

The Feasibility of Make My Day—A Randomized Controlled Pilot Trial of a Stroke Prevention Program in Primary Healthcare
Abstract
:1. Introduction
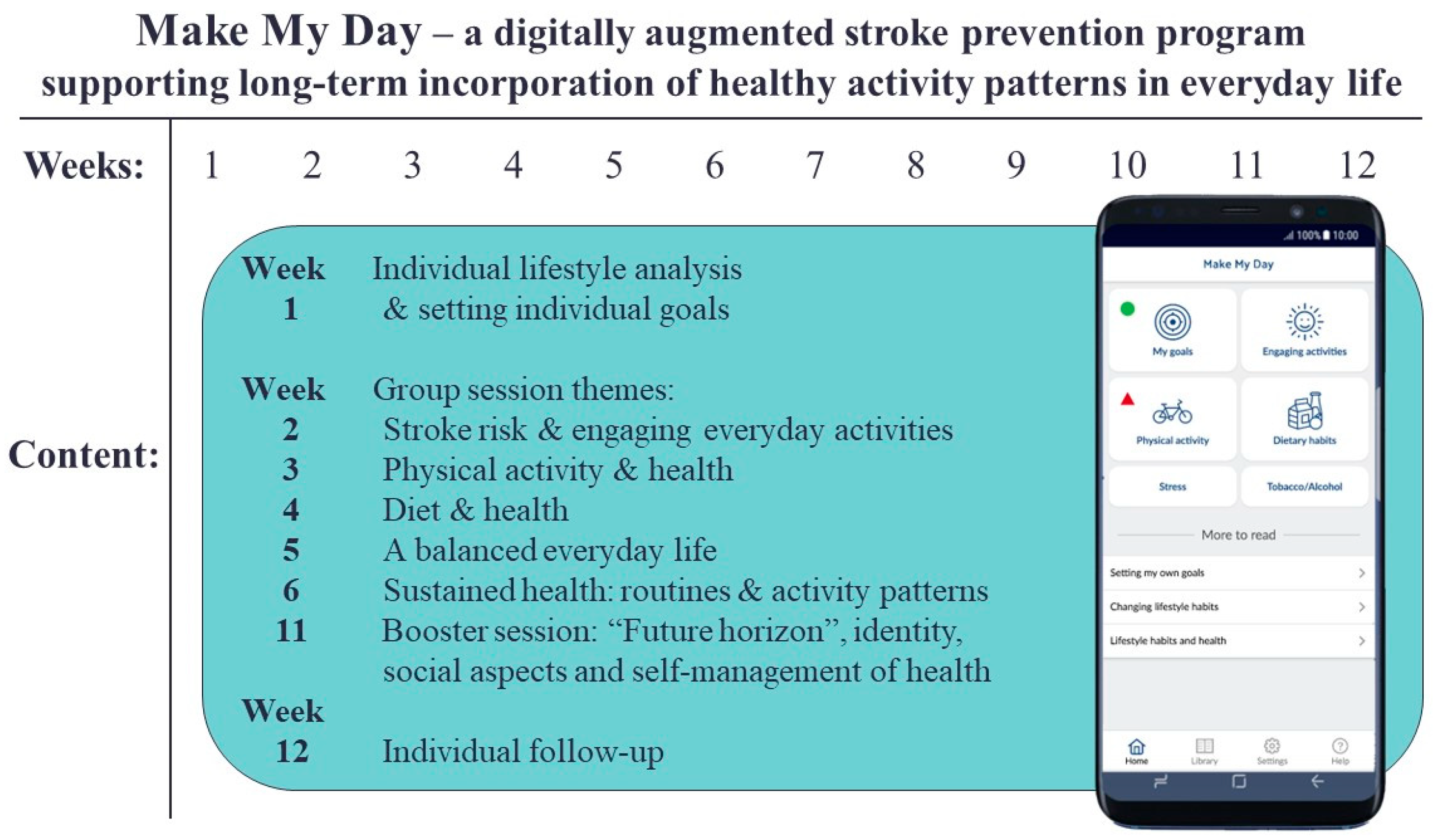
The Make My Day Intervention
- (1)
- the success of recruitment and retention procedures;
- (2)
- the acceptability and suitability of the instruments and response rates;
- (3)
- adherence to the MMD pilot trial and prevention program;
- (4)
- sensitivity to change in the outcome measures.
