
The TELE-DD Randomised Controlled Trial on Treatment Adherence in Patients with Type 2 Diabetes and Comorbid Depression: Clinical Outcomes after 18-Month Follow-Up

 , , ,
, , ,
Abstract
:1. Introduction
Background
2. Materials and Methods
3. Results
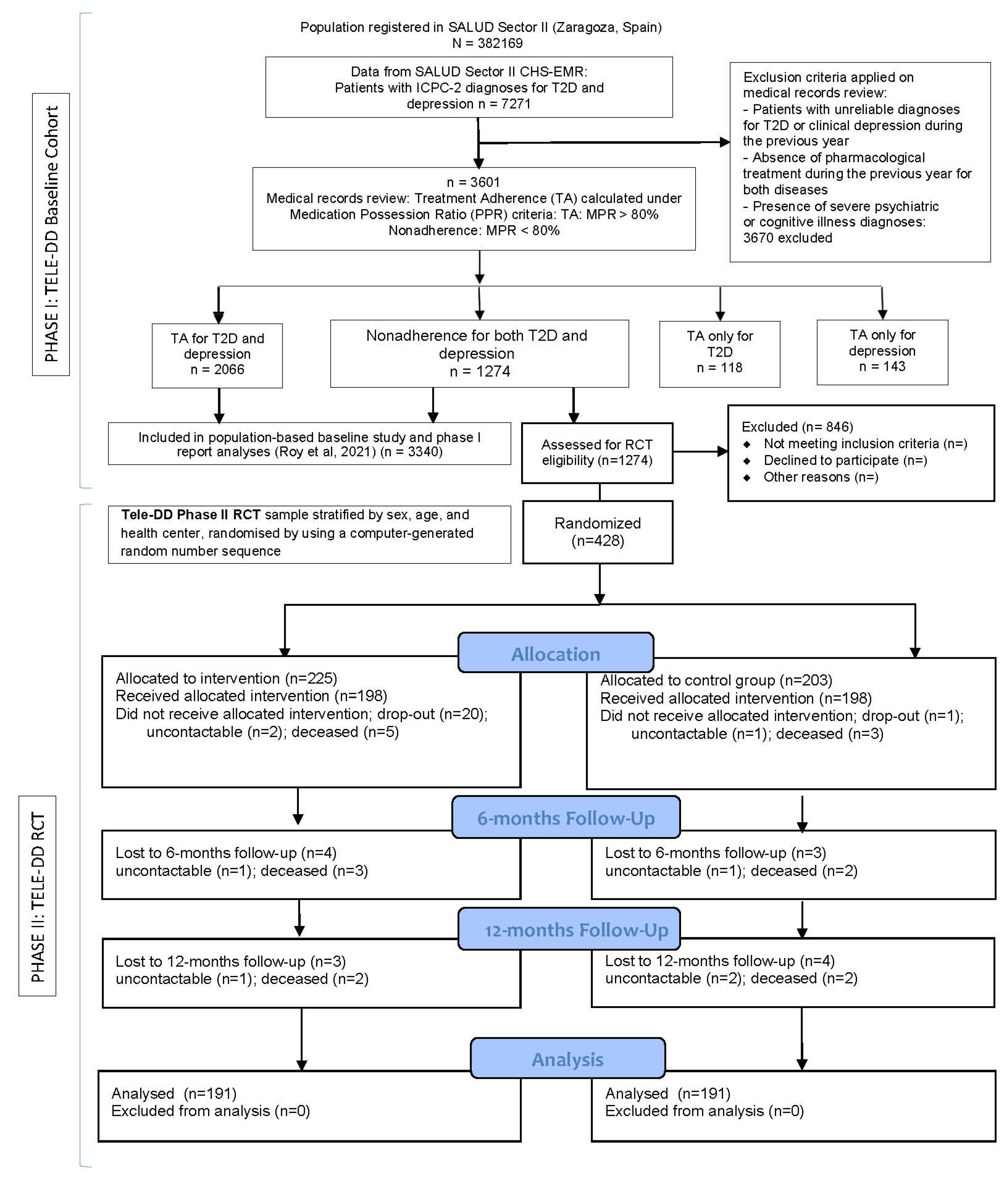
3.1. Characteristics of the RCT Sample
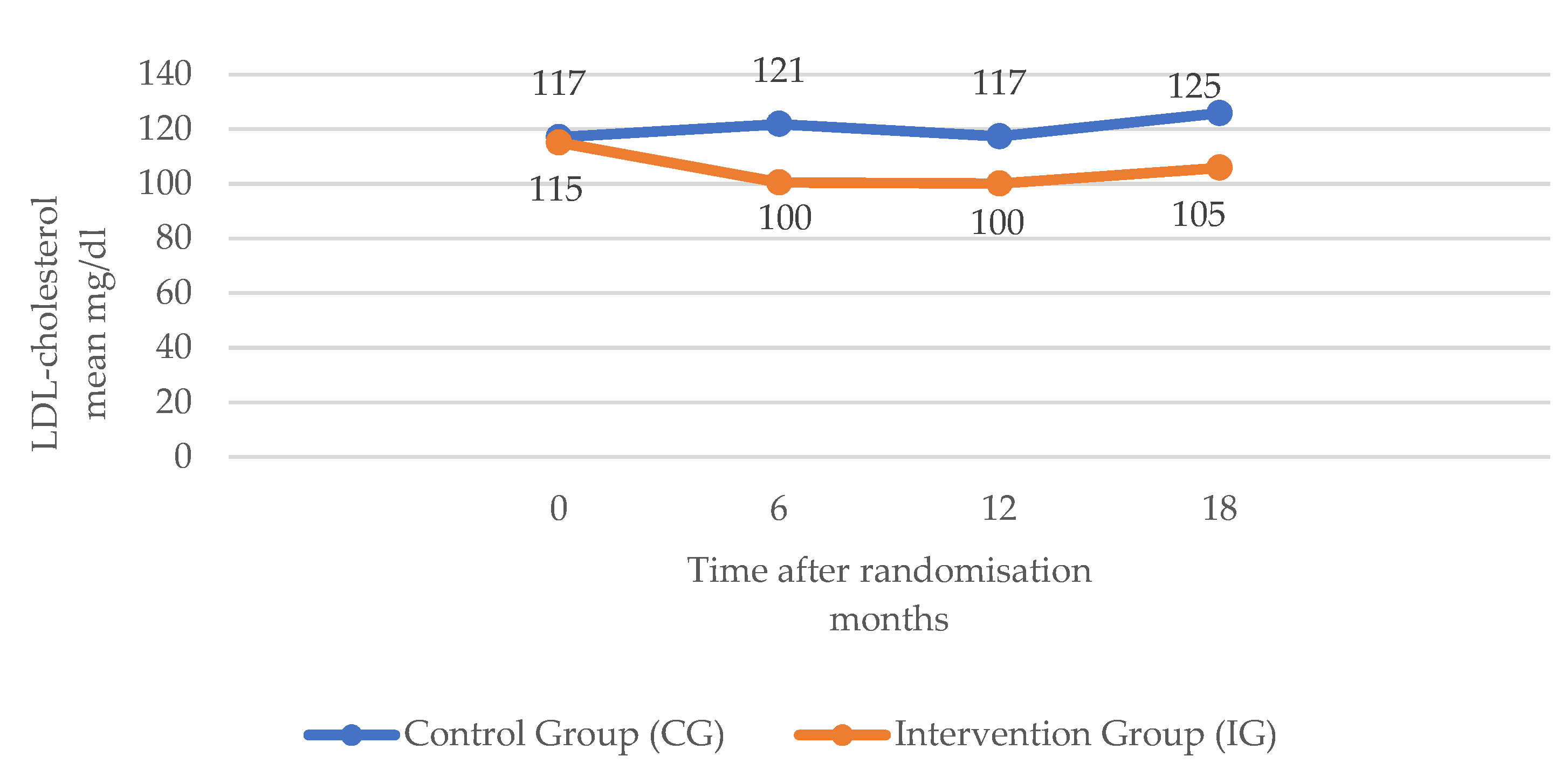
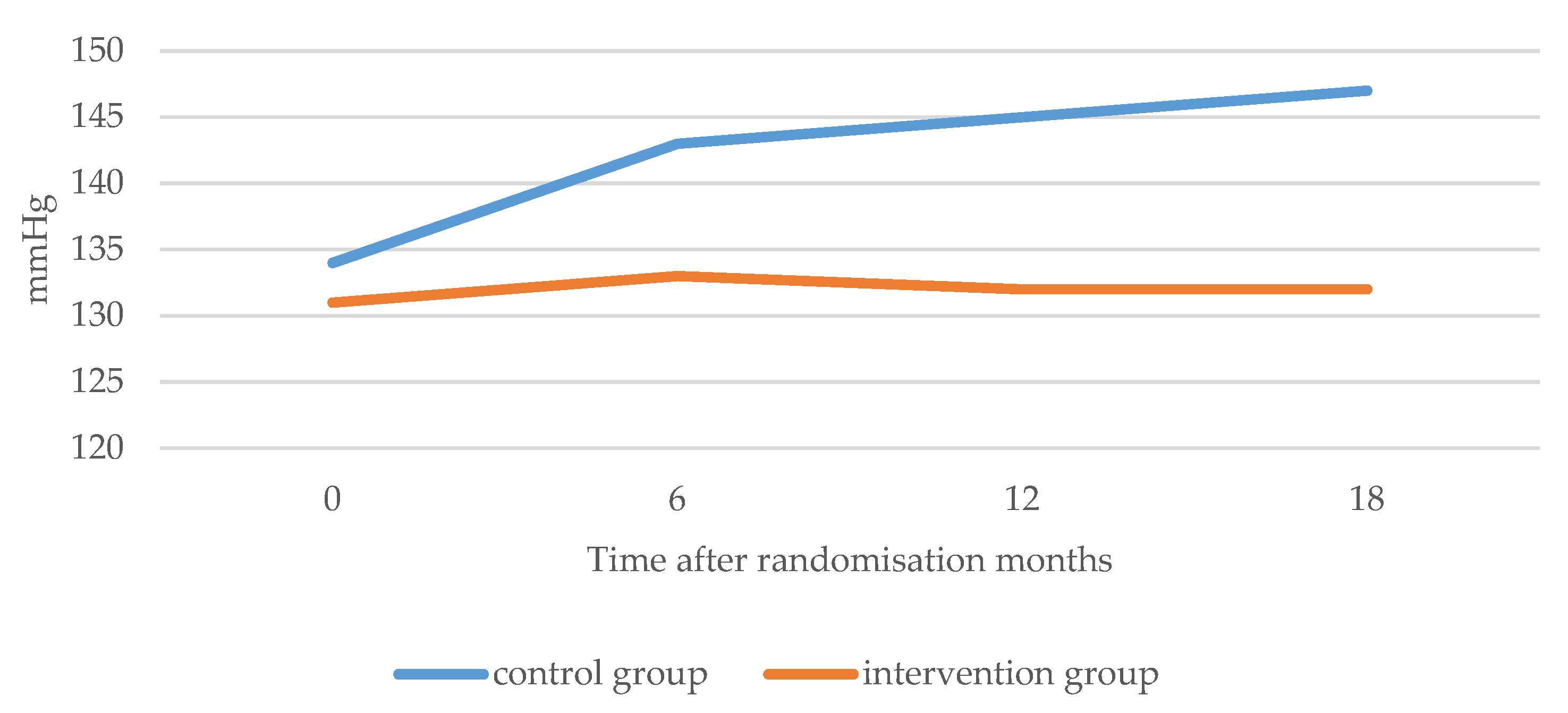
3.2. Metabolic Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global Estimates for the Prevalence of Diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, M.H.; Bojer, A.S.; Broadbent, D.A.; Plein, S.; Madsen, P.L.; Gæde, P. Cardiac Perfusion, Structure, and Function in Type 2 Diabetes Mellitus with and without Diabetic Complications. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study at 30 Years: Overview. Diabetes Care 2014, 37, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De-la-Camara, C.; Gracia-Garcia, P.; Roy, J.F.; Santabarbara, J.; Lopez-Anton, R.; Campayo, A. Influence of gender on baseline characteristics of depression and future risk for incident stroke an elderly population: Results from the ZARADEMP project. J. Psychosom. Res. 2010, 68, 618–628. [Google Scholar]
- Jaakko, T.; Jaana, L.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar]
- Dilla, T.; Amparo, V.; Luis, L.; José, A.S. Treatment Adherence and Persistence: Causes, Consequences and Improvement Strategies. Aten. Primaria 2009, 41, 342–348. [Google Scholar] [CrossRef] [Green Version]
- De Jonge, P.R. Prevalent and incident depression in community-dwelling elderly persons with diabetes mellitus: Results from the ZARADEMP project. Diabetologia 2006, 49, 2627–2633. [Google Scholar] [CrossRef] [Green Version]
- Campayo, A.D. Depressive disorder and incident diabetes mellitus: The effect of characteristics of depression. Am. J. Psychiatry 2010, 167, 580–588. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Stone, M.A.; Peters, J.L.; Davies, M.J.; Khunti, K. The Prevalence of Co-Morbid Depression in Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabet. Med. 2006, 23, 1165–1173. [Google Scholar] [CrossRef]
- Krapek, K.; King, K.; Warren, S.S.; George, K.G.; Caputo, D.A.; Mihelich, K.; Holst, E.M.; Nichol, M.B.; Shi, S.G.; Livengood, K.B.; et al. Medication Adherence and Associated Hemoglobin A1c in Type 2 Diabetes. Ann. Pharmacother. 2004, 38, 1357–1362. [Google Scholar] [CrossRef]
- .Gonzalez, J.S.; Peyrot, M.; McCarl, L.A.; Collins, E.M.; Serpa, L.; Mimiaga, M.J.; Safren, S.A. Depression and Diabetes Treatment Nonadherence: A Meta-Analysis. Diabetes Care 2008, 31, 2398–2403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santabarbara, J.; Roy, J.F.; De-la-Camara, C.; Gracia-Garcia, P.; Lopez-Anton, R.; Martin, A. History of stroke, incident depressive disorder and competing risk of death. J. Psychosom. Res. 2010, 68, 662–668. [Google Scholar]
