

Intimate Partner Violence in Khaliji Women: A Review of the Frequency and Related Factors

 , ,
, , 
Abstract
:1. Introduction
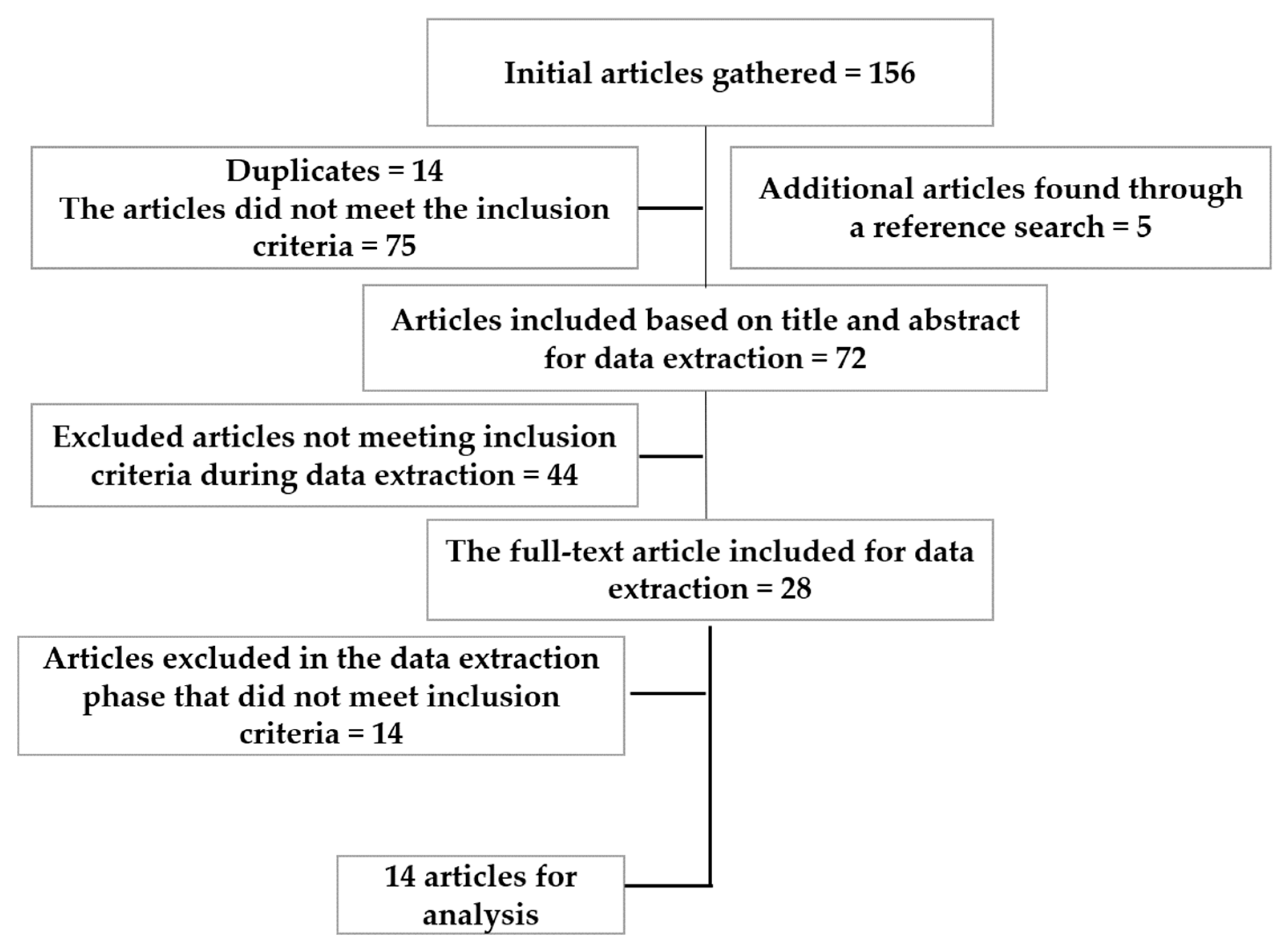
2. Materials and Methods
3. Results
3.1. Frequency
3.2. Associated Factors
4. Discussion
4.1. Associated Factors
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data availability statement
Conflicts of Interest
References
- World Health Organization. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- WHO. Understanding and Addressing Intimate Partner Violence; World Health Organization: Geneva, Switzerland, 2016; WHO/RHR/12.36; Available online: https://apps.who.int/iris/bitstream/handle/10665/42495/9241545615_eng.pdf (accessed on 23 June 2023).
