

Effects of Virtual Reality Exercises versus Isokinetic Exercises in comparison with Conventional Exercises on the Imaging Findings and Inflammatory Biomarker Changes in Soccer Players with Non-Specific Low Back Pain: A Randomized Controlled Trial

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
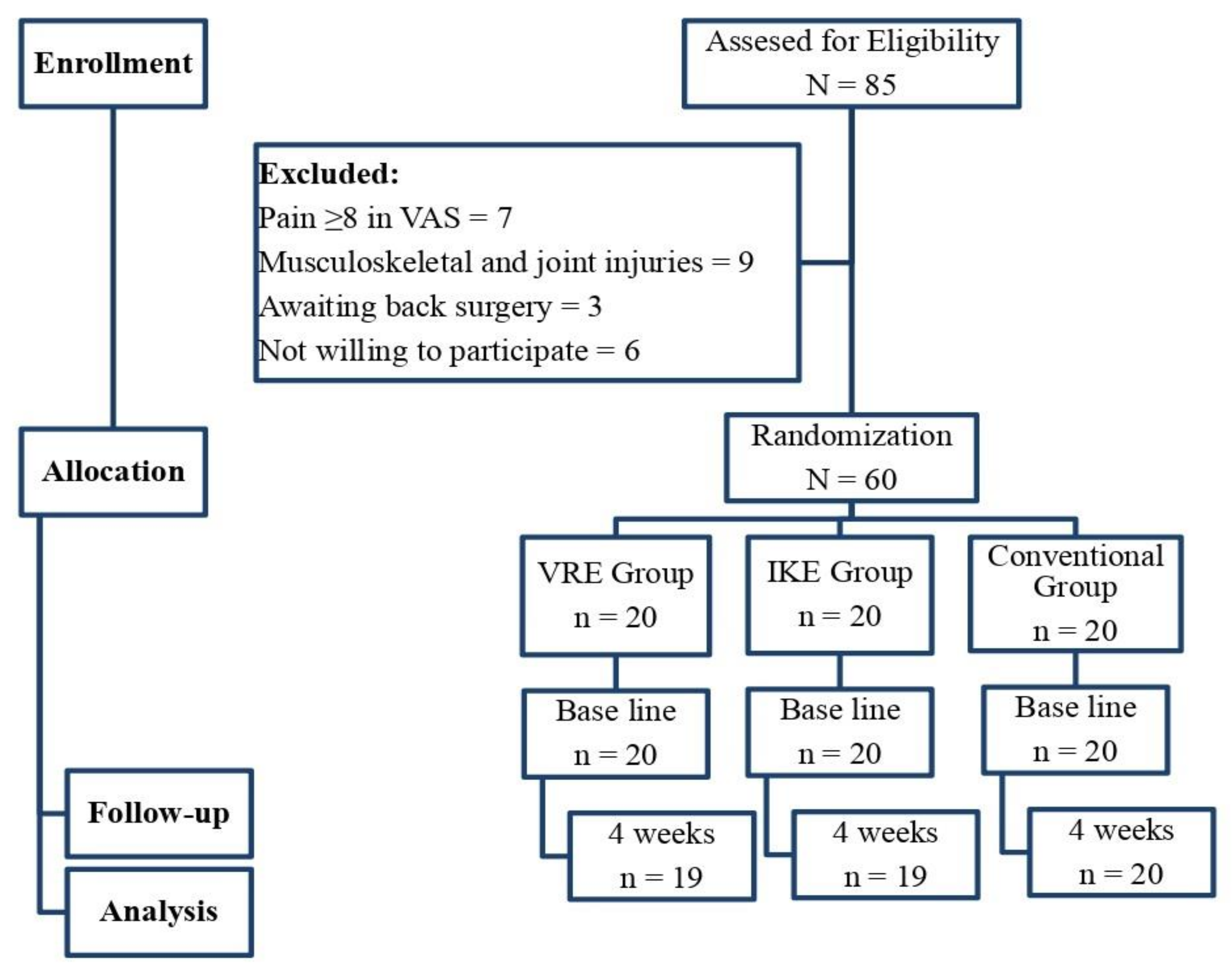
2.3. Recruitment, Randomization, and Allocation
2.4. Blinding
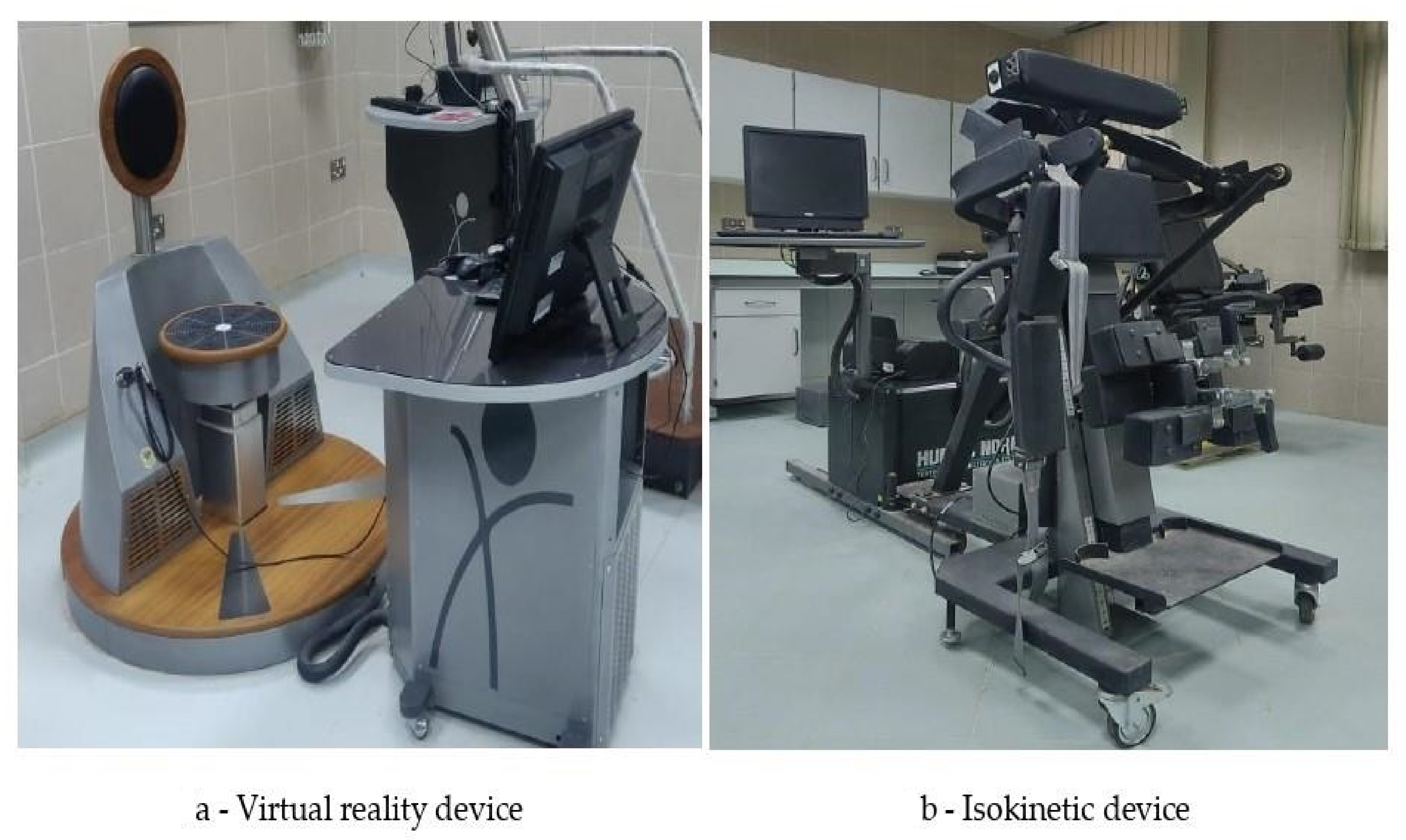
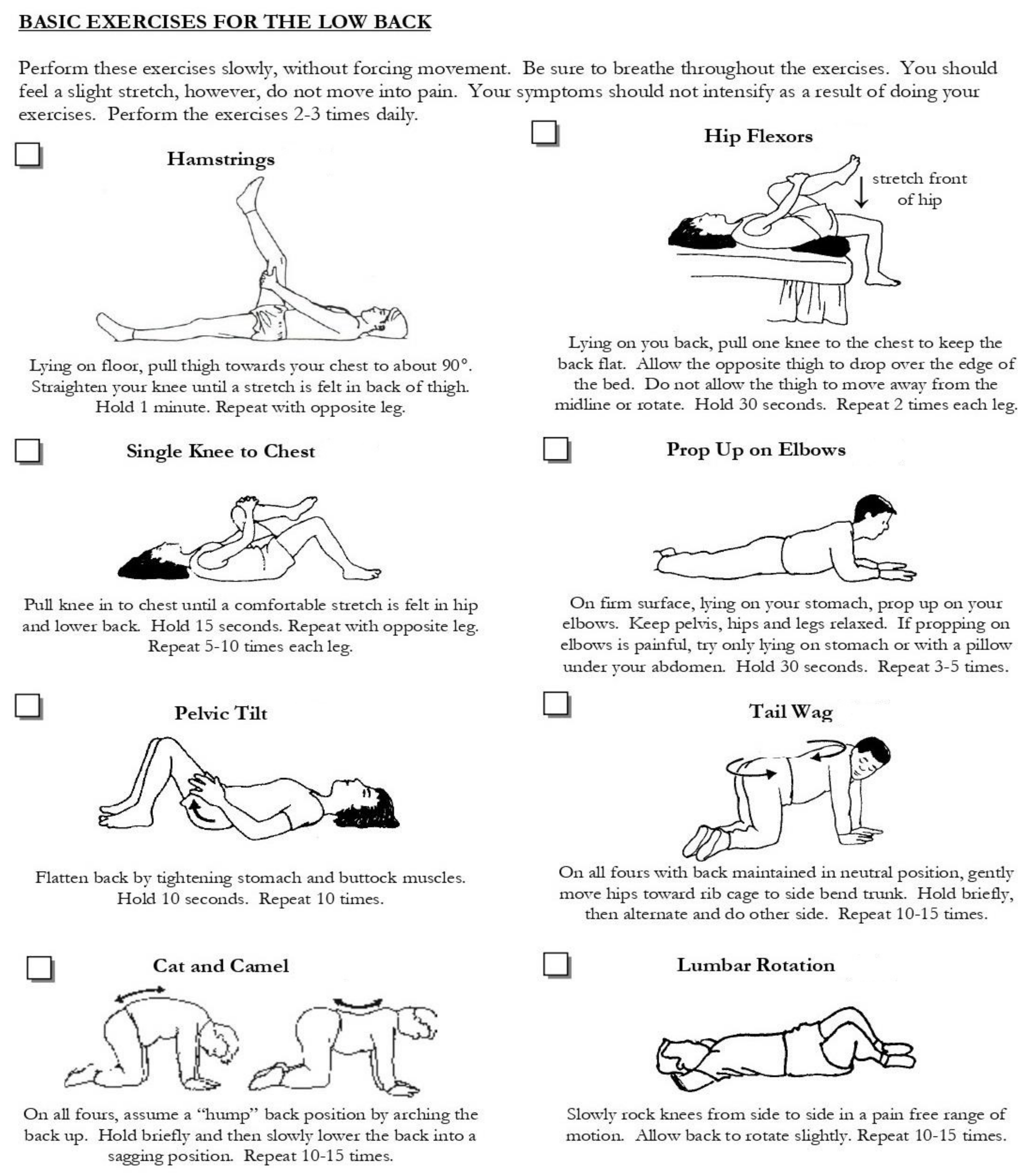
2.5. Interventions
2.6. Outcome Measures
2.6.1. Primary Outcome
2.6.2. Secondary Outcome
2.7. Sample Size
2.8. Statistical Tests
3. Results
3.1. Participants
3.2. Pain Intensity
3.3. Radiological Measures
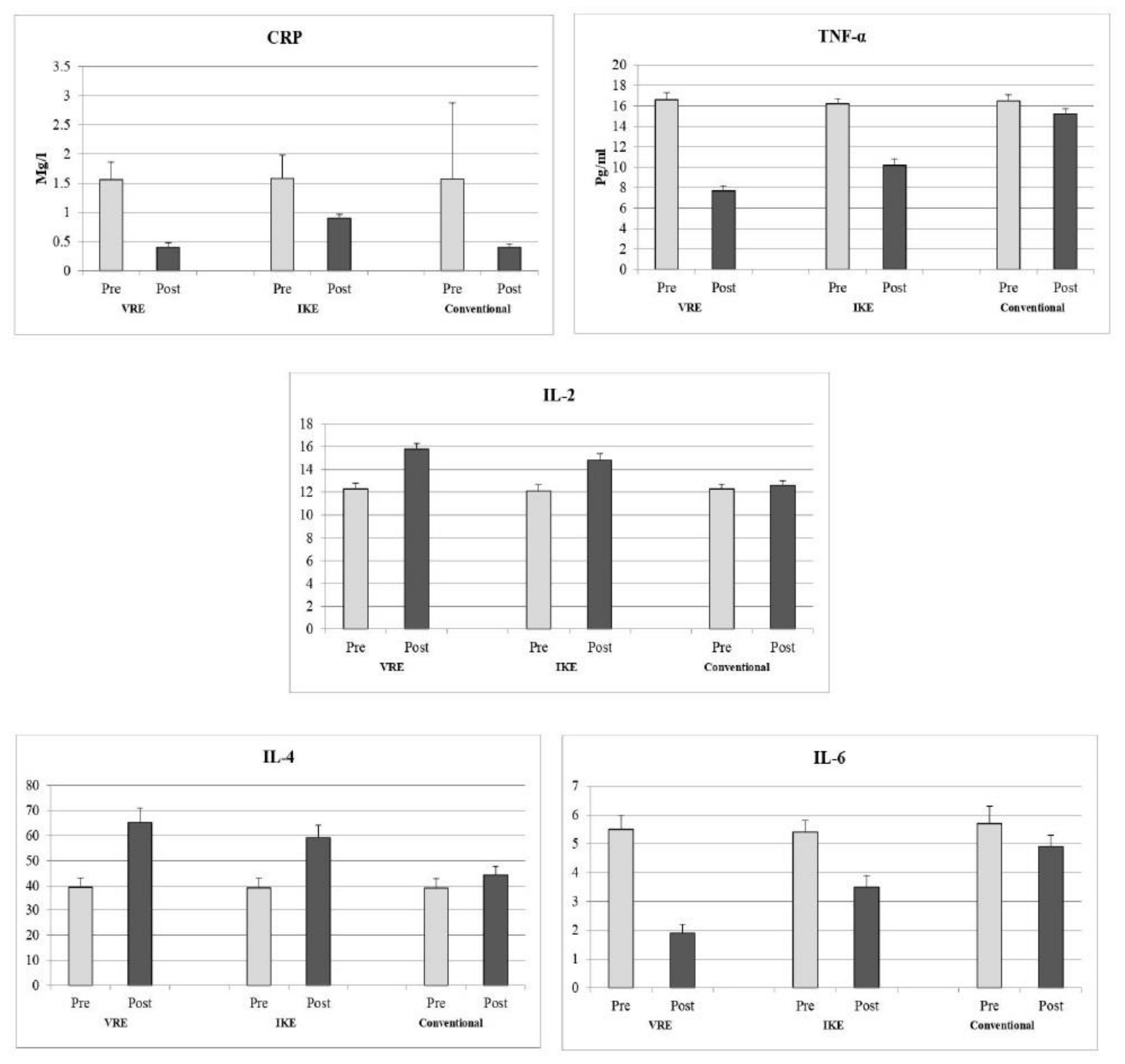
3.4. Inflammatory Biomarker Measures
4. Discussion
4.1. Radiological Measures
4.2. Inflammatory Biomarker Measures
5. Strength and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Myrick, K.M. Head Injuries in Soccer. Rehabil. Nurs. 2016, 41, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Nandlall, N.; Rivaz, H.; Rizk, A.; Frenette, S.; Boily, M.; Fortin, M. The effect of low back pain and lower limb injury on lumbar multifidus muscle morphology and function in university soccer players. BMC Musculoskelet. Disord. 2020, 21, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maselli, F.; Storari, L.; Barbari, V.; Colombi, A.; Turolla, A.; Gianola, S.; Rossettini, G.; Testa, M. Prevalence and incidence of low back pain among runners: A systematic review. BMC Musculoskelet. Disord. 2020, 21, 343. [Google Scholar] [CrossRef] [PubMed]
- Urits, I.; Burshtein, A.; Sharma, M.; Testa, L.; Gold, P.A.; Orhurhu, V.; Viswanath, O.; Jones, M.R.; Sidransky, M.A.; Spektor, B.; et al. Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment. Curr. Pain Headache Rep. 2019, 23, 23. [Google Scholar] [CrossRef]