- Roy, J.F.; De la Camara, C.; Saz, P.; Martin, A.; Quintanilla, M.A.; Lobo-Escolar, A.; Lobo, A. Psychosomatic implications in the longitudinal study of late-life depression in the community: The ZARADEMP project. J. Psychosom. Res. 2008, 64, 671–679. [Google Scholar]
- Hoogendoorn, C.J.; Roy, J.F.; Gonzalez, J.S. Shared dysregulation of homeostatic brain-body pathways in depression and type 2 diabetes. Curr. Diabetes Rep. 2017, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Nicolucci, A.; Burns, K.K.; Holt, R.I.G.; Comaschi, M.; Hermanns, N.; Ishii, H.; Kokoszka, A.; Pouwer, F.; Skovlund, S.E.; Stuckey, H.; et al. Diabetes Attitudes, Wishes and Needs Second Study (DAWN2TM): Cross-National Benchmarking of Diabetes-Related Psychosocial Outcomes for People with Diabetes. Diabet. Med. 2013, 30, 767–777. [Google Scholar] [CrossRef]
- Hoogendoorn, C.J.; Shapira, A.; Roy, J.F.; Walker, E.A.; Cohen, H.W.; Gonzalez, J.S. Depressive symptom dimensions and medication non-adherence in suboptimally controlled type 2 diabetes. J. Diabetes Its Complicat. 2019, 33, 217–222. [Google Scholar] [CrossRef]
- Roy, J.F.; del Hoyo, M.L.L.; Urcola-Pardo, F.; Monreal-Bartolomé, A.; Ruiz, D.C.G.; Borao, M.M.G.; Alcázar, A.B.A.; Casbas, J.P.M.; Casas, A.A.; Funcia, M.T.A.; et al. The TELE-DD Project on Treatment Nonadherence in the Population with Type 2 Diabetes and Comorbid Depression. Sci. Rep. 2021, 11, 8889. [Google Scholar] [CrossRef]
- Al-Hayek, A.A.; Robert, A.A.; Alzaid, A.A.; Nusair, H.M.; Zbaidi, N.S.; Al-Eithan, M.H.; Sam, A.E. Association between Diabetes Self-Care, Medication Adherence, Anxiety, Depression, and Glycaemic Control in Type 2 Diabetes. Saudi Med. J. 2012, 33, 681–683. [Google Scholar]
- Horne, R.; Chapman, S.C.E.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding Patients’ Adherence-Related Beliefs about Medicines Prescribed for Long-Term Conditions: A Meta-Analytic Review of the Necessity-Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar] [CrossRef]
- World Health Organization. 2022. Available online: https://www.who.int/standards/classifications/other-classifications/international-classification-of-primary-care (accessed on 23 August 2022).
- Grant, S.; Mayo-Wilson, E.; Montgomery, P.; Macdonald, G.; Michie, S.; Hopewell, S.; Moher, D.; Aber, J.L.; Altman, D.; Bhui, K.; et al. CONSORT-SPI 2018 Explanation and Elaboration: Guidance for Reporting Social and Psychological Intervention Trials. Trials 2018, 19, 406. [Google Scholar] [CrossRef] [Green Version]