- World Bank. Nearly 2.4 Billion Women Globally Don’t Have Same Economic Rights as Men. Available online: https://www.worldbank.org/en/news/press-release/2022/03/01/nearly-2-4-billion-women-globally-don-t-have-same-economic-rights-as-men (accessed on 1 March 2022).
- Al-Adawi, S. Adolescence in Oman. In International Encyclopedia of Adolescence: A Historical and Cultural Survey of Young People around the World; Routledge: New York, NY, USA, 2006; Volume 2, pp. 713–728. [Google Scholar]
- Al-Adawi, S.; Al-Bahlani, S. Domestic violence: “What’s love got to do with it?”. Sultan Qaboos Univ. Med. J. 2007, 7, 5–14. [Google Scholar] [PubMed]
- Devries, K.M.; Mak, J.Y.; Garcia-Moreno, C.; Petzold, M.; Child, J.C.; Falder, G.; Lim, S.; Bacchus, L.J.; Engell, R.E.; Rosenfeld, L.; et al. The global prevalence of intimate partner violence against women. Science 2013, 340, 1527–1528. [Google Scholar] [CrossRef] [PubMed]
- Oram, S.; Fisher, H.L.; Minnis, H.; Seedat, S.; Walby, S.; Hegarty, K.; Rouf, K.; Angénieux, C.; Callard, F.; Chandra, P.S.; et al. The Lancet Psychiatry Commission on intimate partner violence and mental health: Advancing mental health services, research, and policy. Lancet Psychiatry 2022, 9, 487–524. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.C.; Anderson, J.C.; McFadgion, A.; Gill, J.; Zink, E.; Patch, M.; Callwood, G.; Campbell, D. The Effects of Intimate Partner Violence and Probable Traumatic Brain Injury on Central Nervous System Symptoms. J. Women’s Health 2018, 27, 761–767. [Google Scholar] [CrossRef] [Green Version]
- Bogat, G.A.; Levendosky, A.A.; Cochran, K. Developmental consequences of Intimate Partner Violence on children. Annu. Rev. Clin. Psychol. 2023, 19, 303–329. [Google Scholar] [CrossRef]
- Elghossain, T.; Bott, S.; Akik, C.; Obermeyer, C.M. Prevalence of intimate partner violence against women in the Arab world: A systematic review. BMC Int. Health Hum. Rights 2019, 19, 29. [Google Scholar] [CrossRef] [Green Version]
- Kisa, S.; Gungor, R.; Kisa, A. Domestic Violence Against Women in North African and Middle Eastern Countries: A Scoping Review. Trauma Violence Abus. 2023, 24, 549–575. [Google Scholar] [CrossRef]
- Al-Adawi, S.; Al-Sibani, N.; Al-Harthi, L.; Shetty, M.; Valentina, J.; Al Sadoon, M. The frequency and correlates of mental health problems among Khaliji students in post-secondary education. In Post-Secondary Education Student Mental Health: A Global Perspective; Zangeneh, M., Nouroozifar, M., Eds.; Humber College Institute of Technology and Advanced Learning: Toronto, ON, Canada, 2021; Available online: https://concurrentdisorders.ca/2021/06/23/3117/ (accessed on 15 April 2023).
- The World Bank. Urban Population (% of Total Population)-Middle East & North Africa. Available online: https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS?locations=ZQ (accessed on 11 April 2023).
- Eickelman, D.F. Tribes and Tribal Identity in the Arab Gulf States. In The Emergence of the Gulf States: Studies in Modern History; Peterson, J., Ed.; Bloomsbury Academic: New York, NY, USA, 2016; pp. 223–240. [Google Scholar]
- Dhami, S.; Sheikh, A. The Muslim family: Predicament and promise. West. J. Med. 2000, 173, 352–356. [Google Scholar] [CrossRef] [Green Version]
- The World Bank. Women, Business and the Law. 2020. Available online: https://openknowledge.worldbank.org/server/api/core/bitstreams/6c2b5974-9a3b-5249-995b-2b22e5fd7909/content (accessed on 5 May 2023).