- Bliven, K.C.H.; Anderson, B.E. Core stability training for injury prevention. Sports Health 2013, 5, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Ganesh, G.S.; Chhabra, D.; Pattnaik, M.; Mohanty, P.; Patel, R.; Mrityunjay, K. Effect of trunk muscles training using a star excursion balance test grid on strength, endurance and disability in persons with chronic low back pain. J. Back Musculoskelet. Rehabil. 2015, 28, 521–530. [Google Scholar] [CrossRef]
- Lauersen, J.B.; Bertelsen, D.M.; Andersen, L.B. The effectiveness of exercise interventions to prevent sports injuries: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2014, 48, 871–877. [Google Scholar] [CrossRef]
- Hill, J.; Leiszler, M. Review and role of plyometrics and core rehabilitation in competitive sport. Curr. Sports Med. Rep. 2011, 10, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Zemková, E.; Zapletalová, L. Back Problems: Pros and Cons of Core Strengthening Exercises as a Part of Athlete Training. Int. J. Environ. Res. Public Health 2021, 18, 5400. [Google Scholar] [CrossRef]
- Reiman, M.P.; Lorenz, D.S. Integration of strength and conditioning principles into a rehabilitation program. Int. J. Sports Phys. Ther. 2011, 6, 241–253. [Google Scholar]
- Nambi, G.; Kamal, W.; Shanmugananath, E.S.; Joshi, S.; Trivedi, P. Spinal manipulation plus laser therapy versus laser therapy alone in the treatment of chronic non-specific low back pain: A randomized controlled study. Eur. J. Phys. Rehabil. Med. 2018, 54, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; McDonough, D.J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.S.; Requejo, P.; Flynn, S.M.; Rizzo, A.A.; Valero-Cuevas, F.J.; Baker, L.; Winstein, C. The potential of virtual reality and gaming to assist successful aging with disability. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 339–356. [Google Scholar] [CrossRef] [PubMed]
- Adamovich, S.V.; Fluet, G.G.; Tunik, E.; Merians, A.S. Sensorimotor training in virtual reality: A review. NeuroRehabilitation 2009, 25, 29–44. [Google Scholar] [CrossRef] [Green Version]
