
Lifestyle Profiles and Their Sociodemographic Correlate in an Academic Community Sample

 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Lifestyle Measures
2.2.1. Diet
2.2.2. Physical Activity
2.2.3. Cigarette Smoking
2.2.4. Alcohol Consumption
2.3. Data Analysis
3. Results
3.1. Description of Lifestyles
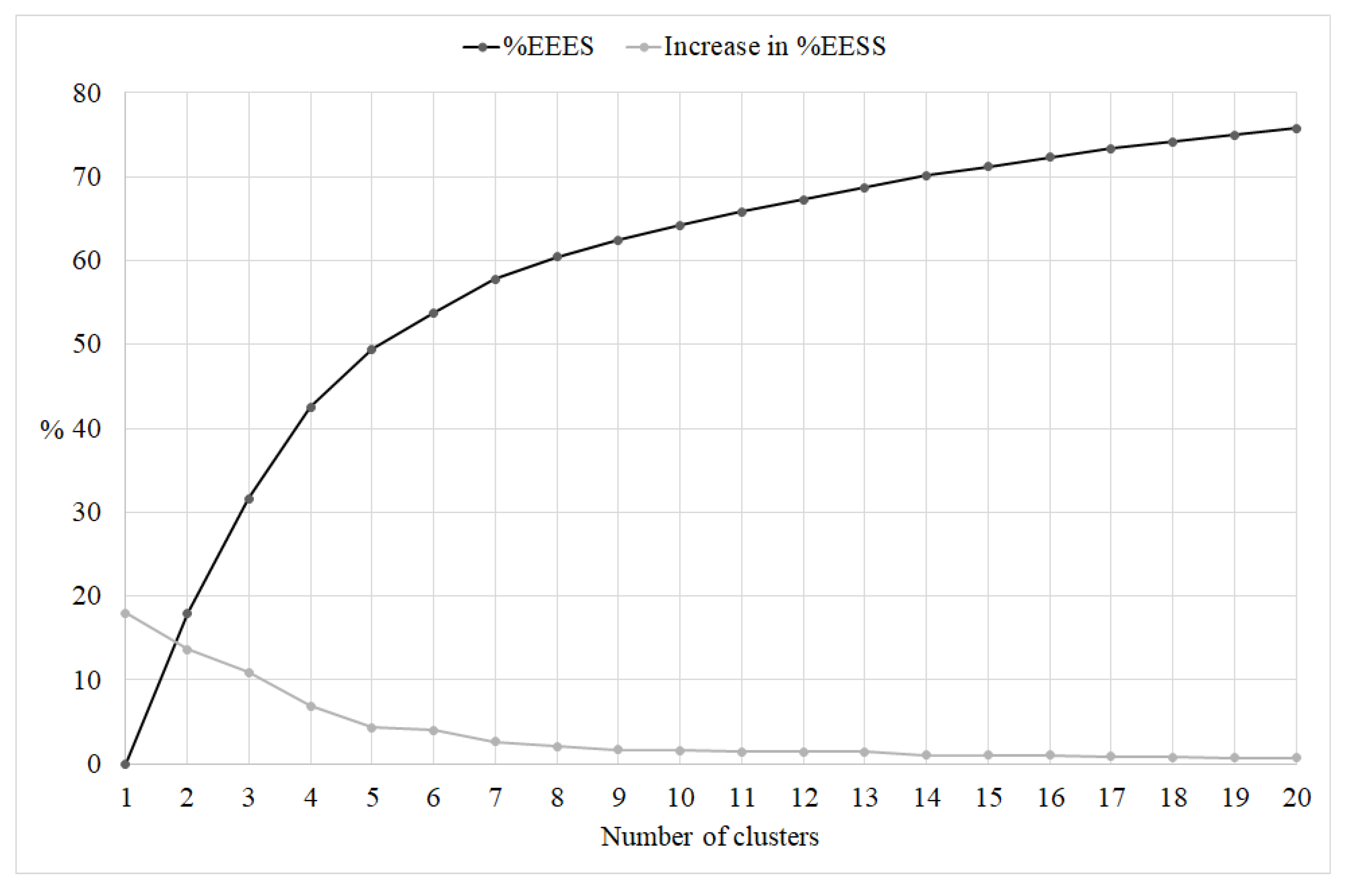
3.2. Identification of Lifestyle Profiles
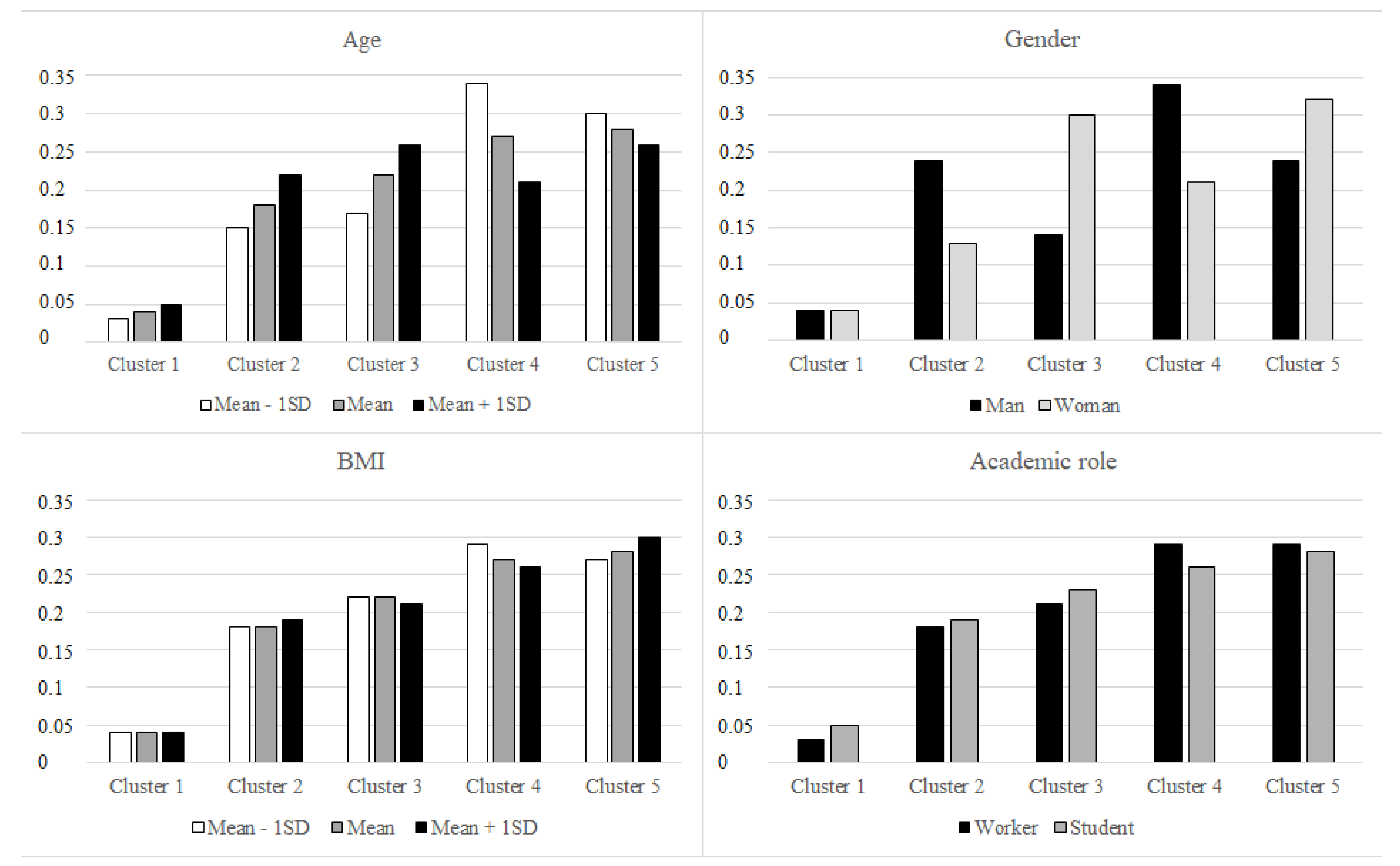
3.3. Associations between Lifestyle Profile and Sociodemographic Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; et al. Impact of Healthy Lifestyle Factors on Life Expectancies in the US Population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Adorni, R.; Zanatta, F.; D’Addario, M.; Atella, F.; Costantino, E.; Iaderosa, C.; Petarle, G.; Steca, P. Health-Related Lifestyle Profiles in Healthy Adults: Associations with Sociodemographic Indicators, Dispositional Optimism, and Sense of Coherence. Nutrients 2021, 13, 3778. [Google Scholar] [CrossRef] [PubMed]
- Mawditt, C.; Sacker, A.; Britton, A.; Kelly, Y.; Cable, N. The clustering of health-related behaviours in a British population sample: Testing for cohort differences. Prev. Med. 2016, 88, 95–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 657. [Google Scholar] [CrossRef] [Green Version]
