

Social Correlates of HIV-Risky Behaviours among African Canadian Adolescents Living in British Columbia, Canada: A Secondary Data Analysis



Abstract
:Highlights
- African Canadian adolescents generally have low rates of HIV-risky behaviours;
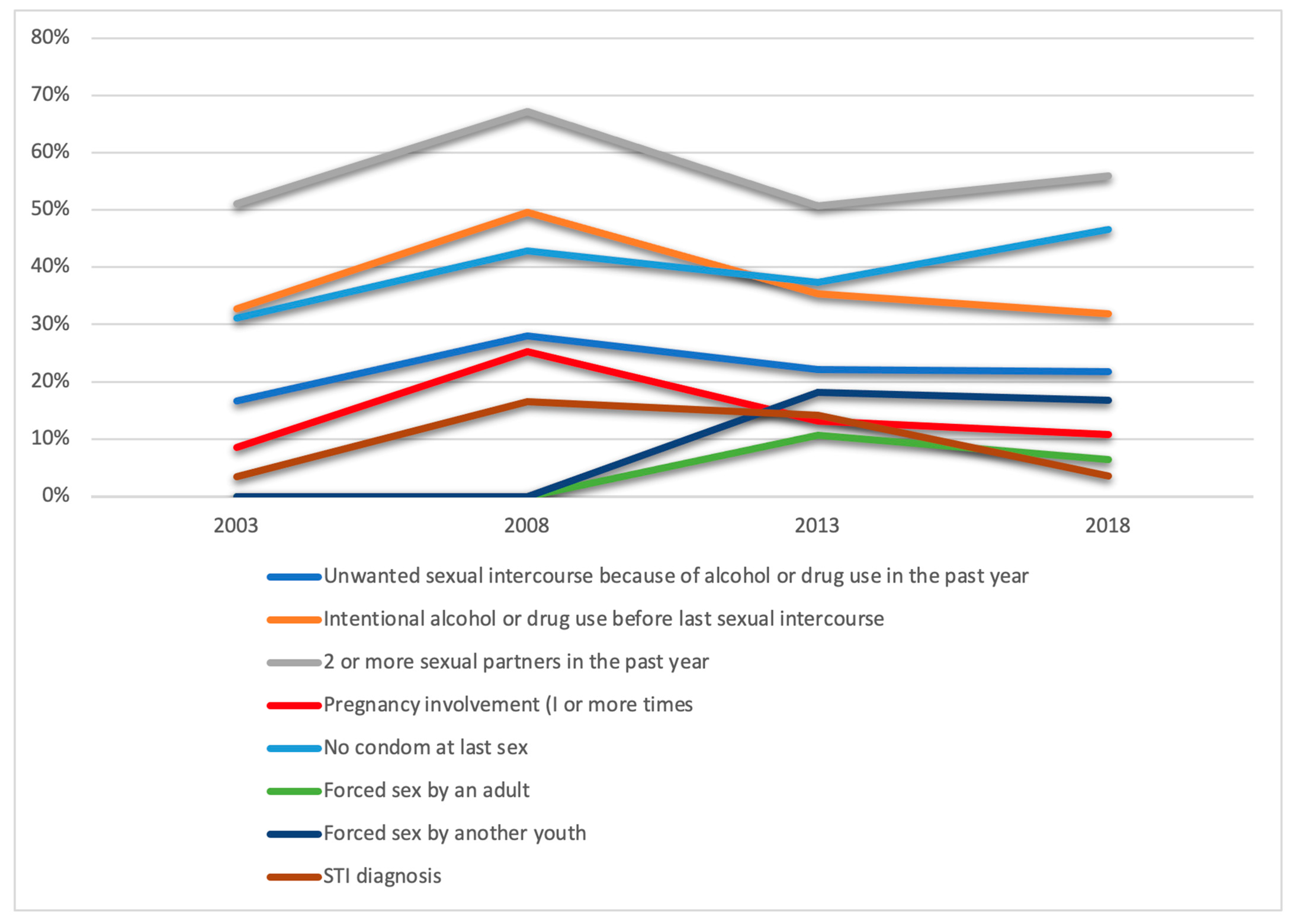
- Rates increased from 2003 to 2018; particularly rates of condomless sex and sex due to the influence of drugs or alcohol;
- Of the sexually active in 2018, ≈50% had 2 or more partners and condomless sex at last intercourse;
- Unsafe neighbourhood, perceived racism and sexism were significant predictors of HIV-risky behavior.