- Vourvopoulos, A.; Bermúdez, I.; Badia, S. Motor priming in virtual reality can augment motor-imagery training efficacy in restorative brain-computer interaction: A within-subject analysis. J. Neuroeng. Rehabil. 2016, 13, 69. [Google Scholar] [CrossRef] [Green Version]
- Ho, C.-W.; Chen, L.-C.; Hsu, H.-H.; Chiang, S.-L.; Li, M.-H.; Jiang, S.-H.; Tsai, K.-C. Isokinetic muscle strength of the trunk and bilateral knees in young subjects with lumbar disc herniation. Spine 2005, 30, E528–E533. [Google Scholar] [CrossRef] [PubMed]
- Dvir, Z.; Keting, J.L. Trunk extension effort in patients with chronic low back dysfunction. Spine 2003, 28, 685–692. [Google Scholar] [CrossRef]
- Calmes, P.; Jacob, J.F.; Fayolle-Minon, I.; Charles, C.; Bouchet, J.P.; Rimaud, D.; Thomas, T. Use of isokinetic techniques vs Standard physiotherapy in patients with chronic low back pain. Preliminary results. Ann. Readapt Med. Phys. 2004, 47, 20–27. [Google Scholar]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
- Krzysztofik, M.; Wilk, M.; Wojdała, G.; Gołaś, A. Maximizing Muscle Hypertrophy: A Systematic Review of Advanced Resistance Training Techniques and Methods. Int. J. Environ. Res. Public Health 2019, 16, 4897. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.I.; Song, J.; Lee, H.S.; Kang, J.Y.; Kim, M.; Ryu, J.S. Association between Cross-sectional Areas of Lumbar Muscles on Magnetic Resonance Imaging and Chronicity of Low Back Pain. Ann. Rehabil. Med. 2011, 35, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Sions, J.M.; Teyhen, D.S.; Hicks, G.E. Criterion Validity of Ultrasound Imaging: Assessment of Multifidi Cross-Sectional Area in Older Adults with and Without Chronic Low Back Pain. J. Geriatr. Phys. Ther. 2017, 40, 74–79. [Google Scholar] [CrossRef]
- Klyne, D.M.; Barbe, M.F.; Hodges, P.W. Systemic inflammatory profiles and their relationships with demographic, behavioural and clinical features in acute low back pain. Brain Behav. Immun. 2017, 60, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wi, S.-Y.; Kang, J.-H. The Effects of Virtual Reality Interactive Games on the Balance Ability of Elderly Women with Knee Osteoarthritis. J. Phys. 2012, 7, 387–393. [Google Scholar]