2. Materials and Methods
2.1. Study Design
2.2. Recruitment of Persons at Risk for Stroke
2.3. Randomization
2.4. Intervention Group: Make My Day
2.5. Control Group
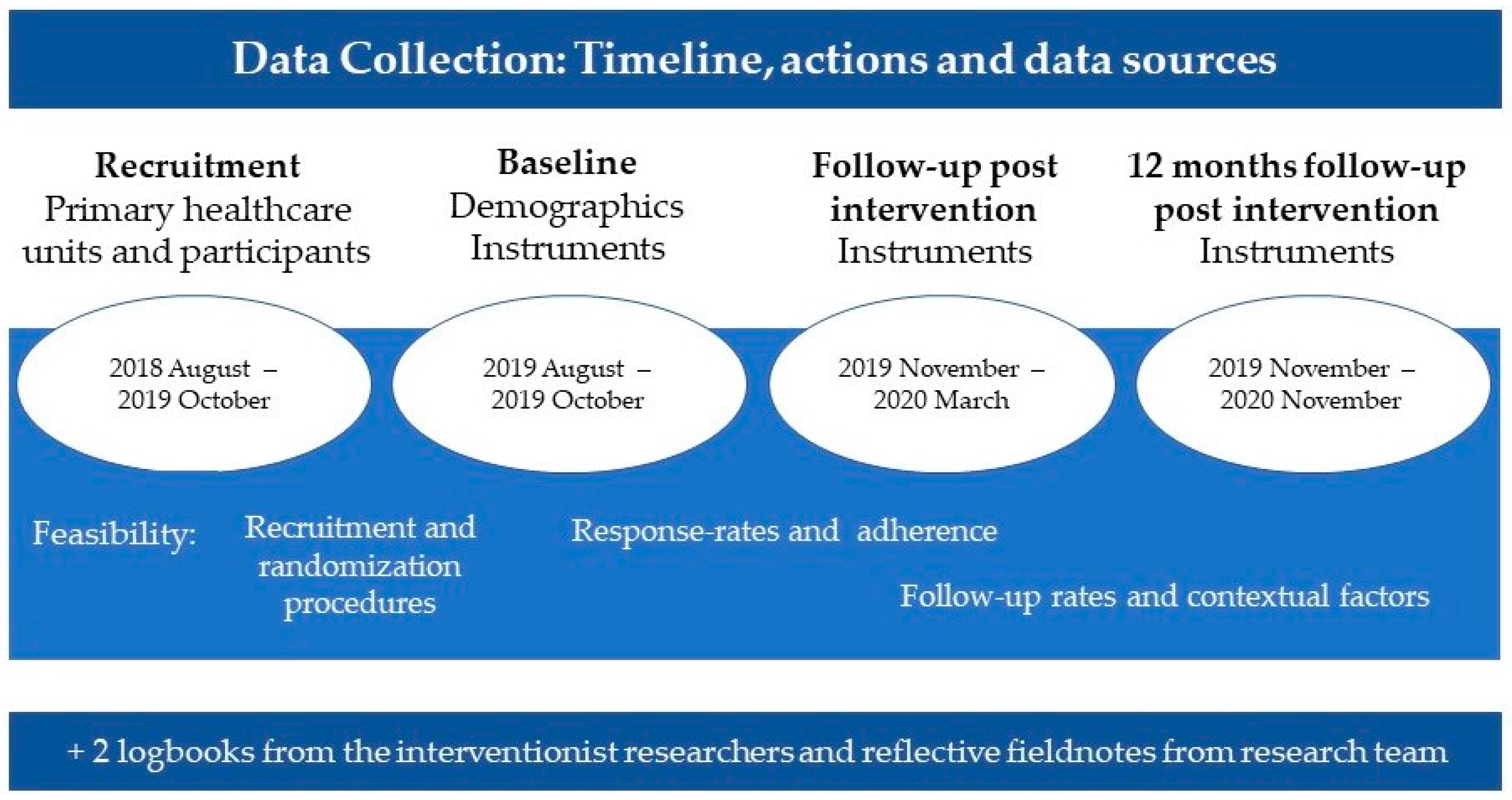
2.6. Data Collection
2.7. Outcome Measurements
2.7.1. Overall Stroke Risk
2.7.2. Individual Risk Factors for Stroke
2.7.3. Physical Performance
2.7.4. Activity Performance
2.7.5. Healthy Activity Patterns
2.7.6. Participation in Health-Promoting Activities
2.7.7. Activity Balance
2.7.8. Stroke Risk Literacy
2.7.9. Quality of Life
2.8. Data Analysis
2.9. Ethical Considerations
3. Results
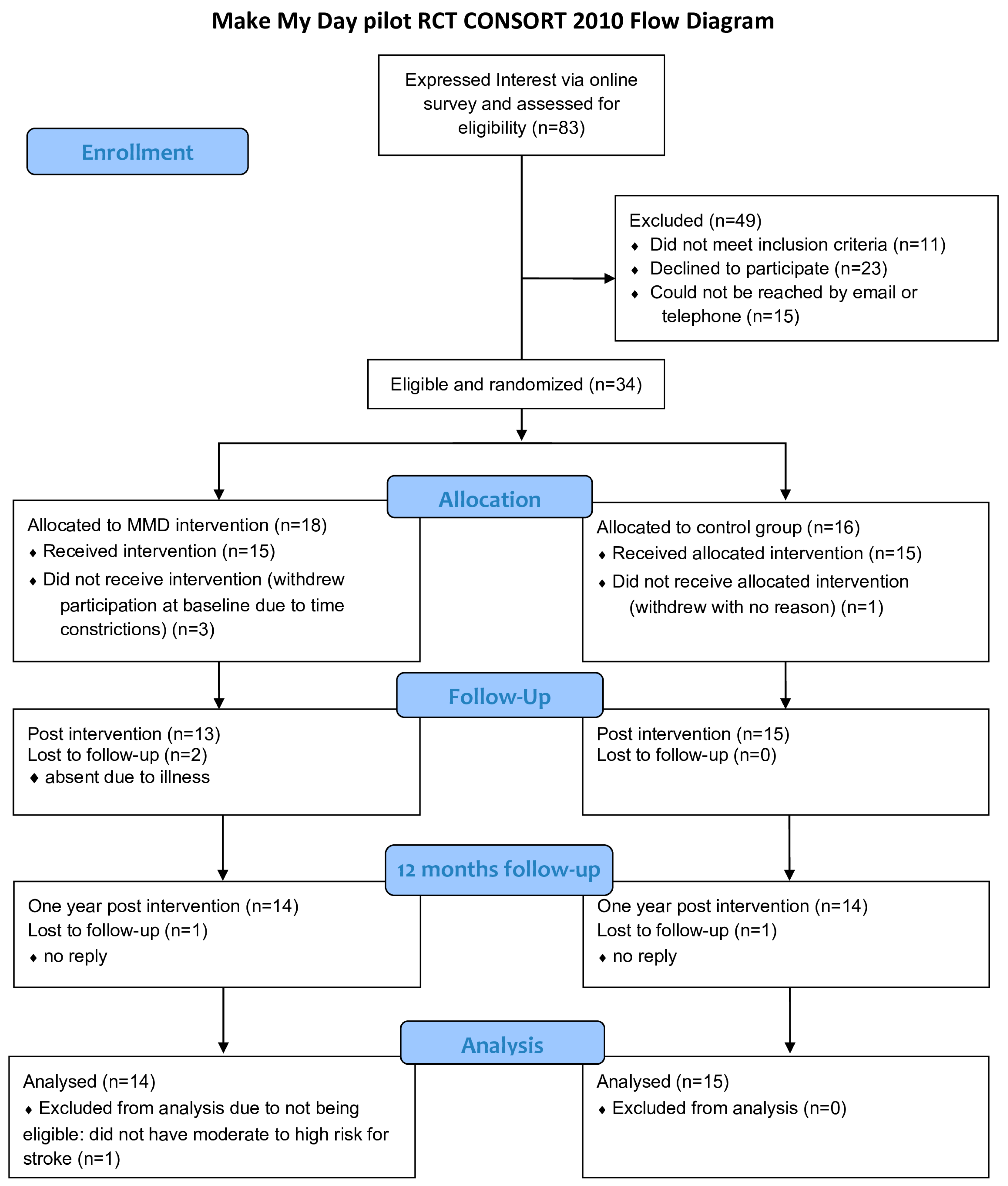
3.1. Participant Recruitment and Baseline Characteristics
3.2. Acceptability and Suitability of Instruments and Response Rates
3.3. Adherence
3.4. Outcome Measurements
3.4.1. Overall Stroke Risk
3.4.2. Individual Cardiometabolic and Lifestyle Risk Factors
3.4.3. Stroke Risk Literacy
3.4.4. Activity Performance
3.4.5. Time Use and Experience of Health in Everyday Activities
3.4.6. Participation in Health-Promoting Activities
3.4.7. Activity Balance
3.4.8. Quality of Life
3.4.9. Physical Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patomella, A.-H.; Guidetti, S.; Mälstam, E.; Eriksson, C.; Bergström, A.; Åkesson, E.; Kottorp, A.; Asaba, E. Primary prevention of stroke: Randomised controlled pilot trial protocol on engaging everyday activities promoting health. BMJ Open 2019, 9, e031984. [Google Scholar] [CrossRef]
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Rienks, J.; Nöthlings, U. Lifestyle Indices and Cardiovascular Disease Risk: A Meta-analysis. Am. J. Prev. Med. 2018, 55, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Short, S.E.; Mollborn, S. Social determinants and health behaviors: Conceptual frames and empirical advances. Curr. Opin. Psychol. 2015, 5, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.; Carlson, M.; Mandel, D.; Zemke, R.; Clark, F. Occupation in Lifestyle Redesign: The Well Elderly Study Occupational Therapy Program. Am. J. Occup. Ther. 1998, 52, 326–336. [Google Scholar] [CrossRef]
