


Reviewing Publicly Available Reports on Child Health Disparities in Indigenous and Remote Communities of Australia
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
Result Synthesis
3. Results
3.1. Data Sources
3.2. Sociodemographic and Housing Conditions
3.3. Maternal and Child Health Outcomes
3.4. Long-Term Health Conditions
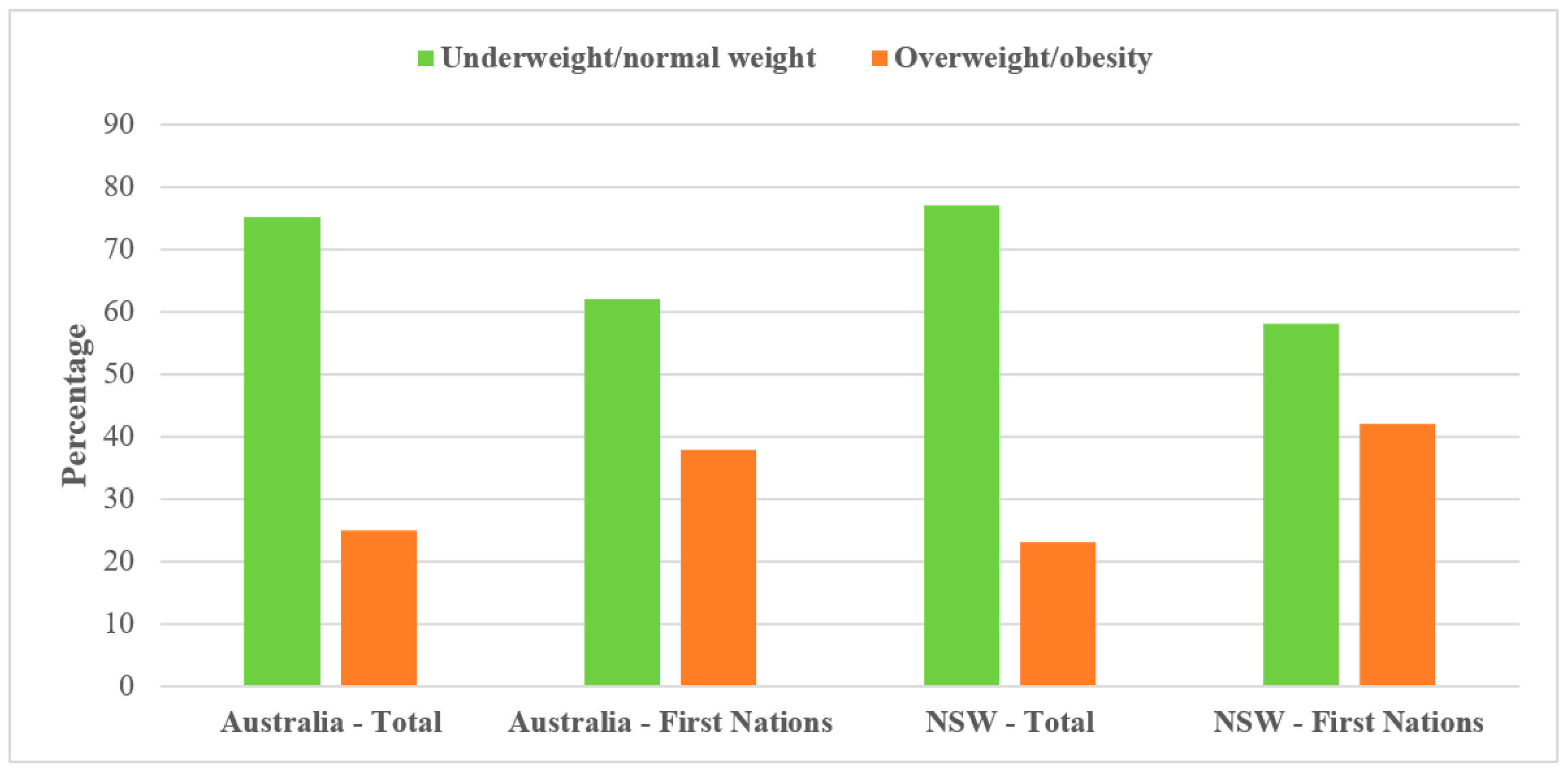
3.5. Overweight and/or Obesity
3.6. Fruit and Vegetable Consumption
3.7. Physical Activity and Sedentary Behaviours
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Health Inequities and Their Causes. 2018. Available online: https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes (accessed on 30 November 2022).
