

Physical Activity and Sleep Quality Association in Different Populations: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search
2.2. Eligibility Criteria
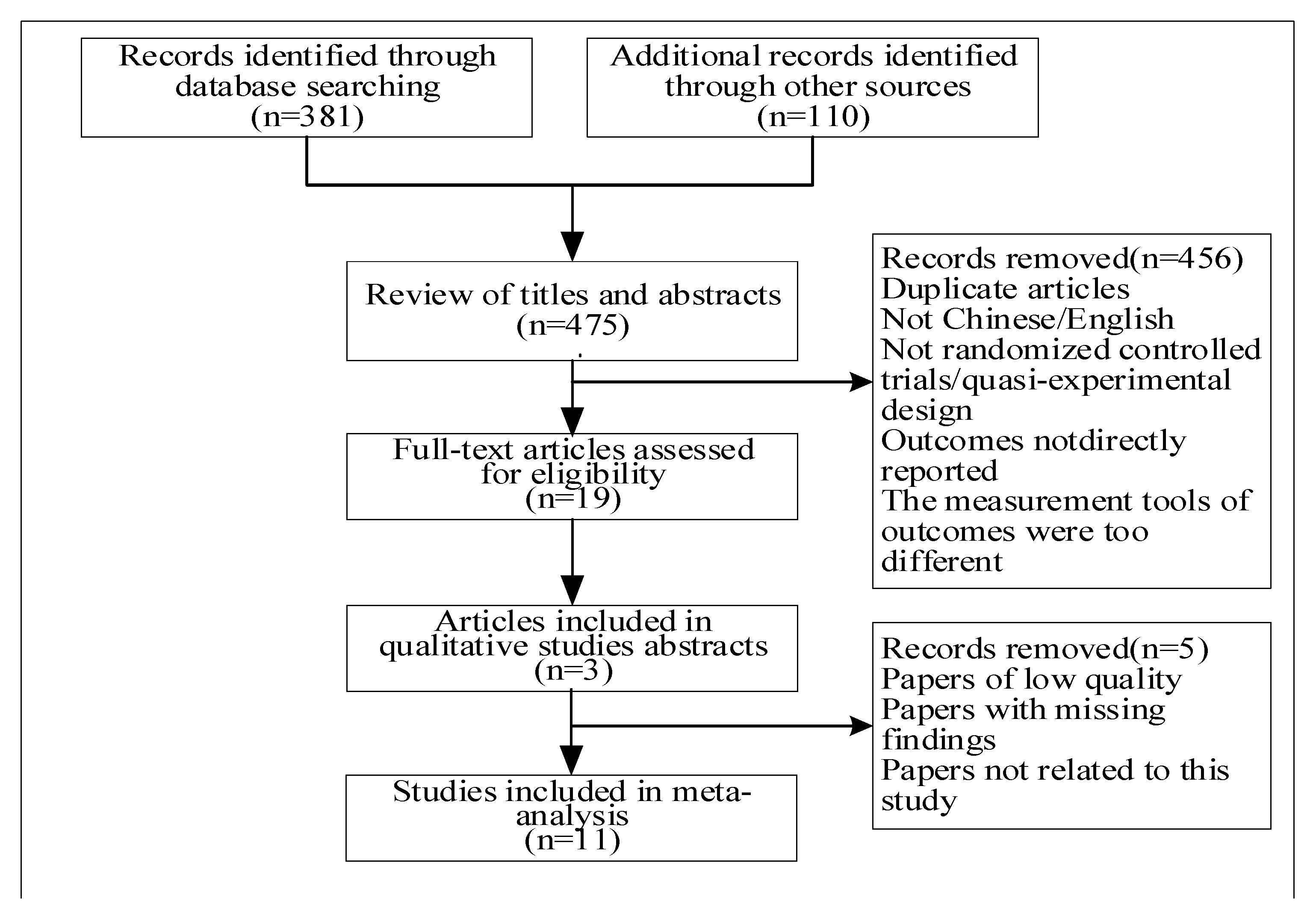
2.3. Study Selection and Extraction
2.4. Study Quality Assessment
2.5. Quantitative Data Analysis
3. Results
3.1. Study Characteristics
3.2. The Overall Effect of Physical Activity on Sleep Quality
3.3. Regulating the Variable Subgroup Analysis
- Intensity of physical activity: As some of the included literature did not classify the intensity of physical activity, only five articles of this moderating variable were included (two articles of low intensity, two articles of medium intensity and one article of high intensity). The 5 papers involved 3 groups of physical activity intensity (low-intensity, Moderate-intensity, high-intensity), with different intensities showing moderate heterogeneity regarding the effect size (I2 = 37.8%). Moderate-intensity physical activity had a larger effect size (d = 2.56, p = 0.015) regarding improving sleep quality, followed by low-intensity physical activity (d = 1.38, p = 0.03), and high-intensity physical activity had the lowest effect size (d = 1.12, p = 0.32).