- Engagement in sexual risky behaviours may expose African, Caribbean and Black adolescents to HIV-risk.
- Addressing the impacts of social determinants of health and socioecologic factors such as the absence of familial support, the negative influence of peer pressure (physical and sexual abuse, and exposure to substances) can help mitigate engagement in HIV-risky behaviors among African, Caribbean and Black adolescents.
- The provision of safe, stable housing as well as feeling safe in schools can help mitigate engagement in HIV-risky behaviors among African, Caribbean and Black adolescents.
- Racism, sexism and various forms of intersecting stigma must be sufficiently addressed to curb rates of engagement in HIV-risky behaviours among African, Caribbean and Black adolescents.
Abstract
1. Introduction
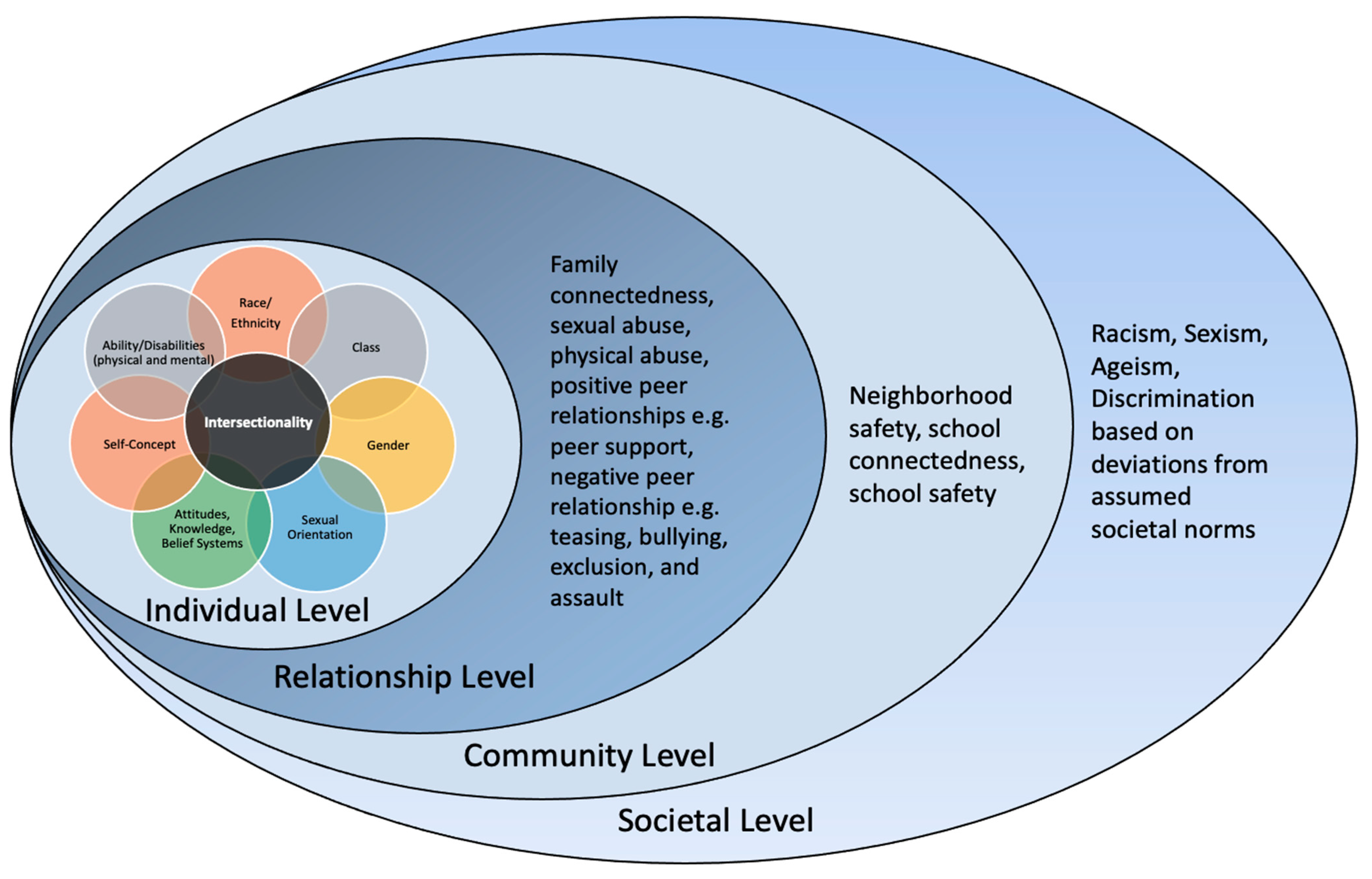
2. Theoretical Framework
3. Methods
3.1. Survey Design
3.2. Sample
3.3. Inclusion and Exclusion Criteria
3.4. Measures
3.5. Data Analyses
4. Results
4.1. Characteristics of African Canadian Adolescents from 2003 to 2018
4.2. Differences in HIV-Risky Behavior among African Canadian Adolescents across Survey Years from 2003 to 2018
4.3. Incidence of HIV-Risky Behavior among African Canadian Adolescents in 2018
4.4. Social Correlates of HIV-Risky Behaviours among African Canadian Adolescents in 2018
5. Discussion
6. Strengths and Limitations
7. Patient and Public Opinion
8. Healthcare Implications
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth Risk Behavior Surveillance—United States, 2017. MMWR. Surveill. Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Forsyth, K.; Poon, C.; Peled, M.; Saewyc, E.; McCreary Centre Society. Balance and Connection in BC: The Health and Well-Being of Our Youth; McCreary Centre Society: Vancouver, BC, Canada, 2019. [Google Scholar]
- Bartlett, R.; Buck, R.; Shattel, M.M. Risk and protection for HIV/AIDS in African-American, Hispanic, and White adolescents. J. Natl. Black Nurses Assoc. 2008, 19, 19–25. [Google Scholar] [PubMed]
- Kangmennaang, J.; Mkandawire, P.; Luginaah, I. Determinants of risky sexual behaviours among adolescents in Central African Republic, Eswatini and Ghana: Evidence from multi-indicator cluster surveys. Afr. J. AIDS Res. 2019, 18, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada [PHAC]. HIV in Canada—Surveillance Report 2019; PHAC: Ottawa, ON, Canada, 2021. [Google Scholar]
- Fleming, N.; O′driscoll, T.; Becker, G.; Spitzer, R.F.; Allen, L.; Millar, D.; Brain, P.; Dalziel, N.; Dubuc, E.; Hakim, J.; et al. Adolescent Pregnancy Guidelines. J. Obstet. Gynaecol. Can. 2015, 37, 740–756. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. Social Determinants of Health; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 22 July 2022).
