
Is There a Correlation between Dental Occlusion, Postural Stability and Selected Gait Parameters in Adults?



Abstract
:1. Introduction
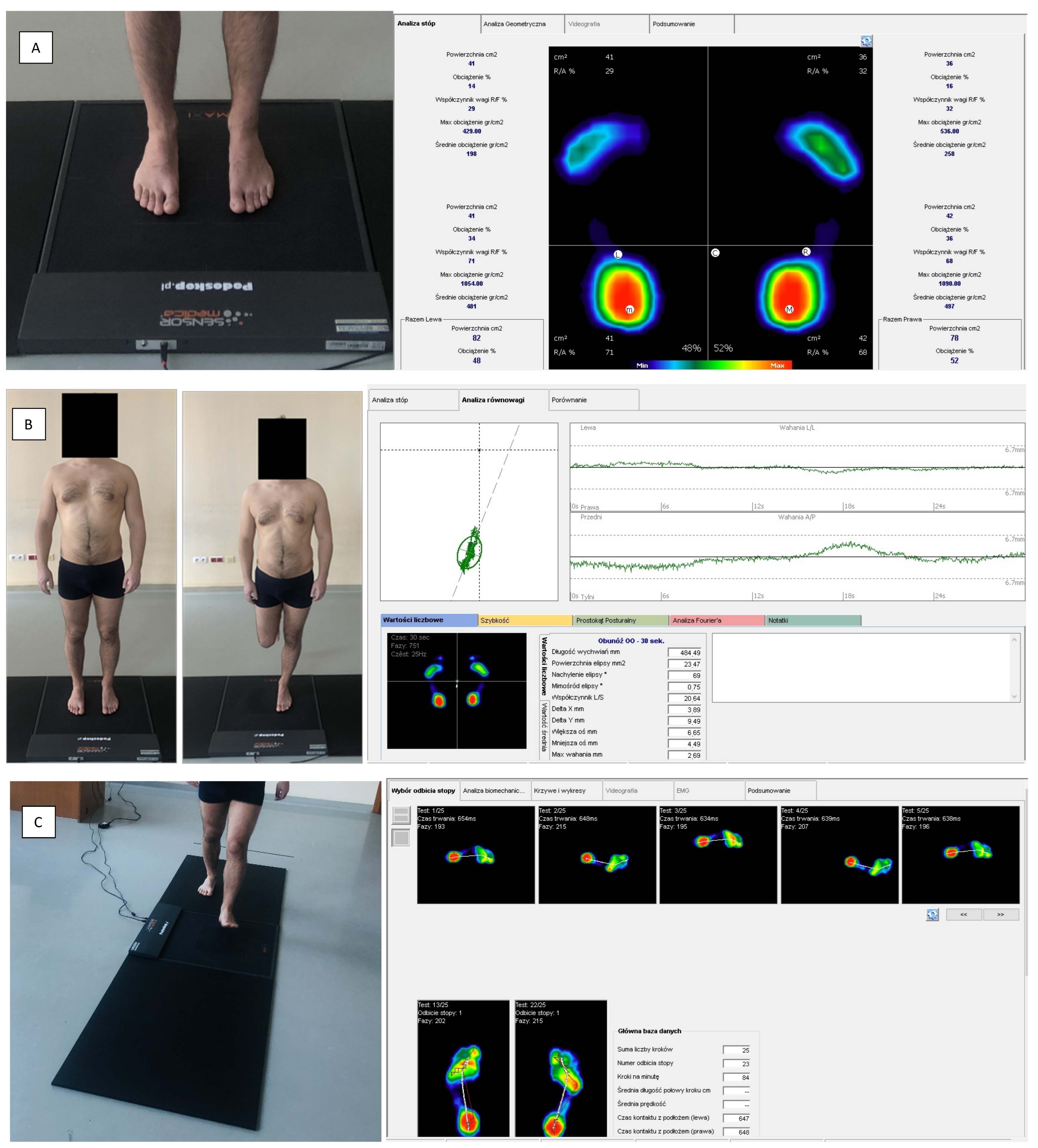
2. Materials and Methods
- (1)
- Standing on both feet with eyes open;
- (2)
- Standing on both feet with eyes closed;
- (3)
- Standing on the left foot with eyes open;
- (4)
- Standing on the right foot with eyes open;
- (5)
- Standing on the left foot with eyes closed;
- (6)
- Standing on the right foot with eyes closed.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guez, G. The Posture. In Principles of Neural Science; Kandel, E., Schwartz, J., Eds.; Elsevier: Amsterdam, The Netherlands, 1991; pp. 612–623. [Google Scholar]
- Czaprowski, D.; Stoliński, L.; Tyrakowski, M.; Kozinoga, M.; Kotwicki, T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis Spinal Disord. 2018, 13, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwanenko, J.; Gurfinkel, V. Human postural control. Front. Neurosci. 2018, 12, 17. [Google Scholar]
- Guerraz, M.; Bronstein, A.M. Ocular versus extraocular control of posture and equilibrium. Neurophysiol. Clin. 2008, 38, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Hamaoui, A.; Frianta, Y.; Le Bozec, S. Does increased muscular tension along the torso impair postural equilibrium in a standing posture? Gait Posture 2011, 34, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Kolar, P.; Sulc, J.; Kyncl, M.; Sanda, J.; Neuwirth, J.; Bokarius, A.V.; Kriz, J.; Kobesova, A. Stabilizing function of the diaphragm: Dynamic MRI and synchronized spirometric assessment. J. Appl. Physiol. 2010, 109, 1064–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczygieł, E.; Fudacz, N.; Golec, J.; Golec, E. The impact of the position of the head on the functioning of the human body: A systematic review. Int. J. Occup. Med. Environ. Health 2020, 33, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Tardieu, C.; Dumitrescu, M.; Giraudeau, A.; Blanc, J.L.; Cheynet, F.; Borel, L. Dental occlusion and postural control in adults. Neurosci. Lett. 2009, 450, 221–224. [Google Scholar] [CrossRef]
- Munhoz, W.C.; Hsing, W.T. Interrelations between orthostatic postural deviations and subjects’ age, sex, malocclusion, and specific signs and symptoms of functional pathologies of the temporomandibular system: A preliminary correlation and regression study. Cranio 2014, 32, 175–186. [Google Scholar] [CrossRef]
- Pérez-Belloso, A.J.; Coheña-Jiménez, M.; Cabrera-Domínguez, M.E.; Galan-González, A.F.; Domínguez-Reyes, A.; Pabón-Carrasco, M. Influence of dental malocclusion on body posture and foot posture in children: A cross-sectional study. Healthcare 2020, 8, 485. [Google Scholar] [CrossRef]
- Amaricai, E.; Onofrei, R.R.; Suciu, O.; Marcauteanu, C.; Stoica, E.T.; Negruțiu, M.L.; David, V.L.; Sinescu, C. Do different dental conditions influence the static plantar pressure and stabilometry in young adults? PLoS ONE 2020, 15, e0228816. [Google Scholar] [CrossRef] [Green Version]
- Cabrera-Domínguez, M.E.; Domínguez-Reyes, A.; Pabón-Carrasco, M.; Pérez-Belloso, A.J.; Coheña-Jiménez, M.; Galán-González, A.F. Dental malocclusion and its relation to the podal system. Front. Pediatr. 2021, 9, 654229. [Google Scholar] [CrossRef]
- Myers, T. Anatomy Trains: Myofasziale Leitbahnen (für Manual- und Bewegungstherapeuten); Elsevier Health Sciences: Berlin, Germany, 2015. [Google Scholar]