- Age stage: According to the characteristics of different age stages in the included literature, the ages were divided into three stages: children (3–12 years), youth (13–35 years), and middle and old age (36–<60 years). The sample size of 1 study design was children and 8 studies involved young people (middle school students, college students and young people). Physical activity had a large effect size on the sleep quality of children and middle-aged and elderly people, and the effect was obvious (children: d = 1.24, p = 0.03; middle-aged and elderly people: d = 1.98, p = 0.037; young people: no significant effect (d = 1.32, p = 0.11)).
4. Discussion
4.1. Quality of the Included Literature and the Overall Effect Size
4.2. Analysis of the Influence of Moderating Variables of Physical Activity Programs on Sleep Quality
- In terms of the intervention of physical activity intensity, physical activity intensity was taken as a variable, and three sub-variables, namely, low intensity, medium intensity and high intensity, were introduced for the heterogeneity and significance analysis. The results showed that the effect size of the three different intensity groups had moderate heterogeneity (I2 = 37.8%). Moderate-intensity physical activity had a larger effect size (d = 2.56) regarding improving sleep quality (p = 0.015), followed by low intensity (d = 1.38, p = 0.03), and high-intensity physical activity had the lowest effect size (d = 1.12, p = 0.32).
- In terms of age, according to the different age stages tested, the samples were divided into three age groups: children, young people, and middle-aged and elderly people. The results showed that physical activity had a larger effect on the sleep quality of children and middle-aged and elderly people. Among them, the effect was more obvious in the children group (d = 1.24, p = 0.03), followed by the middle-aged and elderly group (d = 1.98, p = 0.037), but the effect was not significant in the young people group (d = 1.32, p = 0.11).
4.3. An Analysis of the Effects of the Moderating Variables of Physical Activity Programs on Sleep Quality
- Age category: Through statistical tests, it was found that children and middle-aged and elderly people were able to improve the quality of sleep via physical exercise, the effect of which was larger than for young people. Therefore, physical activity had a significant impact on the sleep quality of children and middle-aged and elderly people. However, among the included studies, there were two children and two middle-aged and elderly studies, each accounting for 20% of the total studies. Due to the small number of included studies, the research conclusions may be biased to some extent. Furthermore, the number of included studies and sample size of young people were large, but the effect of physical activity on sleep quality was not significant. This showed that physical activity affected sleep quality differently at different ages. Studies found that the association between physical activity and sleep quality changes with age. Children’s sleep quality problems are related to the developmental changes in the body’s internal clock and the influence of the external social environment. Different forms of physical activity, such as outdoor activities and sports games, can help to regulate the body clock and reduce sleep quality problems caused by social environments, such as noise and a bad mood [35]. Circadian rhythm changes are a major cause of insomnia in middle-aged and older adults. Middle-aged and elderly people who engage in appropriate physical activity can effectively improve their quality of sleep [36]. Young people’s sleep problems are due to study and work pressure, life and rest disorders, long-term mental work and other related factors. However, proper physical activity cannot effectively eliminate long-term mental stress, mental work, and irregular life and rest on the quality of sleep [37]. This result is basically consistent with the research conclusion of K. J. Reid et al. (2010) [38]. These studies also further confirmed the main reasons for the significant effect of physical activity on children and the middle-aged and elderly.
- Activity intensity type: It was found that moderate- and low-intensity physical activity had larger effect sizes, followed by high-intensity physical activity. The use of the three subgroups of moderating variables included in the literature was basically the same, and the number of samples with moderate intensity was the largest, followed by low intensity and high intensity. The analysis concluded that moderate- and low-intensity physical activity improved sleep quality better than high-intensity physical activity. Studies found that after moderate-to-low-intensity physical activity, certain amounts of sweat are eliminated. The sweating process can reduce orexin levels and concentration. Since orexin has the function of maintaining arousal and participates in the immune response, proper perspiration can reduce the arousal level by reducing the concentration of orexin, thus promoting sleep and improving sleep quality [39]. The research results showing that low- and medium-intensity exercise can effectively improve sleep quality were basically the same as the results of Rubio-Arias and other studies. It was confirmed that moderate- and low-intensity physical activity had a significant effect on improving sleep quality.