- Everett, B.G.; Myers, K.; Sanders, J.N.; Turok, D.K. Male Abortion Beneficiaries: Exploring the Long-Term Educational and Economic Associations of Abortion Among Men Who Report Teen Pregnancy. J. Adolesc. Health 2019, 65, 520–526. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Boston, MA, USA, 1979. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Archibald, C. Knowledge and attitudes toward HIV/AIDS and risky sexual behaviours among Caribbean African American female adolescents. J. Assoc. Nurses AIDS Care 2007, 18, 64–72. [Google Scholar] [CrossRef]
- Saewyc, E.M.; Taylor, D.; Homma, Y.; Ogilvie, G. Trends in sexual health and risk behaviours among adolescent students in British Columbia. Can. J. Hum. Sex. 2008, 17, 1–13. [Google Scholar]
- Saewyc, E.; Clark, T.; Barney, L.; Brunanski, D.; Homma, Y. Enacted stigma and HIV-risky behavior. HIV-risky behaviours among sexual minority Indigenous youth in Canada, New Zealand, and the United States. Pimatisiwin 2014, 11, 411–420. [Google Scholar] [CrossRef]
- Umaña-Taylor, A.J.; Quintana, S.M.; Lee, R.M.; William, E.C., Jr.; Rivas-Drake, D.; Schwartz, S.J.; Syed, M.; Yip, T.; Seaton, E. Ethnic and Racial Identity During Adolescence and Into Young Adulthood: An Integrated Conceptualization. Child Dev. 2014, 85, 21–39. [Google Scholar] [CrossRef]
- Quinn, K.; Walsh, J.; Dickson-Gomez, J. Multiple Marginality and the Variation in Delinquency and Substance use Among Adolescent Gang Members. Subst. Use Misuse 2019, 54, 612–627. [Google Scholar] [CrossRef] [PubMed]
- Dallas, R.H.; Loew, M.M.; Wilkins, M.L.; Sun, Y.; Tang, L.; Porter, J.S.; Gaur, A.H. Body Image and Risk Behaviors in Youth with HIV. AIDS Patient Care STDs 2017, 31, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Deardorff, J.; Tschann, J.M.; Flores, E.; Ozer, E.J. Sexual values and risky sexual behaviours among Latino youths. Perspect. Sex. Reprod. Health 2010, 42, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.M.; Cintron, A.; Kocher, S. Factors Related to Risky Sexual Behaviours and Effective STI/HIV and Pregnancy Intervention Programs for African American Adolescents. Public Health Nurs. 2014, 31, 414–427. [Google Scholar] [CrossRef] [PubMed]
- Patrick, M.E.; Maggs, J.L. Profiles of motivations for alcohol use and sexual behavior among first-year university students. J. Adolesc. 2010, 33, 755–765. [Google Scholar] [CrossRef]
- Littleton, H.L.; Grills-Taquechel, A.E.; Buck, K.S.; Rosman, L.; Dodd, J.C. Health Risk Behavior and Sexual Assault Among Ethnically Diverse Women. Psychol. Women Q. 2013, 37, 7–21. [Google Scholar] [CrossRef]
- Goodrum, N.M.; Armistead, L.P.; Tully, E.C.; Cook, S.L.; Skinner, D. Parenting and youth sexual risk in context: The role of community factors. J. Adolesc. 2017, 57, 1–12. [Google Scholar] [CrossRef]
- Assari, S.; Moazen-Zadeh, E.; Caldwell, C.H.; Zimmerman, M.A. Racial discrimination during 475 adolescence predicts mental health deterioration in adulthood: Gender differences among Blacks. Front. Public Health 2017, 5, 104. [Google Scholar] [CrossRef]