- Juste, A.M.; Miguel, A.G.; Plou, B.P.; Rubio, F.G.; Pascual-Salcedo, M.M.A.; Menditto, E.; Torres, A.P. Adherence to treatment of hypertension, hypercholesterolaemia and diabetes in an elderly population of a Spanish cohort. Med. Clínica 2019, 153, 1–5. [Google Scholar]
- Andrade, S.E.; Kahler, K.H.; Frech, F.; Chan, K.A. Methods for Evaluation of Medication Adherence and Persistence Using Automated Databases. Pharmacoepidemiol. Drug Saf. 2006, 15, 565–574. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, M.; Teeling, M.; Bennett, K. The Prevalence and Ingredient Cost of Chronic Comorbidity in the Irish Elderly Population with Medication Treated Type 2 Diabetes: A Retrospective Cross-Sectional Study Using a National Pharmacy Claims Database. BMC Health Serv. Res. 2013, 13, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Standards of Medical Care in Diabetes—2015 Abridged for Primary Care Providers. Clin. Diabetes 2015, 33, 97–111. [Google Scholar] [CrossRef] [Green Version]
- Saleem, T.; Mohammad, K.H.; Abdel-Fattah, M.M.; Abbasi, A.H. Association of glycosylated haemoglobin level and diabetes mellitus duration with the severity of coronary artery disease. Diabetes Vasc. Dis. Res. 2008, 5, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Catapano, A.L.; Reiner, Ž.; de Backer, G.; Graham, I.; Taskinen, M.-R.; Wiklund, O.; Agewall, S.; Alegria, E.; Chapman, M.J.; Durrington, P.; et al. ESC/EAS Guidelines for the Management of Dyslipidaemias. Atherosclerosis 2011, 217 (Suppl. S1), S1–S44. [Google Scholar] [CrossRef]
- Roy, J.F.; Santabarbara, J.; De-la-Camara, C.; Gracia-Garcia, P.; Lopez-Anton, R.; Ventura, T. Cardiovascular burden and long-term risk of first-ever depression: Implications for the vascular depression hypothesis from a population-based study. J. Psychosom. Res. 2010, 68, 661–669. [Google Scholar]
- Owens-Gary, M.D.; Zhang, X.; Jawanda, S.; Bullard, K.M.K.; Allweiss, P.; Smith, B.D. The Importance of Addressing Depression and Diabetes Distress in Adults with Type 2 Diabetes. J. Gen. Intern. Med. 2019, 34, 320–324. [Google Scholar] [CrossRef] [Green Version]
- Santos, I.S.; Tavares, B.F.; Munhoz, T.N.; de Almeida, L.S.P.; da Silva, N.T.B.; Tams, B.D.; Patella, A.M.; Matijasevich, A. Sensibilidade e Especificidade Do Patient Health Questionnaire-9 (PHQ-9) Entre Adultos Da População Geral. Cad. De Saude Publica 2013, 29, 1533–1543. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Fisher, L.; Earles, J.; Dudl, R.J.; Lees, J.; Mullan, J.; Jackson, R.A. Assessing Psychosocial Distress in Diabetes Development of the Diabetes Distress Scale. Diabetes Care 2005, 28, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Hoogendoorn, C.J. Diabetes distress and quality of life in adults with diabetes. In Behavioral Diabetes. Ecological Perspectives; Springer: Cham, Switzerland, 2020; pp. 303–328. [Google Scholar]
