
The Impact of a Six-Year Existing Screening Programme Using the Faecal Immunochemical Test in Flanders (Belgium) on Colorectal Cancer Incidence, Mortality and Survival: A Population-Based Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Flemish Organised CRC Screening Programme
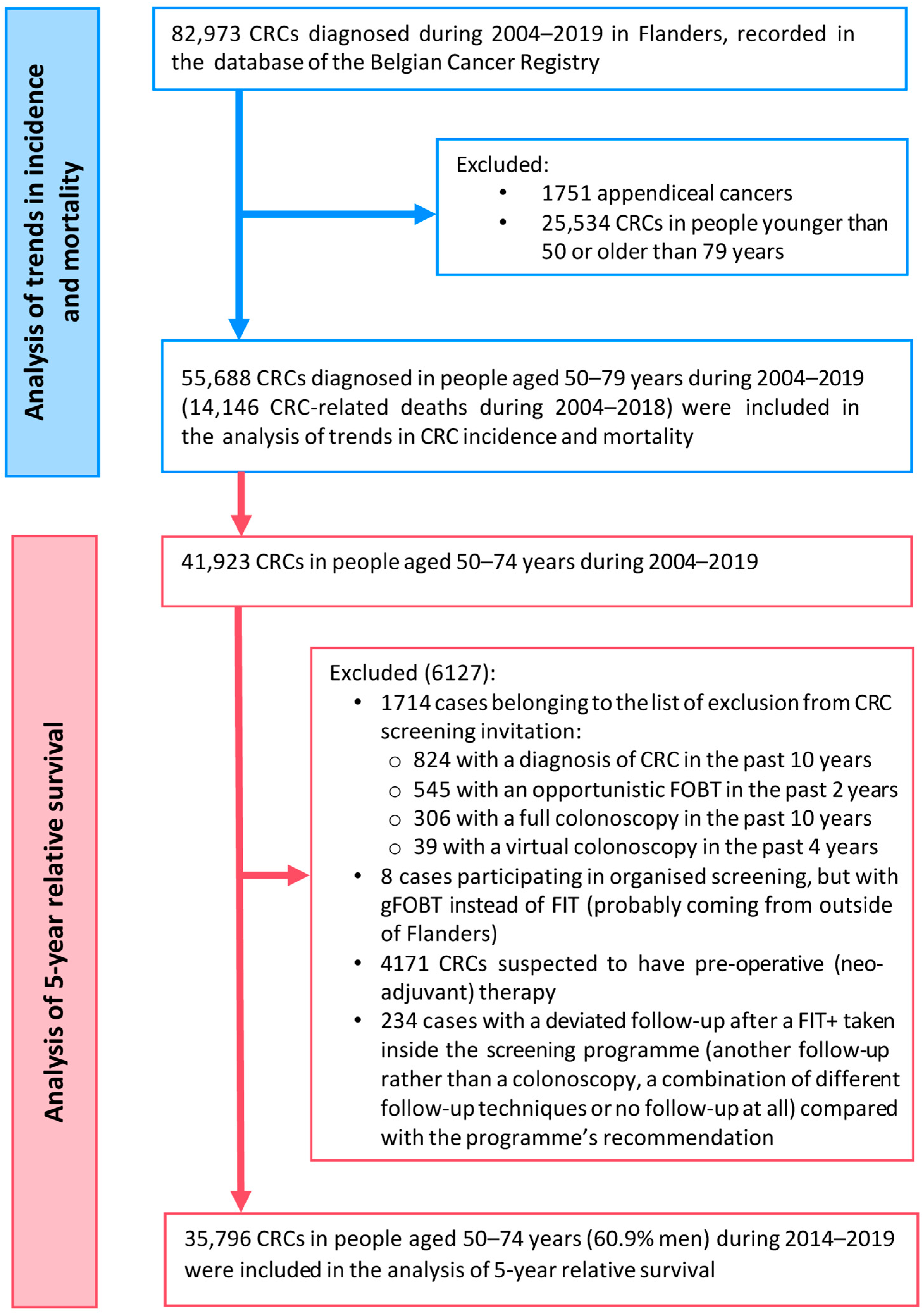
2.2. Study Design, Outcomes and Study Populations
2.3. Data Sources
2.4. Statistical Analysis
2.4.1. Sample Size
2.4.2. Missing Data
2.4.3. Main Analysis
2.5. Privacy and Ethics
3. Results
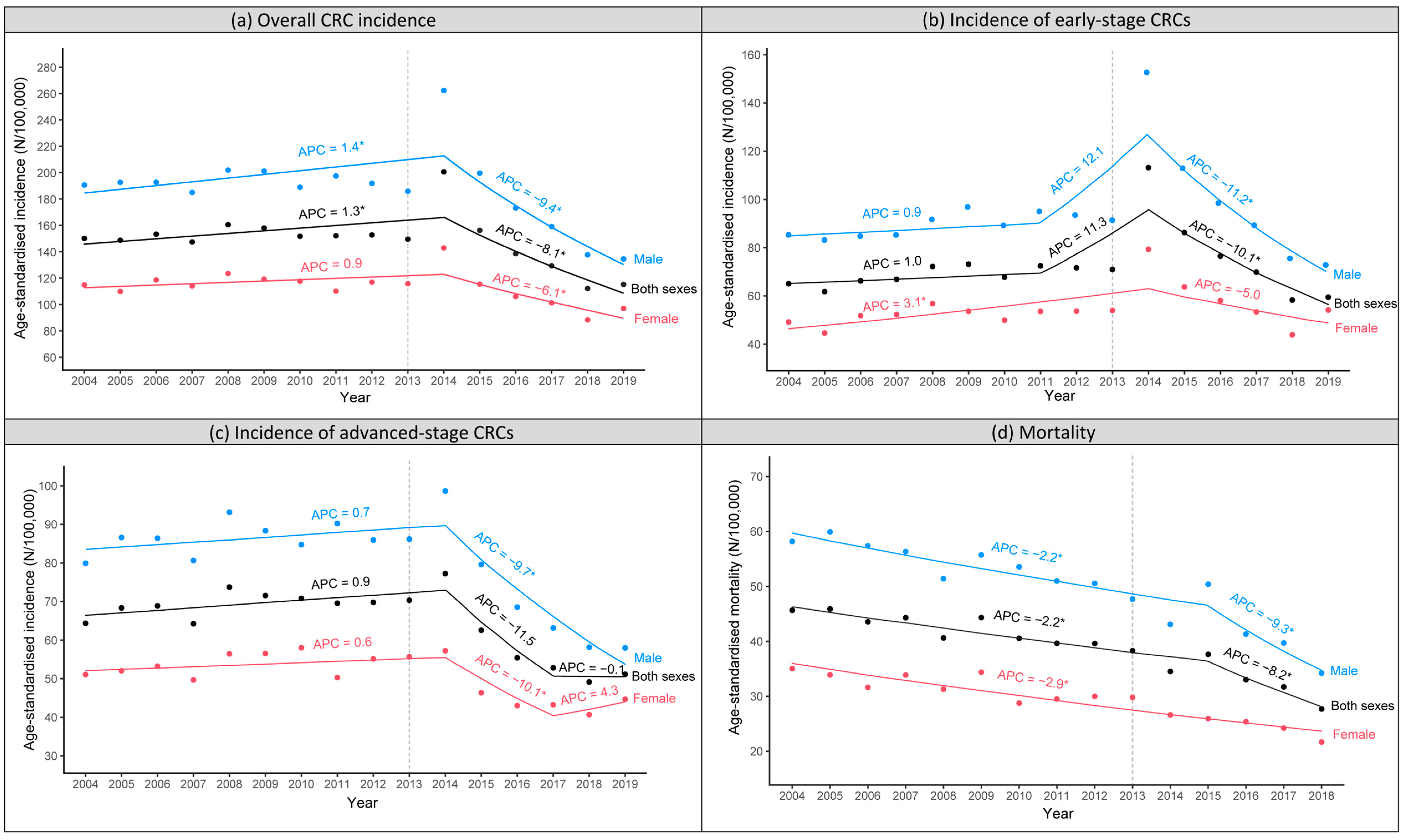
