

A Systematic Review of Qualitative Research Literature and a Thematic Synthesis of Older LGBTQ People’s Experiences of Quality of Life, Minority Joy, Resilience, Minority Stress, Discrimination, and Stigmatization in Japan and Sweden

 , , , and
, , , and
Abstract
:1. Introduction
- In-depth understanding: By focusing on qualitative research, we can develop knowledge based on the details of participants’ experiences, capturing the richness and complexity of their stories.
- Contextual insights: By examining the social interactions and individual experiences in natural, non-experimental situations, we can gain valuable insights into the specific cultural, social, and historical factors that shape the experiences of older LGBTQ individuals in Japan and Sweden.
- Bridging research gaps: Synthesizing qualitative research findings can also help identify research gaps. By examining existing qualitative studies, we can identify areas where more in-depth investigations are needed and contribute to the development of future primary studies. This process can help fill the knowledge gaps and further advance our understanding of the experiences of older LGBTQ individuals.
1.1. Aim
Research Question
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
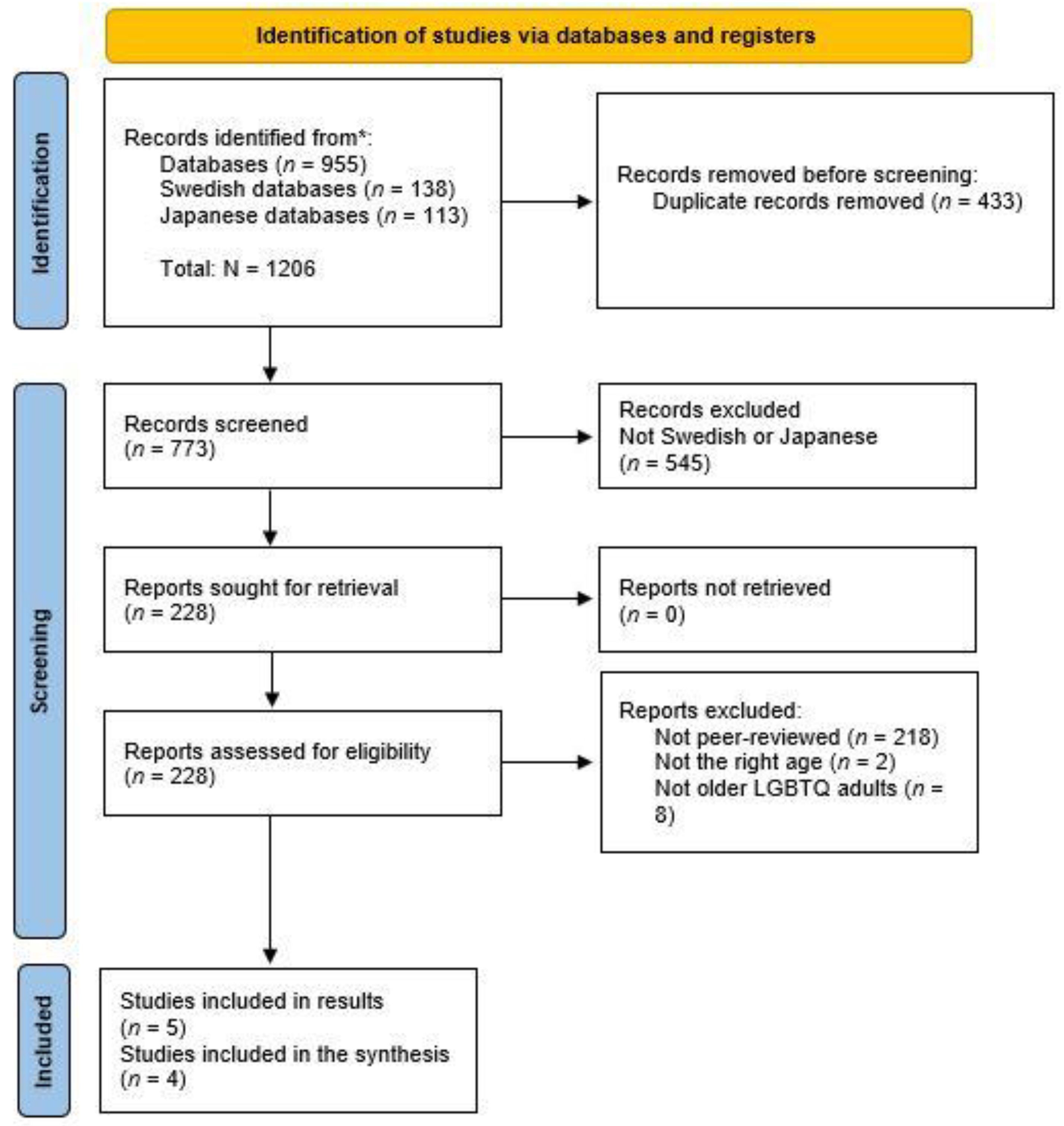
2.3. Search Strategy and Study Selection
2.4. Synthesis Methodology
3. Results
3.1. Data Extraction
3.2. Findings
3.2.1. QOL, Minority Joy, and Resilience
… We’re all individuals and we’re all different. You have to show consideration to everyone.