- Pachter, L.M.; Caldwell, C.H.; Jackson, J.S.; Bernstein, B.A. Discrimination and Mental Health in a Representative Sample of African-American and Afro-Caribbean Youth. J. Racial Ethn. Health Disparities 2018, 5, 831–837. [Google Scholar] [CrossRef]
- Brown, C.S.; Bigler, R.S.; Chu, H. An experimental study of the correlates and consequences of perceiving oneself to be the target of gender discrimination. J. Exp. Child Psychol. 2010, 107, 100–117. [Google Scholar] [CrossRef]
- Cogburn, C.D.; Chavous, T.M.; Griffin, T.M. School-Based Racial and Gender Discrimination among African American Adolescents: Exploring Gender Variation in Frequency and Implications for Adjustment. Race Soc. Probl. 2011, 3, 25–37. [Google Scholar] [CrossRef] [PubMed]
- English, D.; Lambert, S.F.; Ialongo, N.S. Longitudinal associations between experienced racial discrimination and depressive symptoms in African American adolescents. Dev. Psychol. 2014, 50, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Okoye, H.U.; Saewyc, E. Fifteen-year trends in self-reported racism and link with health and well-being of African Canadian adolescents: A secondary data analysis. Int. J. Equity Health 2021, 20, 1–13. [Google Scholar] [CrossRef]
- Devries, K.M.; Free, C.J.; Morison, L.; Saewyc, E. Factors associated with sexual behavior of Aboriginal youth: Implications for health promotion. Am. J. Public Health 2009, 99, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Fairbairn, N.; Wood, E.; Dong, H.; Kerr, T.; DeBeck, K. Unsafe sexual behaviour associated with hazardous alcohol use among street-involved youth. AIDS Care 2017, 29, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Saewyc, E.M.; Wong, S.T.; Zumbo, B.D. Sexual health and risk behaviour among East Asian adolescents in British Columbia. Can. J. Hum. Sex. 2013, 22, 13–24. [Google Scholar] [CrossRef]
- Crenshaw, K. Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanf. Law Rev. 1991, 43, 1241. [Google Scholar] [CrossRef]
- Shaffer, C.S.; Adjei, J.; Viljoen, J.L.; Douglas, K.S.; Saewyc, E.M. Ten-Year Trends in Physical Dating Violence Victimization Among Adolescent Boys and Girls in British Columbia, Canada. J. Interpers. Violence 2021, 36, 3947–3964. [Google Scholar] [CrossRef]
- Sandy, P.T.; Vhembo, T.; Molotsi, T.K. Sexual behaviour among adolescents living with the human immunodeficiency virus in Zimbabwe: Educational implications. Afr. J. AIDS Res. 2019, 18, 130–137. [Google Scholar] [CrossRef]
- Saewyc, E.M.; Homma, Y.; Skay, C.L.; Bearinger, L.H.; Resnick, M.D.; Reis, E. Protective factors in the lives of bisexual adolescents in North America. Am. J. Public Health 2009, 99, 110–117. [Google Scholar] [CrossRef]
