

Social Return on Investment of Social Prescribing via a Diabetes Technician for Preventing Type 2 Diabetes Progression


Abstract
:1. Introduction
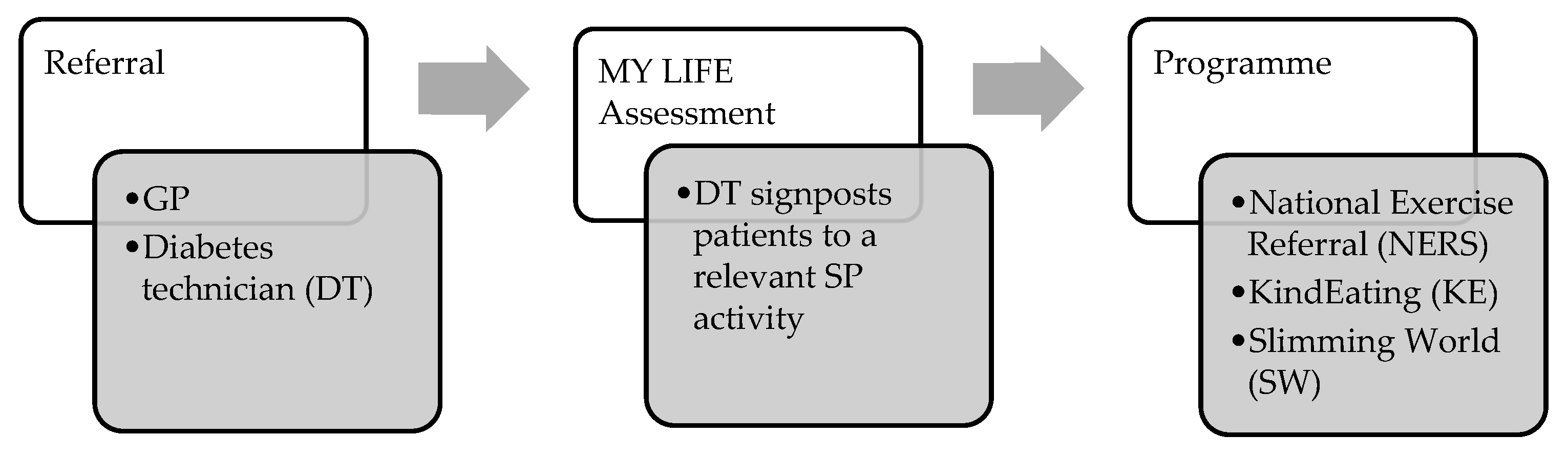
- NERS consists of two supervised physical activity sessions per week, lasting approximately 1-h. NERS is delivered by an exercise professional who provides support throughout a 16-week period. The activities involved are primarily exercise and fitness classes.
- KE is a 12-week programme delivered by a registered dietician which includes weekly or fortnightly weigh-ins to measure progress. The dietician provides advice on healthy weight loss, eating habits, goal setting, physical activity, meal planning, dining out, and food labels.
- SW is a 12-week programme delivered by a SW group consultant with a focus on weight management advice and guidance, telephone support, buddy systems, and online support.
2. Materials and Methods
3. Results
3.1. Identifying Stakeholders
3.2. Theory of Change
3.3. Calculating Inputs
3.4. Evidencing and Valuing Outcomes
3.4.1. Good Overall Health
3.4.2. Wellbeing Valuation Using the Social Value Calculator
3.4.3. Deadweight, Attribution and Displacement
3.4.4. Wellbeing Valuation Using Mental Health Social Value Calculator
3.4.5. Health Service Resource Use
3.5. Calculating the SROI Ratios
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Furmli, S.; Elmasry, R.; Ramos, M.; Fung, J. Therapeutic use of intermittent fasting for people with type 2 diabetes as an alternative to insulin. Br. Med. J. Case Rep. 2018, 2018, bcr-2017-221854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Look AHEAD Research Group. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mata-Cases, M.; Franch-Nadal, J.; Real, J.; Cedenilla, M.; Mauricio, D. Prevalence and coprevalence of chronic comorbid conditions in patients with type 2 diabetes in Catalonia: A population-based cross-sectional study. BMJ Open 2019, 9, e031281. [Google Scholar] [CrossRef]
- Kaur, G.; Lakshmi PV, M.; Rastogi, A.; Bhansali, A.; Jain, S.; Teerawattananon, Y.; Prinja, S. Diagnostic accuracy of tests for type 2 diabetes and prediabetes: A systematic review and meta-analysis. PLoS ONE 2020, 15, 3. [Google Scholar] [CrossRef]
- NHS England. NHS England Impact Analysis of Implementing NHS Diabetes Prevention Programme, 2016 to 2021. NHS England. 2016. Available online: https://www.england.nhs.uk/ltphimenu/diabetes-prevention/nhs-diabetes-prevention-programme-nhs-dpp/ (accessed on 22 April 2022).