- Lobo-Escolar, A.; Roy, J.F.; Saz, P.; De-la-Cámara, C.; Marcos, G.; Lobo, A. Association of Hypertension with Depression in Community-Dwelling Elderly Persons: Results from the ZARADEMP Project. Psychother. Psychosom. 2008, 77, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Grossman, A.; Grossman, E. Blood Pressure Control in Type 2 Diabetic Patients. Cardiovasc. Diabetol. 2017, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chireh, B.; D’Arcy, C. Shared and Unique Risk Factors for Depression and Diabetes Mellitus in a Longitudinal Study, Implications for Prevention: An Analysis of a Longitudinal Population Sample Aged ≥45 Years. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819865828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, M.A.; Bardsley, J.; Cypress, M.; Duker, P.; Funnell, M.M.; Fischl, A.H.; Maryniuk, M.D.; Siminerio, L.; Vivian, E. Diabetes Self-Management Education and Support in Type 2 Diabetes: A Joint Position Statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Diabetes Care 2015, 38, 1372–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marqués de·Sá, J.P. Applied Statistics: Using SPSS, STATISTICA, and MATLAB; Springer: Cham, Switzerland, 2013. [Google Scholar]
- Patel, P.J.; Hayward, K.L.; Rudra, R.; Horsfall, L.U.; Hossain, F.; Williams, S.; Johnson, T.; Brown, N.N.; Saad, N.; Clouston, A.D.; et al. Multimorbidity and polypharmacy in diabetic patients with NAFLD: Implications for disease severity and management. Medicine 2017, 96, e6761. [Google Scholar] [CrossRef]
- Johnson, J.A.; Al Sayah, F.; Wozniak, L.; Rees, S.; Soprovich, A.; Chik, C.L.; Chue, P.; Florence, P.; Jacquier, J.; Lysak, P.; et al. Controlled trial of a collaborative primary care team model for patients with diabetes and depression: Rationale and design for a comprehensive evaluation. BMC Health Serv. Res. 2012, 12, 258. [Google Scholar] [CrossRef] [Green Version]
- Katon, W.J.; Lin, E.H.; Von Korff, M.; Ciechanowski, P.; Ludman, E.J.; Young, B.; Peterson, D.; Rutter, C.M.; McGregor, M.; McCulloch, D. Collaborative care for patients with depression and chronic illnesses. N. Engl. J. Med. 2010, 363, 2611–2620. [Google Scholar] [CrossRef]