- National Academies of Sciences, Engineering, and Medicine. Communities in Action: Pathways to Health Equity; The National Academies Press: Washington, DC, USA, 2017; p. 582. [Google Scholar] [CrossRef]
- Braveman, P. Health Disparities and Health Equity: Concepts and Measurement. Annu. Rev. Public Health 2006, 27, 167–194. [Google Scholar] [CrossRef]
- Matthews, T.J.; MacDorman, M.F.; Thoma, M.E. Infant Mortality Statistics from the 2013 Period Linked Birth/Infant Death Data Set. Natl. Vital Stat. Rep. 2015, 64, 1–30. [Google Scholar]
- National Conference of State Legislatures. Health Disparities Overview. 2021. Available online: https://www.ncsl.org/research/health/health-disparities-overview.aspx (accessed on 30 November 2022).
- W.K. Kellogg Foundation. The Business Case for Racial Equity; W.K. Kellogg Foundation: Battle Creek, MI, USA, 2018. [Google Scholar]
- Gracey, M.; King, M. Indigenous health part 1: Determinants and disease patterns. Lancet 2009, 374, 65–75. [Google Scholar] [CrossRef]
- Zambas, S.I.; Wright, J. Impact of colonialism on Māori and Aboriginal healthcare access: A discussion paper. Contemp. Nurse 2016, 52, 398–409. [Google Scholar] [CrossRef]
- Pelcastre-Villafuerte, B.E.; Meneses-Navarro, S.; Sánchez-Domínguez, M.; Meléndez-Navarro, D.; Freyermuth-Encis, G. Health conditions and use of services amongindigenous peoples of Mexico. Salud Publica Mex. 2020, 62, 810–819. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and Causes of Illness and Death in Aboriginal and Torres Strait Islander People 2018; Australian Institute of Health and Welfare: Canberra, ACT, Australia, 2018.
- Sahle, B.W.; Owen, A.J.; Mutowo, M.P.; Krum, H.; Reid, C.M. Prevalence of heart failure in Australia: A systematic review. BMC Cardiovasc. Disord. 2016, 16, 32. [Google Scholar] [CrossRef]
- Gardiner, F.W.; Rallah-Baker, K.; Dos Santos, A.; Sharma, P.; Churilov, L.; Donnan, G.A.; Davis, S.M.; Quinlan, F.; Worley, P. Indigenous Australians have a greater prevalence of heart, stroke, and vascular disease, are younger at death, with higher hospitalisation and more aeromedical retrievals from remote regions. eClinicalMedicine 2021, 42, 101181. [Google Scholar] [CrossRef]
- Hare, M.J.L.; Zhao, Y.; Guthridge, S.; Burgess, P.; Barr, E.L.M.; Ellis, E.; Butler, D.; Rosser, A.; Falhammar, H.; Maple-Brown, L.J. Prevalence and incidence of diabetes among Aboriginal people in remote communities of the Northern Territory, Australia: A retrospective, longitudinal data-linkage study. BMJ Open 2022, 12, e059716. [Google Scholar] [CrossRef]
- Wang, Z.; Hoy, W.E.; Si, D. Incidence of type 2 diabetes in Aboriginal Australians: An 11-year prospective cohort study. BMC Public Health 2010, 10, 487. [Google Scholar] [CrossRef]
- Titmuss, A.; Davis, E.A.; Brown, A.; Maple-Brown, L.J. Emerging diabetes and metabolic conditions among Aboriginal and Torres Strait Islander young people. Med. J. Aust. 2019, 210, 111–113.e1. [Google Scholar] [CrossRef]
- Charlson, F.J.; Erskine, H.E. Burden of mental and substance use disorders in Indigenous Australians and Oceania. Australas. Psychiatry 2015, 23, 13–16. [Google Scholar] [CrossRef]
- Calabria, B.; Doran, C.M.; Vos, T.; Shakeshaft, A.P.; Hall, W. Epidemiology of alcohol-related burden of disease among Indigenous Australians. Aust. N. Z. J. Public Health 2010, 34 (Suppl. 1), S47–S51. [Google Scholar] [CrossRef]
- Atkinson-Briggs, S.; Jenkins, A.; Ryan, C.; Brazionis, L. Health-risk behaviours among Indigenous Australians with diabetes: A study in the integrated Diabetes Education and Eye Screening (iDEES) project. J. Adv. Nurs. 2022, 78, 1305–1316. [Google Scholar] [CrossRef]