4.4. Research Limitations and Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnes, C.M. Working in our sleep: Sleep and self-regulation in organizations. Organ. Psychol. Rev. J. 2012, 2, 234–257. [Google Scholar] [CrossRef]
- Shekleton, J.A.; Flynn-Evans, E.E.; Miller, B.; Epstein, L.J.; Kirsch, D.; Brogna, L.A.; Burke, L.M.; Bremer, E.; Murray, J.M.; Gehrman, P.; et al. Neurobehavioral Performance impairment in insomnia: Relationships with self-reported sleep and daytime functioning. Sleep. J. 2014, 37, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, Z.; Xie, F.; Yu, X. A meta-analysis of self-help cognitive behavioral therapy for insomnia: Efficacy, influencing factors and evidence evaluation. Adv. Psychol. Sci. J. 2016, 24, 173–195. [Google Scholar] [CrossRef]
- Qi, D.; Liu, R.; Wu, X. Investigation of sleep quality and its influencing factors in college students. Mod. Prev. Med. 2007, 34, 875–877. [Google Scholar]
- Irwin, M.R. Why sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 2015, 66, 143. [Google Scholar] [CrossRef] [Green Version]
- Chinese Sleep Research Society: The Sleeping State of Chinese People. Available online: http://www.zgsmyjh.org/nd.jsp?id=777/ (accessed on 21 March 2022).
- Daley, A.; MacArthur, C.; McManus, R.; Stokes-Lampard, H.; Wilson, S.; Roalfe, A.; Mutrie, N. Factors associated with the use of complementary medicine and non-pharmacological interventions in symptomatic menopausal women. Climacteric 2006, 9, 336–346. [Google Scholar] [CrossRef]
- Hu, Y.S. Research Progress of Exercise Therapy Application; People’s Medical Publishing House: Beijing, China, 2010. [Google Scholar]
- Buman, M.; Hekler, E.; Bliwise, D. Modera-tors and Mediators of exercise-induced objective sleep improve-ments in Midlife and older adults with sleep complaints. Health Psychol. J. 2011, 30, 579–587. [Google Scholar] [CrossRef] [Green Version]
- Chaouloff, F. Effects of acute physical exercise on central Serotonergic systems. Med. Sci. Sports. J. 1997, 29, 58–62. [Google Scholar] [CrossRef]
- Krueger, J.; Fang, J.; Hansen, M.K.; Zhang, J.; Obál, F., Jr. Humoral regulation of sleep. News Physiol. Sci. 2008, 35, 189–194. [Google Scholar] [CrossRef]
- Zhao, H. Experimental study on sleep disorder improved by exercise. Zhejiang Sport. Sci. Technol. 2006, 28, 89–92. [Google Scholar]
- Passos, G.S.; Poyares, D.L.; Santana, M.G.; Tufik, S.; de Mello, M.T. Is exercise an Alternative treatment for chronic insomnia. Clinics 2011, 67, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Ding, F.; Xu, J. Clinical analysis of sleep disorders in patients with depression at different ages. Chin. J. Behav. Med. Brain Sci. 2009, 4, 333. (In Chinese) [Google Scholar]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094. [Google Scholar] [CrossRef] [PubMed]
- Ashrafinia, F.; Mirmohammadali, M.; Rajabi, H.; Kazemnejad, A.; Sadeghniiathaghighi, K.; Amelvalizadeh, M.; Chen, H. The effects of Pilates exercise on sleep quality in postpartum women. Bodyw Move Ther. J. 2014, 18, 190–199. [Google Scholar] [CrossRef]
- Rubio-Arias, J.Á.; Marín-Cascales, E.; Ramos-Campo, D.J.; Hernandez, A.V.; Pérez-López, F.R. Effect of exercise on sleep quality and insomnia in middle-aged women: A systematic review and meta-analysis of ran-domized controlled trials. Maturitas 2017, 100, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Lowe, H.; Haddock, G.; Mulligan, L.D.; Gregg, L.; Fuzellier-Hart, A.; Carter, L.; Kyle, S.D. Does exercise improve sleep for adults with insomnia? A systematic review with quality appraisal. Clin. Psychol. Rev. 2019, 68, 1–12. [Google Scholar] [CrossRef]
- Du, S.; Dong, J.; Zhang, H.; Jin, S.; Xu, G.; Liu, Z.; Chen, L.; Yin, H.; Sun, Z. Taichi exercise for self-rat-ed sleep quality in older people: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2015, 52, 368–379. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.; PRISMA-Group. Preferred Reporting Items for Systematic Review and Meta-Analysis protocols (PRISMA) 2015 statement. PLoS Med. J. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altmand, D.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRIS-MA statement for reporting systematic reviews and meta-analysesof studies rather conditioning healthcare interventions: Explanation and elaboration. PLoS Med. J. 2009, 6, 451–460. [Google Scholar]