- Walker, E.A.; Shmukler, C.; Ullman, R.; Blanco, E.; Scollan-Koliopoulus, M.; Cohen, H.W. Results of a successful telephonic intervention to improve diabetes control in urban adults: A randomized trial. Diabetes Care 2011, 34, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Piette, J.D.; Weinberger, M.; Kraemer, F.B.; McPhee, S.J. Impact of automated calls with nurse follow-up on diabetes treatment outcomes in a Department of Veterans Affairs Health Care System: A randomized controlled trial. Diabetes Care 2001, 24, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Hennein, R.; Hwang, S.J.; Au, R.; Levy, D.; Muntner, P.; Fox, C.S.; Ma, J. Barriers to medication adherence and links to cardiovascular disease risk factor control: The Framingham Heart Study. Intern. Med. J. 2018, 48, 414–421. [Google Scholar] [CrossRef]
- Almutairi, N.; Hosseinzadeh, H.; Gopaldasani, V. The effectiveness of patient activation intervention on type 2 diabetes mellitus glycaemic control and self-management behaviors: A systematic review of RCTs. Prim. Care Diabetes 2020, 14, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Haynes, R.B.; Ackloo, E.; Sahota, N.; McDonald, H.P.; Yao, X. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2008, CD000011. [Google Scholar] [CrossRef] [PubMed]
- Kirk, J.; MacDonald, A.; Lavender, P.; Dean, J.; Rubin, G. Can Treatment Adherence Be Improved by Using Rubin’s Four Tendencies Framework to Understand a Patient’s Response to Expectations. Biomed. Hub 2017, 2, 480347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.T.; Bussell, J.K. Medication adherence: WHO cares? Mayo Clin. Proc. 2011, 86, 304–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinosa-García, J.; Cobaleda-Polo, J.; González-Velasco, M.; Fernández-Bergés, D. Validación de la llamada telefónica como método de medida del cumplimiento terapéutico de la hipertensión arterial en Extremadura [Validation of the telephone call as a method for measuring compliance to arterial hypertension treatment in Extremadura]. Semergen 2014, 40, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Eakin, E.G.; Lawler, S.P.; Vandelanotte, C.; Owen, N. Telephone interventions for physical activity and dietary behavior change: A systematic review. Am. J. Prev. Med. 2007, 32, 419–434. [Google Scholar] [CrossRef]
- Krousel-Wood, M.; Thomas, S.; Muntner, P.; Morisky, D. Medication adherence: A key factor in achieving blood pressure control and good clinical outcomes in hypertensive patients. Curr. Opin. Cardiol. 2004, 19, 357–362. [Google Scholar] [CrossRef]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014, 2014, CD000011. [Google Scholar] [CrossRef]
- Osborn, C.Y.; Egede, L.E. The relationship between depressive symptoms and medication nonadherence in type 2 diabetes: The role of social support. Gen. Hosp. Psychiatry 2012, 34, 249–253. [Google Scholar] [CrossRef] [Green Version]