3.1. Trends of CRC Incidence and Mortality by Gender
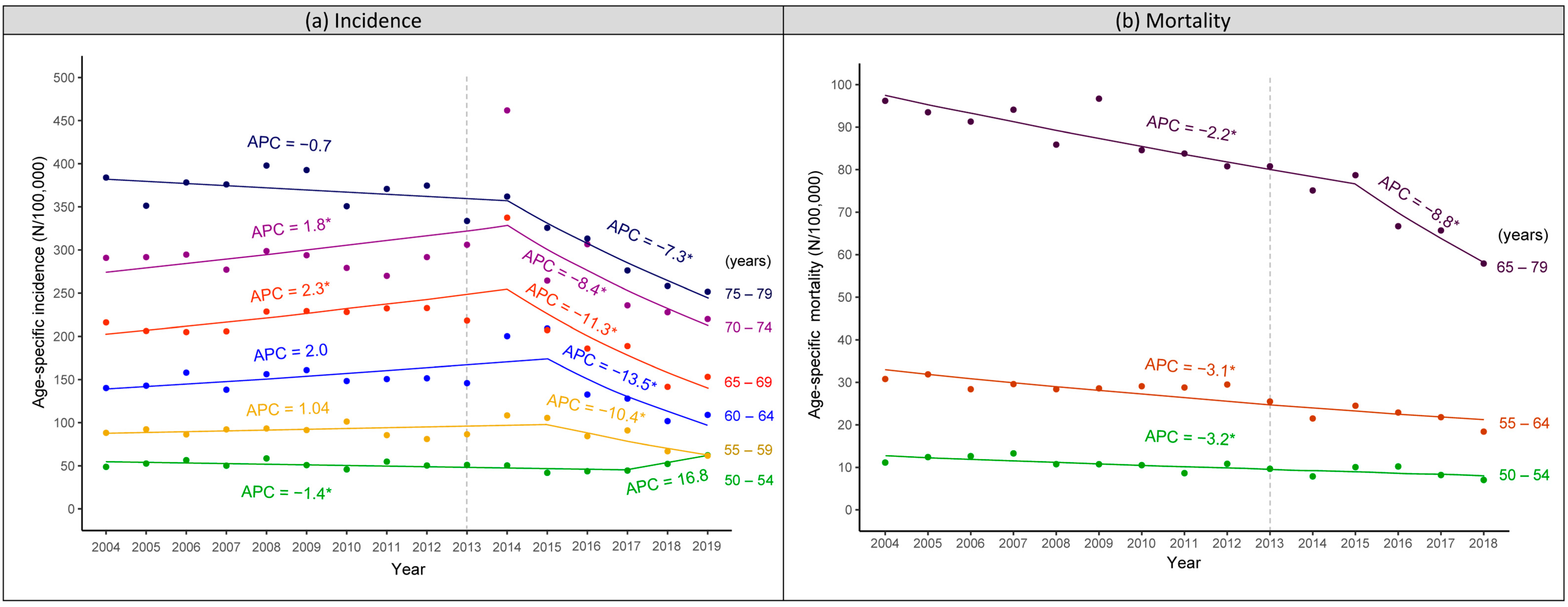
3.2. Trends of CRC Incidence and Mortality by Age Group
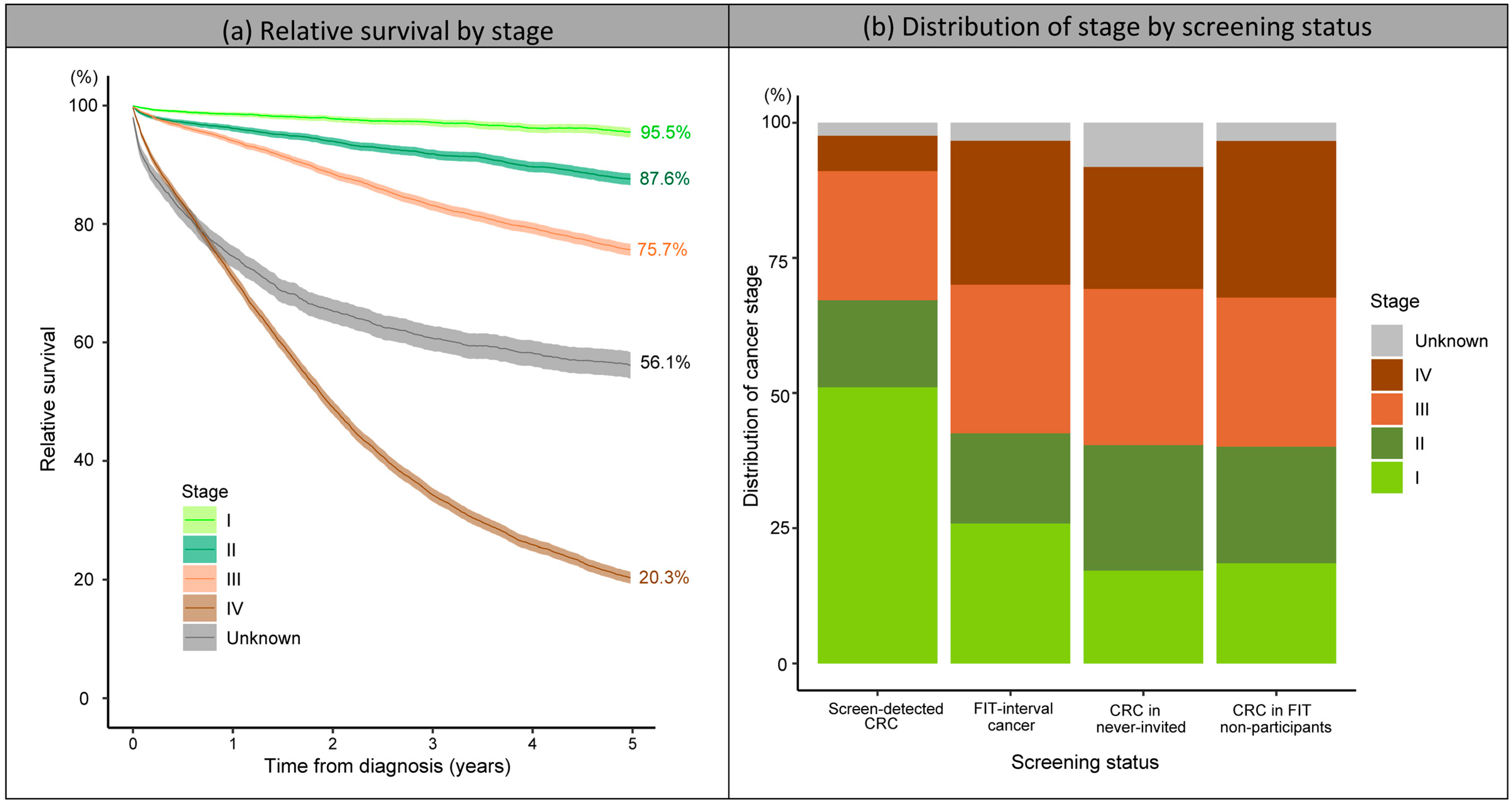
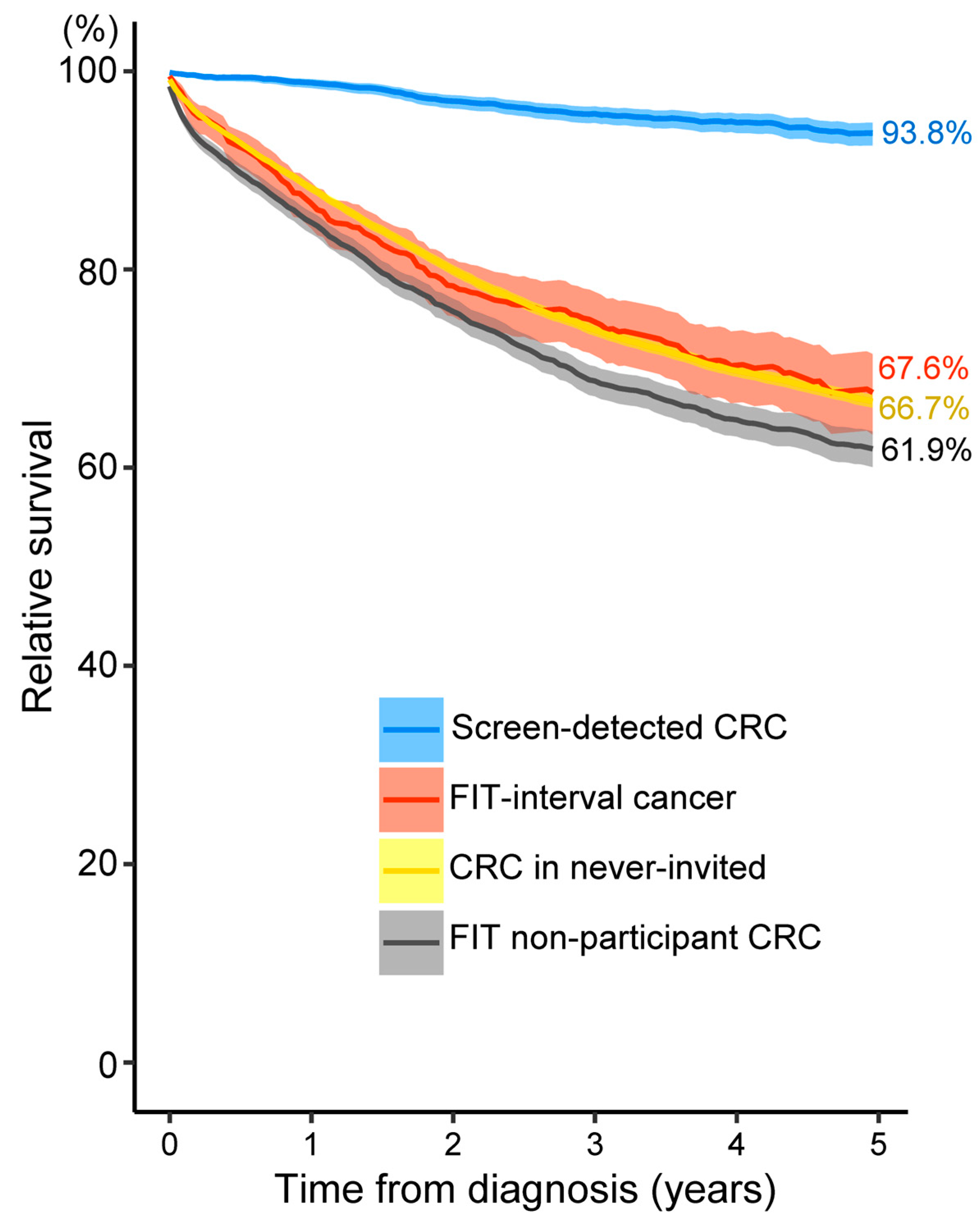
3.3. Relative Survival by Screening Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belgian Cancer Registry. Cancer Fact Sheet Colorectal Cancer: Belgium 2020. Available online: https://kankerregister.org/media/docs/CancerFactSheets/2020/Cancer_Fact_Sheet_ColorectalCancer_2020.pdf (accessed on 6 January 2023).