- Mälstam, E.; Asaba, E.; Åkesson, E.; Guidetti, S.; Patomella, A.-H. ‘Weaving lifestyle habits’: Complex pathways to health for persons at risk for stroke. Scand. J. Occup. Ther. 2022, 29, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Pandian, J.D.; Gall, S.L.; Kate, M.P.; Silva, G.S.; Akinyemi, R.O.; Ovbiagele, B.I.; Lavados, P.M.; Gandhi, D.B.C.; Thrift, A.G. Prevention of stroke: A global perspective. Lancet 2018, 392, 1269–1278. [Google Scholar] [CrossRef]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Feigin, V.L. Primary stroke prevention needs overhaul. Int. J. Stroke 2017, 12, 5–6. [Google Scholar] [CrossRef]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Towfighi, A.; Markovic, D.; Ovbiagele, B. Impact of a healthy lifestyle on all-cause and cardiovascular mortality after stroke in the USA. J. Neurol. Neurosurg. Psychiatry 2012, 83, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Åkesson, A.; Wolk, A. Primary prevention of stroke by a healthy lifestyle in a high-risk group. Neurology 2015, 84, 2224–2228. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Myers, J.; Kokkinos, P. Importance of lifestyle modification on cardiovascular risk reduction: Counseling strategies to maximize patient outcomes. J. Cardiopulm. Rehabil. Prev. 2020, 40, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Clark, F.; Azen, S.P.; Zemke, R.; Jackson, J.; Carlson, M.; Mandel, D.; Hay, J.; Josephson, K.; Cherry, B.; Hessel, C.; et al. Occupational Therapy for Independent-Living Older Adults. JAMA 1997, 278, 1321–1326. [Google Scholar] [CrossRef]
- Clark, F.; Jackson, J.; Carlson, M.; Chou, C.-P.; Cherry, B.J.; Jordan-Marsh, M.; Knight, B.G.; Mandel, D.; Blanchard, J.; Granger, D.A.; et al. Effectiveness of a lifestyle intervention in promoting the well-being of independently living older people: Results of the Well Elderly 2 Randomised Controlled Trial. J. Epidemiol. Community Health 2012, 66, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.; Bigari, K.; Culler, T.; Gregory, H.; Hamilton, J.; Krawczyk, S.; Earley, D.; Herlache, E. Healthy lifestyles through an Adaptive Living Program: A pilot study. Occup. Ther. Int. 2008, 15, 269–283. [Google Scholar] [CrossRef]
- Levasseur, M.; Filiatrault, J.; Larivière, N.; Trépanier, J.; Lévesque, M.H.; Beaudry, M.; Parisien, M.; Provencher, V.; Couturier, Y.; Champoux, N.; et al. Influence of Lifestyle RedesignVR on health, social participation, leisure, and mobility of older French-Canadians. Am. J. Occup. Ther. 2019, 73, 7305205030p1–7305205030p18. [Google Scholar] [CrossRef]