And some people need to act or think in one way. And other people think in another way. And that means you can’t treat everyone the same because it’s wrong somehow…
It has strengthened me a lot. When I meet my old classmates, even if they understand that I am gay, I feel that I have my own life, I belong somewhere, and I have my own context and that is so very important; so I am really happy for the struggle that has been faced
We had several people [in our gay choir] who were HIV positive and died. And some of them got so skinny. We sang at the Rosenlund hospital for those who were hospitalized there, and for some, it was so secretive that they did not even come out of their rooms but just opened the door so they could hear us. Their parents had no idea they were HIV positive. It was pretty horrible.
3.2.2. Discrimination, Stigmatization, and Minority Stress
They [colleagues] used me as a subject for the morning prayers, praying for me to get cured… I experienced more and more opposition at work and then I got called up to my boss, who offered to retire me early.
It has been a threat that someone would find out that I was interested in wearing women’s clothes. So I stayed away from that. I felt I would be completely estranged and left out if I did that. And that is something transvestites live with to a great extent; that you simply get pointed out and shamed. And I lived with this, and still do, as a limiting part.
As long as I live at home, I think it will be alright, but then when you get older and maybe have to move to a nursing home … Yes, when it is time and they come here and see that it is a man in women’s clothes, “God how disgusting; we don’t want to go to that person again,” you know right?
… when they heard that I had atrial fibrillation and a pacemaker and took a lot of heart medicine and Varan [medicine], yes, then [the doctor] just put down the pen and said, “you can forget about that, because no one will put a knife in you if it’s not absolutely necessary”
4. Discussion
4.1. Study Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing and Health [Internet]. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 2 March 2023).
- Wittgens, C.; Fischer, M.M.; Buspavanich, P.; Theobald, S.; Schweizer, K.; Trautmann, S. Mental health in people with minority sexual orientations: A meta-analysis of population-based studies. Acta Psychiatr. Scand. 2022, 145, 357–372. [Google Scholar] [CrossRef]
- Lick, D.J.; Durso, L.E.; Johnson, K.L. Minority Stress and Physical Health Among Sexual Minorities. Perspect. Psychol. Sci. 2013, 8, 521–548. [Google Scholar] [CrossRef] [Green Version]
- Meyer, I.H. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Bränström, R. Minority stress factors as mediators of sexual orientation disparities in mental health treatment: A longitudinal population-based study. J. Epidemiol. Community Health 2017, 71, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Nadal, K.L.; Skolnik, A.; Wong, Y. Interpersonal and Systemic Microaggressions Toward Transgender People: Implications for Counseling. J. LGBT Issues Couns. 2012, 6, 55–82. [Google Scholar] [CrossRef]
- Lundberg, T.; Malmquist, A.; Wurm, M. Upplevelser och hantering av minoritetsstress och mikroaggressioner bland unga hbtq-personer i Sverige. In Jag Är Inte Ensam, Det Finns Andra Som Jag: Unga Hbtqi-Personers Livsvillkor (Experiences and Management of Minority Stress and Micro Aggressions among Young LGBTQ People in Sweden. I Am Not Alone, There Are Others Like Me: The Living Conditions of Young LGBTQI People); Swedish Agency for Youth and Civil Society (Myndigheten för Ungdoms-och Civilsamhällesfrågor (MUCF)): Växjö, Sweden, 2022; pp. 315–344. [Google Scholar]
- Lundberg, T.; Wurm, M.; Malmquist, A. Att göra livet (över)levbart: Transpersoners ontiska, relationella och reflekterande arbete för att skapa minoritetsro och hantera utsatthet i vardagen. (Making life survivable/livable: Transpeople’s ontic, relational and reflective work to create minority calmness and manage vulnerability in everyday life). (Tidskr För Genusvetenskap) J. Gend. Stud. 2022, 43, 7–26. [Google Scholar] [CrossRef]
- Fredriksen Goldsen, K.I.; Jen, S.; Muraco, A. Iridescent Life Course: LGBTQ Aging Research and Blueprint for the Future—A Systematic Review. Gerontology 2019, 65, 253–274. [Google Scholar] [CrossRef]
- Choi, S.K.; Meyer, I.H. LGBT Aging: A Review of Research Findings, Needs, and Policy Implications [Internet]. The Williams Institute at UCLA School of Law. 2016. Available online: https://www.jstor.org/stable/resrep34905 (accessed on 2 March 2023).