- McNeely, C.A.; Nonnemaker, J.M.; Blum, R.W. Promoting school connectedness: Evidence from the National Longitudinal Study of Adolescent Health. J. Sch. Health 2002, 72, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada [PHAC]. HIV/AIDS Epi Updates, October 2014—National HIV Prevalence and Incidence Estimates for 2011; PHAC: Ottawa, ON, Canada, 2014. [Google Scholar]
- Abousselam, N.; Naudé, L.; Lens, W.; Esterhuyse, K. The relationship between future time perspective, self-efficacy, and risky sexual behavior in the Black youth of central South Africa. J. Ment. Health 2016, 25, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Ssewanyana, D.; Newton, C.R.; van Baar, A.; Hassan, A.S.; Stein, A.; Taylor, H.G.; Van De Vijver, F.; Scerif, G.; Abubakar, A. Beyond Their HIV Status: The Occurrence of Multiple Health Risk Behavior Among Adolescents from a Rural Setting of Sub-Saharan Africa. Int. J. Behav. Med. 2020, 27, 426–443. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.-H.; Yuan, S.; Zhang, R.; Yu, J.-F.; Nzala, S.H.; Wang, P.-G.; He, Q.-Q. Risky Sexual Behaviours and Associated Factors Among College Students in Lusaka, Zambia. Arch. Sex. Behav. 2019, 48, 2117–2123. [Google Scholar] [CrossRef]
- Omorodion, F.; Gbadebo, K.; Ishak, P. HIV vulnerability and sexual risk among African youth in Windsor, Canada. Cult. Health Sex. 2007, 9, 429–437. [Google Scholar] [CrossRef]
- Lang, D.L.; Sales, J.M.; Salazar, L.F.; Hardin, J.W.; Diclemente, R.J.; Wingood, G.M.; Rose, E. Rape victimization and high risk sexual behaviours: Longitudinal study of African-American adolescent females. West. J. Emerg. Med. 2011, 12, 333–342. [Google Scholar]
- Elkington, K.S.; Bauermeister, J.; Brackis-Cott, E.; Dolezal, C.; Mellins, C.A. Substance use and sexual risk behaviours in perinatally human immunodeficiency virus-exposed youth: Roles of caregivers, peers, and HIV status. J. Adolesc. Health 2009, 45, 133–141. [Google Scholar] [CrossRef]
- Langille, D.; Asbridge, M.; Kisely, S.; Wilson, K. Risk of depression and multiple sexual risk-taking behaviours in adolescents in Nova Scotia, Canada. Sex. Health 2012, 9, 254–260. [Google Scholar] [CrossRef]
- Katz, J.; Tirone, V. Going along with it: Sexually coercive partner behavior predicts dating women’s compliance with unwanted sex. Violence Against Women 2010, 16, 730–742. [Google Scholar] [CrossRef]
- Stern, E.; Buikema, R.; Cooper, D. South African women’s conceptualisations of and responses to sexual coercion in relation to hegemonic masculinities. Glob. Public Health 2016, 11, 135–152. [Google Scholar] [CrossRef]
