
Associations between Maternal Education and Child Nutrition and Oral Health in an Indigenous Population in Ecuador


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
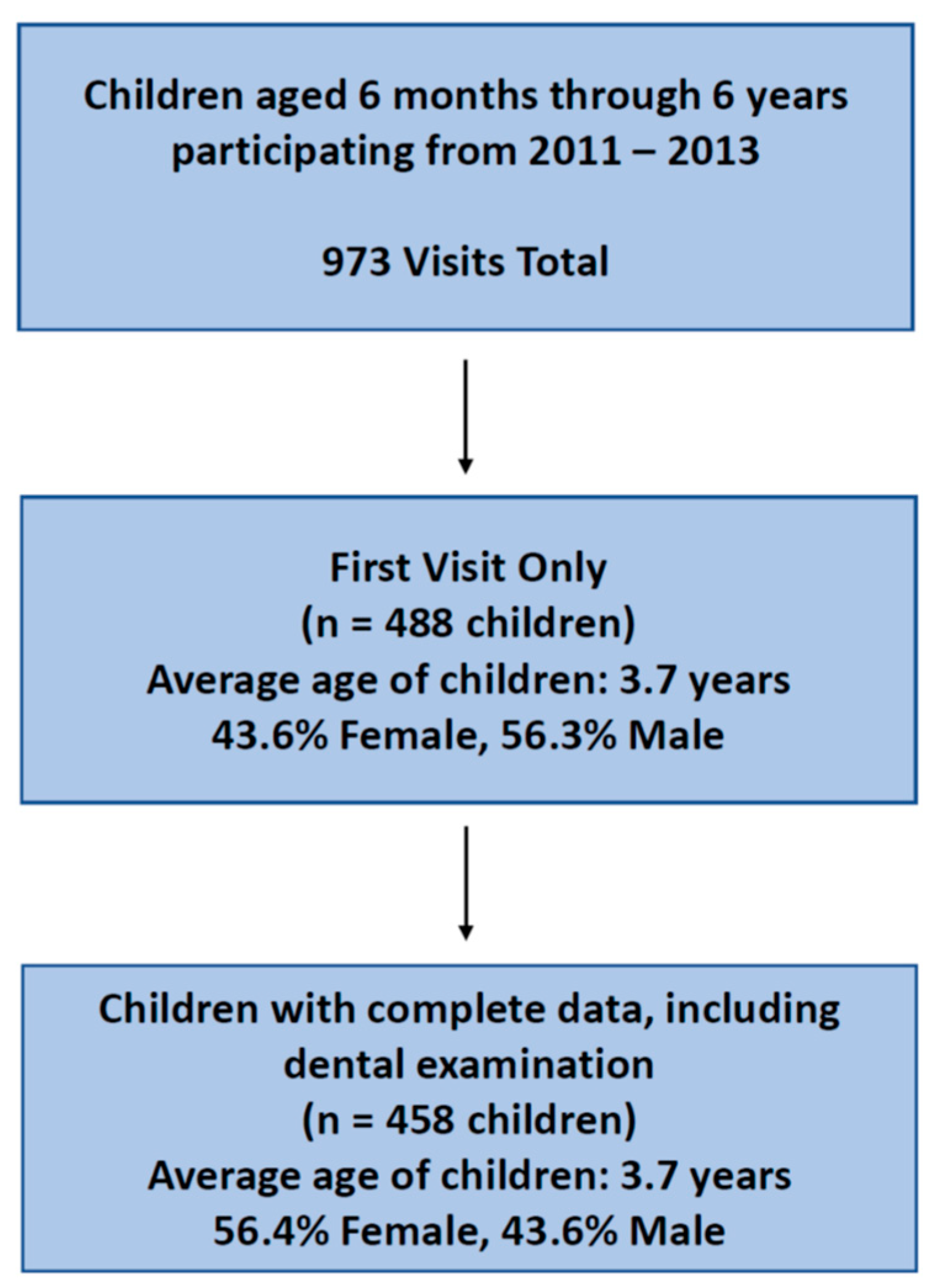
2.1. Study Design and Population
2.2. Data Collection and Measures
2.3. Statistical Analysis
3. Results
3.1. Family Demographic Characteristics
3.2. Maternal-Child Oral Health Practices
3.3. Child Oral Health Outcomes
3.4. Association between Maternal Education, Maternal-Child Nutrition and Oral Health Practices, and Child Oral Health Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M. Relationship between shifts in food system dynamics and acceleration of the global nutrition transition. Nutr. Rev. 2017, 75, 73–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Casamassimo, P.S.; Thikkurissy, S.; Edelstein, B.L.; Maiorini, E. Beyond the dmft: The human and economic cost of early childhood caries. J. Am. Dent. Assoc. 2009, 140, 650–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy on Pediatric Dentistry Council on Clinical Affairs. Policy on early childhood caries (ECC): Unique challenges and treatment option. Pediatr. Dent. 2008, 30 (Suppl. S7), 44–46. [Google Scholar]
- Tanzer, J.M. Dental caries is a transmissible infectious disease: The Keyes and Fitzgerald revolution. J. Dent. Res. 1995, 74, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D. The caries balance: The basis for caries management by risk assessment. Oral Health Prev. Dent. 2004, 2 (Suppl. S1), 259–264. [Google Scholar]
- Fisher-Owens, S.A.; Gansky, S.A.; Platt, L.J.; Weintraub, J.A.; Soobader, M.J.; Bramlett, M.D.; Newacheck, P.W. Influences on children’s oral health: A conceptual model. Pediatrics 2007, 120, e510–e520. [Google Scholar] [CrossRef] [Green Version]
- Peres, M.A.; Macpherson, L.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Jamieson, L.; Gibson, B.; Thomson, W.M. Oral Health Inequalities and the Corporate Determinants of Health: A Commentary. Int. J. Environ. Res. Public Health 2020, 17, 6529. [Google Scholar] [CrossRef]
- Kearns, C.E.; Bero, L.A. Conflicts of interest between the sugary food and beverage industry and dental research organisations: Time for reform. Lancet 2019, 394, 194–196. [Google Scholar] [CrossRef]
- Colak, H.; Dülgergil, C.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Schwendicke, F.; Dörfer, C.E.; Schlattmann, P.; Foster Page, L.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries: A systematic review and meta-analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef]