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c test in diagnosis and prognosis of diabetic patients. Biomark. Insights 2016, 11, 5–104. [Google Scholar] [CrossRef]
- World Health Organisation. Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus. 2013. Available online: https://www.who.int/diabetes/publications/report-hba1c_2011.pdf (accessed on 25 April 2022).
- Marais, C.; Hall, D.R.; van Wyk, L.; Conradie, M. Randomized cross-over trial comparing the diagnosis of gestational diabetes by oral glucose tolerance test and a designed breakfast glucose profile. Int. J. Gynecol. Obstet. 2018, 141, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hex, N.; Bartlett, C.; Wright, D.; Taylor, M.; Varley, D. Estimating the current and future costs of Type1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet. Med. 2012, 29, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Keng, M.J.; Leal, J.; Bowman, L.; Armitage, J.; Mihaylova, B. Hospital costs associated with adverse events in people with diabetes in the UK. Diabetes Obes. Metab. 2022, 24, 2108–2117. [Google Scholar] [CrossRef]
- Keng, M.J.; Tsiachristas, A.; Leal, J.; Gray, A.; Mihaylova, B. Impact of achieving primary care targets in type 2 diabetes on health outcomes and healthcare costs. Diabetes Obes. Metab. 2019, 21, 2405–2412. [Google Scholar] [CrossRef]
- Welsh Government. Diabetes Delivery Plan for Wales 2016–2020: The Best Standard of Care for Everyone with Diabetes. 2016. Available online: https://gov.wales/sites/default/files/publications/2018-12/diabetes-delivery-plan-2016-to-2020.pdf (accessed on 26 April 2022).
- Diabetes UK. Diabetes Statistics. 2020. Available online: https://www.diabetes.org.uk/professionals/position-statements-reports/statistics (accessed on 23 April 2022).
- Gregory, N.; Kirkland, D.; Washbrook-Davies, C.; Jesurasa, A. The All Wales Diabetes Prevention Programme Intervention Protocol. 2022. Available online: https://phw.nhs.wales/services-and-teams/primary-care-division/all-wales-diabetes-prevention-programme/all-wales-diabetes-prevention-programme-intervention-protocol1/ (accessed on 22 April 2022).
- Gheera, M.; Eaton, M. Social Prescribing. UK Parliament. 2020. Available online: https://commonslibrary.parliament.uk/research-briefings/cbp-8997/ (accessed on 17 April 2022).
- Stickley, T.; Hui, A. Social prescribing through arts on prescription in a UK city: Referrers’ perspectives (part 2). Public Health 2012, 126, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Kilgarriff-Foster, A.; O’Cathain, A. Exploring the components and impact of social prescribing. J. Public Ment. Health 2015, 14, 9–10. [Google Scholar] [CrossRef]
- Hartfiel, N.; Gittins, H.; Tudor Edwards, R. Social Return on Investment of the Actif Woods Wales Programme. 2020. Available online: https://www.smallwoods.org.uk/assets/Uploads/Coedlleol-/Research/Reports-and-infographics/SROI-Report-5-May-2021.pdf (accessed on 15 April 2022).
- Roland, M.; Everington, S.; Marshall, M. Social prescribing-transforming the relationship between physicians and their patients. N. Engl. J. Med. 2020, 383, 97–99. [Google Scholar] [CrossRef]
- Polley, M.J.; Pilkington, K. A Review of the Evidence Assessing Impact of Social Prescribing on Healthcare Demand and Cost Implications. Technical Report. University of Westminster. 2017. Available online: https://westminsterresearch.westminster.ac.uk/download/e18716e6c96cc93153baa8e757f8feb602fe99539fa281433535f89af85fb550/297582/review-of-evidence-assessing-impact-of-social-prescribing.pdf (accessed on 26 April 2022).
- Deakin, T.A.; Cade, J.E.; Williams, R.; Greenwood, D.C. Structured patient education: The Diabetes X-PERT Programme makes a difference. Diabet. Med. 2006, 23, 944–954. [Google Scholar] [CrossRef] [Green Version]
- Cabinet Office. A Guide to Social Return on Investment. London. 2012. Available online: https://socialvalueuk.org/wp-content/uploads/2016/03/The%20Guide%20to%20Social%20Return%20on%20Investment%202015.pdf (accessed on 17 April 2022).