- Badicu, G. Physical Activity and Sleep Quality in Students of the Faculty of Physical Education and Sport of Braşov, Romania. Sustainability 2018, 10, 2410. [Google Scholar] [CrossRef] [Green Version]
- Dabrowska-Galas, M.; Dabrowska, J. Physical activity improves sleep quality in women. Ginekol. Pol. 2021, 92, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Sarah, D.; Wolfgang, G.; Sutharsan, S.; Taube, C.; Olivier, M.; Mellies, U.; Koerner-Rettberg, C.; Dillenhöfer, S.; Stehling, F.; Welsner, M. Association between habitual physical activity (HPA)and sleep quality in patients with cystic fibrosis. Sleep Breath 2021, 25, 609–615. [Google Scholar]
- Grimaldi-Puyana, M.; Fernández-Batanero, J.M.; Fennell, C.; Sañudo, B. Associations of objectively-assessed smartphone use with physical activity, sedentary behavior, mood, and sleep quality in young adults: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 3499. [Google Scholar] [CrossRef] [PubMed]
- Herring, M.P.; Monroe, D.C.; Kline, C.E.; O’Connor, P.J.; MacDonncha, C. Sleep quality moderates the association between physical activity frequency and feelings of energy and fatigue in adolescents. Eur. Child Adolesc. Psychiatry 2018, 27, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Mahfouz, M.S.; Ali, S.A.; Bahari, A.Y.; Ajeebi, R.E.; Sabei, H.J.; Somaily, S.Y.; Madkhali, Y.A.; Hrooby, R.H.; Shook, R.N. Association between sleep quality and physical activity in Saudi Arabian University students. Nat. Sci. Sleep 2020, 12, 775. [Google Scholar] [CrossRef]
- Mozaffari-Khosravi, H.; Karandish, M.; Hadianfard, A.M.; Azhdari, M.; Sheikhi, L.; Tabatabaie, M.; Shams-Rad, S.; Mirzavandi, F.; Babaie, S. The relationship between sleep quality and breakfast, mid-morning snack, and dinner and physical activity habits among adolescents: A cross-sectional study in Yazd, Iran. Sleep Biol. Rhythm. 2021, 19, 79–84. [Google Scholar] [CrossRef]
- Osailan, A.M.; Elnaggar, R.K.; Alsubaie, S.F.; Alqahtani, B.A.; Abdelbasset, W.K. The association between cardiorespiratory fitness and reported physical activity with sleep quality in apparently healthy adults: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 4263. [Google Scholar] [CrossRef]
- Štefan, L.; Vrgoč, G.; Rupčić, T.; Sporiš, G.; Sekulić, D. Sleep duration and sleep quality are associated with physical activity in elderly people living in nursing homes. Int. J. Environ. Res. Public Health 2018, 15, 2512. [Google Scholar] [CrossRef] [Green Version]
- Wunsch, K.; Kasten, N.; Fuchs, R. The effect of physical activity on sleep quality, well-being, and affect in academic stress periods. Nat. Sci. Sleep 2017, 9, 117. [Google Scholar] [CrossRef] [Green Version]
- St Laurent, C.W.; Burkart, S.; Rodheim, K.; Marcotte, R.; Spencer, R.M.C. Cross-sectional associations of 24-hour sedentary time, physical activity, and sleep duration compositions with sleep quality and habits in preschoolers. Int. J. Environ. Res. Public Health 2020, 17, 7148. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum. M: Hillsdale, MI, USA, 1988. [Google Scholar]
- Zhang, L.; Lin, Y.C. Moderating and mediating variables in experimental research. Manag. Sci. 2011, 24, 108–111. [Google Scholar]
- Wang, G.H.; Jiang, F. Adolescent sleep health and common sleep disorders. Chin. J. Pediatr. 2019, 57, 733–736. (In Chinese) [Google Scholar]
- Yang, P.Y.; Ho, K.H.; Chen, H.C.; Chien, M.Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: A systematic review. J. Physiother. 2012, 58, 157–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Q.-F.; Meng, Y.-q.; Qin, B. Sleep quality and its Effect on health-related quality of life in Jiangbei New District, Nanjing. J. Pract. Prev. Med. 2022, 9, 1510–1514. [Google Scholar]