- Morris, L.J.; D’Este, C.; Sargent-Cox, K.; Anstey, K.J. Concurrent lifestyle risk factors: Clusters and determinants in an Australian sample. Prev. Med. 2016, 84, 1–5. [Google Scholar] [CrossRef]
- Noble, N.; Paul, C.; Turon, H.; Oldmeadow, C. Which modifiable health risk behaviours are related? A systematic review of the clustering of Smoking, Nutrition, Alcohol and Physical activity (‘SNAP’) health risk factors. Prev. Med. 2015, 81, 16–41. [Google Scholar] [CrossRef]
- Rabel, M.; Laxy, M.; Thorand, B.; Peters, A.; Schwettmann, L.; Mess, F. Clustering of Health-Related Behavior Patterns and Demographics. Results From the Population-Based KORA S4/F4 Cohort Study. Front. Public Health 2018, 6, 387. [Google Scholar] [CrossRef] [Green Version]
- De Vries, H.; van’t Riet, J.; Spigt, M.; Metsemakers, J.; van den Akker, M.; Vermunt, J.K.; Kremers, S. Clusters of lifestyle behaviors: Results from the Dutch SMILE study. Prev. Med. 2008, 46, 203–208. [Google Scholar] [CrossRef]
- McAloney, K.; Graham, H.; Law, C.; Platt, L. A scoping review of statistical approaches to the analysis of multiple health-related behaviours. Prev. Med. 2013, 56, 365–371. [Google Scholar] [CrossRef]
- Okanagan Charter: An International Charter for Health Promoting Universities & Colleges. Available online: https://open.library.ubc.ca/cIRcle/collections/53926/items/1.0132754 (accessed on 25 June 2022).