- Zhang, W. The Role of Sex in Intimate Relationships: An Exploration Based on Martin Buber’s Intersubjective Theory. Front. Psychol. 2022, 13, 850278. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, J.; Fang, H.; Wan, Y. Intimate Partner Violence: A Bibliometric Review of Literature. Int. J. Environ. Res. Public Health 2020, 17, 5607. [Google Scholar] [CrossRef]
- Marmot, M.; Wilkinson, R.G. (Eds.) Social Determinants of Health, 2nd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Wali, R.; Khalil, A.; Alattas, R.; Foudah, R.; Meftah, I.; Sarhan, S. Prevalence and risk factors of domestic violence in women attending the National Guard Primary Health Care Centers in the Western Region, Saudi Arabia, 2018. BMC Public Health 2020, 20, 239. [Google Scholar] [CrossRef] [PubMed]
- Afifi, Z.E.; Al-Muhaideb, N.S.; Hadish, N.F.; Ismail, F.I.; Al-Qeamy, F.M. Domestic violence and its impact on married women’s health in Eastern Saudi Arabia. Saudi Med. J. 2011, 32, 612–620. [Google Scholar] [PubMed]
- Alzahrani, T.A.; Abaalkhail, B.A.; Ramadan, I.K. Prevalence of intimate partner violence and its associated risk factors among Saudi female patients attending the primary healthcare centers in Western Saudi Arabia. Saudi Med. J. 2016, 37, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Alquaiz, A.M.; Almuneef, M.; Kazi, A.; Almeneessier, A. Social Determinants of Domestic Violence Among Saudi Married Women in Riyadh, Kingdom of Saudi Arabia. J. Interpers. Violence 2021, 36, NP1561–1585NP. [Google Scholar] [CrossRef]
- Barnawi, F.H. Prevalence and Risk Factors of Domestic Violence Against Women Attending a Primary Care Center in Riyadh, Saudi Arabia. J. Interpers. Violence 2017, 32, 1171–1186. [Google Scholar] [CrossRef] [PubMed]
- Eldoseri, H.M.; Sharps, P. Risk Factors for Spousal Physical Violence Against Women in Saudi Arabia. J. Interpers. Violence 2020, 35, 1269–1293. [Google Scholar] [CrossRef]
- Abolfotouh, M.A.; Almuneef, M. Prevalence, pattern and factors of intimate partner violence against Saudi women. J. Public Health 2020, 42, e206–e214. [Google Scholar] [CrossRef]
- Al Kendi, A.; Al Shidhani, N.; Al Kiyumi, M. Domestic violence among Omani women: Prevalence, risk factors and help-seeking behaviour. East. Mediterr. Health J. 2021, 27, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Al Serkal, F.; Hussein, H.; El Sawaf, E.; Al Faisal, W.; Mahdy, N.H.; Wasfy, A. Intimate Partner Violence against Women in Dubai: Prevalence, Associated Factors and Health Consequences, 2012–2013. Middle East J. Psychiatry Alzheimers 2014, 5, 19–27. [Google Scholar] [CrossRef]
- AlMulla, K.A.; Alothman, H.M. Spousal Violence Against Women in the UAE Society. Available online: https://web.archive.org/web/20201106104750id_/https://ajsj.journals.ekb.eg/article_102899_7e92ca59bc7dd437d8f0073dfadd1e99.pdf (accessed on 14 April 2023).
- Al-Ghanim, K.A. Violence against women in Qatari society. J. Middle East Women’s Stud. 2009, 5, 80–93. [Google Scholar] [CrossRef]
- Bubshait, M.; Al-Jamea, L.; Al-Ekri, E.; Al Ubaidi, B.A.; Al-Dhubaib, D.; Najem, W.; Husain, H. Prevalence of Domestic Violence & Associated Risk Factors among Adult Females attending Primary Care in the Kingdom of Bahrain. Preval. Int. Med. J. 2021, 28, 4413–4425. [Google Scholar]
- Al Ubaidi, B.; Tawfeeq, F.; Ayed, H.; Hasan, S.; Alahmed, F. Intimate partner violence in the Kingdom of Bahrain: Prevalence, associated factors and WAST screening in primary health centres. J. Fam. Med. Prim. Care 2021, 10, 2893–2899. [Google Scholar] [CrossRef]
- Alsaleh, A. Violence Against Kuwaiti Women. J. Interpers. Violence 2022, 37, NP3628–NP3649. [Google Scholar] [CrossRef]
- Smith, R. Oman: Leaping across the centuries. BMJ 1988, 297, 540–544. [Google Scholar] [CrossRef] [Green Version]
- Secretariat General of the Gulf Cooperation Council. The Cooperation Council for the Arab States of the Gulf. Available online: https://www.gcc-sg.org/en-us/Pages/default.aspx (accessed on 6 April 2023).
