
Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review

 ,
,  ,
,  , , , , ,
, , , , ,  ,
,  , ,
, ,  ,
, 
 ,
,  ,
,  , ,
, ,  ,
,  ,
,  and
and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
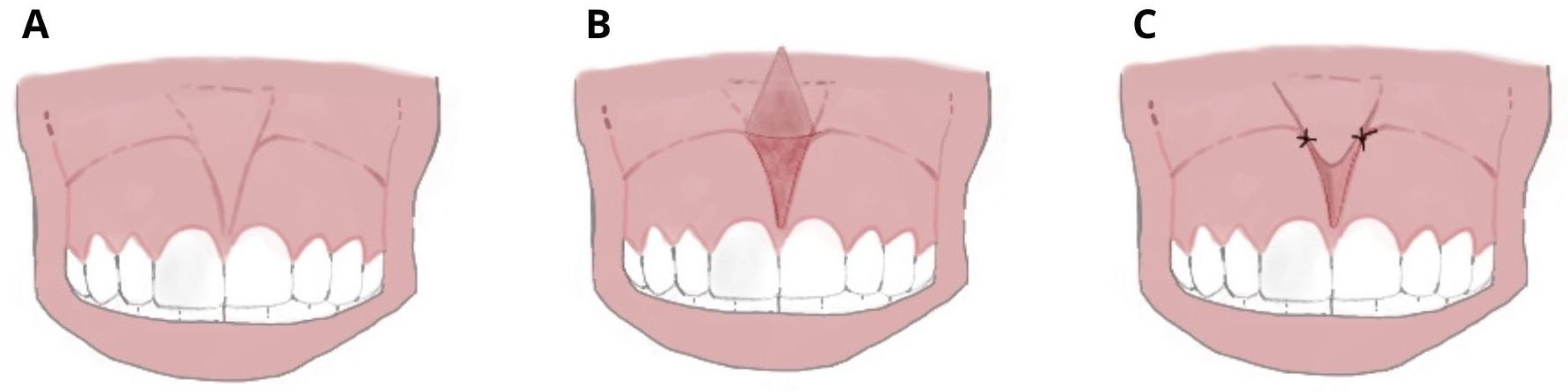
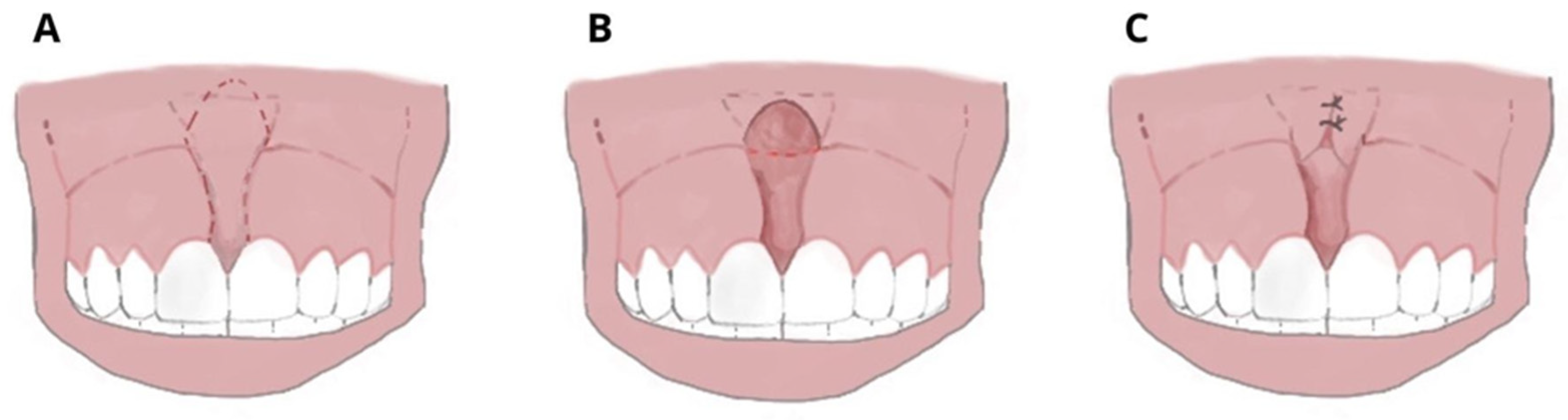
1.1. Conventional Surgery
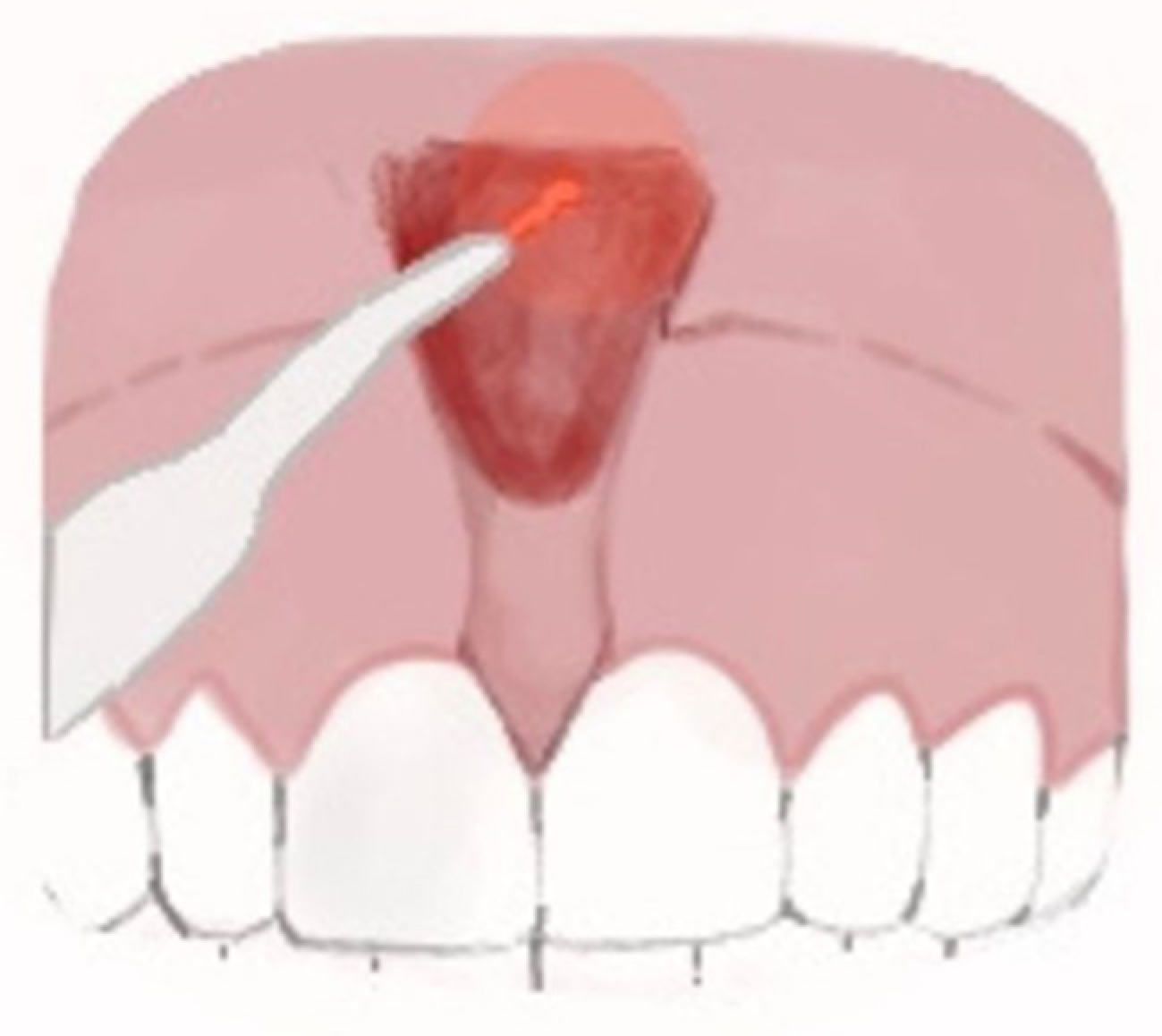
1.2. Laser Surgery
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection
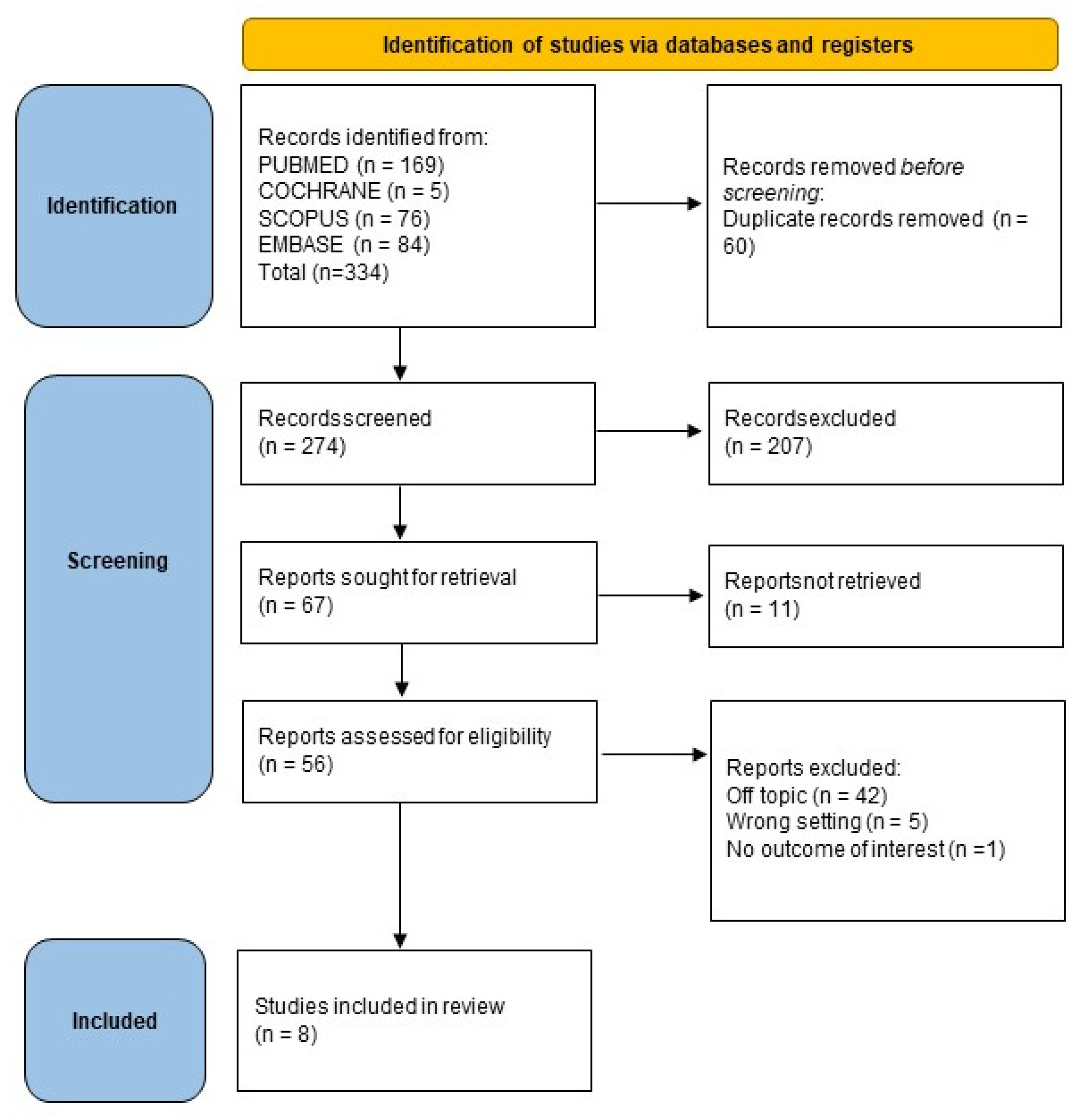
3. Results
Study Selection and Included Study Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CO2 | Carbon dioxide laser |
| Er,Cr:YSGG | Erbium chromium yttrium scandium gallium-garnet laser |
| Er:YAG | Erbium-doped yttrium aluminum garnet laser |
| KTP | Potassium titanyl phosphate laser |
| Nd:YAG | Neodymium-doped yttrium aluminum garnet laser |
| ULF | Upper labial frenulum |
References
- Miotti, A.; Frezza, F.; Favero, G.; Cecchetto, A. Histologic characteristics of the upper labial frenum in individuals with middle interincisor diastema. Mondo Odontostomatol. 1979, 21, 22–25. [Google Scholar] [PubMed]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an Oral Appliance in Patients with Mild to Moderate Obstructive Sleep Apnea Syndrome Intolerant to Continuous Positive Airway Pressure Use: Preliminary Results. Int. J. Immunopathol. Pharm. 2016, 29, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Lorusso, F.; Inchingolo, F.; Postiglione, F.; Petrini, M. The Effects of Erbium-Doped Yttrium Aluminum Garnet Laser (Er: YAG) Irradiation on Sandblasted and Acid-Etched (SLA) Titanium, an In Vitro Study. Materials 2020, 13, 4174. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef]
- Mirko, P.; Miroslav, S.; Lubor, M. Significance of the Labial Frenum Attachment in Periodontal Disease in Man. Part I. Classification and Epidemiology of the Labial Frenum Attachment. J. Periodontol. 1974, 45, 891–894. [Google Scholar] [CrossRef]
- Kramer, P.F.; de Amorim, L.M.; de Moura Alves, N.; Ruschel, H.C.; Bervian, J.; Feldens, C.A. Maxillary Labial Frenum in Preschool Children: Variations, Anomalies and Associated Factors. J. Clin. Pediatr. Dent. 2022, 46, 51–57. [Google Scholar] [CrossRef]