- Magnusson, D. The Logic and Implications of a Person-Oriented Approach. In Methods and Models for Studying the Individual; Cairns, R.B., Bergman, L.R., Kagan, J., Eds.; Sage Publications, Inc.: Newbury Park, CA, USA, 1998; pp. 33–64. [Google Scholar]
- Indagine Multiscopo Sulle Famiglie: Aspetti Della Vita Quotidiana—Parte Generale. Available online: https://www.istat.it/it/archivio/91926 (accessed on 3 October 2022).
- World Health Organization (WHO). Healthy Diet: Key Facts. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 25 January 2022).
- Ministero Della Salute Linee Guida per Una Sana Alimentazione. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=2915 (accessed on 25 June 2022).
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EpiCentro Sorveglianza Passi. Available online: https://www.epicentro.iss.it/passi/ (accessed on 25 June 2022).
- EpiCentro Attività fisica: Parametri e Livelli Consigliati e Ricadute Sullo Stato di Salute. Available online: https://www.epicentro.iss.it/attivita_fisica/livelli-consigliati (accessed on 6 December 2022).
- Physical Activity. Available online: http://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 25 June 2022).
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.-O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Il Consumo di Alcol in Italia. Available online: https://www.istat.it/it/archivio/198903 (accessed on 3 October 2022).