- Tsai, A.Y.; Sun, T.-S.; Chen, M.-D.; Kuo, C.-C.; Su, P.-C.; Chou, Y.-C. The Effectiveness of Short-Term Lifestyle Intervention Programs on Physical Function, Cognition, and Quality of Life Among Community Older Adults: A Pilot Study. Top. Geriatr. Rehabil. 2022, 38, 158–164. [Google Scholar] [CrossRef]
- Kuo, C.-C.; Shyu, H.-J.B.; Park, D.; Tsai, P.-C.; Li, Y.-H. Effects of a Physically Active Lifestyle Modification (PALM) Program for Independent Taiwanese Older Adults: A Mixed-Methods Pilot Study. Top. Geriatr. Rehabil. 2022, 38, 149–157. [Google Scholar] [CrossRef]
- Ng, S.S.; Chan, D.Y.; Chan, M.K.; Chow, K.K. Long-term efficacy of occupational lifestyle redesign programme for stroke. Hong Kong J. Occup. Ther. 2013, 23, 46–53. [Google Scholar] [CrossRef]
- Pyatak, E.; King, M.; Vigen, C.L.; Salazar, E.; Diaz, J.; Schepens Niemiec, S.L.; Blanchard, J.; Jordan, K.; Banerjee, J.; Shukla, J. Addressing diabetes in primary care: Hybrid effectiveness–implementation study of Lifestyle Redesign® occupational therapy. Am. J. Occup. Ther. 2019, 73, 7305185020p1–7305185020p12. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, H. A new direction in the conceptualization and categorization of occupation. J. Occup. Sci. 2008, 15, 3–8. [Google Scholar] [CrossRef]
- Asaba, E.; Bergström, A.; Patomella, A.-H.; Guidetti, S. Engaging occupations among persons at risk for stroke: A health paradox. Scand. J. Occup. Ther. 2022, 29, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; Mills, J. Canadian Occupational Performance Measure; CAOT Publications: Toronto, ON, Canada, 1991. [Google Scholar]
- Patomella, A.-H.; Farias, L.; Eriksson, C.; Guidetti, S.; Asaba, E. Engagement in Everyday Activities for Prevention of Stroke: Feasibility of an mHealth-Supported Program for People with TIA. Healthcare 2021, 9, 968. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Skivington, K.; Matthews, L.; Simpson, S.; Craig, P.; Baird, J.; Blazeby, J.; Boyd, K.; Craig, N.; French, D.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; George, M.G.; Foltz, J.L.; Roth, G.A.; Mensah, G.A. Prevention of stroke: A strategic global imperative. Nat. Rev. Neurol. 2016, 12, 501–512. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- Mälstam, E.; Patomella, A.-H.; Asaba, E. Incorporating new ways of doing by learning from everyday experiences and interactions using a multifactorial mHealth app. Digit. Health 2023, 9, 20552076221149293. [Google Scholar] [CrossRef]