- Morson, B.C. The evolution of colorectal carcinoma. Clin. Radiol. 1984, 35, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.B.; Njor, S.; Ingeholm, P.; Andersen, B. Effectiveness of Colorectal Cancer Screening in Detecting Earlier-Stage Disease-A Nationwide Cohort Study in Denmark. Gastroenterology 2018, 155, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Helsingen, L.M.; Kalager, M. Colorectal Cancer Screening—Approach, Evidence, and Future Directions. NEJM Evid. 2022, 1. [Google Scholar] [CrossRef]
- Ponti, A.; Anttila, A.; Ronco, G.; Senore, C.; Basu, P.; Segnan, N.; Tomatis, M.; Žakelj, M.P.; Dillner, J.; Fernan, M.; et al. Cancer Screening in the European Union. Report on the implementation of Council Recommendation on Cancer Screening; European Commission: Brussels, Belgium, 2017. [Google Scholar]
- Mandel, J.S.; Bond, J.H.; Church, T.R.; Snover, D.C.; Bradley, G.M.; Schuman, L.M.; Ederer, F. Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N. Engl. J. Med. 1993, 328, 1365–1371. [Google Scholar] [CrossRef] [Green Version]
- Hardcastle, J.D.; Chamberlain, J.O.; Robinson, M.H.E.; Moss, S.M.; Amar, S.S.; Balfour, T.W.; James, P.D.; Mangham, C.M. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 1996, 348, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Tinmouth, J.; Lansdorp-Vogelaar, I.; Allison, J.E. Faecal immunochemical tests versus guaiac faecal occult blood tests: What clinicians and colorectal cancer screening programme organisers need to know. Gut 2015, 64, 1327–1337. [Google Scholar] [CrossRef]
- Keys, M.T.; Serra-Burriel, M.; Martinez-Lizaga, N.; Pellise, M.; Balaguer, F.; Sanchez, A.; Bernal-Delgado, E.; Castells, A. Population-based organized screening by faecal immunochemical testing and colorectal cancer mortality: A natural experiment. Int. J. Epidemiol. 2021, 50, 143–155. [Google Scholar] [CrossRef]
- Breekveldt, E.C.H.; Lansdorp-Vogelaar, I.; Toes-Zoutendijk, E.; Spaander, M.C.W.; van Vuuren, A.J.; van Kemenade, F.J.; Ramakers, C.R.B.; Dekker, E.; Nagtegaal, I.D.; Krul, M.F.; et al. Colorectal cancer incidence, mortality, tumour characteristics, and treatment before and after introduction of the faecal immunochemical testing-based screening programme in the Netherlands: A population-based study. Lancet Gastroenterol. Hepatol. 2021, 7, 60–68. [Google Scholar] [CrossRef]
- Levin, T.R.; Corley, D.A.; Jensen, C.D.; Schottinger, J.E.; Quinn, V.P.; Zauber, A.G.; Lee, J.K.; Zhao, W.K.; Udaltsova, N.; Ghai, N.R.; et al. Effects of Organized Colorectal Cancer Screening on Cancer Incidence and Mortality in a Large Community-Based Population. Gastroenterology 2018, 155, 1383–1391.e5. [Google Scholar] [CrossRef]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Gini, A.; Jansen, E.E.L.; Zielonke, N.; Meester, R.G.S.; Senore, C.; Anttila, A.; Segnan, N.; Mlakar, D.N.; de Koning, H.J.; Lansdorp-Vogelaar, I.; et al. Impact of colorectal cancer screening on cancer-specific mortality in Europe: A systematic review. Eur. J. Cancer 2020, 127, 224–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, R.; Guo, F.; Heisser, T.; Hackl, M.; Ihle, P.; De Schutter, H.; Van Damme, N.; Valerianova, Z.; Atanasov, T.; Májek, O.; et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: An international population-based study. Lancet Oncol. 2021, 22, 1002–1013. [Google Scholar] [CrossRef] [PubMed]
- Centre for Cancer Detection. Monitoring Report 2021 of the Flemish Colorectal Cancer Screening Programme. Available online: https://dikkedarmkanker.bevolkingsonderzoek.be/nl (accessed on 5 May 2022).
- Van Eycken, L.; Haustermans, K. Current role and future perspectives of the Belgian Cancer Registry in quality of cancer projects. Belg. J. Med. Oncol. 2010, 4, 216–222. [Google Scholar]
- International Union Against Cancer (UICC). TNM Classification of Malignant Tumours, 6th ed.; Sobin, L.H., Wittekind, C., Eds.; Wiley: New York, NY, USA, 2002. [Google Scholar]
- International Union Against Cancer (UICC). TNM Classification of Malignant Tumours, 7th ed.; Sobin, L.H., Gospodarowicz, M.K., Wittekind, C., Eds.; Wiley-Blackwell: Chichester, UK, 2009. [Google Scholar]
- International Union Against Cancer (UICC). TNM Classification of Malignant Tumours, 8th ed.; Brierley, J.D., Gospodarowicz, M.K., Wittekind, C., Eds.; John Wiley & Sons: Oxford, UK; Hoboken, NJ, USA, 2017. [Google Scholar]
- Statbel (Belgium in Figures). Life Expectancy and Life Tables [Sterftetafels en Levensverwachting]. Available online: https://statbel.fgov.be/en/themes/population/mortality-life-expectancy-and-causes-death/life-expectancy-and-life-tables#figures (accessed on 10 March 2022).