- Popovich, F.; Thompson, G.W.; Main, P.A. The Maxillary Interincisal Diastema and Its Relationship to the Superior Labial Frenum and Intermaxillary Suture. Angle Orthod. 1977, 47, 265–271. [Google Scholar] [CrossRef]
- Komori, S.; Matsumoto, K.; Matsuo, K.; Suzuki, H.; Komori, T. Clinical Study of Laser Treatment for Frenectomy of Pediatric Patients. Int. J. Clin. Pediatr. Dent. 2017, 10, 272–277. [Google Scholar] [CrossRef]
- Delli, K.; Livas, C.; Sculean, A.; Katsaros, C.; Bornstein, M.M. Facts and Myths Regarding the Maxillary Midline Frenum and Its Treatment: A Systematic Review of the Literature. Quintessence Int. 2013, 44, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Malcangi, G.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; De Leonardis, N.; et al. Benefits and Implications of Resveratrol Supplementation on Microbiota Modulations: A Systematic Review of the Literature. Int. J. Mol. Sci. 2022, 23, 4027. [Google Scholar] [CrossRef]
- Ceratti, C.; Maspero, C.; Consonni, D.; Caprioglio, A.; Connelly, S.T.; Inchingolo, F.; Tartaglia, G.M. Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients. Bioengineering 2022, 9, 102. [Google Scholar] [CrossRef]
- Devishree; Gujjari, S.K.; Shubhashini, P.V. Frenectomy: A Review with the Reports of Surgical Techniques. J. Clin. Diagn. Res. 2012, 6, 1587–1592. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ceci, S.; Limongelli, L.; Corriero, A.; Curatoli, L.; Azzollini, D.; Mezzapesa, P.P.; Marinelli, G.; Malcangi, G.; Coloccia, G.; et al. Cavernous Sinus Involvement and Near Miss Mediastinitis Following Mandibular Tooth Infection Treated during the COVID-19 Pandemic: Clinical Diagnosis and Treatment. Case Rep. Dent. 2022, 2022, 8650099. [Google Scholar] [CrossRef]
- Miller, P.D. The Frenectomy Combined with a Laterally Positioned Pedicle Graft. Functional and Esthetic Considerations. J. Periodontol. 1985, 56, 102–106. [Google Scholar] [CrossRef]