- Alzahrani, F.A.; Alenzy, A.E.; Alghamdi, A.M. Stroke in Tabuk, KSA: Awareness and prevalence of risk factors. Life Sci. J. 2019, 16, 38–42. [Google Scholar]
- Enright, P. The Six-Minute Walk Test. Respir. Care 2003, 48, 783–785. [Google Scholar] [PubMed]
- Atler, K.E.; Eakman, A.; Orsi, B. Enhancing construct validity evidence of the Daily Experiences of Pleasure, Productivity and Restoration Profile. J. Occup. Sci. 2015, 23, 278–290. [Google Scholar] [CrossRef]
- Wagman, P.; Håkansson, C. Introducing the Occupational Balance Questionnaire (OBQ). Scand. J. Occup. Ther. 2014, 21, 227–231. [Google Scholar] [CrossRef]
- Dearborn, J.L.; McCullough, L.D. Perception of Risk and Knowledge of Risk Factors in Women at High Risk for Stroke. Stroke 2009, 40, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- EuroQol Research Foundation. User GuideEQ-5D-3L User Guide. 2018, pp. 1–33. Available online: https://euroqol.org/publications/user-guides/ (accessed on 1 June 2023).
- Fugl-Meyer, A.R.; Bränholm, I.-B.; Fugl-Meyer, K.S. Happiness and domain-specific life satisfaction in adult northern Swedes. Clin. Rehabil. 1991, 5, 25–33. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Mahfoud, F.; Weber, M.A.; Townsend, R.; Parati, G.; Fisher, N.D.; Lobo, M.D.; Bloch, M.; Böhm, M.; Sharp, A.S.; et al. Clinical Trial Design Principle and Outcome Definitions for Device-Based Therapies for Hypertension: A Consensus Document From the Hypertension Academic Research Constortium. Circulation 2022, 145, 847–863. [Google Scholar] [CrossRef]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and me-ta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef]
- The Swedish National Board of Health and Welfare (Socialstyrelsen). Questions of Lifestyle Habits. 2018. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/dokument-webb/nationella-riktlinjer/levnadsvanor-fragor-om-levnadsvanor.pdf (accessed on 9 January 2023).