- Stern, E.; Rau, A.; Cooper, D. Sexual and reproductive health perceptions and practices as revealed in the sexual history narratives of South African men living in a time of HIV/AIDS. SAHARA-J J. Soc. Asp. HIV/AIDS 2014, 11, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, T.T.; Voûte, C.; Rose, M.A.; Cleveland, J.; Dean, H.D.; Fenton, K. Social determinants of HIV/AIDS and sexually transmitted diseases among Black women: Implications for health equity. J. Women’s Health 2012, 21, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.K.; Montgomery, A.J. Parent Communication and Sexual Risk Among African Americans. West. J. Nurs. Res. 2007, 29, 691–707. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | 2003 (n ^ = 1072) | 2008 (n ^ = 1677) | 2013 (n ^ = 1331) | 2018 (n ^ = 1111) |
|---|---|---|---|---|
| Mean age | 16.20 | 15.88 | 16.15 | 16.24 |
| Gender | ||||
| Male | 59.9% | 65.3% | 56.0% | 64.7% |
| Born in Canada | ||||
| Yes | 81.4% | 71.1% | 68.7% | 65.4% |
| Spoke a language other than English at Home | ||||
| Never | 61.% | 51.0% | 58.6% | 44.3% |
| Sometimes | 30.0% | 28.5% | 23.6% | 37.9% |
| Most of the time | 8.9% | 20.5% | 17.9% | 17.2% |
| Going to bed hungry | ||||
| Never | a | a | 70.9% | 85.8% |
| Sometimes | a | a | 13.8% | 12.2% |
| Often/always | a | a | 15.3 | 2.0% |
| Sexual orientation | ||||
| Heterosexual, no attraction, unsure, or questioning | 89.9% | 70.3% | 81.6% | 86.2% |
| Mostly Straight | 7.0% | 13.5% | 7.8% | 3.9% |
| Bi, pan sexual, gay, or lesbian | 3.2% | 16.2% | 10.6% | 9.9% |
| Variable | 2003 (n ^ = 1072) | 2008 (n ^ = 1677) | 2013 (n ^ = 1331) | 2018 (n ^ = 1111) | ||||
|---|---|---|---|---|---|---|---|---|
| % | CI | % | CI | % | CI | % | CI | |
| Unwanted sexual intercourse because of alcohol or drug use in the past year | 16.6% | (13.7–20.1) | 28.0% | (21.6–35.5) | 22.1% | (15.3–30.8) | 23.3% | (17.7–29.9) |
| Intentional alcohol or drug use before last sexual intercourse *** | 32.7% | (25.9–40.3) | 49.6% | (42.2–56.9) | 35.3% | (27.5–43.9) | 29.3% | (22.8–36.8) |
| 2 or more sexual partners in the past year ** | 51.1% | (45.1–57.0) | 67.2% | (59.6–74.0) | 50.7% | (42.8–58.7) | 54.2% | (46.1–62.0) |
| Pregnancy involvement (I or more times *** | 8.5% | (6.1–11.6) | 25.3% | (18.1–34.2) | 13.2% | (8.6–19.9) | 9.3% | (5.7–14.7) |
| No condom at last sex | 31.1% | (20.8–43.7) | 42.8% | (36.6–49.2) | 37.3% | (29.6–45.7) | 48.4% | (41.2–55.6) |
| Forced sex by an adult | a | a | 10.7% | (6.5–16.9) | 5.8% | (2.9–11.0) | ||
| Forced sex by another youth | a | a | 18.1% | (12.5–25.5) | 17.9% | (12.9–24.3) | ||
| STI diagnosis *** | 3.4% | (2.1–5.3) | 16.5% | (11.8–22.5) | 14.2% | (8.8–22) | 3.4% | (1.8–6.5) |
| HIV-Risky Behaviours | Males (n) | Females (n) | Total % of Population Engaging in HIV Risky Behaviours |
|---|---|---|---|
| Unwanted sexual intercourse because of alcohol or drug use in the past | 133 | 116 | 23.3 |
| Intentional alcohol or drug use at last sexual intercourse | 192 | 128 | 29.3 |
| 2 or more sexual partners | 391 | 189 | 54.2 |
| Pregnancy involvement 1 or more times | 71 | 26 | 9.3 |
| No condom at last sex | 290 | 231 | 48.4 |
| Forced sex by an adult | 38 | 24 | 5.8 |
| Forced sex by another youth | 57 | 135 | 17.9 |