- Protásio, A.C.R.; Galvão, E.L.; Falci, S.G.M. Laser Techniques or Scalpel Incision for Labial Frenectomy: A Meta-Analysis. J. Maxillofac. Oral Surg. 2019, 18, 490–499. [Google Scholar] [CrossRef]
- Aoki, A.; Sasaki, K.M.; Watanabe, H.; Ishikawa, I. Lasers in Nonsurgical Periodontal Therapy. Periodontol. 2000 2004, 36, 59–97. [Google Scholar] [CrossRef]
- Tachmatzidis, T.; Dabarakis, N. Technology of Lasers and Their Applications in Oral Surgery: Literature Review. Balk. J. Dent. Med. 2016, 20, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Iodice, G.; Nanda, R.; Drago, S.; Repetto, L.; Tonoli, G.; Silvestrini-Biavati, A.; Migliorati, M. Accuracy of Direct Insertion of TADs in the Anterior Palate with Respect to a 3D-Assisted Digital Insertion Virtual Planning. Orthod. Craniofac. Res. 2022, 25, 192–198. [Google Scholar] [CrossRef]
- Capodiferro, S.; Tempesta, A.; Limongelli, L.; Barile, G.; Di Venere, D.; Corsalini, M. Minimally Invasive (Flapless) Crown Lengthening by Erbium:YAG Laser in Aesthetic Zone. F1000Research 2020, 9, 1185. [Google Scholar] [CrossRef]
- Parker, S. Verifiable CPD Paper: Laser-Tissue Interaction. Br. Dent. J. 2007, 202, 73–81. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Cirulli, N.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Marinelli, G.; Malcangi, G.; Coloccia, G.; Montenegro, V.; Di Pede, C.; Ciocia, A.M.; et al. Innovative Application of Diathermy in Orthodontics: A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 7448. [Google Scholar] [CrossRef]
- Ishikawa, I.; Aoki, A.; Takasaki, A.A. Potential Applications of Erbium:YAG Laser in Periodontics. J. Periodontal. Res. 2004, 39, 275–285. [Google Scholar] [CrossRef]
- Russell, A.D. Lethal Effects of Heat on Bacterial Physiology and Structure. Sci. Prog. 2003, 86, 115–137. [Google Scholar] [CrossRef]
- Haytac, M.C.; Ozcelik, O. Evaluation of Patient Perceptions after Frenectomy Operations: A Comparison of Carbon Dioxide Laser and Scalpel Techniques. J. Periodontol. 2006, 77, 1815–1819. [Google Scholar] [CrossRef]
- Azma, E.; Safavi, N. Diode Laser Application in Soft Tissue Oral Surgery. J. Lasers Med. Sci. 2013, 4, 206–211. [Google Scholar]
