Scholar] [CrossRef]
- Chevance, A.; Gourion, D.; Hoertel, N.; Llorca, P.-M.; Thomas, P.; Bocher, R.; Moro, M.-R.; Laprévote, V.; Benyamina, A.; Fossati, P.; et al. Ensuring mental health care during the SARS-CoV-2 epidemic in France: A narrative review. L’Encéphale 2020, 46, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, R.; Hayashi, H.; Kawakatsu, S.; Morioka, D.; Aso, S.; Kimura, M.; Otani, K. Recognition of the coronavirus disease 2019 pandemic and face mask wearing in patients with Alzheimer’s disease: An investigation at a medical centre for dementia in Japan. Psychogeriatrics 2020, 20, 923–925. [Google Scholar] [CrossRef] [PubMed]
- Weirather, R.R. Communication strategies to assist comprehension in dementia. Hawaii Med. J. 2010, 69, 72–74. [Google Scholar] [PubMed]
- Guan, C.; Bouzida, A.; Oncy-Avila, R.M.; Moharana, S.; Riek, L.D. Taking an (Embodied) Cue from Community Health: Designing Dementia Caregiver Support Technology to Advance Health Equity. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; pp. 1–16. [Google Scholar]
- National Health Service Website. Communicating with Someone with Dementia. Available online: https://www.nhs.uk/conditions/dementia/communication-and-dementia/ (accessed on 20 January 2022).
- Mayo Clinic. Alzheimer’s and Dementia: Tips for Better Communication. Available online: https://www.mayoclinic.org/healthy-lifestyle/caregivers/in-depth/alzheimers/art-20047540?reDate=23022022 (accessed on 20 January 2022).
- Alzheimer’s Society. How to Communicate with a Person with Dementia. Available online: https://www.alzheimers.org.uk/about-dementia/symptoms-and-diagnosis/symptoms/how-to-communicate-dementia#content-start (accessed on 20 January 2022).
- Centers for Disease Control and Prevention. Toolkit for People with Disabilities. Available online: https://www.cdc.gov/ncbddd/humandevelopment/covid-19/toolkit-for-people-with-disabilities.html (accessed on 5 February 2022).
- Santé Publique France. Coronavirus. Available online: https://www.santepubliquefrance.fr/l-info-accessible-a-tous/coronavirus (accessed on 5 February 2022).
- Khamis, A.; Meng, J.; Wang, J.; Azar, A.T.; Prestes, E.; Li, H.; Hameed, I.A.; Takács, Á.; Rudas, I.J.; Haidegger, T. Robotics and Intelligent Systems against a Pandemic. Acta Polytech. Hung. 2021, 18, 13–35. [Google Scholar] [CrossRef]
- Avelino, J.; Simão, H.; Ribeiro, R.; Moreno, P.; Figueiredo, R.; Duarte, N.; Odekerken-Schröde, G. Experiments with vizzy as a coach for elderly exercise. In Proceedings of the Workshop Personal Robots Exercising Coaching-HRI Conference (PREC), Chicago, IL, USA, 5 March 2018; pp. 1–6. [Google Scholar]
- Görer, B.; Salah, A.A.; Akın, H.L. An autonomous robotic exercise tutor for elderly people. Auton. Robot. 2017, 41, 657–678. [Google Scholar] [CrossRef]
- Fasola, J.; Mataric, M.J. Using Socially Assistive Human–Robot Interaction to Motivate Physical Exercise for Older Adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]
- Rouaix, N.; Retru-Chavastel, L.; Rigaud, A.-S.; Monnet, C.; Lenoir, H.; Pino, M. Affective and Engagement Issues in the Conception and Assessment of a Robot-Assisted Psychomotor Therapy for Persons with Dementia. Front. Psychol. 2017, 8, 950. [Google Scholar] [CrossRef] [Green Version]
- Winkle, K.; Caleb-Solly, P.; Turton, A.; Bremner, P. Social Robots for Engagement in Rehabilitative Therapies: Design Implications from a Study with Therapists. In Proceedings of the 2018 ACM/IEEE International Conference on Human-Robot Interaction, Chicago, IL, USA, 5–8 March 2018; pp. 289–297. [Google Scholar]