- Vargha, A.; Torma, B.; Bergman, L.R. ROPstat: A general statistical package useful for conducting person-oriented analysis. J. Pers. Res. 2015, 1, 87–98. [Google Scholar] [CrossRef] [Green Version]
- Bergman, L.R.; Nurmi, J.-E.; Eye, A.A. von I-States-as-Objects-Analysis (ISOA): Extensions of an Approach to Studying Short-Term Developmental Processes by Analyzing Typical Patterns. Int. J. Behav. Dev. 2012, 36, 237–246. [Google Scholar] [CrossRef]
- Bergman, L.R.; Magnusson, D.; El Khouri, B.M. Studying Individual Development in an Interindividual Context: A Person-Oriented Approach; Psychology Press: London, UK, 2003. [Google Scholar]
- Mahoney, J.L.; Stattin, H.; Magnusson, D. Youth recreation centre participation and criminal offending: A 20-year longitudinal study of Swedish boys. Int. J. Behav. Dev. 2001, 25, 509–520. [Google Scholar] [CrossRef]
- Braverman, M.T.; Ceraso, M.; Sporrer, F.; Rockler, B.E. Five-year changes in support for tobacco control policy options among students, faculty and staff at a public university. Prev. Med. 2020, 142, 106359. [Google Scholar] [CrossRef]
- Aceijas, C.; Waldhäusl, S.; Lambert, N.; Cassar, S.; Bello-Corassa, R. Determinants of health-related lifestyles among university students. Perspect. Public Health 2016, 137, 227–236. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Arent, S.; Schoenfeld, B.J.; Stout, J.R.; Campbell, B.; Wilborn, C.D.; Taylor, L.; Kalman, D.; Smith-Ryan, A.E.; Kreider, R.B.; et al. International society of sports nutrition position stand: Nutrient timing. J. Int. Soc. Sport. Nutr. 2017, 14, 33. [Google Scholar] [CrossRef]
- Vitale, K.; Getzin, A. Nutrition and Supplement Update for the Endurance Athlete: Review and Recommendations. Nutrients 2019, 11, 1289. [Google Scholar] [CrossRef] [Green Version]
- Gallus, S.; Pacifici, R.; Colombo, P.; La Vecchia, C.; Garattini, S.; Apolone, G.; Zuccaro, P. Tobacco dependence in the general population in Italy. Ann. Oncol. 2005, 16, 703–706. [Google Scholar] [CrossRef]
- Martins, J.; Marques, A.; Gouveia, R.; Carvalho, F.; Sarmento, H.; Valeiro, M.G. Participation in Physical Education Classes and Health-Related Behaviours among Adolescents from 67 Countries. Int. J. Environ. Res. Public Health 2022, 19, 955. [Google Scholar] [CrossRef] [PubMed]
- Carballo-Fazanes, A.; Rico-Díaz, J.; Barcala-Furelos, R.; Rey, E.; Rodríguez-Fernández, J.E.; Varela-Casal, C.; Abelairas-Gómez, C. Physical Activity Habits and Determinants, Sedentary Behaviour and Lifestyle in University Students. Int. J. Environ. Res. Public Health 2020, 17, 3272. [Google Scholar] [CrossRef] [PubMed]
- Erol, A.; Karpyak, V.M. Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug Alcohol Depend. 2015, 156, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Belingheri, M.; Facchetti, R.; Scordo, F.; Butturini, F.; Turato, M.; De Vito, G.; Cesana, G.; Riva, M.A. Risk behaviors among Italian healthcare students: A cross-sectional study for health promotion of future healthcare workers. Med. Lav. 2019, 110, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, C.S. Sex-dependent differences in voluntary physical activity. J. Neurosci. Res. 2016, 95, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Deforche, B.; Van Dyck, D.; Deliens, T.; De Bourdeaudhuij, I. Changes in weight, physical activity, sedentary behaviour and dietary intake during the transition to higher education: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deliens, T.; Deforche, B.; De Bourdeaudhuij, I.; Clarys, P. Determinants of physical activity and sedentary behaviour in university students: A qualitative study using focus group discussions. BMC Public Health 2015, 15, 201. [Google Scholar] [CrossRef] [Green Version]