- Sertpoyraz, F.; Eyigor, S.; Karapolat, H.; Capaci, K.; Kirazli, Y. Comparison of isokinetic exercise versus standard exercise training in patients with chronic low back pain: A randomized controlled study. Clin. Rehabil. 2009, 23, 238–247. [Google Scholar] [CrossRef]
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring with a Traditional Paper-based Visual Analog Scale in Adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Rosenstein, B.; Levesque, J.; Nandlall, N. Ultrasound Imaging Analysis of the Lumbar Multifidus Muscle Echo Intensity: Intra-Rater and Inter-Rater Reliability of a Novice and an Experienced Rater. Medicina 2021, 57, 512. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.; Ali, K.; Merritt, M.; Pelletier, J.; Macedo, L.G. A systematic review of the role of inflammatory biomarkers in acute, subacute and chronic non-specific low back pain. BMC Musculoskelet. Disord. 2020, 21, 142. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [Green Version]
- Noonan, A.M.; Brown, S.H.M. Paraspinal muscle pathophysiology associated with low back pain and spine degenerative disorders. JOR Spine 2021, 4, e1171. [Google Scholar] [CrossRef]
- Gold, J.I.; Belmont, K.A.; Thomas, D.A. The neurobiology of virtual reality pain attenuation. Cyberpsychol. Behav. 2007, 10, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, K.L.; Shamley, D.R.; Jackson, D. Changes in the cross-sectional area of multifidus and psoas in patients with unilateral back pain: The relationship to pain and disability. Spine 2004, 29, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Lim, W.H.; Park, J.W.; Kwon, B.S.; Ryu, K.H.; Lee, J.H.; Park, Y.H. The Relationship between Cross Sectional Area and Strength of Back Muscles in Patients with Chronic Low Back Pain. Ann. Rehabil. Med. 2012, 36, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kang, S.J. The effects of strength exercise and walking on lumbar function, pain level, and body composition in chronic back pain patients. J. Exerc. Rehabil. 