- Chidambaram, V.; Chiang, Y.-H.; Mutlu, B. Designing persuasive robots: How robots might persuade people using vocal and nonverbal cues. In Proceedings of the Seventh Annual ACM/IEEE International Conference on Human-Robot Interaction—HRI ’12, Boston, MA, USA, 5–8 March 2012; Association for Computing Machinery: New York, NY, USA, 2012; Volume 12, pp. 293–300. [Google Scholar]
- Recio, D.L.; Segura, L.M.; Segura, E.M.; Waern, A. The NAO models for the elderly. In Proceedings of the 2013 8th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Tokyo, Japan, 3–6 March 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 187–188. [Google Scholar]
- Shen, Z.; Wu, Y. Investigation of Practical Use of Humanoid Robots in Elderly Care Centres. In Proceedings of the Fourth International Conference on Human Agent Interaction, Singapore, 4–7 October 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 63–66. [Google Scholar]
- Pino, O.; Palestra, G.; Trevino, R.; De Carolis, B. The Humanoid Robot NAO as Trainer in a Memory Program for Elderly People with Mild Cognitive Impairment. Int. J. Soc. Robot. 2020, 12, 21–33. [Google Scholar] [CrossRef]
- Mutlu, B. Designing Embodied Cues for Dialog with Robots. AI Mag. 2011, 32, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Gouaillier, D.; Hugel, V.; Blazevic, P.; Kilner, C.; Monceaux, J.; Lafourcade, P.; Marnier, B.; Serre, J.; Maisonnier, B. The NAO humanoid: A combination of performance and affordability. arXiv 2008, arXiv:0807.3223. [Google Scholar]
- Amirova, A.; Rakhymbayeva, N.; Yadollahi, E.; Sandygulova, A.; Johal, W. 10 Years of Human-NAO Interaction Research: A Scoping Review. Front. Robot. AI 2021, 8, 744526. [Google Scholar] [CrossRef] [PubMed]
- Bouwhuis, D. Current use and possibilities of robots in care. Gerontechnology 2016, 15, 198–208. [Google Scholar] [CrossRef]
- Pot, E.; Monceaux, J.; Gelin, R.; Maisonnier, B.; Robotics, A. Choregraphe: A Graphical Tool for Humanoid Robot Programming. In Proceedings of the RO-MAN 2009-The 18th IEEE International Symposium on Robot and Human Interactive Communication, Toyama, Japan, 27 September–2 October 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 46–51. [Google Scholar] [CrossRef]
- Miskam, M.A.; Shamsuddin, S.; Yussof, H.; Omar, A.R.; Muda, M.Z. Programming platform for NAO robot in cognitive interaction applications. In Proceedings of the 2014 IEEE International Symposium on Robotics and Manufacturing Automation (ROMA), Kuala Lumpur, Malaysia, 15–16 December 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 141–146. [Google Scholar]
- Santé Publique France. Coronavirus: Outils de Prévention Destinés aux Professionnels de Santé et au Grand Public. (Coronavirus: Prevention Tools for Health Professionals and the General Public). Available online: https://www.santepubliquefrance.fr/dossiers/coronavirus-covid-19/coronavirus-outils-de-prevention-destines-aux-professionnels-de-sante-et-au-grand-public (accessed on 7 February 2022).
- Hall, E.T. A System for the Notation of Proxemic Behavior. Am. Anthr. 1963, 65, 1003–1026. [Google Scholar] [CrossRef]
- SoftBank Robotics Europe. Aldebaran Documentation. “Fall Manager”. 2017. Available online: http://doc.aldebaran.com/2-1/naoqi/motion/reflexes-fall-manager.html (accessed on 3 April 2022).