- AlQahtani, S.M.; Almutairi, D.S.; BinAqeel, E.A.; Almutairi, R.A.; Al-Qahtani, R.D.; Menezes, R.G. Honor Killings in the Eastern Mediterranean Region: A Narrative Review. Healthcare 2022, 11, 74. [Google Scholar] [CrossRef]
- Islam, M.M.; Dorvlo, A.S.; Al-Qasmi, A.M. The pattern of female nuptiality in Oman. Sultan Qaboos Univ. Med. J. 2013, 13, 32–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yount, K.M.; Bergenfeld, I.; Mhamud, N.; Clark, C.J.; Kaslow, N.J.; Cheong, Y.F. Monitoring sustainable development goal 5.2: Cross-country cross-time invariance of measures for intimate partner violence. PLoS ONE 2022, 17, e0267373. [Google Scholar] [CrossRef] [PubMed]
- Daher-Nashif, S.; Bawadi, H. Women’s Health and Well-Being in the United Nations Sustainable Development Goals: A Narrative Review of Achievements and Gaps in the Gulf States. Int. J. Environ. Res. Public Health 2020, 17, 1059. [Google Scholar] [CrossRef] [Green Version]
- Sardinha, L.; Maheu-Giroux, M.; Stöckl, H.; Meyer, S.R.; García-Moreno, C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet 2022, 399, 803–813. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Violence against Women. Available online: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed on 23 June 2023).
- Román-Gálvez, R.M.; Martín-Peláez, S.; Fernández-Félix, B.M.; Zamora, J.; Khan, K.S.; Bueno-Cavanillas, A. Worldwide Prevalence of Intimate Partner Violence in Pregnancy. A Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 738459. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Violence against Women and Girls–What the Data Tell Us. 2022. Available online: https://genderdata.worldbank.org/data-stories/overview-of-gender-based-violence/ (accessed on 23 June 2023).
- Chan, M.F.; Al Balushi, R.; Al Falahi, M.; Mahadevan, S.; Al Saadoon, M.; Al-Adawi, S. Child and adolescent mental health disorders in the GCC: A systematic review and meta-analysis. Int. J. Pediatr. Adolesc. Med. 2021, 8, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Roman, N.V.; Frantz, J.M. The prevalence of intimate partner violence in the family: A systematic review of the implications for adolescents in Africa. Fam. Pract. 2013, 30, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusunoki, Y.; Bevilacqua, K.; Barber, J.S. The Dynamics of Intimate Relationships and Violent Victimization Among Young Women. J. Interpers. Violence 2023, 38, 3344–3372. [Google Scholar] [CrossRef]
- Kuckartz, U. Qualitative Text Analysis: A Systematic Approach. In Compendium for Early Career Researchers in Mathematics Education; ICME-13 Monographs; Kaiser, G., Presmeg, N., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef] [Green Version]
- Mthembu, J.; Mabaso, M.; Reis, S.; Zuma, K.; Zungu, N. Prevalence and factors associated with intimate partner violence among the adolescent girls and young women in South Africa: Findings the 2017 population based cross-sectional survey. BMC Public Health 2021, 21, 1160. [Google Scholar] [CrossRef]
- Al-Shroby, W.A.; Sulimani, S.M.; Alhurishi, S.A.; Bin Dayel, M.E.; Alsanie, N.A.; Alhraiwil, N.J. Awareness of Premarital Screening and Genetic Counseling among Saudis and its Association with Sociodemographic Factors: A National Study. J. Multidiscip. Healthc. 2021, 14, 389–399. [Google Scholar] [CrossRef]
- Ministry of Health. Premarital Screening. Available online: https://www.moh.gov.sa/en/HealthAwareness/Beforemarriage/Pages/default.aspx (accessed on 23 June 2023).