2016, 12, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Nambi, G.; Abdelbasset, W.K.; Elsayed, S.H.; Alrawaili, S.M.; Abodonya, A.M.; Saleh, A.K.; Elnegamy, T.E. Comparative Effects of Isokinetic Training and Virtual Reality Training on Sports Performances in University Football Players with Chronic Low Back Pain-Randomized Controlled Study. Evid. Based Complement Alternat. Med. 2020, 2020, 2981273. [Google Scholar] [CrossRef]
- Tiedemann, A.; Sherrington, C.; Lord, S.R. The role of exercise for fall prevention in older age. Mot. Rev. De Educ. Fis. 2013, 19, 541–547. [Google Scholar] [CrossRef]
- Lee, J.C.; Cha, J.G.; Kim, Y.; Kim, Y.I.; Shin, B.J. Quantitative analysis of back muscle degeneration in the patients with the degenerative lumbar flat back using a digital image analysis: Comparison with the normal controls. Spine 2008, 33, 318–325. [Google Scholar] [CrossRef]
- Gebhardt, K.; Brenner, H.; Stürmer, T.; Raum, E.; Richter, W.; Schitenwolf, M.; Buchner, M. The course of high-sensitive C-reactive protein in correlation with pain and clinical function in patients with acute lumbosciatic pain and chronic low back pain—A 6 months prospective longitudinal study. Eur. J. Pain 2006, 10, 711–719. [Google Scholar] [CrossRef]
- Almuzaini, K.S.; Potteiger, J.A.; Green, S.B. Effects of split exercise sessions on excess post exercise oxygen consumption and resting metabolic rate. Can. J. Appl. Physiol. 1998, 23, 433–443. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef]
- Da Cruz Fernandes, I.M.; Pinto, R.Z.; Ferreira, P.; Lira, F.S. Low back pain, obesity, and inflammatory markers: Exercise as potential treatment. J. Exerc. Rehabil. 2018, 14, 168–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libardi, C.A.; De Souza, G.V.; Cavaglieri, C.R.; Madruga, V.A.; Chacon-Mikahil, M.P. Effect of resistance, endurance, and concurrent training on TNF-α, IL-6, and CRP. Med. Sci. Sports Exerc. 2012, 44, 50–56. [Google Scholar] [CrossRef]