- Rai, N.K.; Tiwari, T. Parental Factors Influencing the Development of Early Childhood Caries in Developing Nations: A Systematic Review. Front. Public Health 2018, 6, 64. [Google Scholar] [CrossRef] [Green Version]
- Elamin, A.; Garemo, M.; Mulder, A. Determinants of dental caries in children in the Middle East and North Africa region: A systematic review based on literature published from 2000 to 2019. BMC Oral Health 2021, 21, 237. [Google Scholar] [CrossRef]
- Folayan, M.O.; El Tantawi, M.; Aly, N.M.; Al-Batayneh, O.B.; Schroth, R.J.; Castillo, J.L.; Virtanen, J.I.; Gaffar, B.O.; Amalia, R.; Kemoli, A.; et al. Association between early childhood caries and poverty in low and middle income countries. BMC Oral Health 2020, 20, 8. [Google Scholar] [CrossRef]
- Renggli, E.P.; Turton, B.; Sokal-Gutierrez, K.; Hondru, G.; Chher, T.; Hak, S.; Poirot, E.; Laillou, A. Stunting Malnutrition Associated with Severe Tooth Decay in Cambodian Toddlers. Nutrients 2021, 13, 290. [Google Scholar] [CrossRef]
- Yousaf, M.; Aslam, T.; Saeed, S.; Sarfraz, A.; Sarfraz, Z.; Cherrez-Ojeda, I. Individual, Family, and Socioeconomic Contributors to Dental Caries in Children from Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2022, 19, 7114. [Google Scholar] [CrossRef]
- Wang, J.; Geng, L. Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator. Int. J. Environ. Res. Public Health 2019, 16, 281. [Google Scholar] [CrossRef] [Green Version]
- Lea, A.J.; Waigwa, C.; Muhoya, B.; Lotukoi, F.; Peng, J.; Henry, L.P.; Abhyankar, V.; Kamau, J.; Martins, D.; Gurven, M.; et al. Socioeconomic status effects on health vary between rural and Urban Turkana. Evol. Med. Public Health 2021, 9, 406–419. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Why Education Is the Key to Socioeconomic Differentials in Health. In Handbook of Medical Sociology, 6th ed.; Vanderbilt University Press: Nashville, TN, USA, 2010; pp. 33–51. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E.; European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [Green Version]
- Dabiri, D.; Fontana, M.; Kapila, Y.; Eckert, G.; Sokal-Gutierrez, K. Community-based assessment and intervention for early childhood caries in rural El Salvador. Int. Dent. J. 2016, 66, 221–228. [Google Scholar] [CrossRef]
- Nutritional Failure in Ecuador: Causes, Consequences, and Solutions. Available online: https://openknowledge.worldbank.org/handle/10986/6651 (accessed on 13 December 2021).