- Reid, K.J.; Baron, K.G.; Lu, B.; Naylor, E.; Wolfe, L.; Zee, P.C. Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. Sleep Med. 2010, 11, 934–940. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.O.; Lee, J.B.; Min, Y.K.; Yang, H.M. Heat acclimation affects Circulation levels of prostaglandin E2, COX-2and orexin in Humans. Neurosci. Lett. 2013, 542, 17–20. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Inclusion Criteria | Randomly Assigned | Allocation Concealment | Baseline Similarity | Subject Blinded | Blinding the Intervention Implementers | Blinding the Outcome Measure | At Least One Measurement | Intention-to-Treat Analysis | Statistical Report of En Groups | Results Point Measurements and Variation Measurements | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Badicu, G. (2018) [22] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Dabrowska-Galas, M. (2021) [23] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Dietz-Terjung, S. (2021) [24] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 6 |
| Grimaldi-Puyana, M.(2020) [25] | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Herring, M.P. (2018) [26] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Mahfouz, M.S. (2020) [27] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Mozaffari-Khosravi, H (2021) [28] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Osailan A.M. (2021) [29] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Stefan L. (2018) [30] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 6 |
| Wunsch, K. (2017) [31] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| W.St.Laurent, C. (2020) [32] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Reference | Study Location | Sample Size | Participants | Age (M ± SD) | % Female | Sleep Measure | p-Value |
|---|---|---|---|---|---|---|---|
| Badicu, G. et al. (2018) [22] | Romania | 398 | College student | 20 ± 2.10 | 35% | PSQI | 0.001 |
| Dabrowska-Galas, M. (2021) [23] | Poland | 80 | Elderly | 51.75 ± 5.57 | 100% | AIS | 0.025 |
| Dietz-Terjung, S. (2021) [24] | Germany | 109 | Young | 31.8 ± 13.2 | 41% | Wactigraph-bt | 0.010 |
| Grimaldi-Puyana, M. (2020) [25] | Spain | 306 | Youth | 20.7 ± 1.4 | 40% | PSQI | 0.003 |
| Herring, M.P. (2018) [26] | Ireland | 418 | Middle school student | 15.1 ± 1.7 | 42% | PSQI | 0.570 |
| Mahfouz, M.S. (2020) [27] | Saudi Arabia | 440 | College student | 22.38 ± 1.6 | 51.1% | PSQI | 0.009 |
| Mozaffari-Khosravi, H (2021) [28] | Iran | 569 | High school student | 14.22 ± 0.88 | 47.8% | PSQI | 0.016 |
| Osailan A.M. (2021) [29] | Saudi Arabia | 33 | Youth | 23 ± 1 | 0% | PSQI | 0.040 |
| Stefan L. (2018) [30] | Croatia | 894 | Elderly | 80±3 | 56% | PSQI | 0.879 |
| Wunsch, K. (2017) [31] | Germany | 64 | College student | 23.13 ± 5.12 | 67% | PSQI | 0.010 |
| W.St.Laurent, C. (2020) [32] | United States | 288 | Child | 4.3 ± 0.8 | 47.2% | CSHQ | 0.001 |
| Number of Studies | Test of Heterogeneity | Effect Size and 95% Confidence Interval | Two−Tailed Test | ||||
|---|---|---|---|---|---|---|---|
| X2 | p | I2 | Z | p | |||
| 11 | 26.25 | 0.003 | 62% | 0.02 [−0.01, 0.05] | 1.45 | 0.15 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, H.; Lu, C.; Yi, C. Physical Activity and Sleep Quality Association in Different Populations: A Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 1864. https://doi.org/10.3390/ijerph20031864
Zhao H, Lu C, Yi C. Physical Activity and Sleep Quality Association in Different Populations: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(3):1864. https://doi.org/10.3390/ijerph20031864
Chicago/Turabian StyleZhao, Haitao, Chuntian Lu, and Cuixia Yi. 2023. "Physical Activity and Sleep Quality Association in Different Populations: A Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 3: 1864. https://doi.org/10.3390/ijerph20031864
APA StyleZhao, H., Lu, C., & Yi, C. (2023). Physical Activity and Sleep Quality Association in Different Populations: A Meta-Analysis. International Journal of Environmental Research and Public Health, 20(3), 1864. https://doi.org/10.3390/ijerph20031864