- HM Treasury. The Green Book: Central Government Guidance on Appraisal and Evaluation; HM Treasury: London, UK, 2022.
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh mental well-being scale (WEMWBS): A Rasch analysis using data from the Scottish health education population survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trotter, L.; Vine, J.; Leach, M.; Fujiwara, D. Measuring the Social Impact of Community Investment: A Guide to Using the Wellbeing Valuation Approach; HACT: London, UK, 2014. [Google Scholar]
- van der Zee-Neuen, A.; Strobl, V.; Dobias, H.; Fuchs, H.; Untner, J.; Foisner, W.; Knapp, M.; Edtinger, S.; Offenbacher, M.; Ritter, M.; et al. Sustained improvements in EQ-5D utility scores and self-rated health status in patients with ankylosing spondylitis after spa treatment including low-dose radon—An analysis of prospective radon indication registry data. BMC Musculoskelet Disord 2022, 23, 743. [Google Scholar] [CrossRef] [PubMed]
- Trotter, L.; Rallings-Adams, M.K. Valuing Improvements in Mental Health: Applying the Wellbeing Valuation Method to WEMWBS; HACT: London, UK, 2017. [Google Scholar]
- Dancer, S. Additionality Guide, 4th ed.; Home and Communities Agency: London, UK, 2014.
- National Cost Collection: 2020–21—NHS Trust and NHS Foundation Trusts. 2022. Available online: https://www.england.nhs.uk/publication/2020-21-national-cost-collection-data-publication/ (accessed on 19 April 2022).
- Piper, C.; Marossy, A.; Griffiths, Z.; Adegboye, A. Evaluation of a type 2 diabetes prevention program using a commercial weight management provider for non-diabetic hyperglycemic patients referred by primary care in the UK. BMJ Open Diabetes Res. Care 2017, 5, e000418. [Google Scholar] [CrossRef] [Green Version]
- Carroll, S.; Borkoles, E.; Polman, R. Short-term effects of a non-dieting lifestyle intervention program on weight management, fitness, metabolic risk, and psychological well-being in obese premenopausal females with the metabolic syndrome. Appl. Physiol. Nutr. Metab. 2007, 32, 125–142. [Google Scholar] [CrossRef] [PubMed]
- Akobeng, A.K. Understanding randomised controlled trials. Arch. Dis. Child. 2005, 90, 840–844. [Google Scholar] [CrossRef] [Green Version]
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Uptake and Retention in Group-Based Weight-Management Services: Literature Review and Behavioural Analysis. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/725927/Uptake_and_retention_in_group_based_weight_management_services.pdf (accessed on 23 April 2022).
- Long, E.; Patterson, S.; Maxwell, K.; Blake, C.; Pérez, R.B.; Lewis, R.; McCann, M.; Riddell, J.; Skivington, K.; Wilson-Lowe, R.; et al. COVID-19 pandemic and its impact on social relationships and health. J. Epidemiol. Community Health 2022, 76, 128–132. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline and Follow-Up | |
|---|---|
| Baseline |
|
| Weeks 2–6 |
|
| Week 8 |
|
| Cost Category | Annual Costs per Participant (n = 54) |
|---|---|
| DT equipment costs | Mobile phone = GBP 60 (GBP 5 per month)
|
| DT salary costs |
|
| Total DT costs | GBP 304.61 |
| SP delivery costs | GBP 258 (NERS) × 2 participants= GBP 516 GBP 75 (SW) × 2 participants = GBP 150 GBP 135.70 (KE) × 8 participants = GBP 1085.60 Total SP delivery costs = GBP 1751.60 |
| Total SP delivery costs | GBP 145.96 |