- Gwynn, J.D.; Flood, V.M.; D’Este, C.A.; Attia, J.R.; Turner, N.; Cochrane, J.; Louie, J.C.; Wiggers, J.H. Poor food and nutrient intake among Indigenous and non-Indigenous rural Australian children. BMC Pediatr. 2012, 12, 12. [Google Scholar] [CrossRef]
- Shepherd, C.C.; Li, J.; Mitrou, F.; Zubrick, S.R. Socioeconomic disparities in the mental health of Indigenous children in Western Australia. BMC Public Health 2012, 12, 756. [Google Scholar] [CrossRef]
- Foster, T.; Hall, N.L. Housing conditions and health in Indigenous Australian communities: Current status and recent trends. Int. J. Environ. Health Res. 2021, 31, 325–343. [Google Scholar] [CrossRef]
- Andersen, M.J.; Williamson, A.B.; Fernando, P.; Redman, S.; Vincent, F. “There’s a housing crisis going on in Sydney for Aboriginal people”: Focus group accounts of housing and perceived associations with health. BMC Public Health 2016, 16, 429. [Google Scholar] [CrossRef]
- Closing the Gap. History of Closing the Gap. 2021. Available online: https://www.closingthegap.gov.au/resources/history (accessed on 30 November 2022).
- Coalition of Aboriginal and Torres Strait Islander Peak Organisations; Australian Governments. National Agreement on Closing the Gap; Australian Governments: Canberra, ACT, Australia, 2020.
- Commonwealth of Australia. Closing the Gap Report 2020; Department of the Prime Minister and Cabinet, Ed.; Commonwealth of Australia: Canberra, ACT, Australia, 2020.
- Australian Indigenous HealthInfoNet. Summary of Aboriginal and Torres Strait Islander Health Status—Selected Topics 2021; Australian Indigenous HealthInfoNet: Mount Lawley, WA, Australia, 2021. [Google Scholar]
- National Aboriginal Community Controlled Health Organisation; The Royal Australian College of General Practitioners. National Guide to a Preventive Health Assessment for Aboriginal and Torres Strait Islander People, 3rd ed.; The Royal Australian College of General Practitioners: East Melbourne, VIC, Australia, 2018. [Google Scholar]
- Australian Institute of Health and Welfare. Australia’s Mothers and Babies. 2022. Available online: https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-babies/contents/focus-population-groups/teenage-mothers (accessed on 1 December 2022).
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, ACT, Australia, 2013.
- Department of Health and Aged Care. Australia’s Physical Activity and Sedentary Behaviour Guidelines for Infants, Toddlers and Preschoolers (Birth to 5 Years). 2017. Available online: https://www.health.gov.au/topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians/for-infants-toddlers-and-preschoolers-birth-to-5-years (accessed on 19 December 2022).
- Australian Bureau of Statistics. Search Census Data. 2016. Available online: https://www.abs.gov.au/census/find-census-data/search-by-area (accessed on 17 September 2022).
- Australian Bureau of Statistics. Population: Census. 2021. Available online: https://www.abs.gov.au/statistics/people/population/population-census/latest-release (accessed on 28 November 2022).
- Australian Bureau of Statistics. National Health Survey: First Results. 2017–2018. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-first-results/latest-release (accessed on 25 November 2022).
- Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander Health Survey. 2018–2019. Available online: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/national-aboriginal-and-torres-strait-islander-health-survey/latest-release (accessed on 25 November 2022).