- Ortega-Concepción, D.; Cano-Durán, J.A.; Peña-Cardelles, J.-F.; Paredes-Rodríguez, V.-M.; González-Serrano, J.; López-Quiles, J. The Application of Diode Laser in the Treatment of Oral Soft Tissues Lesions. A Literature Review. J. Clin. Exp. Dent. 2017, 9, e925–e928. [Google Scholar] [CrossRef] [Green Version]
- Maspero, C.; Abate, A.; Inchingolo, F.; Dolci, C.; Cagetti, M.G.; Tartaglia, G.M. Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report. Children 2022, 9, 421. [Google Scholar] [CrossRef]
- Pasciuti, E.; Coloccia, G.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Bordea, I.R.; Cardarelli, F.; Di Venere, D.; Inchingolo, F.; Dipalma, G. Deep Bite Treatment with Aligners: A New Protocol. Appl. Sci. 2022, 12, 6709. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Wang, P.; Ding, Y.; Zhang, L. Comparative Frenectomy with Conventional Scalpel and Dual-Waved Laser in Labial Frenulum. World Jnl. Ped. Surg. 2022, 5, e000363. [Google Scholar] [CrossRef]
- Pie-Sanchez, J.; Espana-Tost, A.; Arnabat-Dominguez, J.; Gay-Escoda, C. Comparative Study of Upper Lip Frenectomy with the CO2 Laser versus the Er, Cr:YSGG Laser. Med. Oral 2012, 17, e228–e232. [Google Scholar] [CrossRef] [Green Version]
- Sfasciotti, G.L.; Zara, F.; Vozza, I.; Carocci, V.; Ierardo, G.; Polimeni, A. Diode versus CO2 Laser Therapy in the Treatment of High Labial Frenulum Attachment: A Pilot Randomized, Double-Blinded Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 7708. [Google Scholar] [CrossRef]
- Onur, S.G. Evaluation of Pain Perception and Wound Healing After Laser-Assisted Frenectomy in Pediatric Patients: A Retrospective Comparative Study. Photobiomodulation Photomed. Laser Surg. 2021, 39, 204–210. [Google Scholar] [CrossRef]
- Pulido Rozo, M.A.; Tirado Amador, L.R.; Madrid Troconis, C.C. Gingivoplastia y frenillectomía labial con láser de alta intensidad: Presentación de caso. Rev. Clín. Periodoncia Implantol. Rehabil. Oral 2015, 8, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Júnior, R.M.; Gueiros, L.A.; Silva, I.H.; de Albuquerque Carvalho, A.; Leão, J.C. Labial Frenectomy with Nd:YAG Laser and Conventional Surgery: A Comparative Study. Lasers Med. Sci. 2015, 30, 851–856. [Google Scholar] [CrossRef]