- United Nations. Violence Against Women ‘Most Shameful’, Pervasive Human Rights Violation, Says Secretary-General in Remarks on International Women’s Day. Press Release SG/SM/6919WOM/1113. 8 March 1999. Available online: https://press.un.org/en/1999/19990308.sgsm6919.html (accessed on 23 June 2023).
- World Health Organization. Global and Regional Estimates of Violence against Women: Prevalence and Health Effects of Intimate Partner Violence and Non-Partner Sexual Violence; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Bott, S.; Guedes, A.; Ruiz-Celis, A.P.; Mendoza, J.A. Intimate partner violence in the Americas: A systematic review and reanalysis of national prevalence estimates. Rev. Panam. Salud Publica 2019, 43, e26. [Google Scholar] [CrossRef] [Green Version]
- Barbier, A.; Chariot, P.; Lefèvre, T. Intimate partner violence against ever-partnered women in Europe: Prevalence and associated factors-Results from the violence against women EU-wide survey. Front. Public Health 2022, 10, 1033465. [Google Scholar] [CrossRef]
- Jewkes, R.; Fulu, E.; Tabassam Naved, R.; Chirwa, E.; Dunkle, K.; Haardörfer, R.; Garcia-Moreno, C.; UN Multi-Country Study on Men and Violence Study Team. Women’s and men’s reports of past-year prevalence of intimate partner violence and rape and women’s risk factors for intimate partner violence: A multicountry cross-sectional study in Asia and the Pacific. PLoS Med. 2017, 14, e1002381. [Google Scholar] [CrossRef] [Green Version]
- Magnussen, L.; Shoultz, J.; Richardson, K.; Oneha, M.F.; Campbell, J.C.; Matsunaga, D.S.; Selifis, S.M.; Sapolu, M.; Samifua, M.; Manzano, H.; et al. Responding to the needs of culturally diverse women who experience intimate partner violence. Hawaii Med. J. 2011, 70, 9–15. [Google Scholar]
- Alhalal, E. Obesity in women who have experienced intimate partner violence. J. Adv. Nurs. 2018, 74, 2785–2797. [Google Scholar] [CrossRef]
- Puhl, R.M.; Latner, J.D. Stigma, obesity, and the health of the nation’s children. Psychol. Bull. 2007, 133, 557–580. [Google Scholar] [CrossRef] [Green Version]
- Mabry, R.M.; Reeves, M.M.; Eakin, E.G.; Owen, N. Evidence of physical activity participation among men and women in the countries of the Gulf cooperation council: A review. Obes. Rev. 2010, 11, 457–464. [Google Scholar] [CrossRef]
- Al-Adawi, S.; Jaju, S.; Al-Zakwani, I.; Dorvlo, A.S. Culture to culture: Fat-phobia and somatization. In Handbook of Behavior, Food and Nutrition; Preedy, V.R., Watson, R.R., Martin, C.R., Eds.; Springer: New York, NY, USA, 2011; pp. 1457–1473. [Google Scholar] [CrossRef]
- Zhou, M. The shifting income-obesity relationship: Conditioning effects from economic development and globalization. SSM Popul. Health 2021, 15, 100849. [Google Scholar] [CrossRef]
- Al-Nozha, M.M.; Al-Hazzaa, H.M.; Arafah, M.R.; Al-Khadra, A.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Khan, N.B.; Al-Marzouki, K.; Al-Harthi, S.S.; Abdullah, M.; et al. Prevalence of physical activity and inactivity among Saudis aged 30–70 years. A population-based cross-sectional study. Saudi Med. J. 2007, 28, 559–568. [Google Scholar]
- World Health Organization. Understanding and Addressing against Women. Available online: https://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf;jsessionid=F5C4834B45B9143D5CE206134E9EA496?sequence=1 (accessed on 23 June 2023).
- Luepnitz, D.A.; Wieland, P. The Family Interpreted: Psychoanalysis, Feminism, and Family Therapy: Feminist Theory in Clinical Practice; Basic Books: New York, NY, USA, 2002. [Google Scholar]
- Willers, M.D. Stigmatization of divorced persons: Effects of multiple divorce and gender. Theses Digit. Proj. 1993, 659. Available online: https://scholarworks.lib.csusb.edu/etd-project/667 (accessed on 14 April 2023).