- Hamer, M.; Sabia, S.; Batty, G.D.; Shipley, M.J.; Tabák, A.G.; Singh-Manoux, A.; Kivimaki, M. Physical activity and inflammatory markers over 10 years: Follow-up in men and women from the Whitehall II cohort study. Circulation 2012, 126, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Hart, M.J.; Torres, S.J.; McNaughton, S.A.; Milte, C.M. Dietary patterns and associations with biomarkers of inflammation in adults: A systematic review of observational studies. Nutr. J. 2021, 20, 24. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No | Variable | VRE | IKE | Conventional | p-Value |
| 1 | Age (year) | 23.2 ± 1.6 | 22.9 ± 1.7 | 22.8 ± 1.8 | 0.742 * |
| 2 | Height (meter) | 1.72 ± 0.16 | 1.69 ± 0.17 | 1.72 ± 0.18 | 0.813 * |
| 3 | Weight (kilogram) | 69.5 ± 2.8 | 70.2 ± 2.4 | 71.6 ± 2.9 | 0.051 * |
| 4 | BMI (kg/m2) | 24.5 ± 1.5 | 23.8 ± 1.4 | 24.2 ± 1.5 | 0.325 * |
| 5 | maxVO2 peak (mL/kg/min) | 38.2 ± 4.2 | 38.6 ± 4.3 | 37.8 ± 4.3 | 0.839 * |
| 6 | HR (beats/min) | 74 ± 6.5 | 73 ± 6.6 | 72 ± 7.2 | 0.648 * |
| 7 | Years of playing (year) | 5.1 ± 1.3 | 4.9 ± 1.4 | 4.8 ± 1.3 | 0.770 * |
| 8 | Duration of Injury (months) | 4.8 ± 1.1 | 5.2 ± 0.9 | 5.5 ± 0.8 | 0.070 * |
| No | Variable | VRE | IKE | Conventional | F-Score | p-Value | |
|---|---|---|---|---|---|---|---|
| 1 | Pain intensity | Pre | 7.2 ± 0.4 | 7.3 ± 0.3 | 7.2 ± 0.3 | 295.60 | 0.558 * |
| VAS (cm) | Post | 1.8 ± 0.3 | 2.5 ± 0.5 | 4.8 ± 0.4 | 0.001 ** | ||
| 2 | Psoas Major CSA (cm2)—R | Pre | 8.6 ± 0.4 | 8.5 ± 0.5 | 8.5 ± 0.4 | 102.06 | 0.705 * |
| Post | 9.5 ± 0.3 | 10.1 ± 0.4 | 8.7 ± 0.2 | 0.001 ** | |||
| 3 | Psoas Major CSA (cm2)—L | Pre | 7.9 ± 0.5 | 8.2 ± 0.4 | 8.1 ± 0.5 | 170.34 | 0.271 * |
| Post | 9.5 ± 0.4 | 10.2 ± 0.3 | 8.4 ± 0.2 | 0.001 ** | |||
| 4 | Quadratus. Lumb CSA (cm2)—R | Pre | 4.6 ± 0.3 | 4.8 ± 0.4 | 4.7 ± 0.6 | 88.82 | 0.380 * |