- De SPinheiroa, A.F.; Furtadoa, G.S.; Sanderb, H.H.; Serraa, L.L.; Lagoa, A.D. Duas propostas cirúrgicas para frenectomia labial—Convencional e a laser de alta potência. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2018, 59, 125–130. [Google Scholar] [CrossRef]
- Coscia, M.F.; Monno, R.; Ballini, A.; Mirgaldi, R.; Dipalma, G.; Pettini, F.; Cristallo, V.; Inchingolo, F.; Foti, C.; de Vito, D. Human Papilloma Virus (HPV) Genotypes Prevalence in a Region of South Italy (Apulia). Ann. Ist. Super Sanita 2015, 51, 248–251. [Google Scholar] [CrossRef]
- Saucedo, C.L.; Courtois, E.C.; Wade, Z.S.; Kelley, M.N.; Kheradbin, N.; Barrett, D.W.; Gonzalez-Lima, F. Transcranial Laser Stimulation: Mitochondrial and Cerebrovascular Effects in Younger and Older Healthy Adults. Brain Stimul. 2021, 14, 440–449. [Google Scholar] [CrossRef]
- Farronato, M.; Maspero, C.; Abate, A.; Grippaudo, C.; Connelly, S.T.; Tartaglia, G.M. 3D Cephalometry on Reduced FOV CBCT: Skeletal Class Assessment through AF-BF on Frankfurt Plane-Validity and Reliability through Comparison with 2D Measurements. Eur. Radiol. 2020, 30, 6295–6302. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.M.; Isacco, C.G.; et al. SARS-CoV-2 Disease through Viral Genomic and Receptor Implications: An Overview of Diagnostic and Immunology Breakthroughs. Microorganisms 2021, 9, 793. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Hazballa, D.; Inchingolo, A.D.; Malcangi, G.; Marinelli, G.; Mancini, A.; Maggiore, M.E.; Bordea, I.R.; Scarano, A.; Farronato, M.; et al. Innovative Concepts and Recent Breakthrough for Engineered Graft and Constructs for Bone Regeneration: A Literature Systematic Review. Materials 2022, 15, 1120. [Google Scholar] [CrossRef]
- Maspero, C.; Cappella, A.; Dolci, C.; Cagetti, M.G.; Inchingolo, F.; Sforza, C. Is Orthodontic Treatment with Microperforations Worth It? A Scoping Review. Children 2022, 9, 208. [Google Scholar] [CrossRef]