- Mahieu, L.; Cavolo, A.; Gastmans, C. How do community-dwelling LGBT people perceive sexuality in residential aged care? A systematic literature review. Aging Ment. Health 2019, 23, 529–540. [Google Scholar] [CrossRef]
- Fredriksen Goldsen, K.; Kim, H.J.; Jung, H.; Goldsen, J. The Evolution of Aging With Pride—National Health, Aging, and Sexuality/Gender Study: Illuminating the Iridescent Life Course of LGBTQ Adults Aged 80 Years and Older in the United States. Int. J. Aging Hum. Dev. 2019, 88, 380–404. [Google Scholar] [CrossRef]
- Fredriksen-Goldsen, K.I.; Muraco, A. Aging and Sexual Orientation: A 25-Year Review of the Literature. Res. Aging 2010, 32, 372–413. [Google Scholar] [CrossRef]
- Plöderl, M.; Tremblay, P. Mental health of sexual minorities. A systematic review. Int. Rev. Psychiatry 2015, 27, 367–385. [Google Scholar] [CrossRef]
- Thummapol, O.; Srithumsuk, W.; Park, T. A scoping review of experiences and needs of older LGBTI adults in Asia. J. Gay Lesbian Soc. Serv. 2022, 34, 403–414. [Google Scholar] [CrossRef]
- Mirai|MIRAI—Connecting Swedish och Japanese Universities [Internet]. Available online: https://www.mirai.nu/ (accessed on 5 June 2023).
- Aspers, P.; Corte, U. What is Qualitative in Qualitative Research. Qual. Sociol. 2019, 42, 139–160. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.; Noyes, J.; Flemming, K.; Gerhardus, A.; Wahlster, P.; Van Der Wilt, G.J.; Mozygemba, K.; Refolo, P.; Sacchini, D.; Tummers, M.; et al. Guidance on Choosing Qualitative Evidence Synthesis Methods for Use in Health Technology Assessments of Complex Interventions [Internet]. 2016. Available online: http://www.integrate-hta.eu/downloads/ (accessed on 22 April 2023).