- Australian Bureau of Statistics. Australian Aboriginal and Torres Strait Islander Health Survey: First Results, Australia. 2012–2013. Available online: https://www.abs.gov.au/ausstats/[email protected]/Lookup/4727.0.55.001main+features802012-13#:~:text=General%20health,rated%20their%20health%20as%20poor (accessed on 28 November 2022).
- Australian Institute of Health and Welfare. Australian Children; AIHW: Canberra, ACT, Australia, 2020.
- Australian Institute of Health and Welfare. Australian Burden of Disease Study 2018: Key Findings for Aboriginal and Torres Strait Islander People. Available online: https://www.aihw.gov.au/reports/burden-of-disease/australian-bod-study-2018-key-findings-indigenous/contents/key-findings (accessed on 28 November 2022).
- Australian Institute of Health and Welfare. National Indigenous Australians Agency. Ear Health. 2022. Available online: https://www.indigenoushpf.gov.au/measures/1-15-ear-health (accessed on 1 December 2022).
- Australian Institute of Health and Welfare; National Indigenous Australians Agency. 2.18 Physical Activity. 2022. Available online: https://www.indigenoushpf.gov.au/measures/2-18-physical-activity (accessed on 5 December 2022).
- Valery, P.C.; Moloney, A.; Cotterill, A.; Harris, M.; Sinha, A.K.; Green, A.C. Prevalence of obesity and metabolic syndrome in Indigenous Australian youths. Obes. Rev. 2009, 10, 255–261. [Google Scholar] [CrossRef]
- Oudin, A.; Richter, J.C.; Taj, T.; Al-nahar, L.; Jakobsson, K. Poor housing conditions in association with child health in a disadvantaged immigrant population: A cross-sectional study in Rosengård, Malmö, Sweden. BMJ Open 2016, 6, e007979. [Google Scholar] [CrossRef]
- Perera, F.; Viswanathan, S.; Whyatt, R.; Tang, D.; Miller, R.L.; Rauh, V. Children’s environmental health research--highlights from the Columbia Center for Children’s Environmental Health. Ann. N. Y. Acad. Sci. 2006, 1076, 15–28. [Google Scholar] [CrossRef]
- An Australian Government Initiative. Closing the Gap on Indigenous Disadvantage: The Challange for Australia; An Australian Government Initiative: Canberra, ACT, Australia, 2009.
- Torzillo, P.J.; Pholeros, P.; Rainow, S.; Barker, G.; Sowerbutts, T.; Short, T.; Irvine, A. The state of health hardware in Aboriginal communities in rural and remote Australia. Aust. N. Z. J. Public Health 2008, 32, 7–11. [Google Scholar] [CrossRef]
- Greenhalgh, E.; Ford, C.; Winstanley, M. 3.8—Child health and maternal smoking before and after birth. In Tobacco in Australia: Facts and Issues; Greenhalgh, E., Scollo, M.M., Winstanley, M.H., Eds.; Cancer Council Victoria: Melbourne, VIC, Australia, 2021. [Google Scholar]
- Banderali, G.; Martelli, A.; Landi, M.; Moretti, F.; Betti, F.; Radaelli, G.; Lassandro, C.; Verduci, E. Short and long term health effects of parental tobacco smoking during pregnancy and lactation: A descriptive review. J. Transl. Med. 2015, 13, 327. [Google Scholar] [CrossRef]
- Avşar, T.S.; McLeod, H.; Jackson, L. Health outcomes of smoking during pregnancy and the postpartum period: An umbrella review. BMC Pregnancy Childbirth 2021, 21, 254. [Google Scholar] [CrossRef]
- Hamułka, J.; Zielińska, M.A.; Chądzyńska, K. The combined effects of alcohol and tobacco use during pregnancy on birth outcomes. Rocz. Panstw. Zakl. Hig. 2018, 69, 45–54. [Google Scholar]