- Riebe, D.; Greene, G.W.; Ruggiero, L.; Stillwell, K.M.; Blissmer, B.; Nigg, C.R.; Caldwell, M. Evaluation of a Healthy-Lifestyle Approach to Weight Management. Prev. Med. 2003, 36, 45–54. [Google Scholar] [CrossRef]
- Brown, A.; Flint, S.W.; Batterham, R.L. Pervasiveness, impact and implications of weight stigma. eClinicalMedicine 2022, 47, 101408. [Google Scholar] [CrossRef]
- Paulhus, D.L.; Vazire, S. The Self-Report Method. Handbook of Research Methods in Personality Psychology; The Guilford Press: New York, NY, USA, 2007; Volume 1, pp. 224–239. [Google Scholar]
- Cotten, E.; Prapavessis, H. Increasing Nonsedentary Behaviors in University Students Using Text Messages: Randomized Controlled Trial. JMIR Mhealth Uhealth 2016, 4, e99. [Google Scholar] [CrossRef]
- Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Academic Role | Gender | n (%) | Response Rate (%) | Age Mean (SD) Range | BMI Mean (SD) Range |
|---|---|---|---|---|---|
| Students | Males | 2101 (24.1) | 15.9 | 23 (5.07) 18–68 | 23 (2.87) 15–35 |
| Females | 5272 (60.5) | 25.6 | 23 (4.89) 18–67 | 21 (3.06) 13–35 | |
| Administrative technical staff | Males | 146 (1.7) | 45.9 | 45 (8.74) 24–64 | 25 (2.88) 19–32 |
| Females | 292 (3.4) | 57.5 | 46 (8.92) 21–66 | 23 (3.56) 17–33 | |
| Ph.D. students, research fellows, postgraduates | Males | 177 (2) | 44.5 | 30 (5.55) 19–56 | 23 (2.87) 17–33 |
| Females | 286 (3.3) | 66.5 | 30 (5.45) 19–55 | 21 (2.76) 16–34 | |
| Researchers, professors | Males | 213 (2.4) | 38.0 | 49 (10.18) 28–76 | 25 (2.93) 19–34 |
| Females | 228 (2.6) | 55.9 | 50 (9.13) 27–75 | 22 (3.06) 16–32 |
| Diet | Physical Activity | Smoking | Alcohol Consumption | |
|---|---|---|---|---|
| Mean (SD) | 11.18 (2.55) | 2.24 (1.89) | 9.68 (1.03) | 8.02 (1.00) |
| Range | 3–18 | 0–9 | 1–10 | 2.5–9 |
| Skewness (SE) | −0.11 (0.03) | 0.65 (0.03) | −4.11 (0.03) | −1.25 (0.03) |
| Kurtosis (SE) | −0.35 (0.05) | 0.11 (0.05) | 19.07 (0.05) | 1.69 (0.05) |
| Behavior’s classification | NA = 25.7% Suff-A = 70.2% Fully A = 4.1% | NA = 36.4% A = 57.6% Intensive = 6.0% | NA = 13.5% A = 86.5% | NA = 31.9% A = 68.1% |
| 5 Clusters | 6 Clusters | Best Solution | |
|---|---|---|---|
| %EESS | 57.24 | 59.83 | 6 clusters |
| Point-biserial correlation coefficient | 0.318 | 0.319 | 6 clusters |
| Modified Xie-Beni index | 0.492 | 0.541 | 5 clusters |
| Silhouette Coefficient | 0.575 | 0.572 | 5 clusters |
| Weighted mean of cluster homogeneity coefficients (HC, weights are cluster sizes) | 0.856 | 0.804 | 5 clusters |
| % Healthy Lifestyles | |||||||
|---|---|---|---|---|---|---|---|
| Cl | n (%) | Mean Age (SD) | n Male (%) | Diet | Physical Activity | Cigarette Smoking | Alcohol Consumption |
| 1 | 393 (4.5%) | 27.65 (10.28) | 127 (32.3%) | 227 a (57.8%) 12 b (3.1%) | 188 c (47.8%) 10 d (2.5%) | 0 (0%) | 171 (43.5%) |
| 2 | 1445 (16.6%) | 27.67 (10.65) | 649 (44.9%) | 1083 (74.9%) 29 (2.0%) | 1002 (69.3%) 46 (3.2%) | 1108 (76.7%) | 0 (0%) |
| 3 | 2210 (25.4%) | 27.41 (10.22) | 377 (17.1%) | 1960 (88.7%) 250 (11.3%) | 1173 (53.1%) 0 (0%) | 2079 (94.1%) | 1948 (88.1%) |