- Penafiel, D.; Termote, C.; Lachat, C.; Espinel, R.; Kolsteren, P.; Van Damme, P. Barriers to Eating Traditional Foods Vary by Age Group in Ecuador With Biodiversity Loss as a Key Issue. J. Nutr. Educ. Behav. 2016, 48, 258–268.e1. [Google Scholar] [CrossRef] [PubMed]
- Principales Resultados ENSANUT 2018. Available online: https://www.ecuadorencifras.gob.ec/documentos/web-inec/Estadisticas_Sociales/ENSANUT/ENSANUT_2018/Principales%20resultados%20ENSANUT_2018.pdf (accessed on 13 December 2021).
- Paiva, S.M.; Abreu-Placeres, N.; Camacho, M.; Frias, A.C.; Tello, G.; Perazzo, M.F.; Pucca-Júnior, G.A. Dental caries experience and its impact on quality of life in Latin American and Caribbean countries. Braz. Oral Res. 2021, 35 (Suppl. S1), e052. [Google Scholar] [CrossRef]
- Ecuador Education System. Available online: https://www.scholaro.com/db/countries/ecuador/education-system (accessed on 12 December 2022).
- Malnutrition in Infants and Young Children in Latin America and the Caribbean: Achieving the Millennium Development Goals. Available online: http://iris.paho.org/xmlui/bitstream/handle/123456789/18641/9789275129289_eng.pdf?sequence=1&isAllowed=y (accessed on 13 December 2021).
- Pan, W.K.-Y.; Erlien, C.; Bilsborrow, R.E. Morbidity and mortality disparities among colonist and indigenous populations in the Ecuadorian Amazon. Soc. Sci. Med. 2010, 70, 401–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina, W.; Hurtig, A.K.; San Sebastián, M.; Quizhpe, E.; Romero, C. Dental caries in 6–12-year-old indigenous and non-indigenous schoolchildren in the Amazon basin of Ecuador. Braz. Dent. J. 2008, 19, 83–86. [Google Scholar] [CrossRef]
- Martignon, S.; Roncalli, A.G.; Alvarez, E.; Aránguiz, V.; Feldens, C.A.; Buzalaf, M. Risk factors for dental caries in Latin American and Caribbean countries. Braz. Oral Res. 2021, 35 (Suppl. S1), e053. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, T.; Jamieson, L.; Broughton, J.; Lawrence, H.P.; Batliner, T.S.; Arantes, R.; Albino, J. Reducing Indigenous Oral Health Inequalities: A Review from 5 Nations. J. Dent. Res. 2018, 97, 869–877. [Google Scholar] [CrossRef]
- Mejia, G.C.; Parker, E.J.; Jamieson, L.M. An introduction to oral health inequalities among Indigenous and non-Indigenous populations. Int. Dent. J. 2010, 60 (Suppl. S2), 212–215. [Google Scholar]
- Parker, E.J.; Jamieson, L.M.; Broughton, J.; Albino, J.; Lawrence, H.P.; Roberts-Thomson, K. The oral health of Indigenous children: A review of four nations. J. Paediatr. Child Health 2010, 46, 483–486. [Google Scholar] [CrossRef]
- Nath, S.; Ju, X.; Haag, D.G.; Kapellas, K.; Santiago, P.; Jamieson, L. Prevalence of dental caries among Indigenous populations compared to non-Indigenous populations: A quantitative systematic review protocol. JBI Evid. Synth. 2021, 19, 3096–3101. [Google Scholar] [CrossRef]
- Petersen, P.E. World Health Organization global policy for improvement of oral health—World Health Assembly 2007. Int. Dent. J. 2008, 58, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Mossey, P.A.; Petersen, P.E. Budapest Declaration: IADR-GOHIRA®. J. Dent. Res. 2014, 93 (Suppl. S7), 120S–121S. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M.; Mossey, P.A.; Mathur, M.R. Leadership in global oral health. J. Dent. 2019, 87, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Holve, S.; Braun, P.; Irvine, J.D.; Nadeau, K.; Schroth, R.J.; Bell, S.L.; American Academy of Pediatrics Committee on Native American Child Health. Early childhood caries in indigenous communities. Pediatrics 2021, 147, e2021051481. [Google Scholar] [CrossRef] [PubMed]
- Oral Health Surveys: Basic Methods. Available online: https://apps.who.int/iris/handle/10665/41905 (accessed on 11 January 2022).