- Riek, L.D. Wizard of Oz Studies in HRI: A Systematic Review and New Reporting Guidelines. J. Human-Robot Interact. 2012, 1, 119–136. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-M.; Mutlu, B. Modeling and Evaluating Narrative Gestures for Humanlike Robots. In Proceedings of the Robotics: Science and Systems IX, Berlin, Germany, 24–28 June 2013; pp. 57–64. [Google Scholar] [CrossRef]
- Werner, K.; Oberzaucher, J.; Werner, F. Evaluation of Human Robot Interaction Factors of a Socially Assistive Robot Together with Older People. In Proceedings of the 6th International Conference on Complex, Intelligent, and Software Intensive Systems, Palermo, Italy, 4–6 July 2012; IEEE: Piscataway, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Torta, E.; Oberzaucher, J.; Werner, F.; Cuijpers, R.H.; Juola, J.F. Attitudes towards Socially Assistive Robots in Intelligent Homes: Results from Laboratory Studies and Field Trials. J. Human-Robot Interact. 2013, 1, 76–99. [Google Scholar] [CrossRef] [Green Version]
- Olde Keizer, R.A.C.M.; Van Velsen, L.; Moncharmont, M.; Riche, B.; Ammour, N.; Del Signore, S.; Zia, G.; Hermens, H.; N’Dja, A. Using socially assistive robots for monitoring and preventing frailty among older adults: A study on usability and user experience challenges. Health Technol. 2019, 9, 595–605. [Google Scholar] [CrossRef] [Green Version]
- Melkas, H.; Hennala, L.; Pekkarinen, S.; Kyrki, V. Human impact assessment of robot implementation in Finnish elderly care. In Proceedings of the International Conference on Serviceology, Tokyo, Japan, 6–8 September 2016; pp. 202–206. [Google Scholar]
- Rudzicz, F.; Wang, R.; Begum, M.; Mihailidis, A. Speech Interaction with Personal Assistive Robots Supporting Aging at Home for Individuals with Alzheimer’s Disease. ACM Trans. Access. Comput. 2015, 7, 1–22. [Google Scholar] [CrossRef]
- Huisman, C.; Kort, H. Two-Year Use of Care Robot Zora in Dutch Nursing Homes: An Evaluation Study. Healthcare 2019, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Khosla, R.; Nguyen, K.; Chu, M.-T. Human Robot Engagement and Acceptability in Residential Aged Care. Int. J. Human-Computer Interact. 2016, 33, 510–522. [Google Scholar] [CrossRef]
- Liang, A.; Piroth, I.; Robinson, H.; MacDonald, B.; Fisher, M.; Nater, U.; Skoluda, N.; Broadbent, E. A Pilot Randomized Trial of a Companion Robot for People with Dementia Living in the Community. J. Am. Med. Dir. Assoc. 2017, 18, 871–878. [Google Scholar] [CrossRef]
- Avioz-Sarig, O.; Olatunji, S.; Sarne-Fleischmann, V.; Edan, Y. Robotic System for Physical Training of Older Adults. Int. J. Soc. Robot. 2021, 13, 1109–1124. [Google Scholar] [CrossRef] [PubMed]
- Young, J.E.; Sung, J.; Voida, A.; Sharlin, E.; Igarashi, T.; Christensen, H.I.; Grinter, R.E. Evaluating Human-Robot Interaction: Focusing on the Holistic Interaction Experience. Int. J. Soc. Robot. 2010, 3, 53–67. [Google Scholar] [CrossRef]
- Heerink, M.; Kröse, B.; Evers, V.; Wielinga, B. Assessing Acceptance of Assistive Social Agent Technology by Older Adults: The Almere Model. Int. J. Soc. Robot. 2010, 2, 361–375. [Google Scholar] [CrossRef] [Green Version]
- McColl, D.; Nejat, G. Meal-Time with a Socially Assistive Robot and Older Adults at a Long-term Care Facility. J. Human-Robot Interact. 2013, 2, 152–171. [Google Scholar] [CrossRef] [Green Version]
- Speros, C. More than Words: Promoting Health Literacy in Older Adults. OJIN: Online J. Issues Nurs. 2009, 14, 5. [Google Scholar] [CrossRef]
- Chesser, A.K.; Woods, N.K.; Smothers, K.; Rogers, N. Health Literacy and Older Adults: A Systematic Review. Gerontol. Geriatr. Med. 2016, 2, 233372141663049. [Google Scholar] [CrossRef] [Green Version]