- Committee for the Protection of Privacy (Commissie voor de Bescherming van de Persoonlijke Levenssfeer). SCSZG/18/064. Available online: https://www.ehealth.fgov.be/ehealthplatform/file/view/AWJNUKfuJW4b-4n3_A_Z?filename=13-091-n064-bevolkingsonderzoek%20dikkedarmkanker-gewijzigd%20op%2020%20maart%2020....pdf (accessed on 2 September 2022).
- eHealth. Informatieveiligheidscomité (Information Security Committee). Available online: https://www.ehealth.fgov.be/ehealthplatform/nl/informatieveiligheidscomite (accessed on 9 November 2022).
- Crossroads Bank for Social Security (CBSS). Documentation. Available online: https://www.ksz-bcss.fgov.be/nl/documents-list (accessed on 15 May 2022).
- Belgian Cancer Registry. Cancer Survival in Belgium. Available online: https://kankerregister.org/media/docs/publications/CancerSurvivalinBelgium.PDF (accessed on 15 May 2022).
- Ederer, F.; Axtell, L.M.; Cutler, S.J. The relative survival rate: A statistical methodology. Natl. Cancer Inst. Monogr. 1961, 6, 101–121. [Google Scholar] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, H.M.; Jen, G.H.; Wang, Y.W.; Fann, J.C.; Hsu, C.Y.; Jeng, Y.C.; Yen, A.M.; Chiu, S.Y.; Chen, S.L.; Hsu, W.F.; et al. Long-term effectiveness of faecal immunochemical test screening for proximal and distal colorectal cancers. Gut 2021, 70, 2321–2329. [Google Scholar] [CrossRef]
- Giorgi Rossi, P.; Vicentini, M.; Sacchettini, C.; Di Felice, E.; Caroli, S.; Ferrari, F.; Mangone, L.; Pezzarossi, A.; Roncaglia, F.; Campari, C.; et al. Impact of Screening Program on Incidence of Colorectal Cancer: A Cohort Study in Italy. Am. J. Gastroenterol. 2015, 110, 1359–1366. [Google Scholar] [CrossRef]
- Mar, J.; Arrospide, A.; Larranaga, I.; Iruretagoiena, M.L.; Imaz, L.; Gorostiza, A.; Ibarrondo, O. Impact of an organised population screening programme for colorectal cancer: Measurement after first and second rounds. J. Med. Screen 2021, 28, 122–130. [Google Scholar] [CrossRef]
- Tepes, B.; Mlakar, D.N.; Stefanovic, M.; Stabuc, B.; Grazio, S.F.; Zakotnik, J.M. The impact of 6 years of the National Colorectal Cancer Screening Program on colorectal cancer incidence and 5-year survival. Eur. J. Cancer Prev. 2021, 30, 304–310. [Google Scholar] [CrossRef]
- Parente, F.; Vailati, C.; Boemo, C.; Bonoldi, E.; Ardizzoia, A.; Ilardo, A.; Tortorella, F.; Cereda, D.; Cremaschini, M.; Moretti, R. Improved 5-year survival of patients with immunochemical faecal blood test-screen-detected colorectal cancer versus non-screening cancers in northern Italy. Dig. Liver Dis. 2015, 47, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Idigoras Rubio, I.; Arana-Arri, E.; Portillo Villares, I.; Bilbao Iturribarrria, I.; Martinez-Indart, L.; Imaz-Ayo, N.; de la Cruz, M.; de Castro, V.; Lopez de Munain, A.; Torrejon Perez, I.; et al. Participation in a population-based screening for colorectal cancer using the faecal immunochemical test decreases mortality in 5 years. Eur. J. Gastroenterol. Hepatol. 2019, 31, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Analysis of Bowel Cancer Outcomes for the National Bowel Cancer Screening Program. Available online: https://www.aihw.gov.au/reports/cancer-screening/analysis-of-bowel-cancer-outcomes-nbcsp-2018/summary (accessed on 11 April 2022).