- Contaldo, M.; Itro, A.; Lajolo, C.; Gioco, G.; Inchingolo, F.; Serpico, R. Overview on Osteoporosis, Periodontitis and Oral Dysbiosis: The Emerging Role of Oral Microbiota. Appl. Sci. 2020, 10, 6000. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ferrara, I.; Viapiano, F.; Netti, A.; Campanelli, M.; Buongiorno, S.; Latini, G.; Carpentiere, V.; Ciocia, A.M.; Ceci, S.; et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. [Google Scholar] [CrossRef] [PubMed]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Pezzolla, C.; Patano, A.; Ceci, S.; Ciocia, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Cardarelli, F.; Piras, F.; et al. Experimental Analysis of the Use of Cranial Electromyography in Athletes and Clinical Implications. Int. J. Environ. Res. Public Health 2022, 19, 7975. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Cesarano, F.; Arazzi, M.; Di Liberato, L.; Scacco, S.; Grassi, R.; Grassi, F.R.; Gnoni, A.; et al. Periodontal Microbiological Status Influences the Occurrence of Cyclosporine-A and Tacrolimus-Induced Gingival Overgrowth. Antibiotics 2019, 8, 124. [Google Scholar] [CrossRef] [Green Version]
- Lorusso, F.; Inchingolo, F.; Dipalma, G.; Postiglione, F.; Fulle, S.; Scarano, A. Synthetic Scaffold/Dental Pulp Stem Cell (DPSC) Tissue Engineering Constructs for Bone Defect Treatment: An Animal Studies Literature Review. Int. J. Mol. Sci. 2020, 21, 9765. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | KEYWORDS: A: “frenulum”; B: “surgery” |
| Boolean Indicators: (“A” AND “B”) | |
| Timespan: from 13 November 2012 to 13 November 2022 | |
| Electronic Database: Pubmed, Cochrane, Scopus and Embase |
| Author/ Year | Study Design | Sample Size | Average Age at Intervention (Years) | Type of Surgery | Follow-Up |
|---|---|---|---|---|---|
| Komori S. et al. 2017 [8] | Retrospective | 21 total laser surgery 15 lingual 6 labial | 6.0 Lingual: 5.2 Labial: 8.2 | CO2 laser with a continuous wave at 2 to 5 W for ~60 s | 4.6 months Re-adhesion in 1 patient of the lingual frenulum |