- Addis, S.; Davies, M.; Greene, G.; MacBride-Stewart, S.; Shepherd, M. The health, social care and housing needs of lesbian, gay, bisexual and transgender older people: A review of the literature. Health Soc. Care Community 2009, 17, 647–658. [Google Scholar] [CrossRef]
- Averett, P.; Jenkins, C. Review of the literature on older lesbians: Implications for education, practice, and research. J. Appl. Gerontol. 2012, 31, 537–561. [Google Scholar] [CrossRef]
- Caceres, B.A.; Jackman, K.B.; Ferrer, L.; Cato, K.D.; Hughes, T.L. A scoping review of sexual minority women’s health in Latin America and the Caribbean. Int. J. Nurs. Stud. 2019, 94, 85–97. [Google Scholar] [CrossRef]
- Chen, J.; McLaren, H.; Jones, M.; Shams, L. The Aging Experiences of LGBTQ Ethnic Minority Older Adults: A Systematic Review. Gerontologist 2020, 62, e162–e177. [Google Scholar] [CrossRef]
- Fish, J.; Weis, C. All the lonely people, where do they all belong? An interpretive synthesis of loneliness and social support in older lesbian, gay and bisexual communities. Qual. Ageing Older Adults 2019, 20, 130–142. [Google Scholar] [CrossRef]
- Lecompte, M.; Ducharme, J.; Beauchamp, J.; Couture, M. Inclusive Practices toward LGBT Older Adults in Healthcare and Social Services: A Scoping Review of Quantitative and Qualitative Evidence. Clin. Gerontol. 2021, 44, 210–221. [Google Scholar] [CrossRef]
- McParland, J.; Camic, P.M. Psychosocial factors and ageing in older lesbian, gay and bisexual people: A systematic review of the literature. J. Clin. Nurs. 2016, 25, 3415–3437. [Google Scholar] [CrossRef] [PubMed]
- McCann, E.; Brown, M.J. The mental health needs and concerns of older people who identify as LGBTQ+: A narrative review of the international evidence. J. Adv. Nurs. 2019, 75, 3390–3403. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S. Stigma, time to address the issues: A literature review. HIV Nurs. 2017, 17, 103–107. [Google Scholar]
- Siverskog, A. “They Just Don’t Have a Clue”: Transgender Aging and Implications for Social Work. J. Gerontol. Soc. Work 2014, 57, 386–406. [Google Scholar] [CrossRef] [PubMed]
- Kottorp, A.; Johansson, K.; Aase, P.; Rosenberg, L. Housing for ageing LGBTQ people in Sweden: A descriptive study of needs, preferences, and concerns. Scand. J. Occup. Ther. 2016, 23, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Jönson, H.; Siverskog, A. Turning vinegar into wine: Humorous self-presentations among older GLBTQ online daters. J. Aging Stud. 2012, 26, 55–64. [Google Scholar] [CrossRef]
- Whoqol Group. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar]
- Kenkou Nippon 21. Kenkou Nippon 21 Souron Sankou Shiryou [Internet]. The Japanese Ministry of Health, Labour and Welfare. 2000. Available online: https://www.mhlw.go.jp/www1/topics/kenko21_11/s1.html#A1 (accessed on 7 April 2023).
- Government Bill A Dignified Life in Eldercare [2009/10:116] 2010. Available online: https://www.regeringen.se/rattsliga-dokument/proposition/2010/03/prop.-200910116 (accessed on 7 April 2023).
- Swedish Official Report. A Dignified Life in Eldercare [2008:51] 2008. Available online: https://www.regeringen.se/rattsliga-dokument/statens-offentliga-utredningar/2008/05/sou-200851/ (accessed on 7 April 2023).
- Swedish Official Report. Read Me! Simplified Decision Making and Special Accommodation for Older people (Part 1 and 2) [2017:21] 2017. Available online: https://www.regeringen.se/rattsliga-dokument/statens-offentliga-utredningar/2017/03/sou-201721/ (accessed on 7 April 2023).
- Swedish Social Services Act [2001:453] Chapter 5, Article 4. 2023. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453 (accessed on 7 April 2023).
- Wurm, M.; Mejias-Nihlén, T.; Filis, P.; Lundberg, T.; Malmquist, A. Minority joy: Positive aspects experienced by trans* people. In Proceedings of the Oral Presentation at the 8th Nordic Trans Conference, Tampere, Finland, 23–25 February 2023. [Google Scholar]
- Fletcher, D.; Sarkar, M. Psychological Resilience. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Hash, K.M.; Rogers, A. Clinical Practice with Older LGBT Clients: Overcoming Lifelong Stigma Through Strength and Resilience. Clin. Soc. Work. J. 2013, 41, 249–257. [Google Scholar] [CrossRef]
- Higgins, A.; Sharek, D.; Glacken, M. Building resilience in the face of adversity: Navigation processes used by older lesbian, gay, bisexual and transgender adults living in Ireland. J. Clin. Nurs. 2016, 25, 3652–3664. [Google Scholar] [CrossRef]
- The Swedish Discrimination Act [2008:567] 2023. Available online: https://www.do.se/choose-language/english/discrimination-act-2008567 (accessed on 7 April 2023).
