
Effects of a Cool-Down after Supramaximal Interval Exercise on Autonomic Modulation

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
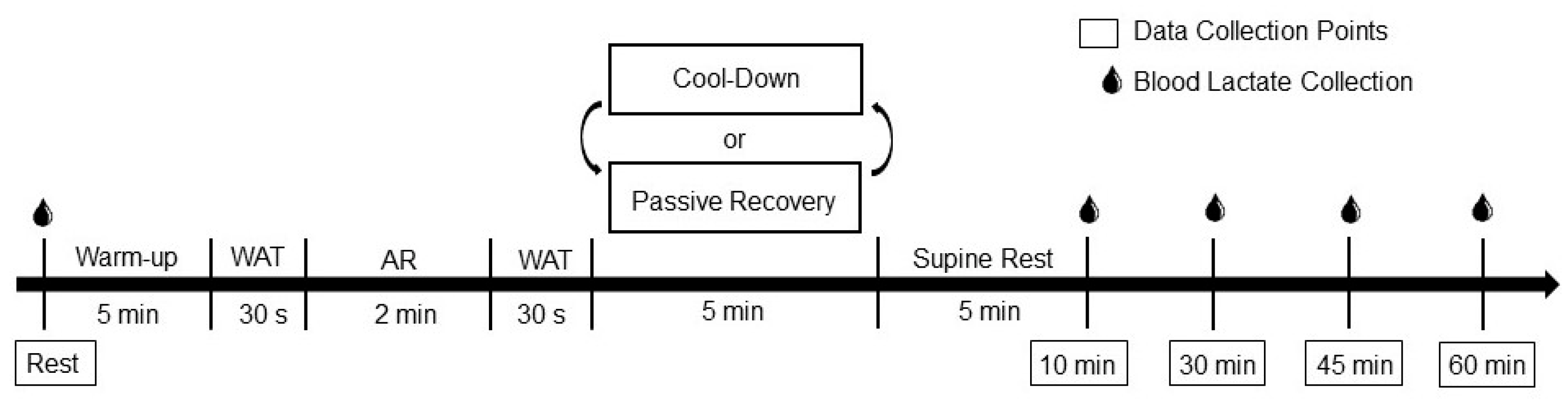
2.2. Study Design
2.3. Anthropometrics
2.4. Autonomic Modulation
2.5. Blood Lactate
2.6. Supramaximal Interval Exercise
2.7. Statistical Analysis
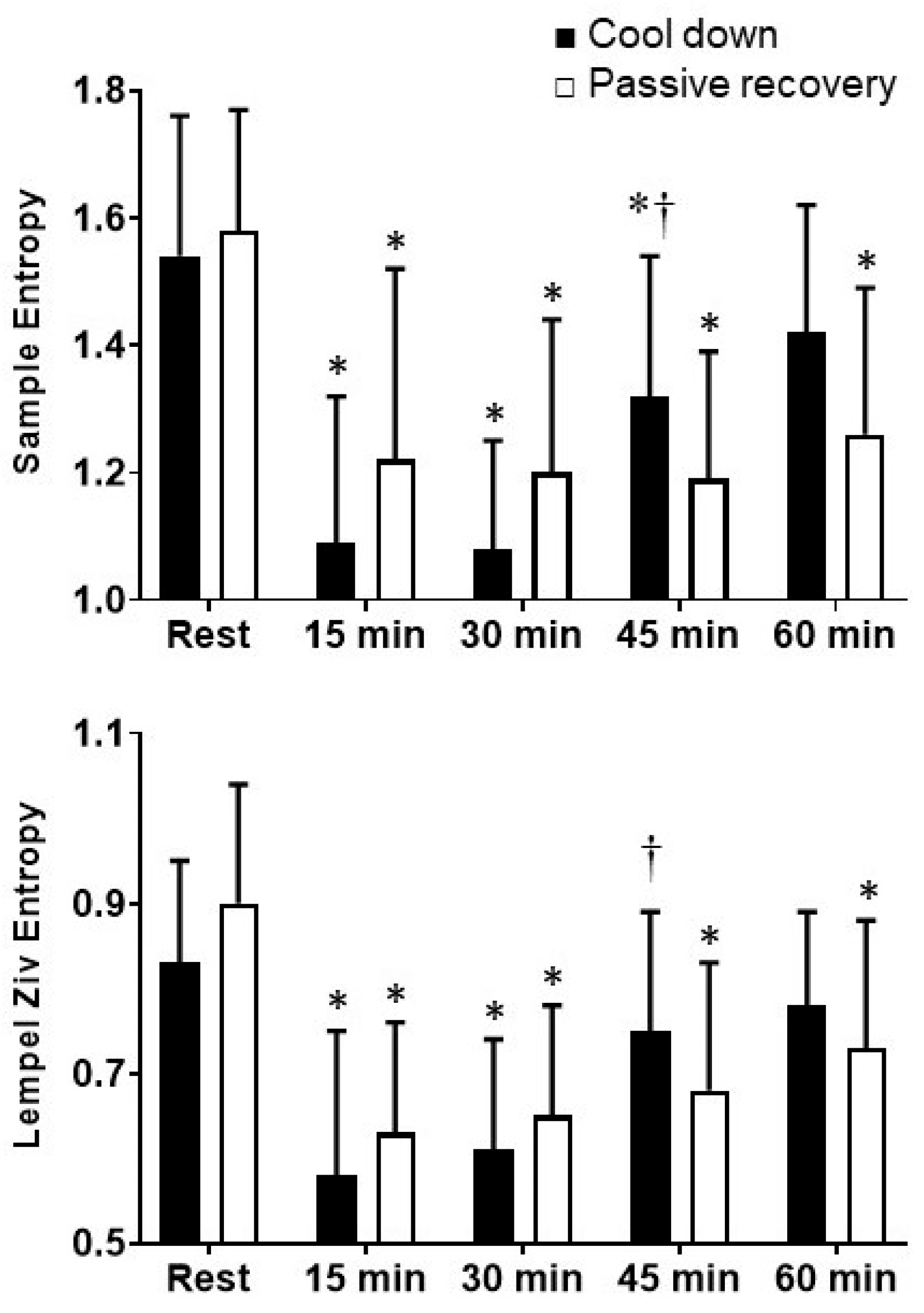
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rakobowchuk, M.; Tanguay, S.; Burgomaster, K.A.; Howarth, K.R.; Gibala, M.J.; MacDonald, M.J. Sprint interval and traditional endurance training induce similar improvements in peripheral arterial stiffness and flow-mediated dilation in healthy humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R236–R242. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, J.; Komine, H.; Miyazawa, T.; Imai, T.; Ogoh, S. Influence of single bout of aerobic exercise on aortic pulse pressure. Eur. J. Appl. Physiol. 2015, 115, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Rodas, G.; Ventura, J.L.; Cadefau, J.A.; Cussó, R.; Parra, J. A short training programme for the rapid improvement of both aerobic and anaerobic metabolism. Eur. J. Appl. Physiol. 2000, 82, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Millar, P.J.; Rakobowchuk, M.; McCartney, N.; MacDonald, M.J. Heart rate variability and nonlinear analysis of heart rate dynamics following single and multiple Wingate bouts. Appl. Physiol. Nutr. Metab. 2009, 34, 875–883. [Google Scholar] [CrossRef]
- Stuckey, M.I.; Tordi, N.; Mourot, L.; Gurr, L.J.; Rakobowchuk, M.; Millar, P.J.; Toth, R.; MacDonald, M.J.; Kamath, M.V. Autonomic recovery following sprint interval exercise. Scand. J. Med. Sci. Sports 2012, 22, 756–763. [Google Scholar] [CrossRef]
- Perkins, S.E.; Jelinek, H.F.; Al-Aubaidy, H.A.; de Jong, B. Immediate and long term effects of endurance and high intensity interval exercise on linear and nonlinear heart rate variability. J. Sci. Med. Sport 2017, 20, 312–316. [Google Scholar] [CrossRef]