- Manea, L.; Gilbody, S.; McMillan, D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiatry 2015, 37, 67–75. [Google Scholar] [CrossRef]
- Cichoń, E.; Kiejna, A.; Kokoszka, A.; Gondek, T.M.; Radzio, R.; Jastrzębski, A.; Andrzejewska, B.E.; Alosaimi, F.D.; Lloyd, C.E.; Sartorius, N. People with diabetes need a lower cut-off than others for depression screening with PHQ-9. PLoS ONE 2020, 15, e0240209. [Google Scholar] [CrossRef]
- Perrin, N.E.; Davies, M.J.; Robertson, N.; Snoek, F.J.; Khunti, K. The prevalence of diabetes-specific emotional distress in people with Type 2 diabetes: A systematic review and meta-analysis. Diabet. Med. A J. Br. Diabet. Assoc. 2017, 34, 1508–1520. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Vega, I.P.; Doubova, S.V.; Pérez-Cuevas, R. Distress and its association with self-care in people with type 2 diabetes. Salud Ment. 2017, 40, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Hessler, D.M.; Polonsky, W.H.; Mullan, J. When is diabetes distress clinically meaningful?: Establishing cut points for the Diabetes Distress Scale. Diabetes Care 2012, 35, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, M. Alteraciones Psicosociales de la Diabetes, Relación con Calidad de Vida, Control Metabólico y Complicaciones Crónicas; Universidad de Murcia: Murcia, Spain, 2020. [Google Scholar]
- Lutes, L.D.; Cummings, D.M.; Littlewood, K.; Solar, C.; Carraway, M.; Kirian, K.; Patil, S.; Adams, A.; Ciszewski, S.; Hambidge, B. COMRADE: A randomized trial of an individually tailored integrated care intervention for uncontrolled type 2 diabetes with depression and/or distress in the rural southeastern US. Contemp. Clin. Trials 2018, 70, 8–14. [Google Scholar] [CrossRef]
- Schmitt, A.; Reimer, A.; Ehrmann, D.; Kulzer, B.; Haak, T.; Hermanns, N. Reduction of depressive symptoms predicts improved glycaemic control: Secondary results from the DIAMOS study. J. Diabetes Its Complicat. 2017, 31, 1608–1613. [Google Scholar] [CrossRef]
- Fisher, L.; Gonzalez, J.S.; Polonsky, W.H. The confusing tale of depression and distress in patients with diabetes: A call for greater clarity and precision. Diabet. Med. A J. Br. Diabet. Assoc. 2014, 31, 764–772. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | RCT Group | p | |
|---|---|---|---|
| Control Group | Intervention Group | ||
| Age * | 71.5 (10.5) | 71.4 (10.3) | 0.857 |
| Age IC. mean (95%) | 70.1–73.0 | 70.0–72.7 | |
| <50 years * | 5 (2.5%) | 8 (3.6%) | 0.626 |
| 50–60 years * | 31 (15.3%) | 27 (12.0%) | |
| 61–70 years * | 48 (23.6%) | 65 (2.9%) | |
| 71–80 years * | 76 (37.4%) | 78 (34.7%) | |
| >80 years * | 43 (21.2%) | 47 (20.9%) | |
| Gender | |||
| Male ** | 57 (28.1%) | 64 (28.4%) | 0.933 |