- Tamaki, T. National Report: Japan. Am. Univ. J. Gend. Soc. Policy Law 2011, 19, 251–264. [Google Scholar]
- Mink, M.D.; Lindley, L.L.; Weinstein, A.A. Stress, Stigma, and Sexual Minority Status: The Intersectional Ecology Model of LGBTQ Health. J. Gay Lesbian Soc. Serv. 2014, 26, 502–521. [Google Scholar] [CrossRef]
- Marques, S.; Mariano, J.; Mendonça, J.; De Tavernier, W.; Hess, M.; Naegele, L.; Peixeiro, F.; Martins, D. Determinants of Ageism against Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2560. [Google Scholar] [CrossRef] [Green Version]
- Chang, E.S.; Kannoth, S.; Levy, S.; Wang, S.Y.; Lee, J.E.; Levy, B.R. Global reach of ageism on older persons’ health: A systematic review. PLoS ONE 2020, 15, e0220857. [Google Scholar] [CrossRef] [Green Version]
- Meyer, I.H. Minority Stress and Mental Health in Gay Men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef]
- Husa, J.; Nuotio, K.; Pihlajamaki, H. Nordic Law—Between Tradition and Dynamism. TICOM—Tilburg Inst Comp Transnatl Law Work Pap [Internet]. 1 October 2008. Available online: https://papers.ssrn.com/abstract=1287088 (accessed on 8 June 2023).
- McLelland, M. Japan’s Queer Cultures. In The Routledge Handbook of Japanese Culture and Society [Internet]. 2011, pp. 140–149. Available online: https://ro.uow.edu.au/artspapers/265 (accessed on 3 March 2023).
- Österberg, E. Den synliga och den osynliga synden: Sexualitet i norm och verklighet under 1600- och 1700-talen. Lambda Nord. 1996, 2, 58–70. [Google Scholar]
- Government Offices of Sweden. The Swedish Ministry of Employment; Government Offices of Sweden: Stockholm, Sweden, 2014.
- Tamagawa, M. Coming Out of the Closet in Japan: An Exploratory Sociological Study. J. GLBT Fam. Stud. 2018, 14, 488–518. [Google Scholar] [CrossRef] [Green Version]
- Flores, A. Social Acceptance of LGBTI People in 175 Countries and Locations [Internet]. Williams Institute. 2021. Available online: https://williamsinstitute.law.ucla.edu/publications/global-acceptance-index-lgbt/ (accessed on 5 June 2023).
- Act on the Prevention of Elder Abuse and Support for Caregivers of Elderly Persons [Internet]. The House of Representatives, Japan. 2005. Available online: https://www.japaneselawtranslation.go.jp/en/laws/view/3929/en (accessed on 15 March 2023).
- Bill for the Act on Promotion of Elimination of Discrimination on the Grounds of Sexual Orientation or Gender Identity [Internet]. The House of Representatives, Japan. 2016. Available online: https://www.shugiin.go.jp/internet/itdb_gian.nsf/html/gian/honbun/houan/g19001057.htm (accessed on 15 March 2023).
- The Constitution of Sweden. The Instrument of Government (1974:152) Up to and including Swedish Code of Statutes (SFS) 2018:1903; The Constitution of Sweden: Stockholm, Sweden, 2018.
- Sweden’s Legal Gender Recognition Act [Internet]. Regeringskansliet. 1972. Available online: https://tgeu.org/sweden-gender-recognition-act-reformed-2012/ (accessed on 7 April 2023).
- Riksmötet 2022/23. Regeringskansliet, 20230117. Available online: https://www.regeringen.se/contentassets/0e418b396c044cf39acb6daae9f33f10/propositionsforteckning-varen-2023.pdf (accessed on 7 April 2023).
- MHLW. Zenkoku Kaigo Hoken Koureisha Hoken Fukushi Tantoukachou Kaigisiryou (Meeting Materials of National Director of Long-Term Care Insurance and Elderly Health and Welfare); MHLW: Tokyo, Japan, 2023.