- Pinganaud, G.; Bourcier, F.; Buisseret-Delmas, C.; Buisseret, P. Primary trigeminal afferents to the vestibular nuclei in the rat: Existence of a collateral projection to the vestibulo-cerebellum. Neurosci. Lett. 1999, 264, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Bracco, P.; Deregibus, A.; Piscetta, R. Effects of different jaw relations on postural stability in human subjects. Neurosci. Lett. 2004, 356, 228–230. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Castroflorio, T.; Perinetti, G.; Guarda-Nardini, L. Dental occlusion, body posture and temporomandibular disorders: Where we are now and where we are heading for. J. Oral Rehabil. 2012, 39, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, K.; Mehta, N.R.; Abdallah, E.F.; Forgione, A.G.; Hirayama, H.; Kawasaki, T.; Yokoyama, A. Examination of the relationship between mandibular position and body posture. Cranio 2007, 25, 237–249. [Google Scholar] [CrossRef]
- Cuccia, A.; Caradonna, C. The relationship between the stomatognathic system and body posture. Clinics 2009, 64, 61–63. [Google Scholar] [CrossRef] [Green Version]
- Marchena-Rodríguez, A.; Moreno-Morales, N.; Ramírez-Parga, E.; Labajo-Manzanares, M.T.; Luque-Suárez, A.; Gijon-Nogueron, G. Relationship between foot posture and dental malocclusions in children aged 6 to 9 years. A cross-sectional study. Medicine 2018, 97, e0701. [Google Scholar] [CrossRef]
- Iacob, S.M.; Chisnoiu, A.M.; Buduru, S.D.; Berar, A.; Fluerasu, M.I.; Iacob, I.; Objelean, A.; Studnicska, W.; Viman, L.M. Plantar pressure variations induced by experimental malocclusion—A pilot case series study. Healthcare 2021, 9, 599. [Google Scholar] [CrossRef]
- Michelotti, A.; Buonocore, G.; Farella, M.; Pellegrino, G.; Piergentili, C.; Altobelli, S.; Martina, R. Postural stability and unilateral posterior crossbite: Is there a relationship? Neurosci. Lett. 2006, 392, 140–144. [Google Scholar] [CrossRef]
- Perinetti, G.; Contardo, L.; Silvestrini-Biavati, A.; Perdoni, L.; Castaldo, A. Dental malocclusion and body posture in young subjects: A multiple regression study. Clinics 2010, 65, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Scharnweber, B.; Adjami, F.; Schuster, G.; Kopp, S.; Natrup, J.; Erbe, C.; Ohlendorf, D. Influence of dental occlusion on postural control and plantar pressure distribution. Cranio 2017, 35, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Isaia, B.; Ravarotto, M.; Finotti, P.; Nogara, M.; Piran, G.; Gamberini, J.; Biz, C.; Masiero, S.; Frizziero, A. Analysis of dental malocclusion and neuromotor control in young healthy subjects through new evaluation tools. J. Funct. Morphol. Kinesiol. 2019, 4, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michalakis, K.X.; Kamalakidis, S.N.; Pissiotis, A.L.; Hirayama, H. The Effect of clenching and occlusal instability on body weight distribution, assessed by a postural platform. BioMed Res. Int. 2019, 2019, 7342541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julià-Sánchez, S.; Álvarez-Herms, J.; Cirer-Sastre, R.; Corbi, F.; Burtscher, M. The influence of dental occlusion on dynamic balance and muscular tone. Front. Physiol. 2020, 10, 1626. [Google Scholar] [CrossRef]
- Pacella, E.; Dari, M.; Giovannoni, D.; Mezio, M.; Caterini, L.; Costantini, A. The relationship between occlusion and posture: A systematic review. Orthodontics 2017, 8, WMC005374. [Google Scholar]
- Moon, H.J.; Lee, Y.K. The relationship between dental occlusion/temporomandibular joint status and general body health: Part 1. Dental occlusion and TMJ status exert an influence on general body health. J. Altern. Complement. Med. 2011, 17, 995–1000. [Google Scholar] [CrossRef] [Green Version]
- Souza, J.A.; Pasinato, F.; Correa, E.A.; da Silva, A.M. Global body posture and plantar pressure distribution in individuals with and without temporomandibular disorder: A preliminary study. J. Manip. Physiol. Ther. 2014, 37, 407–414. [Google Scholar]