- Lee, Y.C.; Hsu, C.Y.; Chen, S.L.; Yen, A.M.; Chiu, S.Y.; Fann, J.C.; Chuang, S.L.; Hsu, W.F.; Chiang, T.H.; Chiu, H.M.; et al. Effects of screening and universal healthcare on long-term colorectal cancer mortality. Int. J. Epidemiol. 2019, 48, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, M.; Fedeli, U.; Schievano, E.; Bovo, E.; Guzzinati, S.; Baracco, S.; Fedato, C.; Saugo, M.; Dei Tos, A.P. Impact on colorectal cancer mortality of screening programmes based on the faecal immunochemical test. Gut 2015, 64, 784–790. [Google Scholar] [CrossRef]
- Welch, H.G.; Robertson, D.J. Colorectal Cancer on the Decline--Why Screening Can’t Explain It All. N. Engl. J. Med. 2016, 374, 1605–1607. [Google Scholar] [CrossRef]
- Ventura, L.; Mantellini, P.; Grazzini, G.; Castiglione, G.; Buzzoni, C.; Rubeca, T.; Sacchettini, C.; Paci, E.; Zappa, M. The impact of immunochemical faecal occult blood testing on colorectal cancer incidence. Dig. Liver Dis. 2014, 46, 82–86. [Google Scholar] [CrossRef]
- Chiu, H.M.; Chen, S.L.; Yen, A.M.; Chiu, S.Y.; Fann, J.C.; Lee, Y.C.; Pan, S.L.; Wu, M.S.; Liao, C.S.; Chen, H.H.; et al. Effectiveness of fecal immunochemical testing in reducing colorectal cancer mortality from the One Million Taiwanese Screening Program. Cancer 2015, 121, 3221–3229. [Google Scholar] [CrossRef] [Green Version]
- White, A.; Ironmonger, L.; Steele, R.J.C.; Ormiston-Smith, N.; Crawford, C.; Seims, A. A review of sex-related differences in colorectal cancer incidence, screening uptake, routes to diagnosis, cancer stage and survival in the UK. BMC Cancer 2018, 18, 906. [Google Scholar] [CrossRef] [Green Version]
- Tran, T.N.; Peeters, M.; Hoeck, S.; Van Hal, G.; Janssens, S.; De Schutter, H. Optimizing the colorectal cancer screening programme using faecal immunochemical test (FIT) in Flanders, Belgium from the “interval cancer” perspective. Br. J. Cancer 2022, 126, 1091–1099. [Google Scholar] [CrossRef]
- Chiu, H.M.; Lee, Y.C.; Tu, C.H.; Chen, C.C.; Tseng, P.H.; Liang, J.T.; Shun, C.T.; Lin, J.T.; Wu, M.S. Association between early stage colon neoplasms and false-negative results from the fecal immunochemical test. Clin. Gastroenterol. Hepatol. 2013, 11, 832–838.e2. [Google Scholar] [CrossRef]
- Digby, J.; Fraser, C.G.; Carey, F.A.; Lang, J.; Stanners, G.; Steele, R.J. Interval cancers using a quantitative faecal immunochemical test (FIT) for haemoglobin when colonoscopy capacity is limited. J. Med. Screen 2016, 23, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Steele, R.J.; Stanners, G.; Lang, J.; Brewster, D.H.; Carey, F.A.; Fraser, C.G. Interval cancers in a national colorectal cancer screening programme. United Eur. Gastroenterol. J. 2016, 4, 587–594. [Google Scholar] [CrossRef] [Green Version]
- Selby, K.; Levine, E.H.; Doan, C.; Gies, A.; Brenner, H.; Quesenberry, C.; Lee, J.K.; Corley, D.A. Effect of Sex, Age, and Positivity Threshold on Fecal Immunochemical Test Accuracy: A Systematic Review and Meta-analysis. Gastroenterology 2019, 157, 1494–1505. [Google Scholar] [CrossRef] [Green Version]
- Imperiale, T.F.; Ransohoff, D.F.; Itzkowitz, S.H.; Levin, T.R.; Lavin, P.; Lidgard, G.P.; Ahlquist, D.A.; Berger, B.M. Multitarget stool DNA testing for colorectal-cancer screening. N. Engl. J. Med. 2014, 370, 1287–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, A.; Neefs, I.; Hoeck, S.; Peeters, M.; Van Hal, G. Towards Novel Non-Invasive Colorectal Cancer Screening Methods: A Comprehensive Review. Cancers 2021, 13, 1820. [Google Scholar] [CrossRef] [PubMed]
- Ibanez-Sanz, G.; Mila, N.; Vidal, C.; Rocamora, J.; Moreno, V.; Sanz-Pamplona, R.; Garcia, M. Positive impact of a faecal-based screening programme on colorectal cancer mortality risk. PLoS ONE 2021, 16, e0253369. [Google Scholar] [CrossRef]
- Gutierrez-Stampa, M.A.; Aguilar, V.; Sarasqueta, C.; Cubiella, J.; Portillo, I.; Bujanda, L. Colorectal Cancer Survival in 50- to 69-Year-Olds after Introducing the Faecal Immunochemical Test. Cancers 2020, 12, 2412. [Google Scholar] [CrossRef]
- Li, X.; Zhou, Y.; Luo, Z.; Gu, Y.; Chen, Y.; Yang, C.; Wang, J.; Xiao, S.; Sun, Q.; Qian, M.; et al. The impact of screening on the survival of colorectal cancer in Shanghai, China: A population based study. BMC Public Health 2019, 19, 1016. [Google Scholar] [CrossRef]