| Post | 5.8 ± 0.3 | 6.3 ± 0.4 | 4.9 ± 0.3 | 0.001 ** | |||
| 5 | Quadratus. Lumb CSA (cm2)—L | Pre | 4.7 ± 0.6 | 4.5 ± 0.5 | 4.3 ± 0.5 | 197.64 | 0.069 * |
| Post | 6.5 ± 0.3 | 6.9 ± 0.4 | 4.9 ± 0.3 | 0.001 ** | |||
| 6 | Multifidus CSA (cm2)—R | Pre | 5.6 ± 0.6 | 5.4 ± 0.6 | 5.5 ± 0.5 | 90.87 | 0.542 * |
| Post | 7.1 ± 0.5 | 7.6 ± 0.4 | 5.8 ± 0.4 | 0.001 ** | |||
| 7 | Multifidus CSA (cm2)—L | Pre | 5.5 ± 0.5 | 5.6 ± 0.6 | 5.6 ± 0.7 | 71.25 | 0.834 * |
| Post | 6.8 ± 0.4 | 7.4 ± 0.4 | 5.9 ± 0.4 | 0.001 ** | |||
| 8 | Erector Spinae CSA (cm2)—R | Pre | 16.2 ± 0.9 | 15.9 ± 1.3 | 16.1 ± 1.2 | 45.97 | 0.702 * |
| Post | 17.5 ± 0.5 | 18.1 ± 0.6 | 16.4 ± 0.6 | 0.001 ** | |||
| 9 | Erector Spinae CSA (cm2)—L | Pre | 16.4 ± 1.3 | 16.5 ± 0.9 | 16.6 ± 1.2 | 22.62 | 0.859 * |
| Post | 17.7 ± 0.7 | 18.1 ± 0.5 | 16.9 ± 0.5 | 0.001 ** | |||
| 10 | Multifidus Thickness (mm)—R | Pre | 33.8 ± 3.3 | 33.6 ± 3.4 | 32.9 ± 3.6 | 6.50 | 0.686 * |
| Post | 35.2 ± 2.2 | 35.4 ± 2.3 | 33.1 ± 2.2 | 0.002 ** | |||
| 11 | Multifidus Thickness (mm)—L | Pre | 31.5 ± 2.6 | 31.6 ± 2.8 | 32.1 ± 3.2 | 3.20 | 0.780 * |
| Post | 33.5 ± 2.1 | 34.2 ± 2.1 | 32.5 ± 2.2 | 0.047 ** |
| Sr. No | Variable | VRE | IKE | Conventional | F-Score | p-Value | |
| 1 | CRP mg/L | Pre | 1.56 ± 0.3 | 1.58 ± 0.4 | 1.57 ± 0.4 | 818.79 | 0.985 * |
| Post | 0.4 ± 0.08 | 0.9 ± 0.07 | 1.3 ± 0.06 | 0.001 ** | |||
| 2 | TNF-α pg/mL | Pre | 16.6 ± 0.7 | 16.2 ± 0.5 | 16.5 ± 0.6 | 1017.44 | 0.103 * |
| Post | 7.7 ± 0.5 | 10.2 ± 0.6 | 15.2 ± 0.5 | 0.001 ** | |||
| 3 | IL-2 pg/mL | Pre | 12.3 ± 0.5 | 12.1 ± 0.6 | 12.3 ± 0.4 | 208.83 | 0.360 * |
| Post | 15.8 ± 0.5 | 14.8 ± 0.6 | 12.6 ± 0.4 | 0.001 ** | |||
| 4 | IL-4 pg/mL | Pre | 39.5 ± 3.6 | 39.3 ± 3.7 | 39.2 ± 3.6 | 103.55 | 0.965 * |
| Post | 65.3 ± 5.6 | 59.2 ± 4.9 | 44.3 ± 3.5 | 0.001 ** | |||
| 5 | IL-6 pg/mL | Pre | 5.5 ± 0.5 | 5.4 ± 0.4 | 5.7 ± 0.6 | 329.75 | 0.171 * |