- Van Gerwen, M.; Alsen, M.; Little, C.; Barlow, J.; Genden, E.; Naymagon, L.; Tremblay, D. Risk factors and outcomes of COVID-19 in New York City; a retrospective cohort study. J. Med. Virol. 2021, 93, 907–915. [Google Scholar] [CrossRef]
- Schnelli, A.; Hirt, J.; Zeller, A. Persons with dementia as internet users: What are their needs? A qualitative study. J. Clin. Nurs. 2020, 30, 849–860. [Google Scholar] [CrossRef]
- Alshammari, M.; Doody, O.; Richardson, I. Barriers to the Access and use of Health Information by Individuals with Intellectual and Developmental Disability IDD: A Review of the Literature. In Proceedings of the 2018 IEEE International Conference on Healthcare Informatics (ICHI), New York, NY, USA, 4–7 June 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 294–298. [Google Scholar]
- Cordasco, K.M.; Homeier, D.C.; Franco, I.; Wang, P.-C.; Sarkisian, C.A. Health literacy screening of geriatric monolingual Spanish-speaking patients using single-item literacy screening questions and education. Health Educ. J. 2012, 71, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Bickmore, T.W.; Pfeifer, L.M.; Byron, D.; Forsythe, S.; Henault, L.E.; Jack, B.; Silliman, R.; Paasche-Orlow, M. Usability of Conversational Agents by Patients with Inadequate Health Literacy: Evidence from Two Clinical Trials. J. Health Commun. 2010, 15, 197–210. [Google Scholar] [CrossRef]
- Sidner, C.L.; Bickmore, T.; Nooraie, B.; Rich, C.; Ring, L.; Shayganfar, M.; Vardoulakis, L. Creating New Technologies for Companionable Agents to Support Isolated Older Adults. ACM Trans. Interact. Intell. Syst. 2018, 8, 1–27. [Google Scholar] [CrossRef]
- Gongor, F.; Tutsoy, O. Social distance measurement algorithm and its aplication to the humanoid robot to halt the pandemic diseases spread. In Proceedings of the 8th International Congress on Engineering, Architecture and Design, North Cyprus, Turkey, 16–17 May 2021. [Google Scholar]
- Sang, H.; Wang, Z.; He, B.; Zhou, Y.; Li, G. A Novel Intelligent Robot for Epidemic Identification and Prevention. In Proceedings of the 2020 IEEE 16th International Conference on Control & Automation (ICCA), Singapore, 9–11 October 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 183–186. [Google Scholar]
- Vandemeulebroucke, T.; de Casterlé, B.D.; Gastmans, C. The use of care robots in aged care: A systematic review of argument-based ethics literature. Arch. Gerontol. Geriatr. 2018, 74, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Parviainen, J.; Pirhonen, J. Vulnerable bodies in human–robot interactions: Embodiment as ethical issue in robot care for the elderly. Transformations 2017, 29, 104–115. [Google Scholar]
- King, M.F.; Bruner, G.C. Social desirability bias: A neglected aspect of validity testing. Psychol. Mark. 2020, 17, 79–103. [Google Scholar] [CrossRef]
- Parker, R.; Baker, D.W.; Williams, M.V.; Nurss, J.R. The test of functional health literacy in adults: A new instrument for measuring patients’ literacy skills. J. Gen. Intern. Med. 1995, 10, 537–541. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimensions | Questions (Answer Modality) |
|---|---|
| Socio-demographic data | Gender (Check box: Female; Male) |
| Year of birth (__|__|__) | |
| Profile (Check box: patients; accompanying persons; professional category for health professionals) | |
| Knowledge of precautionary measures | Do you know the different precautionary measures to protect yourself from COVID-19 infection? (Yes/Moderately/No) |
| Where did you hear about precautionary measures? (Free comments) | |
| Perception of the activity | Did you find the robot-mediated activity long? (Yes/No) |
| Did you find the content of the activity easy to understand (Yes/No, why?/free comments) | |
| Perceived usefulness of the activity | Did you learn anything about precautionary measures (Yes/No) |