- Swedish National Board of Housing, Building and Planning (Boverket). Classification of Housing Areas. Available online: https://segregationsbarometern.boverket.se/labbet/#/omradesstatistik/map?indicator=0-1,2,3,4,5&location=riket&bg=0 (accessed on 13 March 2023).
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 25 May 2023).
- Norden. Nordic Nutrition Recommendations—Integrating Nutrition and Physical Activity. 2012. Available online: http://norden.diva-portal.org/smash/get/diva2:745780/FULLTEXT01.pdf (accessed on 25 May 2023).
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar]
- McDonald, A.M.; Knight, R.C.; Campbell, M.K.; Entwistle, V.A.; Grant, A.M.; Cook, J.A.; Elbourne, D.R.; Francis, D.; Garcia, J.; Roberts, I.; et al. What influences recruitment to randomised controlled trials? A review of trials funded by two UK funding agencies. Trials 2006, 7, 9. [Google Scholar] [CrossRef]
- Treweek, S.; Mitchell, E.; Pitkethly, M.; Cook, J.; Kjeldstrøm, M.; Johansen, M.; Taskila, T.K.; Sullivan, F.; Wilson, S.; Jackson, C.; et al. Strategies to improve recruitment to randomised trials. Cochrane Database Syst. Rev. 2018, 2, MR000013. [Google Scholar] [CrossRef] [PubMed]
- Tsaltskan, V.; Nguyen, K.; Eaglin, C.; Holers, V.M.; Deane, K.D.; Firestein, G.S. Comparison of Web-Based Advertising and a Social Media Platform as Recruitment Tools for Underserved and Hard-to-Reach Populations in Rheumatology Clinical Research. ACR Open Rheumatol. 2022, 4, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Blukacz, A.; Cabieses, B.; Obach, A.; Calderón, A.C.; Álvarez, M.I.; Madrid, P.; Rada, I. Promoting the Participation of “Hard-to-Reach” Migrant Populations in Qualitative Public Health Research during the COVID-19 Pandemic in Chile. Int. J. Environ. Res. Public Health 2023, 20, 1956. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, D.A.; Vargas, E.; Kamsickas, L.; Carnethon, M. The role of behavioral science in addressing cardiovascular health disparities: A narrative review of efforts, challenges, and future directions. Heal. Psychol. 2022, 41, 740–754. [Google Scholar] [CrossRef] [PubMed]
- Raifman, S.; DeVost, M.A.; Digitale, J.C.; Chen, Y.H.; Morris, M.D. Respondent-Driven Sampling: A Sampling Method for Hard-to-Reach Populations and Beyond. Curr. Epidemiol. Rep. 2022, 9, 38–47. [Google Scholar] [CrossRef]
- Prince, S.; Cardilli, L.; Reed, J.L.; Saunders, T.J.; Kite, C.; Douillette, K.; Fournier, K.; Buckley, J.P. A comparison of self-reported and device measured sedentary behavior in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Signore, A.K.; Jung, M.E.; Semenchuk, B.; Kullman, S.M.; Tefft, O.; Webber, S.; Ferguson, L.J.; Kowalski, K.; Fortier, M.; McGavock, J.; et al. A pilot and feasibility study of a randomized clinical trial testing a self-compassion intervention aimed to increase physical activity behaviour among people with prediabetes. BMC Pilot Feasibility Stud. 2022, 8, 111. [Google Scholar] [CrossRef]
- American Heart Association. Available online: https://www.stroke.org/en/about-stroke/stroke-risk-factors/stroke-risk-assessment (accessed on 19 May 2023).