- Albert, C.M.; Mittleman, M.A.; Chae, C.U.; Lee, I.M.; Hennekens, C.H.; Manson, J.E. Triggering of sudden death from cardiac causes by vigorous exertion. N. Engl. J. Med. 2000, 343, 1355–1361. [Google Scholar] [CrossRef]
- Tuzcu, V.; Nas, S.; Borklu, T.; Ugur, A. Decrease in the heart rate complexity prior to the onset of atrial fibrillation. Europace 2006, 8, 398–402. [Google Scholar] [CrossRef]
- Vikman, S.; Mäkikallio, T.H.; Yli-Mäyry, S.; Pikkujämsä, S.; Koivisto, A.-M.; Reinikainen, P.; Airaksinen, K.J.; Huikuri, H.V. Altered complexity and correlation properties of RR interval dynamics before the spontaneous onset of paroxysmal atrial fibrillation. Circulation 1999, 100, 2079–2084. [Google Scholar] [CrossRef] [Green Version]
- Riebe, D.; Ehrman, J.; Liguori, G.; Magal, M. American College of Sports Medicine’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017. [Google Scholar]
- Takahashi, T.; Okada, A.; Hayano, J.; Tamura, T. Influence of cool-down exercise on autonomic control of heart rate during recovery from dynamic exercise. Front. Med. Biol. Eng. 2002, 11, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Forjaz, C.L.; Cardoso, C.G., Jr.; Rezk, C.C.; Santaella, D.F.; Tinucci, T. Postexercise hypotension and hemodynamics: The role of exercise intensity. J. Sports Med. Phys. Fit. 2004, 44, 54–62. [Google Scholar]
- Rakobowchuk, M.; Stuckey, M.I.; Millar, P.J.; Gurr, L.; Macdonald, M.J. Effect of acute sprint interval exercise on central and peripheral artery distensibility in young healthy males. Eur. J. Appl. Physiol. 2009, 105, 787–795. [Google Scholar] [CrossRef]
- Kingsley, J.D.; Tai, Y.L.; Vaughan, J.A.; Mayo, X. High-intensity interval cycling exercise on wave reflection and pulse wave velocity. J. Strength Cond. Res. 2016, 31, 1313–1320. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Jacobs, D.R., Jr.; Leon, A.S. Validity and reliability of self-reported physical activity status: The Lipid Research Clinics questionnaire. Med. Sci. Sports Exerc. 1993, 25, 92–98. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Malik, M. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use: Task force of the European society of cardiology and the north American society for pacing and electrophysiology. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.-S.; Roy, R.J.; Jensen, E.W. EEG complexity as a measure of depth of anesthesia for patients. IEEE Trans. Biomed. Eng. 2001, 48, 1424–1433. [Google Scholar] [CrossRef]
- Lempel, A.; Ziv, J. On the complexity of finite sequences. IEEE Trans. Biomed. Eng. 1976, 22, 75–81. [Google Scholar] [CrossRef]
- Kanaley, J.; Goulopoulou, S.; Franklin, R.; Baynard, T.; Holmstrup, M.; Carhart Jr, R.; Weinstock, R.; Fernhall, B. Plasticity of heart rate signalling and complexity with exercise training in obese individuals with and without type 2 diabetes. Int. J. Obes. 2009, 33, 1198. [Google Scholar] [CrossRef] [Green Version]
- Tanner, R.K.; Fuller, K.L.; Ross, M.L. Evaluation of three portable blood lactate analysers: Lactate Pro, Lactate Scout and Lactate Plus. Eur. J. Appl. Physiol. 2010, 109, 551–559. [Google Scholar] [CrossRef]
- Bar-Or, O. The Wingate anaerobic test. An update on methodology, reliability and validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Keppel, G. Design and Analysis: A Researcher’s Handbook, 4th ed.; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 1991. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Martin, N.A.; Zoeller, R.F.; Robertson, R.J.; Lephart, S.M. The comparative effects of sports massage, active recovery, and rest in promoting blood lactate clearance after supramaximal leg exercise. J. Athl. Train. 1998, 33, 30–35. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Indicators | |
|---|---|
| Age (y) | 23 ± 3 |
| Height (m) | 1.76 ± 0.10 |
| Weight (kg) | 74.6 ± 13.7 |
| BMI (kg·m2) | 24.0 ± 2.7 |
| Cool Down | Passive Recovery | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rest | 15 min | 30 min | 45 min | 60 min | Rest | 15 min | 30 min | 45 min | 60 min | |
| Heart rate (bpm) | 58 ± 8 | 91 ± 9 * | 81 ± 9 * | 73 ± 9 * | 71 ± 8 * | 59 ± 8 | 90 ± 10 * | 82 ± 10 * | 75 ± 9 * | 72 ± 10 * |