- Ferrillo, M.; Marotta, N.; Giudice, A.; Calafiore, D.; Curci, C.; Fortunato, L.; Ammendolia, A.; de Sire, A. Effects of occlusal splints on spinal posture in patients with temporomandibular disorders: A systematic review. Healthcare 2022, 10, 739. [Google Scholar] [CrossRef]
- Saccucci, M.; Tettamanti, L.; Mummolo, S.; Polimeni, A.; Festa, F.; Tecco, S. Scoliosis and dental occlusion: A review of the literature. Scoliosis 2011, 6, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Sforza, C.; Tartaglia, G.M.; Solimene, U.; Morgan, V.; Kaspranskiy, R.R.; Ferrario, V.F. Occlusion, sternocleidomastoid muscle activity, and body sway: A pilot study in male astronauts. Cranio 2006, 24, 43–49. [Google Scholar] [CrossRef]
- Michelotti, A.; Buonocore, G.; Manzo, P.; Pellegrino, G.; Farella, M. Dental occlusion and posture: An overview. Prog. Orthod. 2011, 12, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Ishizawa, T.; Xu, H.; Onodera, K.; Ooya, K. Weight distributions on soles of feet in the primary and early permanent dentition with normal occlusion. J. Clin. Pediatr. Dent. 2005, 30, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Bernabé, E.; Sheiham, A.; de Oliveira, C.M. Condition-specific impacts on quality of life attributed to malocclusion by adolescents with normal occlusion and Class I, II and III malocclusion. Angle Orthod. 2008, 78, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion; Mosby: Maryland Heights, MO, USA, 2019. [Google Scholar]
- Lombardo, G.; Vena, F.; Negr, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–122. [Google Scholar] [PubMed]
- Kawala, B.; Szumielewicz, M.; Kozanecka, A. Are orthodontists still needed? Epidemiology of malocclusion among polish children and teenagers in last 15 years. Dent. Med. Probl. 2009, 46, 273–278. [Google Scholar]
- Buldt, A.K.; Murley, G.S.; Butterworth, P.; Levinger, P.; Menz, H.B.; Landorf, K.B. The relationship between foot posture and lower limb kinematics during walking: A systematic review. Gait Posture 2013, 38, 363–372. [Google Scholar] [CrossRef]
- Baldini, A.; Nota, A.; Tripodi, D.; Longoni, S.; Cozza, P. Evaluation of the correlation between dental occlusion and posture using a force platform. Clinics 2013, 68, 45–49. [Google Scholar] [CrossRef]
- Cuccia, A.M. Interrelationships between dental occlusion and plantar arch. J. Bodyw. Mov. Ther. 2011, 15, 242–250. [Google Scholar] [CrossRef]
- Maurer, C.; Holzgreve, F.; Erbe, C.; Wanke, E.M.; Kopp, S.; Groneberg, D.A.; Ohlendorf, D. Influence of dental occlusion conditions on plantar pressure distribution during standing and walking—A gender perspective. Med. Eng. Phys. 2021, 88, 47–53. [Google Scholar] [CrossRef]
- Pyda-Dulewicz, A.; Konopka, W.; Fedorowicz, J.; Pepaś, R. Effect of physical activity on posturography in healthy subjects. Otorynolaryngol 2017, 16, 125–130. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Nobili, A.; Adversi, R. Relationship between posture and occlusion: A clinical and experimental investigation. Cranio 1996, 14, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Syed, N.; Karvannan, H.; Maiya, A.G.; Binukumar, B.; Prem, V.; Chakravarty, R.D. Plantar pressure distribution among asymptomatic individuals: A cross-sectional study. Foot Ankle Spec. 2012, 5, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Pomarino, D.; Pomarino, A. Plantar static pressure distribution in healthy individuals: Percentiles for the evaluation of forefoot loading. Foot Ankle Spec. 2014, 7, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Šidlauskienė, M.; Smailienė, D.; Lopatienė, K.; Čekanauskas, E.; Pribuišienė, R.; Šidlauskas, M. Relationships between malocclusion, body posture, and nasopharyngeal pathology in pre-orthodontic children. Med. Sci. Monit. 2015, 18, 1765–1773. [Google Scholar]