- Mengual-Ballester, M.; Pellicer-Franco, E.; Valero-Navarro, G.; Soria-Aledo, V.; Garcia-Marin, J.A.; Aguayo-Albasini, J.L. Increased survival and decreased recurrence in colorectal cancer patients diagnosed in a screening programme. Cancer Epidemiol. 2016, 43, 70–75. [Google Scholar] [CrossRef]
- McClements, P.L.; Madurasinghe, V.; Thomson, C.S.; Fraser, C.G.; Carey, F.A.; Steele, R.J.; Lawrence, G.; Brewster, D.H. Impact of the UK colorectal cancer screening pilot studies on incidence, stage distribution and mortality trends. Cancer Epidemiol. 2012, 36, e232–e242. [Google Scholar] [CrossRef]
- Vicentini, M.; Zorzi, M.; Bovo, E.; Mancuso, P.; Zappa, M.; Manneschi, G.; Mangone, L.; Giorgi Rossi, P.; Colorectal Cancer Screening IMPATTO study working group. Impact of screening programme using the faecal immunochemical test on stage of colorectal cancer: Results from the IMPATTO study. Int. J. Cancer 2019, 145, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Shrank, W.H.; Patrick, A.R.; Brookhart, M.A. Healthy user and related biases in observational studies of preventive interventions: A primer for physicians. J. Gen. Intern. Med. 2011, 26, 546–550. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroup | Definition |
|---|---|
| Screen-detected CRC | CRC diagnosed after a FIT+ result, within six months after the first follow-up colonoscopy and before the next recommended FIT invitation (24 months). |
| FIT-interval cancer | CRC diagnosed after a negative FIT result and before the next recommended FIT invitation (24 months). |
| Post-colonoscopy CRC after a FIT+ | CRC diagnosed after a FIT+ result but later than six months after the first follow-up colonoscopy and before the next recommended colonoscopy examination (10 years, 4 years and 2 years for a complete, virtual and incomplete colonoscopy, respectively). |
| CRC in FIT non-participant | CRC diagnosed but no FIT participation recorded after screening invitation. |
| CRC in never-invited * |
|
| Screen-Detected CRC (N = 4959) | FIT-Interval Cancer (N = 905) | CRC in Never-Invited (N = 25,353) | FIT Non-Participant CRC (N = 4555) | |
|---|---|---|---|---|
| Men | 3157 (63.7%) | 468 (51.7%) | 15,298 (60.3%) | 2854 (62.7%) |
| Mean age (years) ± SD | 65.7 ± 5.8 | 66.5 ± 5.4 | 64.4 ± 6.9 | 66.2 ± 5.6 |
| Stage | ||||
| • I | 2532 (51.0%) | 234 (25.9%) | 4352 (17.2%) | 845 (18.6%) |
| • II | 799 (16.1%) | 151 (16.7%) | 5880 (23.2%) | 980 (21.5%) |
| • III | 1185 (23.9%) | 249 (27.5%) | 7325 (28.9%) | 1257 (27.6%) |
| • IV | 325 (6.6%) | 241 (26.6%) | 5723 (22.6%) | 1321 (29.0%) |
| • Unknown | 118 (2.4%) | 30 (3.3%) | 2073 (8.2%) | 152 (3.3%) |
| Mean time between FIT and diagnosis (days) | 77.9 | 425.0 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, T.N.; Hoeck, S.; De Schutter, H.; Janssens, S.; Peeters, M.; Van Hal, G. The Impact of a Six-Year Existing Screening Programme Using the Faecal Immunochemical Test in Flanders (Belgium) on Colorectal Cancer Incidence, Mortality and Survival: A Population-Based Study. Int. J. Environ. Res. Public Health 2023, 20, 1654. https://doi.org/10.3390/ijerph20021654
Tran TN, Hoeck S, De Schutter H, Janssens S, Peeters M, Van Hal G. The Impact of a Six-Year Existing Screening Programme Using the Faecal Immunochemical Test in Flanders (Belgium) on Colorectal Cancer Incidence, Mortality and Survival: A Population-Based Study. International Journal of Environmental Research and Public Health. 2023; 20(2):1654. https://doi.org/10.3390/ijerph20021654
Chicago/Turabian StyleTran, Thuy Ngan, Sarah Hoeck, Harlinde De Schutter, Sharon Janssens, Marc Peeters, and Guido Van Hal. 2023. "The Impact of a Six-Year Existing Screening Programme Using the Faecal Immunochemical Test in Flanders (Belgium) on Colorectal Cancer Incidence, Mortality and Survival: A Population-Based Study" International Journal of Environmental Research and Public Health 20, no. 2: 1654. https://doi.org/10.3390/ijerph20021654
APA StyleTran, T. N., Hoeck, S., De Schutter, H., Janssens, S., Peeters, M., & Van Hal, G. (2023). The Impact of a Six-Year Existing Screening Programme Using the Faecal Immunochemical Test in Flanders (Belgium) on Colorectal Cancer Incidence, Mortality and Survival: A Population-Based Study. International Journal of Environmental Research and Public Health, 20(2), 1654. https://doi.org/10.3390/ijerph20021654