- Sokal-Gutierrez, K.; Turton, B.; Husby, H.; Paz, C.L. Early childhood caries and malnutrition: Baseline and two-year follow-up results of a community-based prevention intervention in rural Ecuador. BMC Nutr. 2016, 2, 73. [Google Scholar] [CrossRef] [Green Version]
- Huang, D.; Sokal-Gutierrez, K.; Chung, K.; Lin, W.; Khanh, L.N.; Chung, R.; Hoang, H.T.; Ivey, S.L. Maternal and Child Nutrition and Oral Health in Urban Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 2579. [Google Scholar] [CrossRef] [Green Version]
- Athavale, P.; Khadka, N.; Roy, S.; Mohan, D.C.; Mukherjee, P.; Turton, B.; Sokal-Gutierrez, K. Early Childhood Junk Food Consumption, Severe Dental Caries, and Undernutrition: A Mixed-Methods Study from Mumbai, India. Int. J. Environ. Res. Public Health 2020, 17, 8629. [Google Scholar] [CrossRef]
- Tsang, C.; Sokal-Gutierrez, K.; Patel, P.; Lewis, B.; Huang, D.; Ronsin, K.; Baral, A.; Bhatta, A.; Khadka, A.; Barkan, H.; et al. Early Childhood Oral Health and Nutrition in Urban and Rural Nepal. Int. J. Environ. Res. Public Health 2019, 16, 2456. [Google Scholar] [CrossRef] [Green Version]
- WHO Child Growth Standards and the Identification of Severe Acute Malnutrition in Infants and Children: A Joint Statement. Available online: http://apps.who.int/iris/bitstream/handle/10665/44129/9789241598163_eng.pdf?sequence=1 (accessed on 11 January 2022).
- Aarø, L.E.; Flisher, A.J.; Kaaya, S.; Onya, H.; Namisi, F.S.; Wubs, A. Parental education as an indicator of socioeconomic status: Improving quality of data by requiring consistency across measurement occasions. Scand. J. Public Health 2008, 37 (Suppl. S2), 16–27. [Google Scholar] [CrossRef] [Green Version]
- Poulsen, G.; Strandberg-Larsen, K.; Mortensen, L.; Barros, H.; Cordier, S.; Correia, S.; Danileviciute, A.; van Eijsden, M.; Fer-nández-Somoano, A.; Gehring, U.; et al. Exploring educational disparities in risk of preterm delivery: A comparative study of 12 European birth cohorts. Paediatr. Perinat. Epidemiol. 2015, 29, 172–183. [Google Scholar] [CrossRef]
- Howe, L.D.; Tilling, K.; Galobardes, B.; Smith, G.D.; Ness, A.R.; Lawlor, D.A. Socioeconomic disparities in trajectories of adiposity across childhood. Int. J. Pediatr. Obes. 2011, 6, e144–e153. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, R.; Pamuk, E.; Lutz, W. Education or Wealth: Which Matters More for Reducing Child Mortality in Developing Countries? Vienna Yearb. Popul. Res. 2010, 8, 175–199. [Google Scholar] [CrossRef]
- Balaj, M.; York, H.W.; Sripada, K.; Besnier, E.; Vonen, H.D.; Aravkin, A.; Friedman, J.; Griswold, M.; Jensen, M.R.; Mohammad, T.; et al. Parental education and inequalities in child mortality: A global systematic review and meta-analysis. Lancet 2021, 398, 608–620. [Google Scholar] [CrossRef] [PubMed]
- Growth Reference Data for 5–19 Years—Application Tools. Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/application-tools (accessed on 20 January 2022).