- Szczygieł, E.; Piotrowski, K.; Golec, J.; Czechowska, D.; Masłoń, A.; Bac, A.; Golec, E. Head position influence on stabilographic variables. Acta Bioeng. Biomech. 2016, 18, 49–54. [Google Scholar]
- Palm, H.G.; Strobel, J.; Achatz, G.; von Luebken, F.; Friemert, B. The role and interaction of visual and auditory afferents in postural stability. Gait Posture 2009, 30, 328–333. [Google Scholar] [CrossRef]
- Massery, M.; Hagins, M.; Stafford, R.; Moerchen, V.; Hodges, P.W. Effect of airway control by glottal structures on postural stability. J. Appl. Physiol. 2013, 115, 483–490. [Google Scholar] [CrossRef]
- Gawron, W.; Pośpiech, L.; Orendorz-Fraczkowska, K. An evaluation of postural stability and the effects of middle-ear drainage on vestibulo-spinal reflexes of children with chronic otitis media with effusion. Int. J. Pediatr. Otorhinolaryngol. 2004, 68, 1175–1179. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Fay, V.; Avaniadi, I.; Erbe, C.; Wanke, E.M.; Groneberg, D.A. Association between constitution, axiography, analysis of dental casts, and postural control in women aged between 41 and 50 years. Clin. Oral Investig. 2021, 25, 2595–2607. [Google Scholar] [CrossRef]
- Julia-Sanchez, S.; Alvarez-Herms, J.; Gatterer, H.; Burtscher, M.; Pages, T. Dental occlusion influences the standing balance on an unstable platform. Motor Control 2015, 19, 341–354. [Google Scholar] [CrossRef]
- Stancker, T.G.; Silva, A.C.; Neto, H.P.; Rodrigues, C.D.A. Malocclusion influence on balance and posture: A systematic review. Man Ther. Posturology Rehabil. J. 2015, 13, 320. [Google Scholar] [CrossRef] [Green Version]
- Gangloff, P.; Louis, J.P.; Perrin, P.P. Dental occlusion modifies gaze and posture stabilization in human subjects. Neurosci. Lett. 2000, 293, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Szczygieł, E.; Gędek, R.; Golec, J.; Golec, E.; Bac, A.; Walocha, J.; Marchewka, A. Analysis of chosen posturographic parametres in specific age groups. J. Orthop. Trauma Surg. Relat. Res. 2012, 27, 56–67. [Google Scholar]
- Arumugam, P.; Padmanabhan, S.; Chitharanjan, A. The relationship of postural body stability and severity of malocclusion. APOS Trends Orthod. 2016, 6, 205–210. [Google Scholar] [CrossRef]
- Álvarez Solano, C.; González Camacho, L.A.; Castaño Duque, S.P.; Cortés Velosa, T.; Vanoy Martin, J.A.; Chambrone, L. To evaluate whether there is a relationship between occlusion and body posture as delineated by a stabilometric platform: A systematic review. Cranio 2020, 24, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Menz, H.B. Visual contributions to postural stability in older adults. Gerontology 2000, 46, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Polimeni, A.; Saccucci, M.; Festa, F. Postural loads during walking after an imbalance of occlusion created with unilateral cotton rolls. BMC Res. Notes 2010, 3, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, M.; Hayakawa, L.; Hirano, S.; Watanabe, I. Changes in gait stability induced by alteration of mandibular position. J. Med. Dent. Sci. 2001, 48, 131–136. [Google Scholar]
- Ohlendorf, D.; Seebach, K.; Hoerzer, S.; Nigg, S.; Kopp, S. The effects of a temporarily manipulated dental occlusion on the position of the spine: A comparison during standing and walking. Spine J. 2014, 14, 2384–2391. [Google Scholar] [CrossRef]
- Dias, A.; Redinha, L.; Rodrigues, M.J.; Silva, L.; Pezarat-Correia, P. A kinematic analysis on the immediate effects of occlusal splints in gait and running body sway patterns. Cranio 2020, 29, 1–7. [Google Scholar] [CrossRef]