- Al-Barwani, T.A.; Albeely, T.S. The Omani family: Strengths and challenges. Marriage Fam. Rev. 2007, 41, 119–142. [Google Scholar] [CrossRef]
- Lari, N.; Al-Thani, M. Divorce Legislation in the Arab Gulf: Trends and Educational Differentials. J. Arab. Stud. 2021, 11, 289–313. [Google Scholar] [CrossRef]
- Mokdad Zmitri, M. Couples and families’ resilience in facing sociocultural changes: “Co-maternity” and “Oedipus in law” in the Tunisian transitional context. Psychoanal. Cult. Soc. 2023, 28, 93–106. [Google Scholar] [CrossRef]
- Weitzman, A. Does Increasing Women’s Education Reduce Their Risk of Intimate Partner Violence? Evidence from an Edu-cation Policy Reform. Criminology 2018, 56, 574–607. [Google Scholar] [CrossRef] [PubMed]
- Abousleiman, I. GCC Reforms Are Changing Women’s Lives. The World Bank. 4 March 2020. Available online: https://www.worldbank.org/en/news/opinion/2020/03/04/gcc-reforms-are-changing-womens-lives (accessed on 25 May 2023).
- Abdallah, H. Qatari Women ‘Outnumber Men’ at Local Universities. Dohanews 7 March 2021. Available online: https://dohanews.co/qatari-women-outnumber-men-at-local-universities/ (accessed on 3 June 2023).
- Mohamed, N.A.; Abdulhadi, N.N.; Al-Maniri, A.A.; Al-Lawati, N.R.; Al-Qasmi, A.M. The trend of feminization of doctors’ workforce in Oman: Is it a phenomenon that could rouse the health system? Hum. Resour. Health 2018, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.D.; Nguyen, H.; Fisher, J. Attitudes towards intimate partner violence against women among women and men in 39 low-and middle-income countries. PLoS ONE 2016, 11, e0167438. [Google Scholar] [CrossRef] [Green Version]
- Yamani, M. Polygamy and Law in Contemporary Saudi Arabia; Ithaca Press: Ithaca, NY, USA, 2008. [Google Scholar]
- Ahinkorah, B.O. Polygyny and intimate partner violence in sub-Saharan Africa: Evidence from 16 cross-sectional demographic and health surveys. SSM Popul. Health 2021, 13, 100729. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.J.; Perera, R.A.; Masho, S.W.; Mezuk, B.; Cohen, S.A. Adverse childhood experiences and intimate partner aggression in the US: Sex differences and similarities in psychosocial mediation. Soc. Sci. Med. 2015, 131, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Mair, C.; Cunradi, C.B.; Todd, M. Adverse childhood experiences and intimate partner violence: Testing psychosocial mediational pathways among couples. Ann. Epidemiol. 2012, 22, 832–839. [Google Scholar] [CrossRef] [Green Version]
- Khoury, L.; Tang, Y.L.; Bradley, B.; Cubells, J.F.; Ressler, K.J. Substance use, childhood traumatic experience, and Posttraumatic Stress Disorder in an urban civilian population. Depress. Anxiety 2010, 27, 1077–1086. [Google Scholar] [CrossRef]
- Kwan, J.; Sparrow, K.; Facer-Irwin, E.; Thandi, G.; Fear, N.T.; MacManus, D. Prevalence of intimate partner violence perpetration among military populations: A systematic review and meta-analysis. Aggress. Violent Behav. 2020, 53, 101419. [Google Scholar] [CrossRef]
- Centers for Disease Control and Preventation. Violence Prevention: Risk and Protective Factors for Perpetration. CDC 24/7; Saving Lives, Protecting People. Available online: https://www.cdc.gov/violenceprevention/intimatepartnerviolence/riskprotectivefactors.html (accessed on 4 May 2023).