- Medvedev, O.; Truong, Q.C.; Merkin, A.; Borotkanics, R.; Krishnamurthi, R.; Feigin, V. Cross-cultural validation of the stroke riskometer using generalizability theory. Sci. Rep. 2021, 11, 19064. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological Momentary Assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Outcome | Instrument | Purpose | Measure |
|---|---|---|---|
| Stroke risk | Stroke Risk Score Card (SRSC) [33] | Overall stroke risk combining modifiable and non-modifiable risk factors | 8 domains with three categories each. Total score, summing up each category: ≥3 = High Stroke Risk, 4–6 = Caution, 6–8 = Low Stroke Risk |
| Anthropometric measures | Body Mass Index (BMI) | Indicator for body fat and weight status | <18.5 = Underweight, 18.5–24.9 = Normal, 25.0–29.9 = Overweight, >30.0 = Obesity |
| Blood pressure (BP) [40,41] | Measurement of systolic and diastolic blood pressure | High blood pressure: >140/90, Elevated blood pressure: 120–139/80–89, Normal blood pressure: <120/80. A decrease of 10 mm Hg in systolic blood pressure and 5 mm Hg in diastolic blood pressure was considered a clinically meaningful change. | |
| Lifestyle habits | Lifestyle habit survey [42]. | Estimation of lifestyle habits in everyday life: tobacco use, alcohol consumption, physical activity, and eating habits. | Four habits with 11 questions in total, subdivided into 4–5 levels of performance during a week or the last months. For example, “how often do you eat fruit or berries?” 1 = Two times each day or more 2 = One’s a day 3 = A couple of times during a week 4 = One time, or less, during a week. |
| Physical performance | 6 min walk test (6MWT) [34] | Physical performance while walking 6 min. | Measurements before and after 6 min walk between a marking of 30 m: distance in meters, saturation (SpO2), pulse (beat/minute), blood pressure (mm Hg systolic and diastolic), and estimating shortness of breath and leg fatigue with Borg Scale (1–10). |
| Activity performance and satisfaction | Canadian Occupational Performance Measure (COPM) [24]. | Perceived performance and satisfaction with activities in everyday life. | Scale ranging from 1 to 10 in two aspects: (i) current performance, 1 = not able to perform the activity at all to 10 = able to do it extremely well, and (ii) satisfaction with doing, 1 = not satisfied to 10 = extremely satisfied. |
| Activity patterns | The Daily Experiences of Pleasure, Productivity and Restoration Profile (PPRP) [35]. | Perceived pleasure, productivity, and restoration during three days (two week days and one weekend day). | Time as measured in hours. Scale of 1–7 in four dimensions (pleasure, productivity, restoration and health) related to the time use. For example: 1 = Extreme displeasure 2 = Moderate displeasure 3 = A little displeasure 4 = Neither pleasure nor displeasure 5 = Moderate pleasure 6 = Extreme pleasure. |
| Participation in health-promoting activities | PHPA questionnaire | Perceived participation in activities in everyday life that can increase or decrease health. | 10 statements with 5 levels of agreement: 1 = No, do not participate, 2: Sometimes (less than once a week), 3 = Often (up to twice a week), 4 = regularly (three or more times a week), 5 = Daily. |
| Perception of balance in everyday life | Occupational Balance Questionnaire (OBQ) [36] | Perception of balance within or between different occupations in everyday life. | 13 statements with 4 level of agreements: 0 = Do not agree at all 1 = Agree partially 2 = Agree a lot 3 = Totally agree, with a sum ranging from 0–39. |
| Stroke risk literacy | Items from a stroke risk knowledge and awareness of stroke risk questionnaire [37] | Three questions indicating literacy of stroke risks, stroke risks that can be impacted by modifiable means, and scoring of one’s one stroke risk. | Counting of stroke risk factors were counted from 1–7, and the scoring of own risk by 1–10. |
| Quality of life | EQ-5D-3L Questionnaire [38] | General life quality. Perceived state of health in five aspects: mobility, hygiene, main activities, pain, and anxiety. | Index scale from 0 to 1, based on scores from 1 to 3, subdivided into three levels of severity: 1 = no problem, 2 = some/moderate problems, 3 = extreme problems. |