- Maurer, C.; Stief, F.; Jonas, A.; Kovac, A.; Groneberg, D.A.; Meurer, A.; Ohlendorf, D. Influence of the lower jaw position on the running pattern. PLoS ONE 2015, 10, e0135712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, T.S.; Flavel, S.C.; Nordstrom, M.A. Control of human mandibular posture during locomotion. J. Physiol. 2004, 554, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Tramonti Fantozzi, M.P.; Diciotti, S.; Tessa, C.; Castagna, B.; Chiesa, D.; Barresi, M.; Ravenna, G.; Faraguna, U.; Vignali, C.; De Cicco, V.; et al. Unbalanced occlusion modifies the pattern of brain activity during execution of a finger to thumb motor task. Front. Neurosci. 2019, 13, 499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manni, E.; Palmieri, G.; Marini, R.; Pettorossi, V.E. Trigeminal influences on extensor muscles of the neck. Exp. Neurol. 1975, 47, 330–342. [Google Scholar] [CrossRef]
- Herbert, R.; Jamtvedt, G.; Mead, J.; Hagen, K.B. Practical Evidence-Based Physiotheraphy; Elsevier Butterworth Heinemann: Edinburg, UK, 2005; pp. 2–10. [Google Scholar]


{kind=link}
| Analysed Groups | N | Age [Years] | Body Height [cm] | Body Weight [kg] | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Av. | Min. | Max. | Av. | Min. | Max. | Av. | Min. | Max. | ||
| I (Angle Class III) | 30 | 22.77 | 20 | 30 | 170.93 | 157 | 186 | 68.23 | 48 | 100 |
| II (Angle Class II) | 30 | 23.87 | 19 | 35 | 172.8 | 157 | 183 | 66.93 | 48 | 91 |
| III (Angle Class I) | 30 | 22.63 | 19 | 32 | 171.73 | 155 | 192 | 67.27 | 47 | 90 |
| Parameters | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class | II Class | III Class | |||
| Forefoot percentage weight-bearing left—LL [%] | Av ± SD | 36.73 ± 10.35 | 45.53 ± 15.11 | 31.43 ± 14.26 | p = 0.002 * |
| Median | 36 | 42.5 | 30 | ||
| Quartiles | 27.25–43.75 | 35.5–52 | 21–40.25 | Cl.II > Cl.I, Cl.III | |
| Forefoot percentage weight-bearing right—LL [%] | Av ± SD | 37.1 ± 11.83 | 46.7 ± 14.96 | 29.57 ± 10.56 | p < 0.001 * |
| Median | 38 | 46 | 28 | ||
| Quartiles | 29.25–44.5 | 35.25–57.75 | 21.25–36 | Cl.II > Cl.I > Cl.III | |
| Hindfoot percentage weight-bearing—left LL [%] | Av ± SD | 63.27 ± 10.35 | 54.47 ± 15.11 | 67.07 ± 16.61 | p = 0.004 * |
| Median | 64 | 57.5 | 70 | ||
| Quartiles | 56.25–72.75 | 48–64.5 | 57.5–79 | Cl.III, Cl.I > Cl.II | |
| Hindfoot percentage weight-bearing—left LL [%] | Av ± SD | 62.9 ± 11.83 | 53.3 ± 14.96 | 68.6 ± 13.12 | p < 0.001 * |
| Median | 62 | 54 | 71 | ||
| Quartiles | 55.5–70.75 | 42.25–64.75 | 61.75–74.75 | Cl.III, Cl.I > Cl.II | |
| Mean forefoot pressure values—left LL [g/cm2] | Av ± SD | 295.73 ± 67.06 | 329.53 ± 63.6 | 283.47 ± 70.63 | p = 0.018 * |
| Median | 295.5 | 329.5 | 290.5 | ||
| Quartiles | 245.5–329.5 | 303.75–355.5 | 247–323.25 | Cl.II > Cl.I, Cl.III | |
| Mean forefoot pressure values—right LL [g/cm2] | Av ± SD | 284.57 ± 60.48 | 351.7 ± 62.8 | 293.67 ± 114.31 | p < 0.001 * |
| Median | 288.5 | 346 | 267 | ||
| Quartiles | 233–318.25 | 307–386 | 237.5–313.25 | Cl.II > Cl.III, Cl.I | |
| Mean hindfoot pressure values—left LL [g/cm2] | Av ±SD | 540.17 ± 120.86 | 488.03 ± 157.95 | 608.3 ± 263.09 | p = 0.142 |
| Median | 523 | 501.5 | 569 | ||
| Quartiles | 474.75–636.75 | 371–601 | 465.75–682.25 | ||
| Mean hindfoot pressure values—right LL [g/cm2] | Av ± SD | 515.17 ± 116.6 | 460.47 ± 121.8 | 637.3 ± 316.44 | p = 0.002 * |
| Median | 498.5 | 431.5 | 573 | ||
| Quartiles | 435.5–583 | 400–553.25 | 511–704 | Cl.III > Cl.I, Cl.II | |
| Parameters | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class | II Class | III Class | |||
| CoP displacement in sagittal plane | Forward | 11 (36.67%) | 20 (66.67%) | 5 (16.67%) | p < 0.001 * |