- Baker, K.A.; Dwairy, M. Cultural norms versus state law in treating incest: A suggested model for Arab families. Child Abuse Negl. 2003, 27, 109–123. [Google Scholar] [CrossRef]
- Richards, B. Autonomy and the Law: Widely Used, Poorly Defined. In Beyond Autonomy: Limits and Alternatives to Informed Consent in Research Ethics and Law; Cambridge Bioethics and Law; Kirchhoffer, D., Richards, B., Eds.; Cambridge University Press: Cambridge, UK, 2019; pp. 17–32. [Google Scholar] [CrossRef]
- Ford, J.D.; Grasso, D.J.; Elhai, J.D.; Courtois, C.A. Social, cultural, and other diversity issues in the traumatic stress field. Posttraumatic Stress Disord. 2015, 503–546. [Google Scholar] [CrossRef]
- McCauley, H.L.; Bonomi, A.E.; Maas, M.K.; Bogen, K.W.; O’Malley, T.L. #MaybeHeDoesntHitYou: Social Media Underscore the Re-alities of Intimate Partner Violence. J. Women’s Health 2018, 27, 885–891. [Google Scholar] [CrossRef]
- Homan, C.M.; Schrading, J.N.; Ptucha, R.W.; Cerulli, C.; Ovesdotter Alm, C. Quantitative Methods for Analyzing Intimate Partner Violence in Microblogs: Observational Study. J. Med. Internet Res. 2020, 22, e15347. [Google Scholar] [CrossRef] [PubMed]
- Roesch, E.; Amin, A.; Gupta, J.; García-Moreno, C. Violence against women during COVID-19 pandemic restrictions. BMJ 2020, 369, m1712. [Google Scholar] [CrossRef] [PubMed]
- Almegewly, W.H.; Hawamdah, S.; Moussa, F.L.; Dator WL, T.; Alonezi, A.; Al-Eissa, M. Measuring Nurses’ and Physicians’ Attitudes and Perceptions of the Appropriate Interventions towards Intimate Partner Violence in Saudi Arabia. Healthcare 2022, 10, 1430. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuwari, M. Tribe and Tribalism: The Trojan Horse of GCC States? In Divided Gulf, Contemporary Gulf Studies; Krieg, A., Ed.; Springer Nature: Singapore, 2019; pp. 37–51. [Google Scholar]


{kind=link}
| Country | Authors | IPV Detection Tool | n | Catchment Area | Prevalence |
|---|---|---|---|---|---|
| Saudi Arabia | Wali et al. [21] | Norvold Domestic Abuse Questionnaire | n = 1845 | Primary Health Care, Western Region | Lifetime prevalence = 33.24% |
| Psychological abuse = 48.47% | |||||
| Physical abuse = 34.77% | |||||
| Sexual abuse = 16.75% | |||||
| All three types of abuse = 4.1% | |||||
| Afif et al. [22] | The authors’ self-developed questionnaire with input from WHO Multi-country Study | n = 2000 | Al-Ahsa Oasis in the Eastern Province | Lifetime—39.3% | |
| Mental—35.9% | |||||
| Physical—17.9% | |||||
| Sexual—6.9% | |||||
| Alzahrani, Abaalkhail, and Ramadan [23] | Self-developed questionnaire with input from the World Health Organisation | n = 497 | Primary Health Care, Taif City | Overall—11.9% | |
| Alquaiz et al. [24] | Modified from the Intimate Partner Violence Against Women Questionnaire developed by the World Health Organisation | n = 1883 | Primary Health Care, Riyadh | Lifetime violence—43% | |
| Controlling behaviour—36.8% | |||||
| Emotional—22% | |||||
| Physical—9% | |||||
| Sexual—12.7% | |||||
| Barnawi [25] | Author’s self-developed questionnaire | n = 720 | Al-Wazarat Primary Health Care, Riyadh | Overall—20% | |
| Emotional—69% | |||||
| Social—34% | |||||
| Financial—26% | |||||
| Physical—20% | |||||
| Sexual—10% | |||||
| Eldoseri and Sharps [26] | World Health Organisation Violence against Women Questionnaire (v.10.0) | n = 200 | Primary Health Care, Jeddah City | Physical violence = 45.5% | |
| Abolfotouh and Almuneef [27] | WHO multi-country instrument on violence against women | n = 400 | Primary Health Care, Riyadh | Overall—44.8% | |
| Physical—18.5% | |||||
| Emotional—25.5 | |||||
| Sexual—19.2% | |||||
| Financial—25.3% | |||||
| Oman | Al Kendi et al. [28] | The authors developed a self-developed questionnaire with input from the Norvold Domestic Abuse Questionnaire | n = 978 | Primary Health Care, Muscat Governorate | Lifetime—28.8% |
| Emotional—21% | |||||
| Physical—18% | |||||