- Gould, G.S.; Patten, C.; Glover, M.; Kira, A.; Jayasinghe, H. Smoking in Pregnancy Among Indigenous Women in High-Income Countries: A Narrative Review. Nicotine Tob. Res. 2017, 19, 506–517. [Google Scholar] [CrossRef]
- Jeha, D.; Usta, I.; Ghulmiyyah, L.; Nassar, A. A review of the risks and consequences of adolescent pregnancy. J. Neonatal Perinatal Med. 2015, 8, 1–8. [Google Scholar] [CrossRef]
- Marino, J.L.; Lewis, L.N.; Hickey, M.; Skinner, S.R.; Bateson, D. Teenage mothers. Aust. J. Gen. Pract. 2016, 45, 712–717. [Google Scholar]
- Heywood, W.; Patrick, K.; Smith, A.M.; Pitts, M.K. Associations between early first sexual intercourse and later sexual and reproductive outcomes: A systematic review of population-based data. Arch. Sex. Behav. 2015, 44, 531–569. [Google Scholar] [CrossRef]
- True, K.; Bajos, N.; Bohet, A.; Moreau, C. Timing of contraceptive initiation and association with future sexual and reproductive outcomes. Hum. Reprod. 2014, 29, 1651–1658. [Google Scholar] [CrossRef]
- Kim, K. Intergenerational Transmission of Age at First Birth in the United States: Evidence from Multiple Surveys. Popul. Res. Policy Rev. 2014, 33, 649–671. [Google Scholar] [CrossRef]
- Gaudie, J.; Mitrou, F.; Lawrence, D.; Stanley, F.J.; Silburn, S.R.; Zubrick, S.R. Antecedents of teenage pregnancy from a 14-year follow-up study using data linkage. BMC Public Health 2010, 10, 63. [Google Scholar] [CrossRef]
- Batchelor, M.; Brown, S.J.; Glover, K.; Gartland, D. A Systematic Review of Child Health and Developmental Outcomes Associated with Low Birthweight and/or Small for Gestational Age in Indigenous Children from Australia, Canada and New Zealand. Int. J. Environ. Res. Public Health 2021, 18, 12669. [Google Scholar] [CrossRef]
- Gibberd, A.J.; Simpson, J.M.; Jones, J.; Williams, R.; Stanley, F.; Eades, S.J. A large proportion of poor birth outcomes among Aboriginal Western Australians are attributable to smoking, alcohol and substance misuse, and assault. BMC Pregnancy Childbirth 2019, 19, 110. [Google Scholar] [CrossRef]
- Sherriff, S.; Baur, L.; Lambert, M.; Dickson, M.; Eades, S.; Muthayya, S. Aboriginal childhood overweight and obesity: The need for Aboriginal designed and led initiatives. Public Health Res. Pract. 2019, 29, e2941925. [Google Scholar] [CrossRef]
- Vos, T.; Barker, B.; Begg, S.; Stanley, L.; Lopez, A.D. Burden of disease and injury in Aboriginal and Torres Strait Islander Peoples: The Indigenous health gap. Int. J. Epidemiol. 2009, 38, 470–477. [Google Scholar] [CrossRef]
- Halford, J.C.; Boyland, E.J.; Hughes, G.M.; Stacey, L.; McKean, S.; Dovey, T.M. Beyond-brand effect of television food advertisements on food choice in children: The effects of weight status. Public Health Nutr. 2008, 11, 897–904. [Google Scholar] [CrossRef]
- Thurber, K.A.; Dobbins, T.; Neeman, T.; Banwell, C.; Banks, E. Body mass index trajectories of Indigenous Australian children and relation to screen time, diet, and demographic factors. Obesity 2017, 25, 747–756. [Google Scholar] [CrossRef]
- Ritchie, S.A.; Connell, J.M.C. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef]
- Lockeridge, A.; Innes-Hughes, C.; O’Hara, B.J.; McGill, B.; Rissel, C. Munch & Move: Evidence and Evaluation Summary; Ministry of Health North Sydney: Sydney, NSW, Australia, 2015.
- Bravo, A.; Innes-Hughes, C.; O’Hara, B.J.; McGill, B.; Rissel, C. Live Life Well @ School: Evidence and Evaluation Summary 2008–2015; Ministry of Health North Sydney: Sydney, NSW, Australia, 2016.