| Did you learn anything about technology? (Yes/No) | |
| Did you learn anything else? (If so, what did you learn?/free comments) | |
| Acceptability of the Nao robot | I enjoyed the activity (Yes/No, why?/free comments) |
| I felt confident in this activity (Yes/No, why?/free comments) | |
| I would like to see the Nao robot in another activity (Yes/No) | |
| Other | Do you have any other comments or information to share with us? (Free comments) |
| Dimensions | Questions (Answer Modality) |
|---|---|
| Socio-demographic data | Gender (Check box: Female; Male) |
| Year of birth (__|__|__) | |
| Profession (Free comment) | |
| Knowledge of the Nao robot | Did you already know the Nao robot? (Y/N, If yes, in what context?) |
| Acceptability of the NAO robot | Did you enjoy the activity with the NAO robot? (Y/N/free comments) |
| Perception of the activity | Do you think that the activity is too long for older adults and/or persons with cognitive impairment? (Y/N/free comments) |
| Do you think the activity is understandable for older adults and/or persons with cognitive impairment? (Y/N/free comments) | |
| Perceived usefulness of the activity | Did you learn anything new about precautionary measures? (Y/N/free comments) |
| Did you learn anything about technology? (Y/N/free comments) | |
| Did you learn anything else? (If so, what did you learn?) Do you think that the robot-mediated activity can be useful for the transmission of preventive health information? (Y/N, why?/free comments) | |
| Others | Concerning the overall activity with the Nao robot, do you have any suggestions for improvement? (Free comments) |
| Do you have any other comments or information to share with us? (Free comments) |
| Variables | Modalities | Patients | Accompanying Persons n (%) | Health Professionals n (%) |
|---|---|---|---|---|
| Count | - | 45 (36%) | 39 (32%) | 40 (32%) |
| Gender | Male | 15 (35%) | 14 (35%) | 11 (28%) |
| Female | 30 (65%) | 25 (65%) | 29 (72%) | |
| Age | 64 y/o or younger | 1 (02%) | 21 (54%) | 40 (100%) |
| 65–80 y/o | 13 (29%) | 11 (28%) | 0 | |
| 80–95 y/o | 31 (69%) | 7 (18%) | 0 | |
| Average | 81.57 | 62.90 | 44.56 |
| Variables | Modalities | Patients n (%) | Accompanying Persons n (%) |
|---|---|---|---|
| Do you know the different precautionary measures? | Yes | 27 (60%) | 35 (90%) |
| Partly | 11 (24%) | 3 (08%) | |
| No | 7 (16%) | 1 (02%) | |
| Where did you hear about them? | Public media | 25 (55%) | 20 (51%) |
| Family context | 6 (13%) | 6 (15%) | |
| Work | 0 (0%) | 6 (15%) | |
| Hospital | 7 (15%) | 3 (8%) | |
| Everywhere | 7 (15%) | 4 (10%) |
| Barriers | Enablers |
|---|---|
| Feasibility | |
| Robot’s connection time “The robot is a bit slow to connect.” (professional) Robot’s voice, flow “The robot’s voice is not very understandable.” (patient) “The artificial voice of the robot can be annoying for older adults.” (professional) Robot ‘s annoying noises “The robot makes some annoying engine noises.” (professional) “The footsteps of the robot are unpleasant to hear.” (patient) Robot’s limited gestures “The robot shows Interesting but limited gestures.” (patient) Robot’s small size “The size of the robot a bit small if you want to communicate with it standing up.” (professional) Accessibility issues “People with hearing impairment may have difficulties to understand the robot.” (patient) “The activity may be difficult to follow for people with attention difficulties or other neurocognitive disorders” (professional) “The activity is satisfactory for patients with mild cognitive impairment but more difficult for patients with moderate or severe cognitive deficits.” (professional) | Presence of a facilitator “It is easier to understand the activity with a little additional explanation from the animator.” (patient) “I enjoy the friendly atmosphere created by the animator who conducted the activity” (accompanying person) |
