
Symptoms of Sarcopenia and Physical Fitness through the Senior Fitness Test

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Sample and Study Design
2.2. Instruments
2.2.1. Anthropometric Measurements
2.2.2. Symptomatology of Sarcopenia
2.2.3. Senior Fitness Test (SFT)
2.2.4. Body Balance
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosisReport of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Bahat, G.; Yilmaz, O.; Kiliç, C.; Oren, M.; Karan, M. Performance of SARC-F in regard to sarcopenia definitions, muscle mass and functional measures. J. Nutr. Health Aging 2018, 22, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Orsso, C.E.; Tibaes, J.R.; Oliveira, C.L.; Rubin, D.A.; Field, C.J.; Heymsfield, S.B.; Prado, C.M.; Haqq, A.M. Low muscle mass and strength in pediatrics patients: Why should we care? Clin. Nutr. 2019, 38, 2002–2015. [Google Scholar] [CrossRef]
- Baptista, F.; Zymbal, V.; Janz, K.F. Predictive validity of handgrip strength, vertical jump power, and plank time in the identification of pediatric sarcopenia. Meas. Phys. Educ. Exerc. Sci. 2021, 26, 361–370. [Google Scholar] [CrossRef]
- Ackermans, L.L.; Rabou, J.; Basrai, M.; Schweinlin, A.; Bischoff, S.; Cussenot, O.; Cancel-Tassin, G.; Renken, R.; Gómez, E.; Sánchez-González, P. Screening, Diagnosis and Monitoring of Sarcopenia: When to use which tool? Clin. Nutr. ESPEN 2022, 48, 36–44. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.; Cruz-Jentoft, A.; Arai, H.; Kritchevsky, S.; Guralnik, J.; Bauer, J.; Pahor, M.; Clark, B.; Cesari, M. International clinical practice guidelines for sarcopenia (ICFSR): Screening, diagnosis and management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Liu, X.; Hao, Q.; Yue, J.; Hou, L.; Xia, X.; Zhao, W.; Zhang, Y.; Ge, M.; Ge, N.; Dong, B. Sarcopenia, obesity and sarcopenia obesity in comparison: Prevalence, metabolic profile, and key differences: Results from WCHAT study. J. Nutr. Health Aging 2020, 24, 429–437. [Google Scholar] [CrossRef]
- Dent, E.; Woo, J.; Scott, D.; Hoogendijk, E.O. Toward the recognition and management of sarcopenia in routine clinical care. Nat. Aging 2021, 1, 982–990. [Google Scholar] [CrossRef]
- Bahat, G.; Yilmaz, O.; Oren, M.M.; Karan, M.A.; Reginster, J.Y.; Bruyère, O.; Beaudart, C. Cross-cultural adaptation and validation of the SARC-F to assess sarcopenia: Methodological report from European Union Geriatric Medicine Society Sarcopenia Special Interest Group. Eur. Geriatr. Med. 2018, 9, 23–28. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Malmstrom, T.; Morley, J. Sarcopenia: The target population. J. Frailty Aging 2013, 2, 55–56. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Morley, J.E. SARC-F: A simple questionnaire to rapidly diagnose sarcopenia. J. Am. Med. Dir. Assoc. 2013, 14, 531–532. [Google Scholar] [CrossRef]
- Yang, M.; Hu, X.; Xie, L.; Zhang, L.; Zhou, J.; Lin, J.; Wang, Y.; Li, Y.; Han, Z.; Zhang, D. SARC-F for sarcopenia screening in community-dwelling older adults: Are 3 items enough? Medicine 2018, 97, e11726. [Google Scholar] [CrossRef]
- Woo, J.; Leung, J.; Morley, J.E. Validating the SARC-F: A suitable community screening tool for sarcopenia? J. Am. Med. Dir. Assoc. 2014, 15, 630–634. [Google Scholar] [CrossRef]
- Ida, S.; Murata, K.; Nakadachi, D.; Ishihara, Y.; Imataka, K.; Uchida, A.; Monguchi, K.; Kaneko, R.; Fujiwara, R.; Takahashi, H. Development of a Japanese version of the SARC-F for diabetic patients: An examination of reliability and validity. Aging Clin. Exp. Res. 2017, 29, 935–942. [Google Scholar] [CrossRef]
- Yee, X.S.; Ng, Y.S.; Allen, J.C.; Latib, A.; Tay, E.L.; Abu Bakar, H.M.; Ho, C.Y.J.; Koh, W.C.C.; Kwek, H.H.T.; Tay, L. Performance on sit-to-stand tests in relation to measures of functional fitness and sarcopenia diagnosis in community-dwelling older adults. Eur. Rev. Aging Phys. Act. 2021, 18, 1. [Google Scholar] [CrossRef]