| Backward | 19 (63.33%) | 10 (33.33%) | 25 (83.33%) | ||
| CoP displacement in frontal plane | Non | 6 (20.00%) | 9 (30.00%) | 4 (13.33%) | p = 0.419 |
| Left | 19 (63.33%) | 14 (46.67%) | 17 (56.67%) | ||
| Right | 5 (16.67%) | 7 (23.33%) | 9 (30.00%) | ||
| Lateral CoP displacement [cm] | Av ± SD | 1.46 ± 0.89 | 1.95 ± 1.03 | 2.38 ± 1.21 | p = 0.009 * |
| Median | 1.12 | 2.01 | 1.97 | ||
| Quartiles | 0.8–2.21 | 1.16–2.22 | 1.41–3.4 | Cl.III > Cl.I | |
| Romberg Test (on both Feet, Eyes Open) | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class (N = 30) | II Class (N = 30) | III Class (N = 30) | |||
| CoP path length [mm] | Av ± SD | 502.81 ± 119.75 | 645.89 ± 236.91 | 748.86 ± 243.38 | p < 0.001 * |
| Median | 496.74 | 576.86 | 689.7 | ||
| Quartiles | 403.48–573.34 | 482.06–772.48 | 595.54–855.47 | Cl.III, Cl.II > Cl.I | |
| Ellipse area [mm2] | Av ± SD | 90.01 ± 75.1 | 166.81 ± 134.7 | 192.07 ± 161.17 | p = 0.004 * |
| Median | 64.28 | 109.3 | 129.58 | ||
| Quartiles | 34.87–128.2 | 58.54–299.67 | 91.96–308.18 | Cl.III, Cl.II > Cl.I | |
| Mean CoP sway rate [mm/s] | Av ± SD | 18.48 ± 5.04 | 22 ± 8.27 | 24.87 ± 9.46 | p = 0.012 * |
| Median | 19.26 | 19.81 | 23.2 | ||
| Quartiles | 15.03–20.24 | 15.22–26.64 | 19.58–30.66 | Cl.III > Cl.I | |
| Romberg test (on both feet, eyes closed) | Angle Class | p | |||
| I Class(N = 30) | II Class(N = 30) | III Class(N = 30) | |||
| CoP path length [mm] | Av ± SD | 552.53 ± 168.72 | 613.17 ± 206.2 | 745.91 ± 303.7 | p = 0.018 * |
| Median | 517.33 | 561.62 | 723.22 | ||
| Quartiles | 432.88–609.83 | 455.52–734.96 | 511.29–905.92 | Cl.III > Cl.I | |
| Ellipse area [mm2] | Av ± SD | 97.06 ± 110.42 | 159.65 ± 181.06 | 126.31 ± 88.62 | p = 0.03 * |
| Median | 41.3 | 76.7 | 90.56 | ||
| Quartiles | 23.77–109.93 | 54.98–172.12 | 58.5–169.96 | Cl.II, Cl.III > Cl.I | |
| Mean CoP sway rate [mm/s] | Av ± SD | 19.15 ± 6.13 | 21.03 ± 6.97 | 25.94 ± 10.5 | p = 0.013 * |
| Median | 17.24 | 19.4 | 24.36 | ||
| Quartiles | 14.54–23.02 | 15.65–25.5 | 17.55–31.5 | Cl.III > Cl.I | |
| One-Legged Stance Test (Eyes Open) | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class (N = 30) | II Class (N = 30) | III Class (N = 30) | |||
| CoP path length—left LL [mm] | Av ± SD | 417.57 ± 105.61 | 461.88 ± 108.93 | 514.06 ± 164.36 | p = 0.031 * |
| Median | 406.42 | 437.28 | 485.62 | ||
| Quartiles | 355.4–455.47 | 365.33–512.12 | 409.94–570.93 | Cl.III > Cl.I | |
| CoP path length—right LL [mm] | Av ± SD | 486.98 ± 74.98 | 523.49 ± 137.94 | 543.5 ± 166.75 | p = 0.659 |
| Median | 478.93 | 483.74 | 488.61 | ||
| Quartiles | 431.15–545.38 | 415.97–598.14 | 430.94–597.96 | ||
| Mean CoP sway rate—left LL [mm/s] | Av ± SD | 30.94 ± 10.03 | 36.29 ± 11.58 | 40.92 ± 13.63 | p = 0.005 * |
| Median | 30.76 | 33.99 | 39.44 | ||
| Quartiles | 23.26–33.81 | 27.02–42.21 | 31.87–50.22 | Cl.III > Cl.I | |
| Mean CoP sway rate—right LL [mm/s] | Av ± SD | 30.74 ± 7 | 34.15 ± 13.42 | 35.9 ± 13.78 | p = 0.66 |
| Median | 31.34 | 30.57 | 31.66 | ||
| Quartiles | 25.76–35.89 | 25.18–39.97 | 25.99–43.22 | ||
| Ellipse area—left LL [mm2] | Av ± SD | 410.24 ± 313.45 | 428.3 ± 247.6 | 417.79 ± 236.48 | p = 0.683 |
| Median | 299.64 | 398.24 | 357.7 | ||
| Quartiles | 223.85–516.29 | 280.85–487.85 | 267.64–443.97 | ||
| Ellipse area—right LL [mm2] | Av ± SD | 483.21 ± 317.8 | 681.3 ± 523.96 | 554.71 ± 378.34 | p = 0.31 |
| Median | 430.66 | 551.07 | 392.76 | ||
| Quartiles | 307.94–609 | 324.91–839.69 | 279.22–787.9 | ||
| One-Legged Stance Test (Eyes Closed) | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class (N = 30) | II Class (N = 30) | III Class (N = 30) | |||