| Acceptability | |
| The robot may generate anxiety “The robot is not very reassuring.” (accompanying person) “I don’t want to trust the robot.” (patient) Fears of technology replacement “The robot does not replace the human person.” (accompanying person) | The robot does not generate anxiety “I feel good and at ease with this robot.” (patient) Robot engagement “The robot captivates me; it is motivating and exciting. ”(patient) “The patients are engaged in the robot activity” (professional) The novelty of the activity “I discover the capabilities of a robot, this a novelty for me. ”(patient) “This new activity changes from the usual explanations ”(patient) “An original way of explaining things.”(accompanying person) Robot social presence “It is adorable this robot, it has a beautiful head, beautiful shape, and he makes you laugh.”(patient) “Nao has an expressive gaze and seems very friendly. ”(patient) “Nao t looks like a friendly child.” (accompanying person) Robot sociability perception “Nao seems very benevolent and sympathetic. ” (patient) “We want to talk and communicate with it.” (patient) “You feel like talking to him.” (accompanying person) |
| Usefulness | |
| Lack of information in the scenario “The scenario lacks images presenting the hygiene products.” (accompanying person) “The activity lacks information about the need to ventilate rooms, for instance opening windows”. (professional) “The need to keep a distance between people is not well explained.”(patient) | Well-structured and simple activity facilitating learning “The messages are short, precise.” (patient) “The message is simple and direct.” (professional) “The gestures are very useful.” (patient) “This activity is motivating and entertaining.” (accompanying person) The activity stimulates cognitive functions “The activity attracts attention, stimulates sensory and executive functions.” (professional) The activity can be adapted to various contexts “This activity is suitable for various audiences and in different contexts (hospital, school).” (patient) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blavette, L.; Rigaud, A.-S.; Anzalone, S.M.; Kergueris, C.; Isabet, B.; Dacunha, S.; Pino, M. A Robot-Mediated Activity Using the Nao Robot to Promote COVID-19 Precautionary Measures among Older Adults in Geriatric Facilities. Int. J. Environ. Res. Public Health 2022, 19, 5222. https://doi.org/10.3390/ijerph19095222
Blavette L, Rigaud A-S, Anzalone SM, Kergueris C, Isabet B, Dacunha S, Pino M. A Robot-Mediated Activity Using the Nao Robot to Promote COVID-19 Precautionary Measures among Older Adults in Geriatric Facilities. International Journal of Environmental Research and Public Health. 2022; 19(9):5222. https://doi.org/10.3390/ijerph19095222
Chicago/Turabian StyleBlavette, Lauriane, Anne-Sophie Rigaud, Salvatore Maria Anzalone, Clément Kergueris, Baptiste Isabet, Sébastien Dacunha, and Maribel Pino. 2022. "A Robot-Mediated Activity Using the Nao Robot to Promote COVID-19 Precautionary Measures among Older Adults in Geriatric Facilities" International Journal of Environmental Research and Public Health 19, no. 9: 5222. https://doi.org/10.3390/ijerph19095222
APA StyleBlavette, L., Rigaud, A. -S., Anzalone, S. M., Kergueris, C., Isabet, B., Dacunha, S., & Pino, M. (2022). A Robot-Mediated Activity Using the Nao Robot to Promote COVID-19 Precautionary Measures among Older Adults in Geriatric Facilities. International Journal of Environmental Research and Public Health, 19(9), 5222. https://doi.org/10.3390/ijerph19095222