- Curtis, D.C.; Ortega, F.; Eckhart, S.; Monar, J.; Thompson, P. Utilizing the caries risk assessment model (Caries Management by Risk Assessment) in Ecuador. J. Int. Oral Health 2018, 10, 287–292. [Google Scholar] [CrossRef]
- Veléz, E.; Encalada, L.; Fernández, M.J.; Salinas, G. Prevalencia de caries según indice CEOD en escolares de 6 años Cuenca-Ecuador. Rev. KIRU 2019, 16, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Huffman, S.L.; Piwoz, E.G.; Vosti, S.A.; Dewey, K.G. Babies, soft drinks and snacks: A concern in low- and middle-income countries? Matern. Child Nutr. 2014, 10, 562–574. [Google Scholar] [CrossRef] [Green Version]
- Contreras, M.; Zelaya Blandón, E.; Persson, L.Å.; Ekström, E.C. Consumption of highly processed snacks, sugar-sweetened beverages and child feeding practices in a rural area of Nicaragua. Matern. Child Nutr. 2016, 12, 164–176. [Google Scholar] [CrossRef]
- Hoeft, K.S.; Barker, J.C.; Masterson, E.E. Urban Mexican-American mothers’ beliefs about caries etiology in children. Community Dent. Oral Epidemiol. 2010, 38, 244–255. [Google Scholar] [CrossRef] [Green Version]
- Aliakbari, E.; Gray-Burrows, K.A.; Vinall-Collier, K.A.; Edwebi, S.; Marshman, Z.; McEachan, R.; Day, P.F. Home-based toothbrushing interventions for parents of young children to reduce dental caries: A systematic review. Int. J. Paediatr. Dent. 2021, 31, 37–79. [Google Scholar] [CrossRef]
- Alsharairi, N.A.; Somerset, S. Parental work status and children’s dietary consumption: Australian evidence. Int. J. Consum. Stud. 2018, 42, 522–532. [Google Scholar] [CrossRef]
- Folayan, M.O.; El Tantawi, M.; Vukovic, A.; Schroth, R.; Gaffar, B.; Al-Batayneh, O.B.; Amalia, R.; Arheiam, A.; Obiyan, M.; Daryanavard, H.; et al. Women’s economic empowerment, participation in decision-making and exposure to violence as risk indicators for early childhood caries. BMC Oral Health 2020, 20, 54. [Google Scholar] [CrossRef] [Green Version]
- Pitruniak, B.; Adachi, K.; Messelink, M. Ecuador: Communicating to bridge the Education Gap in nutrition. Earth Common J. 2019, 5, 34–39. [Google Scholar] [CrossRef]
- Barrera, L.H.; Rothenberg, S.J.; Barquera, S.; Cifuentes, E. The Toxic Food Environment Around Elementary Schools and Childhood Obesity in Mexican Cities. Am. J. Prev. Med. 2019, 51, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Plan of Action for Prevention of Obesity in Children and Adolescents. Available online: https://www.paho.org/hq/dmdocuments/2015/Obesity-Plan-Of-Action-Child-Eng-2015.pdf?ua=1&ua=1 (accessed on 5 March 2022).
- Ochoa-Aviles, A.; Rivas-Marino, G.; Verstraeten, R. Tackling Overweight and Obesity in Ecuador: Policies and Strategies for Prevention. Nutr. Exch. 2017, 8, 12. Available online: https://www.ennonline.net/nex/8/tacklingoverweightandobesityinecuador (accessed on 5 March 2022).