| Xie L. et al. 2021 [31] | DB-RCT | 34 patients 17 laser surgery 17 scalpel surgery | 5–10 | Laser surgery: First, Er:YAG laser with wavelength 2940 nm short pulse (SP); energy: 60 MJ; Frequency: 30 Hz; power: 1.80 W. Subsequently, Nd:YAG laser, were set as pulse width: very long pulse; frequency: 20 Hz; power: 4.00 W | 1 month Wound healing and no re-adhesion in every group Scar in 1 case of scalpel surgical technique |
| Scalpel surgery: used sterile scalpels, #11 and 4–0 absorbable suture | |||||
| Pie-Sanchez J. et al. 2012 [32] | RCT | 50 total patients 25 CO2 laser surgery 25 Er,Cr:YSGG laser surgery | 11.3 | CO2 laser with 10,600 nm wavelength used in the focused continuous wave mode, a power rating of 5 W | 4 months No difference in post-operatory Intraoperative, bloodless field and faster operation time in CO2 laser group Faster wound healing in Er,Cr: YSGG laser group |
| Er,Cr:YSGG laser 2780 nm wavelength, a pulse duration between 140 and 200 µs, and a 20 Hz frequency. Power settings: 1.5 W with 12% water and 8% air | |||||
| Sfasciotti G.L. et al. 2020 [33] | DB-RCT | 26 total patients 13 Diode laser surgery 13 CO2 laser surgery | 9 | The diode laser 980 nm wavelength with a continuous modality of pulse and set at 2.5 W | 14 days Better biological results and fewer intraoperative errors in Diode laser group |
| The CO2 laser with 10.600 nm in a super pulse wave modality set at 4.5 W | |||||
| Onur S.G et al., 2020 [34] | Retrospective | 22 total patients 11 Er,Cr:YSGG laser surgery 11 diode laser surgery | 8–13 | 2780 nm Er,Cr:YSGG laser: power 2.75 W; frequency, 50 Hz; pulse duration, 60 ls; pulse energy, 55 mJ/pulse; energy density per pulse, 22 J/cm2; 20% air, 40% water | 2 weeks Better wound healing in the Er,Cr:YSGG laser group |
| 940 nm diode laser operated at a power of 1.5 W incontinuous wave mode | |||||
| Pulido Rozo M.A. et al., 2015 [35] | Case report | 1 | 16 | High-intensity laser not specified | 15 days Post-operative edema resolved and good healing |
| Junior et al., 2015 [36] | Prospective | 40 total patients 22 scalpel surgery 18 Nd:YAG laser surgery | 20.9 ± 10.3 | Scalpel blade no. 15 and simple suture with silk thread 4–0 | Reduced surgery time and no sutures in Nd:YAG laser group |