| STI diagnosis | 29 | 8 | 3.4 |
| Moderate to High-Risk HIV Behaviour | ||||
|---|---|---|---|---|
| Unadjusted OR | Age-Adjusted OR | |||
| Individual level | ||||
| Self-report of mental health | 0.32 | (0.13, 0.79) * | 1.81 | (0.89, 3.66) |
| Suicidal ideation in the past year | 2.90 | (1.35, 6.23) ** | 1.43 | (0.37, 5.54) |
| Passed out because of using drugs or alcohol in the past year | 5.79 | (2.29, 14.67) *** | 4.65 | (1.50, 14.4) ** |
| Illicit drug use (e.g cocaine, heroin, ecstasy, mushrooms, etc.) lifetime | 4.93 | (0.61, 2.11) | 4.22 | (1.95, 9.16) |
| 2 or more times | 4.93 | (2.11, 11.52) ** | 8.89 | (2.22, 35.45) ** |
| 1 or 2 times | 0.46 | (0.09, 2.41) | 0.43 | (0.06, 2.84) |
| 0 times | Ref | - | Ref | - |
| Relationship level | ||||
| Negative peer experience (being teased, excluded, and/or assaulted) | 2.69 | (1.05, 6.85) * | 1.30 | (0.43, 3.96) |
| Physical abuse | 2.48 | (1.11, 5.56) * | 0.32 | (0.025, 4.16) |
| Sexual abuse | 5.90 | (2.56, 13.63) *** | 7.77 | (0.84, 71.65) # |
| Could not say “no” to sex | 4.3 | (1.47, 12.68) ** | 14.06 | (1.98, 99.99) ** |
| Community level | ||||
| Neighbourhood safety | 0.56 | (0.39, 0.81) ** | 0.46 | (0.28, 0.76) ** |
| Family connectedness | 0.73 | (0.47, 1.12) | 0.96 | (0.52, 1.78) |
| School Safety | 0.48 | (0.32, 0.71) *** | 1.79 | (0.87, 3.70) |
| School connectedness | 0.49 | (0.271–0.87)* | 0.64 | (0.34, 1.22) |
| Societal Level | ||||
| Racial discrimination | 3.13 | (1.2, 8.16) * | 3.95 | (1.33, 11.73) * |
| Gender discrimination | 3.42 | (1.26, 9.28) * | 6.39 | (1.33, 30.75) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojukwu, E.N.; Okoye, H.U.; Saewyc, E. Social Correlates of HIV-Risky Behaviours among African Canadian Adolescents Living in British Columbia, Canada: A Secondary Data Analysis. Int. J. Environ. Res. Public Health 2023, 20, 6031. https://doi.org/10.3390/ijerph20116031
Ojukwu EN, Okoye HU, Saewyc E. Social Correlates of HIV-Risky Behaviours among African Canadian Adolescents Living in British Columbia, Canada: A Secondary Data Analysis. International Journal of Environmental Research and Public Health. 2023; 20(11):6031. https://doi.org/10.3390/ijerph20116031
Chicago/Turabian StyleOjukwu, Emmanuela Nneamaka, Helen Uche Okoye, and Elizabeth Saewyc. 2023. "Social Correlates of HIV-Risky Behaviours among African Canadian Adolescents Living in British Columbia, Canada: A Secondary Data Analysis" International Journal of Environmental Research and Public Health 20, no. 11: 6031. https://doi.org/10.3390/ijerph20116031
APA StyleOjukwu, E. N., Okoye, H. U., & Saewyc, E. (2023). Social Correlates of HIV-Risky Behaviours among African Canadian Adolescents Living in British Columbia, Canada: A Secondary Data Analysis. International Journal of Environmental Research and Public Health, 20(11), 6031. https://doi.org/10.3390/ijerph20116031