| CoP path length—left LL [mm] | Av ± SD | 795.56 ± 129.87 | 902.89 ± 331.24 | 926.49 ± 441.19 | p = 0.574 |
| Media | 778.53 | 858.54 | 855.54 | ||
| Quartiles | 710.1–895.52 | 644.78–1018.92 | 702.32–962.43 | ||
| CoP path length—right LL [mm] | Av ± SD | 783.5 ± 149.87 | 896.41 ± 224.2 | 920.13 ± 408.51 | p = 0.161 |
| Median | 771.24 | 896.14 | 820.1 | ||
| Quartiles | 685.24–876.58 | 742.9–1067.58 | 695.88–1071.5 | ||
| Mean CoP sway rate—left LL [mm/s] | Av ± SD | 61.63 ± 12.27 | 71.08 ± 33.68 | 72.98 ± 30.36 | p = 0.314 |
| Median | 63.64 | 67.07 | 69.26 | ||
| Quartiles | 51.44–68.04 | 46.44–82.44 | 54.03–77.94 | ||
| Mean CoP sway rate -right LL [mm/s] | Av ± SD | 60.85 ± 14.65 | 71.91 ± 22.12 | 75.45 ± 40.52 | p = 0.125 |
| Median | 57.51 | 70.38 | 61.44 | ||
| Quartiles | 50.62–69.31 | 56.76–87.89 | 54.03–89.28 | ||
| Ellipse area—left LL [mm2] | Av ± SD | 2202.47 ± 1408.12 | 3078.82 ± 3387.25 | 2680.4 ± 2512.45 | p = 0.878 |
| Median | 1951.48 | 1812.28 | 1784.12 | ||
| Quartiles | 1377.34–2598.22 | 1250.5–3821.85 | 1125.59–2876.56 | ||
| Ellipse area—right LL [mm2] | Av ± SD | 2199.2 ± 1163.97 | 3037.05 ± 1602.42 | 5722.58 ± 15289.18 | p = 0.11 |
| Median | 1819.48 | 3005.4 | 2545.61 | ||
| Quartiles | 1293.87–2904.57 | 1724.28–4004.04 | 1269.19–4068.25 | ||
| Romberg Test (on Both Feet) | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class(N = 30) | II Class (N = 30) | III Class (N = 30) | |||
| RR for CoP path length | Av ± SD | 1.15 ± 0.43 | 0.98 ± 0.2 | 1.03 ± 0.37 | p = 0.49 |
| Median | 1.05 | 1.01 | 0.98 | ||
| Quartiles | 0.78–1.42 | 0.88–1.09 | 0.86–1.19 | ||
| RR for ellipse area | Av ± SD | 1.9 ± 2.64 | 1.44 ± 2.38 | 0.89 ± 0.61 | p = 0.88 |
| Median | 0.98 | 0.95 | 0.66 | ||
| Quartiles | 0.26–1.99 | 0.39–1.42 | 0.47–1.22 | ||
| RR for mean CoP sway rate | Av ± SD | 1.09 ± 0.43 | 0.99 ± 0.19 | 1.08 ± 0.34 | p = 0.762 |
| Median | 0.95 | 1 | 1 | ||
| Quartiles | 0.82–1.25 | 0.9–1.09 | 0.91–1.21 | ||
| One-legged stance test (left LL) | Angle Class | p | |||
| I Class (N = 30) | II Class (N = 30) | III Class (N = 30) | |||
| RR for CoP path length | Av ± SD | 2 ± 0.51 | 1.97 ± 0.6 | 1.88 ± 0.72 | p = 0.421 |
| Median | 1.96 | 1.79 | 1.73 | ||
| Quartiles | 1.69–2.21 | 1.53–2.29 | 1.36–2.12 | ||
| RR for ellipse area | Av ± SD | 7.69 ± 6.6 | 10.12 ± 13.23 | 7.79 ± 7.96 | p = 0.778 |
| Median | 7.5 | 4.84 | 4.6 | ||
| Quartiles | 3.43–9.31 | 3.56–8.67 | 3.46–8.31 | ||
| RR for mean CoP sway rate | Av ± SD | 2.15 ± 0.71 | 2 ± 0.84 | 1.9 ± 0.8 | p = 0.227 |
| Median | 2.1 | 1.75 | 1.77 | ||
| Quartiles | 1.72–2.61 | 1.41–2.36 | 1.24–2.23 | ||
| One-legged stance test (right LL) | Angle Class | p | |||
| I Class (N = 30) | II Class (N = 30) | III Class (N = 30) | |||
| RR for CoP path length | Av ± SD | 1.63 ± 0.32 | 1.75 ± 0.4 | 1.71 ± 0.49 | p = 0.576 |
| Median | 1.52 | 1.64 | 1.68 | ||
| Quartiles | 1.43–1.83 | 1.49–1.93 | 1.4–1.9 | ||
| RR for ellipse area | Av ± SD | 6.58 ± 6.06 | 6.3 ± 4.46 | 18.38 ± 62.42 | p = 0.861 |
| Median | 4.65 | 4.88 | 4.72 | ||
| Quartiles | 2.52–8.35 | 2.74–8.98 | 2.92–11.53 | ||
| RR for mean CoP sway rate | Av ± SD | 2.05 ± 0.56 | 2.26 ± 0.7 | 2.16 ± 0.76 | p = 0.598 |
| Median | 1.96 | 2.15 | 2.12 | ||
| Quartiles | 1.6–2.3 | 1.61–2.75 | 1.6–2.31 | ||
| Parameters | Angle Class | p | |||
|---|---|---|---|---|---|
| I Class | II Class | III Class | |||
| Length of gait line—left LL [mm] | Av ± SD | 220.13 ± 18.87 | 223.07 ± 15.38 | 219.03 ± 17.29 | p = 0.596 |
| Median | 217.5 | 220.5 | 218.5 | ||
| Quartiles | 204.75–234.75 | 213.25–234 | 211–230.75 | ||
| Length of gait line—right LL [mm] | Av ± SD | 278.63 ± 327.49 | 220.6 ± 16.46 | 214.03 ± 22.45 | p = 0.407 |
| Median | 217 | 220 | 213 | ||