- Government Offices of Sweden. The Swedish National Board of Health and Welfare. The Old Swedish Criminal Code [number 167]. 1979. Available online: https://www.government.se/contentassets/7a2dcae0787e465e9a2431554b5eab03/the-swedish-criminal-code.pdf (accessed on 7 April 2023).
- The Swedish Homosexual Cohabitees Act. [1987:813]. Abolished 2003. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-1987813-om-homosexuella-sambor_sfs-1987-813 (accessed on 7 April 2023).
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, 160. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER Tool for Qualitative Evidence Synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, D.; Green, S.; Higgins, J.P. Defining the Review Question and Developing Criteria for Including Studies. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2008; pp. 81–94. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/9780470712184.ch5 (accessed on 31 October 2022).
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S.A. The well-built clinical question: A key to evidence-based decisions. ACP J. Club. 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Services S Beredning för Medicinsk Och Social Utvärdering (SBU); SA for HTA and A of S. SBU:s Metodbok [Internet]. 2020. Available online: https://www.sbu.se/sv/metod/sbus-metodbok/ (accessed on 3 March 2023).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Kitajima, H.; Sugisawa, H. Worries about Later Life among Sexual Minorities. J. Gerontoligical Res. 2018, 8, 51–66. [Google Scholar]
- Siverskog, A. Ageing Bodies that Matter: Age, Gender and Embodiment in Older Transgender People’s Life Stories. NORA—Nord. J. Fem. Gend. Res. 2015, 23, 4–19. [Google Scholar] [CrossRef]
- Siverskog, A.; Bromseth, J. Subcultural Spaces: LGBTQ Aging in a Swedish Context. Int. J. Aging Hum. Dev. 2019, 88, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Löf, J.; Olaison, A. ‘I don’t want to go back into the closet just because I need care’: Recognition of older LGBTQ adults in relation to future care needs. Eur. J. Soc. Work 2020, 23, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Nagai, S. Seikatsusha toshiteno mainoritei to sono koureiki. Sexual Minority as Living People and Their Old Age. Jpn J. Gerontol. 2019, 41, 48–53. (In Japanese) [Google Scholar]
- Fujita, K.; Matsunaga, H. Seiteki mainoritei koureisha no kadai to jisatsu taisaku (In Japanese), Sexual Minority Older Adults’ Issue and Prevention of their Suicide. Jpn. J. Geriatr. Psychiatry 2021, 32, 530–537. [Google Scholar]
- Kitajima, H. Infoumaru sapouto no kouchiku ni kankei suru sekushuaritei no eikyou: Gei·bai sekushuaru dannsei koureisha no katari kara. Sutudy on the Impact of Sexuality for building informal support: The Narrations by the Male Gay and Bisexual. Jpn. J. Gerontol. 2019, 41, 60–66. (In Japanese) [Google Scholar]
- Yamashita, N.; Shimizu, M. LGBT× kango gakusei × igakusei sei to sei to iryou no hanashi. LGBT× Nursing Students × Medical Students Talking about Sexuality and Medical care. Jpn. J. Nurs. Educ. 2015, 56, 188–194. (In Japanese) [Google Scholar]
- Kawano, Y. Sekushuaru mainoritei gairon. General Remarks of Sexual Minority. Jpn. J. Geriatr. Psychiatry 2021, 32, 505–511. (In Japanese) [Google Scholar]
- Mitsukashi, J. Souron: “Sei no tayousei” ha ikani sonchou sareru bekika: Kourei toransu gyenda no mentaru herusu wo megutte. How should we respect for “the Diverse of Sexuality”: Focus on transgender older Adults’ Mental Health. Jpn. J. Geriatr. Psychiatry 2021, 32, 518–524. (In Japanese) [Google Scholar]
- Tsuchiya-Ito, R.; Iwarsson, S.; Slaug, B. Environmental Challenges in the Home for Ageing Societies: A Comparison of Sweden and Japan. J. Cross-Cult. Gerontol. 2019, 34, 265–289. [Google Scholar] [CrossRef] [PubMed]
- Pikkarainen, H.; Brodin, B. Discrimination of the Sami: The Rights of the Sami from a Discrimination Perspective; Ombudsmannen mot etnisk diskriminering (DO): Stockholm, Sweden, 2008; p. 43. [Google Scholar]


{kind=link}
| Sample | Phenomenon of Interest | Design | Evaluation | Research Type |
|---|---|---|---|---|
| Japanese or Swedish | Quality of life, minority joy, resilience, discrimination, stigmatization, and minority stress | Focus groups, and interviews | Experiences, feelings, attitudes, perceptions, and views | Qualitative research |
| LGBTQ adults aged 60 years and above | Written in Japanese, Swedish, or English |