| Nd:YAG laser (λ = 1064 nm) with the following parameters: 40 J of energy, 40 Hz frequency, 4 W of power, for 10 s (power density = 5 W/cm2 and energy density = 50 J/cm2), and a short pulse width | |||||
| Pinheiro A. et al., 2018 [37] | Case series | 1 scalpel surgery 1 diode laser surgery | 28 | An incision with scalpel number 15 and suture with nylon thread 5.0 | 7 days More time-effective and less intra- and post-operative bleeding in laser surgery Post-operative drug intake, discomfort, and edema in scalpel surgery |
| Diode laser infrared wavelength 808 nm infrared 808 nm, power of 2 W, the energy of 120 J, pulsed mode pulsed mode and 20 pps repetition frequency |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.M.; Malcangi, G.; Ferrara, I.; Viapiano, F.; Netti, A.; Buongiorno, S.; Latini, G.; Azzollini, D.; De Leonardis, N.; de Ruvo, E.; et al. Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1302. https://doi.org/10.3390/ijerph20021302
Inchingolo AM, Malcangi G, Ferrara I, Viapiano F, Netti A, Buongiorno S, Latini G, Azzollini D, De Leonardis N, de Ruvo E, et al. Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(2):1302. https://doi.org/10.3390/ijerph20021302
Chicago/Turabian StyleInchingolo, Angelo Michele, Giuseppina Malcangi, Irene Ferrara, Fabio Viapiano, Anna Netti, Silvio Buongiorno, Giulia Latini, Daniela Azzollini, Nicole De Leonardis, Elisabetta de Ruvo, and et al. 2023. "Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 2: 1302. https://doi.org/10.3390/ijerph20021302
APA StyleInchingolo, A. M., Malcangi, G., Ferrara, I., Viapiano, F., Netti, A., Buongiorno, S., Latini, G., Azzollini, D., De Leonardis, N., de Ruvo, E., Mancini, A., Rapone, B., Venere, D. D., Patano, A., Avantario, P., Tartaglia, G. M., Lorusso, F., Scarano, A., Sauro, S., ... Dipalma, G. (2023). Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review. International Journal of Environmental Research and Public Health, 20(2), 1302. https://doi.org/10.3390/ijerph20021302