| Emotional and physical—10.1% | |||||
| UAE | Serkal et al. [29] | Self-developed questionnaire | n = 700 | Primary Health Care, Dubai | Physical—7.14% |
| Sexual—3.7% | |||||
| Psychological—7.5% | |||||
| AlMulla and Alothman [30] | Self-developed questionnaire | n = 920 married women | National community survey | Physical—32% | |
| Psychological—46% | |||||
| Sexual—14% | |||||
| Qatar | Al-Ghanim [31] | Author’s self-developed questionnaire | n = 2787 | A national tertiary education centre in Doha | Overall—2.22% |
| Overall—12.4% | |||||
| Bubshait et al. [32] | Authors’ self-developed questionnaire with input from the Norvold Abuse Questionnaire | n = 602 | Primary Health Care | Overall—30.1% | |
| Emotional—60% | |||||
| Physical—32.9% | |||||
| Sexual—13.8% | |||||
| Financial—21.3 | |||||
| Al Ubaidi et al. [33] | Women Abuse Screening Tool—Short Version | n = 810 women | Primary Health Care | Overall—71.7% | |
| Kuwait | Alsaleh [34] | The Severity of Violence Against Women Scales Women’s Experiences with Battering Scale | n = 1335 women, randomly selected community survey | Kuwait City | Physical—71% |
| Sexual—81% | |||||
| Psychological—89% |
| Four Significant Descriptors | Content of Associated Factors |
|---|---|
| Demographic Factors | Age of the victim and duration of the marriage |
| Victims with above-average weight | |
| The victim has divorced parents | |
| The victim has gone through a divorce and remarried | |
| Perpetrator living with a widowed mother | |
| Education level of the victim | |
| Sociocultural Factors | Victims living in a polygamous marriage |
| Victims who live in households that sanction violence in a marital context | |
| Victims allege a lack of support from society | |
| Socioeconomic Factors | The victim does not receive tangible support in her marriage |
| The victim lives in a household with insufficient income | |
| Victim’s perceived lack of financial independence from the perpetrator | |
| The perpetrator controls the financial matters of the victim | |
| Perpetrator-Related Factors | The perpetrator has a history of ACE (adverse childhood experience) |
| The low educational level of the perpetrator | |
| Unemployed perpetrator | |
| Perpetrator’s employment in a military occupation | |
| Perpetrator’s smoking, alcohol use, and gambling habits | |
| A perpetrator with poor self-regulation, poor mental health outcome, and autocratic tendencies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Kiyumi, M.H.; Al Shidhani, A.S.; Al Sumri, H.; Al Saidi, Y.; Al Harrasi, A.; Al Kiyumi, M.; Al Sumri, S.; Al Toubi, A.; Shetty, M.; Al-Adawi, S. Intimate Partner Violence in Khaliji Women: A Review of the Frequency and Related Factors. Int. J. Environ. Res. Public Health 2023, 20, 6241. https://doi.org/10.3390/ijerph20136241
Al Kiyumi MH, Al Shidhani AS, Al Sumri H, Al Saidi Y, Al Harrasi A, Al Kiyumi M, Al Sumri S, Al Toubi A, Shetty M, Al-Adawi S. Intimate Partner Violence in Khaliji Women: A Review of the Frequency and Related Factors. International Journal of Environmental Research and Public Health. 2023; 20(13):6241. https://doi.org/10.3390/ijerph20136241
Chicago/Turabian StyleAl Kiyumi, Maisa H., Asma Said Al Shidhani, Hana Al Sumri, Yaqoub Al Saidi, Amira Al Harrasi, Maryam Al Kiyumi, Sanaa Al Sumri, Aseel Al Toubi, Maithili Shetty, and Samir Al-Adawi. 2023. "Intimate Partner Violence in Khaliji Women: A Review of the Frequency and Related Factors" International Journal of Environmental Research and Public Health 20, no. 13: 6241. https://doi.org/10.3390/ijerph20136241
APA StyleAl Kiyumi, M. H., Al Shidhani, A. S., Al Sumri, H., Al Saidi, Y., Al Harrasi, A., Al Kiyumi, M., Al Sumri, S., Al Toubi, A., Shetty, M., & Al-Adawi, S. (2023). Intimate Partner Violence in Khaliji Women: A Review of the Frequency and Related Factors. International Journal of Environmental Research and Public Health, 20(13), 6241. https://doi.org/10.3390/ijerph20136241