| Article no. | Title | Country | Context/Data Collection | Sample/Age | Phenomenon of Interest/Research Question(s) | Methodology/Analysis | Results | Quality | Included or Excluded | Specified Legal Prerequisites (Quality of Life and Discrimination) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. [31] | Turning vinegar into wine: Humorous self-presentations among older LGBTQ online daters | Sweden | Two web-based forums in Sweden were used for data collection. The first forum was directed at “homosexual, bisexual, queer and trans people along with their friends,” and the second at “homosexual and bisexual girls and women.” Data were collected using the automatic search functions of the forums. | n= 276; male, n= 162; female, n= 88; transgender, n = 26. Age: 60–81 years. | Whether self-mocking comments about old age and age-related topics confirm or subvert prevalent norms and images related to age and sexuality. | Quantitative content analysis. Data were sorted according to the profile contents, stated as attributes concerning personality, interests, body/appearance, education/career, comments on age, sexual content, nude photographs, and mentions of ethnicity as well as humor. The empirical analysis was divided into two sections: (1) self-mocking comments as a form of “age-salient maneuvering” related to existing age norms, and (2) self-mocking comments about old age, gray hair, wrinkles, being overweight, and impotence as a way of performing marketable characteristics, such as humor, self-distance, and honesty. | Themes: 1. Humorous comments on age-related issues. 2. Is humor subversive or conservative? 3. Self-mocking comments used as age-salient maneuvering. | High concerns | Not included. The analysis was not distinctive for the LGBTQ group, and the comments were not related to age concerns in general. | Insignificant concerns; legal prerequisites of minor importance. |
| 2. [29] | “They Just Don’t Have a Clue”: Transgender Aging and Implications for Social Work | Sweden | Recruitment via newspaper ads, snowball sampling, and an online LGBT community. The sample was collected from a larger project including 20 interviews with older LGBTQ people. | Transgender, n = 6 Age: 62–78 years. | How earlier life experiences matter in later life, and how age and (non-conforming) gender identities are understood in relation to one another. | Thematic analysis (Braun and Clarke, 2006). The participants were encouraged to talk freely about their lives, starting with when and where they were born. They were asked to follow-up from their stories, concerning their gender identities, social networks, relations, health, aging, and the body during different periods of their lives. | Themes: 1. Intersections of age and gender during the course of life. 2. The lack of knowledge on transgender issues within different contexts. 3. How previous experiences of accessing care and social services matter in later life and in relation to the future need for care. | High concerns. The analysis is unclear, only one researcher conducted the analysis, reflexivity and how the findings were validated are not described. | Included. The findings are relevant and there is a lack of studies in the field. | Insignificant concerns; relatively strong legal framework (discrimination). |
| 3. [71] | Ageing Bodies that Matter: Age, Gender and Embodiment in Older Transgender People’s Life Stories | Sweden | The same sample as in [29] the project in which six trans-identified persons were included in a sample of 20 older LGBTQ identified adults. | Transgender, n = 6 Age: 62–78 years. | How gender, age, and embodiment intersect in relation to trans identity, and what old age and aging mean for transgender people. | Thematic analysis (Braun and Clarke, 2006). | Themes: 1. Material bodies focus on the physical body: how it matters in the performance of (linear) gender and how it can fail in relation to the desire to “pass,” and how age and aging play into this experience. 2. Performing gender and age. Bodily aging can be perceived differently depending on bodily conditions and one’s ability and need to perform gender. | High concerns | Included | Insignificant concerns; relatively strong legal framework (discrimination). |