| Total Costs | GBP 450.57 |
| Category | DTO (n = 12) | DT + SP (n = 12) |
|---|---|---|
| Age | 50% aged 50 and over | 29% aged 50 and over |
| Gender percentage | 50% Female | 80% Female |
| Ethnic origin | 100% White British | 100% White British |
| Average SWEMWBS score at baseline | 24.4 | 25.6 |
| Average SWEMWBS score at 8 weeks | 26 | 28.2 |
| Average EQ5D-5L at baseline | 0.801 | 0.823 |
| Average EQ5D-5L at 8 weeks | 0.803 | 0.845 |
| Outcomes (n = 24) | Indicators | Net Quantity | Financial Value | Total Social Value | Social Value per Participant |
|---|---|---|---|---|---|
| DT + SP Good Overall Health | EQ5D-5L | 3/12 | GBP 20,141 per year for good overall health | GBP 60,423 | GBP 5035 (n = 12) |
| DTO Good Overall Health | EQ5D-5L | 2/12 | GBP 20,141 per year for good overall health | GBP 40,282 | GBP 3357 (n = 12) |
| Outcomes | Total Social Value per Participant | Deadweight | Attribution | Displacement | Total Social Value per Participant |
|---|---|---|---|---|---|
| DT + SP | GBP 5035 | 43% (×0.57) | 28% (×0.72) | 0% | GBP 2066 |
| DTO: | GBP 3357 | 43% (×0.57) | 28% (×0.72) | 0% | GBP 1378 |
| Programme | ID | Age 1 | Baseline | Week 8 | GBP Value Baseline | GBP Value Week 8 | Value Change | Value—27% Deadweight |
|---|---|---|---|---|---|---|---|---|
| NERS | 1005 | 25–49 | 30 | 30 | GBP 25,470 | GBP 25,470 | GBP 0 | GBP 0 |
| NERS | 109 | 25–49 | 26 | 28 | GBP 24,144 | GBP 25,145 | GBP 1001 | GBP 731 |
| KE | 1014 | 50+ | 25 | 26 | GBP 23,295 | GBP 23,295 | GBP 0 | GBP 0.00 |
| KE | 817 | 50+ | 29 | 28 | GBP 24,480 | GBP 23,563 | −GBP 917 | −GBP 669 |
| KE | 909 | 25–49 | 18 | 21 | GBP 10,523 | GBP 20,831 | GBP 10,308 | GBP 7525 |
| KE | 107 | 25–49 | 16 | 19 | GBP 8587 | GBP 16,701 | GBP 8114 | GBP 5923 |
| KE | 2001 | 50+ | 28 | 27 | GBP 23,563 | GBP 23,563 | GBP 0 | GBP 0 |
| KE | 2011 | 50+ | 24 | 26 | GBP 21,434 | GBP 23,295 | GBP 1861 | GBP 1359 |
| KE | 715 | 25–49 | 26 | 28 | GBP 24,144 | GBP 25,145 | GBP 1001 | GBP 731 |
| KE | 8 | 25–49 | 18 | 24 | GBP 10,523 | GBP 23,383 | GBP 12,860 | GBP 9388 |
| SW | 903 | 25–49 | 31 | 33 | GBP 25,811 | GBP 25,811 | GBP 0 | GBP 0 |
| SW | 813 | 50+ | 22 | 22 | GBP 19,947 | GBP 19,947 | GBP 0 | GBP 0 |
| DTO | 401 | 50+ | 24 | 26 | GBP 21,434 | GBP 23,295 | GBP 1861 | GBP 1359 |
| DTO | 802 | 25–49 | 25 | 27 | GBP 24,144 | GBP 25,145 | GBP 1001 | GBP 731 |
| DTO | 803 | 25–49 | 21 | 25 | GBP 20,831 | GBP 24,144 | GBP 3313 | GBP 2418 |
| DTO | 906 | 50+ | 28 | 31 | GBP 23,563 | GBP 25,132 | GBP 1569 | GBP 1145 |
| DTO | 907 | 50+ | 31 | 33 | GBP 25,132 | GBP 25,609 | GBP 477 | GBP 348 |
| DTO | 911 | 25–49 | 28 | 30 | GBP 25,145 | GBP 25,470 | GBP 325 | GBP 237 |
| DTO | 101 | 50+ | 28 | 32 | GBP 23,563 | GBP 25,811 | GBP 2248 | GBP 1145 |
| DTO | 2006 | 50+ | 19 | 20 | GBP 16,653 | GBP 16,653 | GBP 0.00 | GBP 0 |
| DTO | 701 | 25–49 | 26 | 29 | GBP 24,144 | GBP 25,470 | GBP 1326 | GBP 968 |
| DTO | 713 | 50+ | 28 | 28 | GBP 23,563 | GBP 23,563 | GBP 0 | GBP 0 |
| DTO | 318 | 25–49 | 29 | 33 | GBP 25,470 | GBP 25,811 | GBP 341 | GBP 249 |
| DTO | 15 | 25–49 | 20 | 24 | GBP 16,701 | GBP 23,383 | GBP 6682 | GBP 4878 |
| Total Social Value Per Participant enrolled with DT + SP | GBP 2082 | |||||||
| Total Social Value Per Participant enrolled with DTO | GBP 1123 | |||||||