| Female ** | 146 (71%) | 161 (71.6%) | |
| Years of diagnoses T2D | |||
| Mean (SD) | 9.8 (5.5) | 10.2 (5.7) | 0.470 |
| C. mean (95%) | 9.0–10.6 | 9.4–10.9 | |
| <5 years n (%) | 35 (17.2%) | 36 (16.0%) | 0.831 |
| 5–10 years n (%) | 80 (39.4%) | 85 (37.8%) | |
| >10 years n (%) | 88 (43.3%) | 104 (46.2%) | |
| Years of diagnoses CD * | |||
| Mean (SD) | 9.6 (4.8) | 9.4 (5.3) | 0.766 |
| IC. mean (95%) | 8.9–10.3 | 8.7–10.1 | |
| <5 years n (%) | 33 (16.3%) | 44 (19.6%) | 0.662 |
| 5–10 years n (%) | 79 (38.9%) | 86 (38.2%) | |
| >10 years n (%) | 91 (44.8%) | 95 (42.2%) | |
| Number of nurse consultation appointments | |||
| mean (SD) | 9.5 (10.4) | 9.9 (11.7) | 0.649 |
| IC. Mean (95%) | 8.0–10.9 | 8.4–11.5 | |
| <5 inquiries ** | 74 (36.5%) | 69 (30.7%) | 0.098 |
| 5–10 inquiries ** | 61 (30.0%) | 90 (40.0%) | |
| >10 inquiries ** | 68 (33.5%) | 66 (29.3%) | |
| Number of Medical consultations | |||
| mean (SD) | 11.0 (6.7) | 10.8 (6.7) | 0.726 |
| IC. mean (95%) | 10.1–11.9 | 9.9–11.7 | |
| <5 inquiries ** | 32 (15.8%) | 34 (15.1%) | 0.475 |
| 5–10 inquiries ** | 76 (37.4%) | 97 (43.1%) | |
| >10 inquiries ** | 95 (46.8%) | 94 (41.8%) | |
| Variable | Control Group | Intervention Group | p |
|---|---|---|---|
| HbA1c (%) | Mean (SD) | Mean (SD) | |
| Month 0 | 8.65 (1.40) | 8.72 (1.49) | <0.001 1 <0.001 2 <0.001 3 |
| Month 6 | 8.74 (1.40) | 7.90 (1.22) | |
| Month 12 | 8.81 (1.38) | 7.11 (1.17) | |
| Month 18 | 8.84 (1.38) | 7.03 (1.09) | |
| LDL cholesterol (mg/dL) | |||
| Month 0 | 117.07 (48.12) | 115.09 (47.52) | <0.001 1 <0.001 2 <0.001 3 |
| Month 6 | 121.85 (43.29) | 100.46 (34.85) | |
| Month 12 | 117.36 (40.03) | 100.10 (38.11) | |
| Month 18 | 125.87 (38.60) | 105.86 (35.43) | |
| Body mass index (BMI) | |||
| Month 0 | 30.49 (5.11) | 30.42 (5.04) | 0.162 1 0.434 2 <0.001 3 |
| Month 6 | 30.48 (5.12) | 30.20 (4.99) | |
| Month 12 | 30.67 (5.09) | 30.16 (5.10) | |
| Month 18 | 30.78 (5.02) | 30.05 (5.09) | |
| Systolic Blood Pressure (mmHg) | |||
| Month 0 | 134.41 (15.41) | 131.83 (15.42) | <0.001 1 <0.001 2 <0.001 3 |
| Month 6 | 143.03 (15.36) | 133.35 (14.35) | |
| Month 12 | 145.99 (12.13) | 132.21 (15.26) | |
| Month 18 | 147.29 (11.20) | 132.14 (10.82) | |
| Diastolic Blood Pressure (mmHg) | |||
| Month 0 | 76.86 (9.17) | 75.49 (9.60) | <0.001 1 <0.013 2 <0.001 3 |
| Month 6 | 75.13 (10.56) | 74.84 (9.68) | |
| Month 12 | 75.20 (9.43) | 73.11 (10.20) | |
| Month 18 | 74.25 (8.72) | 70.25 (7.65) |
| Control Group | Intervention Group | p | |||||
|---|---|---|---|---|---|---|---|
| PHQ-Total * | ** No Depression | *** Minor Depression | **** Major Depression | ** No Depression | *** Minor Depression | **** Major Depression | |