- Welsby, D.; Nguyen, B.; O’Hara, B.J.; Innes-Hughes, C.; Bauman, A.; Hardy, L.L. Process evaluation of an up-scaled community based child obesity treatment program: NSW Go4Fun®. BMC Public Health 2014, 14, 140. [Google Scholar] [CrossRef]
- Williams, S.L.; Van Lippevelde, W.; Magarey, A.; Moores, C.J.; Croyden, D.; Esdaile, E.; Daniels, L. Parent engagement and attendance in PEACH™ QLD—An up-scaled parent-led childhood obesity program. BMC Public Health 2017, 17, 559. [Google Scholar] [CrossRef]
- Foley, W. Family food work: Lessons learned from urban Aboriginal women about nutrition promotion. Aust. J. Prim. Health 2010, 16, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Henryks, J.; Brimblecombe, J. Mapping Point-of-Purchase Influencers of Food Choice in Australian Remote Indigenous Communities: A Review of the Literature. SAGE Open 2016, 6, 2158244016629183. [Google Scholar] [CrossRef]
- Thurber, K.A.; Banwell, C.; Neeman, T.; Dobbins, T.; Pescud, M.; Lovett, R.; Banks, E. Understanding barriers to fruit and vegetable intake in the Australian Longitudinal Study of Indigenous Children: A mixed-methods approach. Public Health Nutr. 2017, 20, 832–847. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Data Sources | Research Organisation | Scope of the Data | Measurements | Outcomes | Data Access |
|---|---|---|---|---|---|
| Population: Census 2021 | Australian Bureau of Statistics (ABS) | The 2021 Census counted 25,422,788 people in Australia (excludes overseas visitors) | Self-reported data | Sociodemographic outcomes | Population: Census, 2021 | Australian Bureau of Statistics (abs.gov.au) [accessed on 28 November 2022] |
| Population: Census 2016 | Australian Bureau of Statistics (ABS) | The 2016 Census counted 23.4 million people living in Australia (excludes overseas visitors) | Self-reported data | Housing | 2016 Australia, Census All persons QuickStats | Australian Bureau of Statistics (abs.gov.au) [accessed on 17 September 2022] |
| Report on Australian children 2020 | Australian Institute of Health and Welfare | Examines data on children and their families across seven domains: health, education, social support, household income and finance, parental employment, housing, and justice and safety. | Using different data sources | Smoking during pregnancy; teenage motherhood; low birth weight; child mortality; developmental vulnerability; asthma; Type I diabetes; cancer | Australia’s children (Full publication; 18 March 2020 Edition) (AIHW) |
| National Health Survey: First results 2017–2018 | Australian Bureau of Statistics (ABS) | The NHS was conducted from a sample of approximately 21,300 people in 16,400 private dwellings across Australia. | Self-reported data and physical measurements | Mental and behavioural conditions; overweight/obesity; dietary intake; physical activity | National Health Survey: First results, 2017–2018 financial year | Australian Bureau of Statistics (abs.gov.au) [accessed on 25 November 2022] |
| National Aboriginal and Torres Strait Islander Health Survey 2018–2019 | Australian Bureau of Statistics (ABS) | From a total of 6388 households, 10,579 people included in the sample. | Self-reported and physical measurements | Overweight/obesity; dietary intake; physical activity | National Aboriginal and Torres Strait Islander Health Survey, 2018–2019 financial year | Australian Bureau of Statistics (abs.gov.au) [accessed on 25 November 2022] |
| Australian Burden of Disease Study 2018 | Australian Institute of Health and Welfare | Australian Burden of Disease Study 2018: key findings for Aboriginal and Torres Strait Islander people | Estimates of DALYs, YLL and life expectancy | Burden of diseases | Australian Burden of Disease Study 2018: key findings for Aboriginal and Torres Strait Islander people, Key findings—Australian Institute of Health and Welfare (aihw.gov.au) [accessed on 28 November 2022] |