| 4 | 2094 (24.0%) | 24.37 (7.26) | 839 (40.1%) | 1755 (83.8%) 64 (3.1%) | 1628 (77.7%) 466 (22.3%) | 1972 (94.2%) | 1648 (78.7%) |
| 5 | 2573 (29.5%) | 25.13 (8.29) | 645 (25.1%) | 1094 (42.5%) 0 (0%) | 1031 (40.1%) 0 (0%) | 2380 (92.5%) | 2167 (84.2%) |
| 95% CI | 95% CI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | Cluster Pairs | Log Odds Ratio | Lower | Upper | SE | Z | p | Odds Ratio | Lower | Upper |
| Age | 1 vs. 4 | 0.06 | 0.04 | 0.07 | 0.01 | 6.62 | <0 .001 | 1.06 | 1.04 | 1.07 |
| 1 vs. 5 | 0.04 | 0.02 | 0.05 | 0.01 | 4.81 | <0.001 | 1.04 | 1.02 | 1.05 | |
| 2 vs. 4 | 0.04 | 0.03 | 0.06 | 0.01 | 7.58 | <0.001 | 1.05 | 1.03 | 1.06 | |
| 2 vs. 5 | 0.03 | 0.02 | 0.04 | 0.01 | 5.18 | <0.001 | 1.03 | 1.02 | 1.04 | |
| 3 vs. 4 | 0.05 | 0.04 | 0.06 | 0.01 | 9.19 | <0.001 | 1.05 | 1.04 | 1.06 | |
| 3 vs. 5 | 0.03 | 0.02 | 0.04 | 0.00 | 7.10 | <0.001 | 1.03 | 1.02 | 1.04 | |
| 4 vs. 5 | −0.02 | −0.03 | −0.01 | 0.01 | −3.05 | 0.002 | 0.98 | 0.97 | 0.99 | |
| Gender | 1 vs. 2 | 0.57 | 0.32 | 0.81 | 0.13 | 4.50 | <0.001 | 1.76 | 1.38 | 2.26 |
| 1 vs. 3 | −0.80 | −1.05 | −0.55 | 0.13 | −6.27 | <0.001 | 0.45 | 0.35 | 0.58 | |
| 1 vs. 4 | 0.47 | 0.23 | 0.71 | 0.12 | 3.80 | <0.001 | 1.59 | 1.25 | 2.03 | |
| 1 vs. 5 | −0.30 | −0.54 | −0.06 | 0.12 | −2.47 | 0.014 | 0.74 | 0.58 | 0.94 | |
| 2 vs. 3 | −1.36 | −1.52 | −1.21 | 0.08 | −16.91 | <0.001 | 0.26 | 0.22 | 0.30 | |
| 2 vs. 5 | −0.87 | −1.01 | −0.73 | 0.07 | −11.86 | <0.001 | 0.42 | 0.36 | 0.48 | |
| 3 vs. 4 | 1.26 | 1.11 | 1.41 | 0.08 | 16.70 | <0.001 | 3.54 | 3.05 | 4.10 | |
| 3 vs. 5 | 0.49 | 0.35 | 0.64 | 0.08 | 6.55 | <0.001 | 1.64 | 1.41 | 1.90 | |
| 4 vs. 5 | −0.77 | −0.90 | −0.64 | 0.07 | −11.52 | <0.001 | 0.46 | 0.41 | 0.53 | |
| AR | 1 vs. 4 | 0.51 | 0.08 | 0.94 | 0.22 | 2.31 | 0.021 | 1.66 | 1.08 | 2.56 |
| BMI | 1 vs. 4 | 0.05 | 0.01 | 0.08 | 0.02 | 2.55 | 0.011 | 1.05 | 1.01 | 1.09 |
| 2 vs. 4 | 0.03 | 0.01 | 0.05 | 0.01 | 2.42 | 0.016 | 1.03 | 1.01 | 1.05 | |
| 4 vs. 5 | −0.03 | −0.05 | −0.01 | 0.01 | −3.11 | 0.002 | 0.97 | 0.95 | 0.99 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adorni, R.; Lonati, E.; Zanatta, F.; Belingheri, M.; Rossetti, M.; Colleoni, M.; Riva, M.A.; Palestini, P.; Steca, P. Lifestyle Profiles and Their Sociodemographic Correlate in an Academic Community Sample. Int. J. Environ. Res. Public Health 2023, 20, 231. https://doi.org/10.3390/ijerph20010231
Adorni R, Lonati E, Zanatta F, Belingheri M, Rossetti M, Colleoni M, Riva MA, Palestini P, Steca P. Lifestyle Profiles and Their Sociodemographic Correlate in an Academic Community Sample. International Journal of Environmental Research and Public Health. 2023; 20(1):231. https://doi.org/10.3390/ijerph20010231
Chicago/Turabian StyleAdorni, Roberta, Elena Lonati, Francesco Zanatta, Michael Belingheri, Massimiliano Rossetti, Matteo Colleoni, Michele Augusto Riva, Paola Palestini, and Patrizia Steca. 2023. "Lifestyle Profiles and Their Sociodemographic Correlate in an Academic Community Sample" International Journal of Environmental Research and Public Health 20, no. 1: 231. https://doi.org/10.3390/ijerph20010231
APA StyleAdorni, R., Lonati, E., Zanatta, F., Belingheri, M., Rossetti, M., Colleoni, M., Riva, M. A., Palestini, P., & Steca, P. (2023). Lifestyle Profiles and Their Sociodemographic Correlate in an Academic Community Sample. International Journal of Environmental Research and Public Health, 20(1), 231. https://doi.org/10.3390/ijerph20010231