- Radosevich, A.; Mendes, F.; Villegas, R.; Mora-Garcia, G.; Garcia-Larsen, V. Awareness, Understanding and Use of the ‘Traffic Light’ Food Labelling Policy and Educational Level in Ecuador—Findings from the National Nutrition Survey 2018. Curr. Dev. Nutr. 2020, 4 (Suppl. S2), 1731. [Google Scholar] [CrossRef]
- WHO Expert Consultation on Public Health Intervention against Early Childhood Caries: Report of a Meeting, Bangkok, Thailand, 26–28 January 2016. Available online: https://apps.who.int/iris/handle/10665/255627 (accessed on 12 March 2022).
- Ending Childhood Dental Caries: WHO Implementation Manual. Available online: https://www.who.int/publications/i/item/ending-childhood-dental-caries-who-implementation-manual (accessed on 13 March 2022).
- Follow-Up to the Political Declaration of the Third High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Disease. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_10Add1-en.pdf (accessed on 2 May 2022).
- Delivering Optimal Oral Health for All. Available online: https://www.fdiworlddental.org/sites/default/files/2021-02/Vision-2030-Delivering%20Optimal-Oral-Health-for-All_0.pdf (accessed on 20 April 2022).



{kind=link}
{kind=link}
| Characteristics | Mean ± SD or % n = 252 Mothers n = 458 Children |
|---|---|
| Mother | |
| Age (years) | 30.0 ± 7.8 |
| Education Level (years) | 5.9 ± 4.2 |
| Number of Children | 4.0 ± 2.5 |
| Child | |
| Age (years) | 3.7 ± 2.5 |
| Sex (%) | |
| Female | 56.4 |
| Male | 43.6 |
| Family | |
| Number of People in a Household | 7.2 ± 2.8 |
| Cook with Wood Only (%) | 17.0 |
| No Electricity at Home (%) | 14.0 |
| No Potable Water at Home (%) | 72.0 |
| Walking Distance to Store Selling Junk Food (%) | |
| <5 min | 67.7 |
| 6–20 min | 21.0 |
| >20 min | 11.3 |
| Practices | Mean ± SD or % n = 252 Mothers n = 458 Children |
|---|---|
| Mother | |
| Received Prenatal Care (%) | 79.3 |
| Daily Dietary Consumption (%) | |
| Milk | 19.6 |
| Soda | 6.3 |
| Has Own Toothbrush (%) | 91.7 |
| Has Been to the Dentist (%) | 64.5 |
| Current Oral Health Complaints (e.g., dental pain, decayed teeth, bleeding gums, inflammation) (%) | 52.1 |
| Knows at Least 2 Causes of Child Caries (%) | 34.2 |
| Knows at Least 2 Consequences of Child Caries (%) | 29.2 |
| Child | |
| Vaccines Up-to-date (%) | 80.2 |
| Child Breastfed (including breast milk in bottle) (%) | 97.2 |
| Breastfeeding Duration (months) | 17.0 ± 8.1 |
| Child Bottle-Fed (%) | 34.4 |
| Bottle-Feeding Duration (months) | 13.4 ± 10.8 |
| Drank Sugary Liquid in Baby Bottle (%) | 18.3 |
| Slept with Baby Bottle (%) | 4.1 |
| Daily Dietary Consumption (%) | |
| Milk | 19.6 |
| Soda | 6.3 |
| Sweets | 14.4 |
| Chips | 10.4 |
| Ice Pops | 21.3 |
| Children Consuming Any Junk Food Daily (%) | 52.3 |
| How Mother Calms Fussing Child (%) | |
| With Food | 27.2 |
| With Baby Bottle | 5.5 |
| With Sweets | 7.0 |
| Has Own Toothbrush (%) | 76.7 |
| Has Own Toothpaste (%) | 70.5 |
| Mother Helps Child Brush Teeth (%) | 35.7 |