| National Aboriginal and Torres Strait Islander Health Survey 2012–2013 | Australian Bureau of Statistics (ABS) | From a total of 7700 households, around 9300 people included in the sample. | Self-reported and physical measurements | Asthma; overweight/obesity; dietary intake; physical activity | 4727.0.55.001—Australian Aboriginal and Torres Strait Islander Health Survey: First Results, Australia, 2012–2013 (abs.gov.au) [accessed on 28 November 2022 |
| Health status and outcomes: ear health | Australian Institute of Health and Welfare & National Indigenous Australians Agency | Aboriginal and Torres Strait Islander health performance framework | Using different data sources | Hearing impairment | 1.15 Ear health—AIHW Indigenous HPF [accessed on 1 December 2022] |
| Health status and outcomes: physical activity | Australian Institute of Health and Welfare & National Indigenous Australians Agency | Aboriginal and Torres Strait Islander health performance framework | Using different data sources | Physical activity | 2.18 Physical activity—AIHW Indigenous HPF [accessed on 5 December 2022] |
| MEDLINE/PUBMED | From a total of 158 children aged 5–17 years | Cross-sectional study | Central obesity | Prevalence of obesity and metabolic syndrome in Indigenous Australian youths—Valery—2009—Obesity Reviews—Wiley Online Library |
| Variables | Australia | |
|---|---|---|
| Total Population | Indigenous | |
| Median age (years) | 38 | 24 |
| <15 years (%) | 18.2 | 32.7 |
| ≥65 years (%) | 17.2 | 5.9 |
| Number of children per household | 2.5 | 3.1 |
| Median weekly household income | $1746 | $1507 |
| Median monthly mortgage repayments | $1863 | $1721 |
| Completed year 12 or higher education (%) | 66.7 | 48.7 |
| Unemployment (%) | 5.1 | 12.3 |
| Re-registered motor vehicle per dwelling | 1.8 | 1.9 |
| Variables | Australia | |
|---|---|---|
| Total Population (%) | Indigenous (%) | |
| BMI index | ||
| Underweight/normal weight | 75.1 | 62.1 |
| Overweight/obese | 24.9 | 37.9 |
| Usual daily intake of fruits | ||
| 1 serving or less | 27.2 | 35.8 |
| 2 servings or more | 70.4 | 61.2 |
| Does not eat fruit | 2.5 | 2.7 |
| Usual daily intake of vegetables | ||
| 1 serving or less | 40.9 | 46.6 |
| 2 servings or more | 57.3 | 48.3 |
| Does not eat vegetables | 1.9 | 4.9 |
| Adequate daily fruit consumption | 73.0 | 65.0 |
| Adequate daily vegetable consumption | 6.3 | 6.1 |
| Adequate daily fruit and vegetable consumption | 6.0 | 5.8 |
| Usually consumes sugar-sweetened or diet drinks | 44.8 | 64.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, K.Y.; Allan, J.; Dalton, H.; Sleigh, A.; Seubsman, S.-a.; Ross, A.G. Reviewing Publicly Available Reports on Child Health Disparities in Indigenous and Remote Communities of Australia. Int. J. Environ. Res. Public Health 2023, 20, 5959. https://doi.org/10.3390/ijerph20115959
Ahmed KY, Allan J, Dalton H, Sleigh A, Seubsman S-a, Ross AG. Reviewing Publicly Available Reports on Child Health Disparities in Indigenous and Remote Communities of Australia. International Journal of Environmental Research and Public Health. 2023; 20(11):5959. https://doi.org/10.3390/ijerph20115959
Chicago/Turabian StyleAhmed, Kedir Y., Julaine Allan, Hazel Dalton, Adrian Sleigh, Sam-ang Seubsman, and Allen G. Ross. 2023. "Reviewing Publicly Available Reports on Child Health Disparities in Indigenous and Remote Communities of Australia" International Journal of Environmental Research and Public Health 20, no. 11: 5959. https://doi.org/10.3390/ijerph20115959
APA StyleAhmed, K. Y., Allan, J., Dalton, H., Sleigh, A., Seubsman, S. -a., & Ross, A. G. (2023). Reviewing Publicly Available Reports on Child Health Disparities in Indigenous and Remote Communities of Australia. International Journal of Environmental Research and Public Health, 20(11), 5959. https://doi.org/10.3390/ijerph20115959