| Month 0 | 75 (36.9%) | 98 (48.3%) | 30 (14.8%) | 85 (37.8%) | 108 (48.0%) | 32 (14.2%) | 0.978 |
| Month 6 | 65 (32.8%) | 108 (54.5%) | 25 (12.6%) | 103 (52.0%) | 77 (38.9%) | 18 (9.1%) | 0.001 |
| Month 12 | 78 (40.2%) | 95 (49.0%) | 21 (10.8%) | 122 (62.6%) | 62 (31.8%) | 11 (5.6%) | <0.001 |
| Month 18 | 71 (37.2%) | 97 (50.8%) | 23 (12.0%) | 119 (62.3%) | 69 (36.1%) | 3 (1.6%) | <0.001 |
| Chi-Square test | |||||||
| DDS Total | Control Group 0 | Intervention group 0 | p | ||||
| Month 0 | 1.50 (0.41) | 1.48 (0.40) | <0.001 1 <0.001 2 <0.001 3 | ||||
| Month 6 | 1.52 (0.42) | 1.25 (0.31) | |||||
| Month 12 | 1.48 (0.46) | 1.21 (0.30) | |||||
| Month 18 | 1.48 (0.50) | 1.18 (0.27) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoyo, M.L.L.d.; Rodrigo, M.T.F.; Urcola-Pardo, F.; Monreal-Bartolomé, A.; Ruiz, D.C.G.; Borao, M.G.; Alcázar, A.B.A.; Casbas, J.P.M.; Casas, A.A.; Funcia, M.T.A.; et al. The TELE-DD Randomised Controlled Trial on Treatment Adherence in Patients with Type 2 Diabetes and Comorbid Depression: Clinical Outcomes after 18-Month Follow-Up. Int. J. Environ. Res. Public Health 2023, 20, 328. https://doi.org/10.3390/ijerph20010328
Hoyo MLLd, Rodrigo MTF, Urcola-Pardo F, Monreal-Bartolomé A, Ruiz DCG, Borao MG, Alcázar ABA, Casbas JPM, Casas AA, Funcia MTA, et al. The TELE-DD Randomised Controlled Trial on Treatment Adherence in Patients with Type 2 Diabetes and Comorbid Depression: Clinical Outcomes after 18-Month Follow-Up. International Journal of Environmental Research and Public Health. 2023; 20(1):328. https://doi.org/10.3390/ijerph20010328
Chicago/Turabian StyleHoyo, María Luisa Lozano del, María Teresa Fernandez Rodrigo, Fernando Urcola-Pardo, Alicia Monreal-Bartolomé, Diana Cecilia Gracia Ruiz, Mercedes Gómez Borao, Ana Belén Artigas Alcázar, José Pedro Martínez Casbas, Alexandra Aceituno Casas, María Teresa Andaluz Funcia, and et al. 2023. "The TELE-DD Randomised Controlled Trial on Treatment Adherence in Patients with Type 2 Diabetes and Comorbid Depression: Clinical Outcomes after 18-Month Follow-Up" International Journal of Environmental Research and Public Health 20, no. 1: 328. https://doi.org/10.3390/ijerph20010328
APA StyleHoyo, M. L. L. d., Rodrigo, M. T. F., Urcola-Pardo, F., Monreal-Bartolomé, A., Ruiz, D. C. G., Borao, M. G., Alcázar, A. B. A., Casbas, J. P. M., Casas, A. A., Funcia, M. T. A., & Delgado, J. F. R. (2023). The TELE-DD Randomised Controlled Trial on Treatment Adherence in Patients with Type 2 Diabetes and Comorbid Depression: Clinical Outcomes after 18-Month Follow-Up. International Journal of Environmental Research and Public Health, 20(1), 328. https://doi.org/10.3390/ijerph20010328