| Child Has Been to the Dentist (%) | 28.5 |
| Average Number of Dental Visits | 1.7 ± 2.0 |
| Nutrition Status | |
| Malnutrition (%) | |
| Stunting 1 | 28.1 |
| Wasting 2 | 1.1 |
| Underweight 3 | 7.2 |
| Overweight or Obese 4 | 4.2 |
| Health Status | Mean ± SD or % n = 458 Children |
|---|---|
| Oral Exam | |
| Children with Tooth Decay (%) | 76.7 |
| Average Number of Decayed, Missing, or Filled Teeth (dmft) | 6.7 ± 5.5 |
| Untreated Decayed Teeth (d/dmft) (%) | 87.3 |
| Average Number of Decayed Teeth | 5.9 ± 5.1 |
| Average Number of Missing (Extracted) Teeth | 0.4 ± 1.4 |
| Average Number of Filled Teeth | 0.6 ± 1.4 |
| Mother’s Perception of Child’s Oral Health | |
| Current Child Complaints of Mouth Pain (%) | 38.9 |
| Mother Believes Child’s Oral Health is Poor (%) | 12.6 |
| Mother Believes Child’s Overall Health is Poor (%) | 5.6 |
| Practices | Unadjusted Odds Ratios (95% CI) or Pearson’s Correlation Coefficient (95% CI) | Adjusted Odds Ratios 0 (95% CI) or Pearson’s Correlation Coefficient (95% CI) | p-Value for Adjusted Estimate |
|---|---|---|---|
| Mother | |||
| Received Prenatal Care 1 | 1.10 (1.01–1.20) | 1.09 (0.99–1.20) | 0.085 |
| Drinks Milk Daily 2 | 1.19 (1.09–1.30) | 1.20 (1.08–1.34) | <0.01 ** |
| Drinks Soda Daily 2 | 0.99 (0.90–1.09) | 0.95 (0.85–1.07) | 0.41 |
| Has Own Toothbrush 1 | 1.10 (0.99–1.23) | 1.02 (0.89–1.16) | 0.81 |
| Has Been to the Dentist 2 | 1.04 (0.99–1.11) | 1.03 (0.96–1.10) | 0.39 |
| Current Oral Health Complaints 2 | 1.00 (0.94–1.05) | 1.01 (0.95–1.08) | 0.74 |
| Knows at Least 2 Causes of Child Caries 2 | 0.94 (0.88–0.99) | 0.94 (0.88–1.00) | 0.081 |
| Knows at Least 2 Consequences of Child Caries 2 | 1.11 (1.04–1.18) | 1.17 (1.08–1.27) | <0.01 ** |
| Child | |||
| Vaccines Up-to-date 1 | 1.05 (0.99–1.11) | 1.07 (1.00–1.15) | 0.067 |
| Child Breastfed 1 | 0.95 (0.83–1.09) | 0.85 (0.65–1.06) | 0.17 |
| Breastfeeding Duration 3,5 | −0.0043 (−0.096–0.087) | −0.0039 (−0.032−0.024) | 0.78 |
| Child Bottle-Fed 1 | 1.10 (1.05–1.16) | 1.10 (1.05–1.17) | <0.01 ** |
| Bottle-Feeding Duration 3,5 | 0.20 (0.11–0.29) | 0.20 (0.18–0.23) | <0.01 ** |
| Drank Sugary Liquid in Baby Bottle 2 | 1.14 (1.08–1.21) | 1.14 (1.06–1.22) | <0.01 ** |
| Slept with Baby Bottle 1 | 1.09 (0.98–1.22) | 0.98 (0.86–1.12) | 0.80 |
| Daily Dietary Consumption: | |||
| Milk 2 | 1.18 (1.11–1.25) | 1.20 (1.11–1.29) | <0.01 ** |
| Soda 2 | 1.03 (0.94–1.21) | 1.01 (0.91–1.12) | 0.89 |
| Sweets 2 | 1.10 (1.04–1.18) | 1.11 (1.03–1.20) | <0.01 ** |
| Chips 2 | 1.04 (0.97–1.11) | 1.07 (0.98–1.16) | 0.11 |
| Ice Pops 2 | 1.03 (0.98–1.09) | 1.05 (0.99–1.12) | 0.13 |
| How Mother Calms Fussing Child: | |||
| With Food 1 | 0.99 (0.95–1.04) | 1.04 (0.98–1.10) | 0.17 |
| With Baby Bottle 1 | 1.10 (1.00–1.21) | 1.16 (1.03–1.31) | 0.013 * |
| With Sweets 1 | 1.08 (0.99–1.17) | 1.16 (1.04–1.29) | <0.01 ** |
| Has Own Toothbrush 1 | 1.05 (0.99–1.11) | 1.01 (0.93–1.09) | 0.80 |
| Has Own Toothpaste 1 | 1.08 (1.03–1.14) | 1.03 (0.97–1.10) | 0.33 |