| 4. [72] | Subcultural Spaces: LGBTQ Aging in a Swedish Context | Sweden | The article includes two sub-studies: (1) an ethnographic study based on participant observation and 13 interviews; all participants lived in the Stockholm area and were involved in subcultural communities (lesbian feminist or LGBTQ) in different degrees and with various engagements. (2) the study described in [29,71], is based on interviews with 20 people identifying as LGBTQ. | Sample 1: Non-heterosexual cis and trans women, n = 13. Age: 60–94. Sample 2: LGBTQ, n = 20; trans, n = 6. Age: 64–88 years | Experiences of community among older LGBTQ people. The processes of finding, entering, and creating subcultural spaces. The influence of time and geographical context on these experiences. Aging within these communities? | Thematic analysis (Braun and Clarke, 2006). | 1. Coming in, coming home: finding spaces of belonging. 2. Spaces with friction: uncomfortable spaces. 3. Aging, bodies, and community: continuity and change. | High concerns. Recruitment and data collection were not clearly specified, concerns regarding analysis of the material, and standards of thematic analysis were not followed. | Included | Insignificant concerns; relatively strong legal framework (increased civil rights and discrimination. |
| 5. [73] | “I do not want to go back into the closet just because I need care”: recognition of older LGBTQ adults in relation to future care needs | Sweden | Participants were recruited via pensioners’ organizations; LGBTQ organizations, including those for older LGBTQ adults; one LGBT senior housing facility; and LGBT-certified retirement homes/home care services. Some were recruited through a Pride festival. In addition, a snowball sampling procedure was used. | n= 15, bisexual/lesbian women, n = 5; bisexual/gay men, n = 5; transgender, n = 5 Age: 65 years and older The interviewees lived in large and medium-sized cities in north and south Sweden. The interviewees lived at home and two of them had previous experience with elder care services. Three lived in an LGBT senior housing facility. | How older Swedish LGBTQ adults reason about openness in an elder care context concerning their future needs for services. | Thematic approach (Braun and Clarke, 2006). | Themes: 1. Openness and recognition 2. Preferences regarding how to be treated in elder care 3. LGBTQ housing | Insignificant concerns. Recruitment and analysis were clearly described; however, reflexivity was not discussed. | Included | Insignificant concerns. Concerns about the lack of considerations regarding the legal framework (the right of equal treatment, QOL, etc.) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bratt, A.S.; Hjelm, A.-C.P.; Wurm, M.; Huntley, R.; Hirakawa, Y.; Muraya, T. A Systematic Review of Qualitative Research Literature and a Thematic Synthesis of Older LGBTQ People’s Experiences of Quality of Life, Minority Joy, Resilience, Minority Stress, Discrimination, and Stigmatization in Japan and Sweden. Int. J. Environ. Res. Public Health 2023, 20, 6281. https://doi.org/10.3390/ijerph20136281
Bratt AS, Hjelm A-CP, Wurm M, Huntley R, Hirakawa Y, Muraya T. A Systematic Review of Qualitative Research Literature and a Thematic Synthesis of Older LGBTQ People’s Experiences of Quality of Life, Minority Joy, Resilience, Minority Stress, Discrimination, and Stigmatization in Japan and Sweden. International Journal of Environmental Research and Public Health. 2023; 20(13):6281. https://doi.org/10.3390/ijerph20136281
Chicago/Turabian StyleBratt, Anna Sofia, Ann-Christine Petersson Hjelm, Matilda Wurm, Richard Huntley, Yoshihisa Hirakawa, and Tsukasa Muraya. 2023. "A Systematic Review of Qualitative Research Literature and a Thematic Synthesis of Older LGBTQ People’s Experiences of Quality of Life, Minority Joy, Resilience, Minority Stress, Discrimination, and Stigmatization in Japan and Sweden" International Journal of Environmental Research and Public Health 20, no. 13: 6281. https://doi.org/10.3390/ijerph20136281
APA StyleBratt, A. S., Hjelm, A. -C. P., Wurm, M., Huntley, R., Hirakawa, Y., & Muraya, T. (2023). A Systematic Review of Qualitative Research Literature and a Thematic Synthesis of Older LGBTQ People’s Experiences of Quality of Life, Minority Joy, Resilience, Minority Stress, Discrimination, and Stigmatization in Japan and Sweden. International Journal of Environmental Research and Public Health, 20(13), 6281. https://doi.org/10.3390/ijerph20136281