| Total power (ln ms2) | 8.5 ± 0.9 | 5.8 ± 0.9 * | 6.9 ± 0.9 * | 7.5 ± 1.0 * | 7.6 ± 1.0 * | 8.8 ± 0.9 | 5.9 ± 1.1 * | 6.9 ± 1.2 * | 7.7 ± 1.1 * | 7.8 ± 0.9 * |
| LF (ln ms2) | 6.8 ± 0.6 | 4.2 ± 0.7 * | 5.4 ± 0.9 * | 6.1 ± 1.2 * | 6.2 ± 0.8 * | 7.3 ± 0.9 | 4.1 ± 0.9 * | 5.6 ± 1.2 * | 6.1 ± 0.7 * | 6.2 ± 0.6 * |
| HF (ln ms2) | 8.0 ± 1.0 | 3.8 ± 1.3 * | 4.8 ± 1.8 * | 5.8 ± 1.6 * | 6.4 ± 1.4 * | 8.0 ± 1.1 | 4.1 ± 1.4 * | 4.7 ± 1.6 * | 5.7 ± 1.6 * | 6.1 ± 1.5 * |
| LF/HF ratio (ln) | 3.5 ± 0.6 | 5.1 ± 0.9 * | 5.2 ± 1.2 *‡ | 4.9 ± 1.1 * | 4.4 ± 1.0 * | 3.9 ± 0.7 | 4.7 ± 1.0 * | 5.5 ± 1.1 * | 5.1 ± 1.1 * | 4.7 ± 1.1 * |
| RMSSD (ln ms) | 4.5 ± 0.5 | 2.3 ± 0.7 * | 2.9 ± 0.8 * | 3.4 ± 0.8 * | 3.6 ± 0.7 * | 4.5 ± 0.6 | 2.3 ± 0.9 * | 2.8 ± 0.8 * | 3.3 ± 0.8 * | 3.6 ± 0.8 * |
| Blood lactate (mmol) | 0.6 ± 0.2 | 11.1 ± 1.8 *# | 6.7 ± 1.7 *# | 4.2 ± 1.1 *# | 2.8 ± 0.8 *# | 0.7 ± 0.3 | 13.0 ± 2.0 * | 8.3 ± 2.2 * | 5.2 ± 1.4 * | 3.3 ± 1.0 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parks, J.C.; Marshall, E.M.; Humm, S.M.; Erb, E.K.; Kingsley, J.D. Effects of a Cool-Down after Supramaximal Interval Exercise on Autonomic Modulation. Int. J. Environ. Res. Public Health 2022, 19, 5407. https://doi.org/10.3390/ijerph19095407
Parks JC, Marshall EM, Humm SM, Erb EK, Kingsley JD. Effects of a Cool-Down after Supramaximal Interval Exercise on Autonomic Modulation. International Journal of Environmental Research and Public Health. 2022; 19(9):5407. https://doi.org/10.3390/ijerph19095407
Chicago/Turabian StyleParks, Jason C., Erica M. Marshall, Stacie M. Humm, Emily K. Erb, and J. Derek Kingsley. 2022. "Effects of a Cool-Down after Supramaximal Interval Exercise on Autonomic Modulation" International Journal of Environmental Research and Public Health 19, no. 9: 5407. https://doi.org/10.3390/ijerph19095407
APA StyleParks, J. C., Marshall, E. M., Humm, S. M., Erb, E. K., & Kingsley, J. D. (2022). Effects of a Cool-Down after Supramaximal Interval Exercise on Autonomic Modulation. International Journal of Environmental Research and Public Health, 19(9), 5407. https://doi.org/10.3390/ijerph19095407