| Quartiles | 207.25–227.5 | 210.5–228.25 | 199.25–226.75 | ||
| Forefoot weight-bearing distribution— left LL [%] | Av ± SD | 64.13 ± 5.18 | 63.07 ± 5.2 | 65.03 ± 4.73 | p = 0.447 |
| Median | 64.5 | 63 | 64 | ||
| Quartiles | 61.25–67 | 61–66 | 62–67 | ||
| Forefoot weight-bearing distribution— right LL [%] | Av ± SD | 64.73 ± 5.24 | 63.63 ± 5.66 | 64.4 ± 5.27 | p = 0.876 |
| Median | 65.5 | 64.5 | 63.5 | ||
| Quartiles | 61.25–67.75 | 61–66.75 | 61–67 | ||
| Hindfoot weight-bearing distribution— left LL [%] | Av ± SD | 35.87 ± 5.18 | 36.93 ± 5.2 | 34.97 ± 4.73 | p = 0.447 |
| Median | 35.5 | 37 | 36 | ||
| Quartiles | 33–38.75 | 34–39 | 33–38 | ||
| Hindfoot weight-bearing distribution— right LL [%] | Av ± SD | 35.27 ± 5.24 | 36.37 ± 5.66 | 35.6 ± 5.27 | p = 0.876 |
| Median | 34.5 | 35.5 | 36.5 | ||
| Quartiles | 32.25–38.75 | 33.25–39 | 33–39 | ||
| Medial weight-bearing distribution— left LL [%] | Av ± SD | 48.63 ± 6.29 | 50.97 ± 5.67 | 47.77 ± 7.47 | p = 0.235 |
| Median | 49.5 | 50.5 | 49 | ||
| Quartiles | 43.5–52.75 | 47–54 | 42.25–53.5 | ||
| Lateral weight-bearing distribution— left LL [%] | Av ± SD | 51.37 ± 6.29 | 49.03 ± 5.61 | 52.23 ± 7.39 | p = 0.193 |
| Median | 50.5 | 49.5 | 51 | ||
| Quartiles | 47.25–56.5 | 46–53 | 48–57.75 | ||
| Medial weight-bearing distribution— right LL [%] | Av ± SD | 49.7 ± 5.39 | 52.03 ± 6.09 | 49.97 ± 6.3 | p = 0.315 |
| Median | 49.5 | 52.5 | 51 | ||
| Quartiles | 45.25–54 | 48.25–55 | 45–54.75 | ||
| Lateral weight-bearing distribution— right LL [%] | Av ± SD | 50.3 ± 5.39 | 47.97 ± 6.07 | 50.03 ± 6.29 | p = 0.372 |
| Median | 50.5 | 47.5 | 49 | ||
| Quartiles | 46–54.75 | 45–51.75 | 45.25–55 | ||
| Mean foot propulsion rate— left foot [mm/s] | Av ± SD | 779.43 ± 128.84 | 773.31 ± 101.8 | 841.76 ± 355.66 | p = 0.937 |
| Median | 748.08 | 783.92 | 796.84 | ||
| Quartiles | 702.19–821.66 | 709.22–844.64 | 663.34–855.16 | ||
| Mean foot propulsion rate— right foot [mm/s] | Av ± SD | 778.03 ± 179.68 | 792.8 ± 172.79 | 792.89 ± 120 | p = 0.213 |
| Median | 745.1 | 756.32 | 805.33 | ||
| Quartiles | 700.04–816.92 | 710.55–852.4 | 735.35–888.61 | ||
| Mean foot pressure— left foot [kg] | Av ± SD | 45.16 ± 9.79 | 45.6 ± 9.27 | 46.76 ± 10.9 | p = 0.844 |
| Median | 45.22 | 43.12 | 46.44 | ||
| Quartiles | 37.88–50.2 | 40.01–51.88 | 39.89–50.13 | ||
| Mean foot pressure— right foot [kg] | Av ± SD | 44.94 ± 9.93 | 45.42 ± 8.97 | 46.71 ± 10.91 | p = 0.878 |
| Median | 45.19 | 43.42 | 45.52 | ||
| Quartiles | 36.42–50.24 | 40.56–51.44 | 39.42–50.55 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, M.; Golec, J.; Wieczorek, A.; Golec, P. Is There a Correlation between Dental Occlusion, Postural Stability and Selected Gait Parameters in Adults? Int. J. Environ. Res. Public Health 2023, 20, 1652. https://doi.org/10.3390/ijerph20021652
Nowak M, Golec J, Wieczorek A, Golec P. Is There a Correlation between Dental Occlusion, Postural Stability and Selected Gait Parameters in Adults? International Journal of Environmental Research and Public Health. 2023; 20(2):1652. https://doi.org/10.3390/ijerph20021652
Chicago/Turabian StyleNowak, Monika, Joanna Golec, Aneta Wieczorek, and Piotr Golec. 2023. "Is There a Correlation between Dental Occlusion, Postural Stability and Selected Gait Parameters in Adults?" International Journal of Environmental Research and Public Health 20, no. 2: 1652. https://doi.org/10.3390/ijerph20021652
APA StyleNowak, M., Golec, J., Wieczorek, A., & Golec, P. (2023). Is There a Correlation between Dental Occlusion, Postural Stability and Selected Gait Parameters in Adults? International Journal of Environmental Research and Public Health, 20(2), 1652. https://doi.org/10.3390/ijerph20021652