| Post | 1.9 ± 0.3 | 3.5 ± 0.4 | 4.9 ± 0.4 | 0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nambi, G.; Alghadier, M.; Kashoo, F.Z.; Aldhafian, O.R.; Nwihadh, N.A.; Saleh, A.K.; Omar, M.A.; Hassan, T.G.T.; Ibrahim, M.N.A.; El Behairy, H.F.; et al. Effects of Virtual Reality Exercises versus Isokinetic Exercises in comparison with Conventional Exercises on the Imaging Findings and Inflammatory Biomarker Changes in Soccer Players with Non-Specific Low Back Pain: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 524. https://doi.org/10.3390/ijerph20010524
Nambi G, Alghadier M, Kashoo FZ, Aldhafian OR, Nwihadh NA, Saleh AK, Omar MA, Hassan TGT, Ibrahim MNA, El Behairy HF, et al. Effects of Virtual Reality Exercises versus Isokinetic Exercises in comparison with Conventional Exercises on the Imaging Findings and Inflammatory Biomarker Changes in Soccer Players with Non-Specific Low Back Pain: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(1):524. https://doi.org/10.3390/ijerph20010524
Chicago/Turabian StyleNambi, Gopal, Mshari Alghadier, Faizan Zaffar Kashoo, Osama R. Aldhafian, Naif A. Nwihadh, Ayman K. Saleh, Mohamed A. Omar, Tohamy G. T. Hassan, Mohamed Nagah Ahmed Ibrahim, Hassan Fathy El Behairy, and et al. 2023. "Effects of Virtual Reality Exercises versus Isokinetic Exercises in comparison with Conventional Exercises on the Imaging Findings and Inflammatory Biomarker Changes in Soccer Players with Non-Specific Low Back Pain: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 1: 524. https://doi.org/10.3390/ijerph20010524
APA StyleNambi, G., Alghadier, M., Kashoo, F. Z., Aldhafian, O. R., Nwihadh, N. A., Saleh, A. K., Omar, M. A., Hassan, T. G. T., Ibrahim, M. N. A., El Behairy, H. F., Attallah, A. A., & Ismail, M. A. (2023). Effects of Virtual Reality Exercises versus Isokinetic Exercises in comparison with Conventional Exercises on the Imaging Findings and Inflammatory Biomarker Changes in Soccer Players with Non-Specific Low Back Pain: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(1), 524. https://doi.org/10.3390/ijerph20010524