| Service Use between Baseline and 8 Weeks | 2 Months before Programme | 2 Months during Programme | Difference in Visits | Cost per Visit 1 | Cost Saving per 2 Months | Cost Saving per 12 Months |
|---|---|---|---|---|---|---|
| GP visits | 7 | 3 | 4 | GBP 39/visit | GBP 156 | GBP 936 |
| Nurse | 6 | 6 | 0 | GBP 44/visit | GBP 0 | GBP 0 |
| Outpatient | 2 | 1 | 1 | GBP 120/visit | GBP 120 | GBP 720 |
| 999 Ambulance | 0 | 0 | 0 | GBP 231/visit | GBP 0 | GBP 0 |
| A&E 2 | 0 | 0 | 0 | GBP 135/visit | GBP 0 | GBP 0 |
| Total cost saving | GBP 276 | GBP 1656 | ||||
| Total cost saving per participant at 8 weeks (n = 12) | GBP 138 | |||||
| Service Use between Baseline and 8 Weeks | 2 Months before Programme | 2 Months during Programme | Difference in Visits | Cost per Visit 1 | Cost Saving per 2 Months | Cost Saving per 12 Months |
|---|---|---|---|---|---|---|
| GP visits | 8 | 2 | 6 | GBP 39/visit | GBP 234 | GBP 1404 |
| Nurse | 9 | 4 | 5 | GBP 44/visit | GBP 220 | GBP 1320 |
| Outpatient | 2 | 3 | 1 | GBP 120/visit | −GBP 120 | −GBP 720 |
| 999 Ambulance | 0 | 0 | 0 | GBP 231/visit | GBP 0 | GBP 0 |
| A&E | 0 | 0 | 0 | GBP 135/visit | GBP 0 | GBP 0 |
| Total cost saving | GBP 334 | GBP 2004 | ||||
| Total cost saving per participant at 8 weeks (n = 12) | GBP 167 | |||||
| SROI Ratio (Social Value Calculator) | SROI Ratio (Mental Health Social Value Calculator) | |
|---|---|---|
| Total social value per participant | GBP 2066 | GBP 2082 |
| NHS cost savings per participant | GBP 138 | GBP 138 |
| Total financial value per participant | GBP 2204 | GBP 2220 |
| Total cost per participant | GBP 472 | GBP 472 |
| SROI ratio | GBP 4.67:GBP 1 | GBP 4.70:GBP 1 |
| SROI Ratio (Social Value Calculator) | SROI Ratio (Mental Health Social Value Calculator) | |
|---|---|---|
| Total social value per participant | GBP 1378 | GBP 1123 |
| NHS cost savings per participant | GBP 167 | GBP 167 |
| Total financial value per participant | GBP 1545 | GBP 1290 |
| Total cost per participant | GBP 305 | GBP 305 |
| SROI ratio | GBP 5.07:GBP 1 | GBP 4.23:GBP 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skinner, A.; Hartfiel, N.; Lynch, M.; Jones, A.W.; Edwards, R.T. Social Return on Investment of Social Prescribing via a Diabetes Technician for Preventing Type 2 Diabetes Progression. Int. J. Environ. Res. Public Health 2023, 20, 6074. https://doi.org/10.3390/ijerph20126074
Skinner A, Hartfiel N, Lynch M, Jones AW, Edwards RT. Social Return on Investment of Social Prescribing via a Diabetes Technician for Preventing Type 2 Diabetes Progression. International Journal of Environmental Research and Public Health. 2023; 20(12):6074. https://doi.org/10.3390/ijerph20126074
Chicago/Turabian StyleSkinner, Adam, Ned Hartfiel, Mary Lynch, Aled Wyn Jones, and Rhiannon Tudor Edwards. 2023. "Social Return on Investment of Social Prescribing via a Diabetes Technician for Preventing Type 2 Diabetes Progression" International Journal of Environmental Research and Public Health 20, no. 12: 6074. https://doi.org/10.3390/ijerph20126074
APA StyleSkinner, A., Hartfiel, N., Lynch, M., Jones, A. W., & Edwards, R. T. (2023). Social Return on Investment of Social Prescribing via a Diabetes Technician for Preventing Type 2 Diabetes Progression. International Journal of Environmental Research and Public Health, 20(12), 6074. https://doi.org/10.3390/ijerph20126074