| Mother Helps Child Brush Teeth 1 | 1.00 (0.96–1.04) | 0.93 (0.88–0.98) | 0.011 * |
| Child Has Been to the Dentist 1 | 0.98 (0.93–1.02) | 0.95 (0.89–1.01) | 0.083 |
| Number of Dental Visits 3,5 | 0.023 (−0.069–0.11) | 0.023 (−0.0044−0.051) | 0.099 |
| Nutrition Status4 | |||
| Chronic Stunting Malnutrition | 0.99 (0.94–1.04) | 1.02 (0.96–1.08) | 0.60 |
| Wasting | 1.06 (0.85–1.31) | 1.48 (1.01–2.72) | 0.10 |
| Underweight | 1.00 (0.91–1.08) | 1.05 (0.95–1.16) | 0.39 |
| Overweight/Obese under age 5 | 1.02 (0.93–1.12) | 1.01 (0.90–1.13) | 0.88 |
| Overweight/Obese age 5 and above | 1.01 (0.84–1.19) | 0.98 (0.78–1.23) | 0.85 |
| Mother’s Perception of Child’s Oral Health | |||
| Current Child Complaints of Mouth Pain 2 | 1.00 (0.94–1.06) | 0.99 (0.92–1.07) | 0.82 |
| Mother Believes Child’s Oral Health is Poor 2 | 0.96 (0.89–1.03) | — 6 | — 6 |
| Mother Believes Child’s Overall Health is Poor 2 | 0.84 (0.74–0.94) | 0.90 (0.79–1.02) | 0.10 |
| Oral Health Outcomes | Count Model 1 Estimate (95% CI) | Count Model p-Value | Inflation Model 2 Estimate (95% CI) | Inflation Model p-Value |
|---|---|---|---|---|
| Oral Exam | ||||
| Number of Decayed, Missing, or Filled Teeth (dmft) | 0.99 (0.98–1.00) | 0.023 * | 1.03 (0.92–1.16) | 0.43 |
| Number of Decayed Teeth | 0.98 (0.97–1.00) | <0.01 ** | 1.04 (0.93–1.16) | 0.37 |
| Number of Teeth Missing Due to Caries | 1.00 (0.92–1.08) | 0.88 | 1.03 (0.91–1.20) | 0.60 |
| Number of Filled Teeth | 1.03 (0.97–1.08) | 0.19 | 0.94 (0.85–1.04) | 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinnakotla, B.; Susarla, S.M.; Mohan, D.C.; Turton, B.; Husby, H.M.; Morales, C.P.; Sokal-Gutierrez, K. Associations between Maternal Education and Child Nutrition and Oral Health in an Indigenous Population in Ecuador. Int. J. Environ. Res. Public Health 2023, 20, 473. https://doi.org/10.3390/ijerph20010473
Chinnakotla B, Susarla SM, Mohan DC, Turton B, Husby HM, Morales CP, Sokal-Gutierrez K. Associations between Maternal Education and Child Nutrition and Oral Health in an Indigenous Population in Ecuador. International Journal of Environmental Research and Public Health. 2023; 20(1):473. https://doi.org/10.3390/ijerph20010473
Chicago/Turabian StyleChinnakotla, Bharathi, Sita Manasa Susarla, Deepika Chandra Mohan, Bathsheba Turton, Hannah M. Husby, Cecilia Paz Morales, and Karen Sokal-Gutierrez. 2023. "Associations between Maternal Education and Child Nutrition and Oral Health in an Indigenous Population in Ecuador" International Journal of Environmental Research and Public Health 20, no. 1: 473. https://doi.org/10.3390/ijerph20010473
APA StyleChinnakotla, B., Susarla, S. M., Mohan, D. C., Turton, B., Husby, H. M., Morales, C. P., & Sokal-Gutierrez, K. (2023). Associations between Maternal Education and Child Nutrition and Oral Health in an Indigenous Population in Ecuador. International Journal of Environmental Research and Public Health, 20(1), 473. https://doi.org/10.3390/ijerph20010473