| EQ-Visual Analogue [38] Scale (EQ-VAS) | Perceived state of health. | Scale 0–100: 0 = worst possible health, 100 = best possible health. | |
| Life Satisfaction | Life Satisfaction Scale11 (LiSat-11) [39] | Perceived satisfaction with life | Scale 1–6: 1 = not satisfied to 6 = very satisfied |
| Variables | Intervention Group n = 14 | Control Group n = 15 |
|---|---|---|
| Age, Mean (SD) | 61.9 (8.5) | 59.7 (7.5) |
| Education, Mean (SD) | 13.5 (1.8) | 13.7 (1.9) |
| Sex, Female | 8 (57) | 12 (80) |
| Country of birth country, Sweden | 9 (64) | 11 (73) |
| Living situation Alone | 8 (57) | 7 (47) |
| Together | 6 (43) | 8 (53) |
| Area of housing/living a Good socioeconomic conditions | 11 (79) | 13 (87) |
| Socioeconomic challenges | 3 (21) | 2 (13) |
| Work status Working | 6 (43) | 8 (53) |
| Not working b | 8 (57) | 7 (47) |
| Yearly income, in euro >58,000 | 3 (21) | 1 (7) |
| <58,000 >19,300 | 10 (72) | 11 (73) |
| <19,300 | 1 (7) | 3 (20) |
| mHealth technology use Interest | 13 (93) | 15 (100) |
| Skills c | 9 (64) | 15 (100) |
| Overall stroke risk d High risk | 9 (64) | 6 (40) |
| Caution | 5 (36) | 9 (60) |
| Modifiable risk factors Atrial fibrillation e | 1 (7) | 1 (7) |
| Diabetes type 2 or borderline | 5 (36) | 6 (40) |
| High or elevated blood pressure | 11 (79) | 9 (60) |
| Smoking | 4 (29) | 0 (0) |
| Overweight f | 7 (50) | 9 (60) |
| Insufficient physical exercise g | 10 (71) | 14 (93) |
| Insufficient physical activity h | 7 (50) | 9 (60) |
| Insufficient vegetable consumption i | 5 (36) | 8 (53) |
| Insufficient fruit and berry consumption i | 4 (29) | 8 (53) |
| Limited weekly snack consumption j | 0 (0) | 3 (20) |
| Recurring stress in everyday life k | 10 (71) | 12 (80) |
| Stroke Risk | Intervention Group n = 14 | Control Group n = 15 | |
|---|---|---|---|
| Baseline | High risk | 9 | 6 |
| Caution | 5 | 9 | |
| Follow up | High risk | 5 b | 5 a |
| Caution | 4 a | 8 a | |
| Low risk | 2 | 1 | |
| 12 months | High risk | 5 a | 9 |
| Caution | 7 a | 4 a | |
| Low risk | 0 | 1 |
| Measures | Baseline | 1st Follow up | 12-Month Follow-up | Mean Difference from 1st Follow-up | Mean Difference from 2nd Follow-up | Clinical Cut off Score |
|---|---|---|---|---|---|---|
| Intervention group | ||||||
| SBP ↓ | 141 | 130 | 131 | −11 * | −10 * | 10 |
| DBP ↓ | 93 | 85 | 85 | 8 | 8 | 5 |
| COPM (1–10) ↑ | 4.1 | 6.6 | 5.8 | 2.6 * | 1.7 | >2 |
| EQ-VAS (1–100) ↑ | 65 | 75 | 74 | 10 * | 9 | >10 |
| Control group | ||||||
| SBP ↓ | 131 | 129 | 127 | −2 | −3 | 10 |
| DBP ↓ | 85 | 87 | 83 | +2 | −2 | 5 |
| COPM (1–10) ↑ | 3.8 | 5.4 | 5.8 | 1.6 | 1.9 | >2 |
| EQ-VAS (1–100) ↑ | 63 | 65 | 72 | 2 | 9 | >10 |
| Measures | Intervention Group | Control Group | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline to Follow-up | Baseline to 12 Months | Baseline to Follow-up | Baseline to 12 Months | |||||
| n = 14 | p-Value | n = 14 | p-Value | n = 15 | p-Value | n = 15 | p-Value | |
| COPM (1–10) Median (IQR) | 2.5 (2.7) b | 0.050 * | 1.8 (2.3) a | 0.008 * | 1.0 (2.5) b | 0.002 * | 1.6 (3.8) a | 0.004 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mälstam, E.; Asaba, E.; Åkesson, E.; Guidetti, S.; Patomella, A.-H. The Feasibility of Make My Day—A Randomized Controlled Pilot Trial of a Stroke Prevention Program in Primary Healthcare. Int. J. Environ. Res. Public Health 2023, 20, 6828. https://doi.org/10.3390/ijerph20196828
Mälstam E, Asaba E, Åkesson E, Guidetti S, Patomella A-H. The Feasibility of Make My Day—A Randomized Controlled Pilot Trial of a Stroke Prevention Program in Primary Healthcare. International Journal of Environmental Research and Public Health. 2023; 20(19):6828. https://doi.org/10.3390/ijerph20196828
Chicago/Turabian StyleMälstam, Emelie, Eric Asaba, Elisabet Åkesson, Susanne Guidetti, and Ann-Helen Patomella. 2023. "The Feasibility of Make My Day—A Randomized Controlled Pilot Trial of a Stroke Prevention Program in Primary Healthcare" International Journal of Environmental Research and Public Health 20, no. 19: 6828. https://doi.org/10.3390/ijerph20196828
APA StyleMälstam, E., Asaba, E., Åkesson, E., Guidetti, S., & Patomella, A. -H. (2023). The Feasibility of Make My Day—A Randomized Controlled Pilot Trial of a Stroke Prevention Program in Primary Healthcare. International Journal of Environmental Research and Public Health, 20(19), 6828. https://doi.org/10.3390/ijerph20196828