- Rodrigues, F.; Domingos, C.; Monteiro, D.; Morouco, P. A Review on Aging, Sarcopenia, Falls, and Resistance Training in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 874. [Google Scholar] [CrossRef]
- Patrizio, E.; Calvani, R.; Marzetti, E.; Cesari, M. Physical Functional Assessment in Older Adults. J. Frailty Aging 2021, 10, 141–149. [Google Scholar] [CrossRef]
- Todde, F.; Melis, F.; Mura, R.; Pau, M.; Fois, F.; Magnani, S.; Ibba, G.; Crisafulli, A.; Tocco, F. A 12-week vigorous exercise protocol in a healthy group of persons over 65: Study of physical function by means of the Senior Fitness Test. BioMed Res. Int. 2016, 2016, 7639842. [Google Scholar] [CrossRef] [Green Version]
- de Souza Moreira, A.C.S.; Menezes, E.C.; Custódio, D.; Cardoso, F.L.; Mazo, G.Z. Senior fitness test no risco de queda em idosos: Um estudo prospectivo. Rev. Bras. Educ. Física Esporte 2020, 34, 195–203. [Google Scholar]
- Vagetti, G.C.; Barbosa Filho, V.C.; Oliveira, V.d.; Mazzardo, O.; Moreira, N.B.; Gomes, A.C.; Campos, W.d. Functional fitness in older women from southern brazil: Normative scores and comparison with different countries. Rev. Bras. Cineantropometria Desempenho Hum. 2015, 17, 472–484. [Google Scholar] [CrossRef]
- Chen, H.-H.; Chen, H.-L.; Lin, Y.-T.; Lin, C.-W.; Ho, C.-C.; Lin, H.-Y.; Lee, P.-F. The associations between functional fitness test performance and abdominal obesity in healthy elderly people: Results from the National Physical Fitness Examination Survey in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 264. [Google Scholar] [CrossRef] [PubMed]
- Sui, S.X.; Holloway-Kew, K.L.; Hyde, N.K.; Williams, L.J.; Leach, S.; Pasco, J.A. Muscle strength and gait speed rather than lean mass are better indicators for poor cognitive function in older men. Sci. Rep. 2020, 10, 10367. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 2016, CD011145. [Google Scholar] [CrossRef]
- Barbosa-Silva, T.G.; Menezes, A.M.B.; Bielemann, R.M.; Malmstrom, T.K.; Gonzalez, M.C. Enhancing SARC-F: Improving sarcopenia screening in the clinical practice. J. Am. Med. Dir. Assoc. 2016, 17, 1136–1141. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Functional fitness normative scores for community-residing older adults, ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Hesseberg, K.; Bentzen, H.; Bergland, A. Reliability of the senior fitness test in Community-dwelling older people with cognitive impairment. Physiother. Res. Int. 2015, 20, 37–44. [Google Scholar] [CrossRef]
- Rose, D.J.; Lucchese, N.; Wiersma, L.D. Development of a multidimensional balance scale for use with functionally independent older adults. Arch. Phys. Med. Rehabil. 2006, 87, 1478–1485. [Google Scholar] [CrossRef]
- Rose, D.J. Fallproof!: A Comprehensive Balance and Mobility Training Program; Human Kinetics: Champaign, IL, USA, 2010. [Google Scholar]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Liguori, G.; Medicine, A.C.o.S. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- Liu, J.-D.; Quach, B.; Chung, P.-K. Further understanding of the Senior Fitness Test: Evidence from community-dwelling high function older adults in Hong Kong. Arch. Gerontol. Geriatr. 2019, 82, 286–292. [Google Scholar] [CrossRef]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549. [Google Scholar] [CrossRef]
- Glenn, J.M.; Gray, M.; Binns, A. Relationship of Sit-to-Stand Lower-Body Power With Functional Fitness Measures Among Older Adults With and Without Sarcopenia. J. Geriatr. Phys. Ther. 2017, 40, 42–50. [Google Scholar] [CrossRef]
- Yang, M.; Hu, X.; Xie, L.; Zhang, L.; Zhou, J.; Lin, J.; Wang, Y.; Li, Y.; Han, Z.; Zhang, D. Screening sarcopenia in community-dwelling older adults: SARC-F vs. SARC-F combined with calf circumference (SARC-CalF). J. Am. Med. Dir. Assoc. 2018, 19, e271–277.e278. [Google Scholar] [CrossRef]
- Zasadzka, E.; Pieczyńska, A.; Trzmiel, T.; Pawlaczyk, M. Polish translation and validation of the SARC-F tool for the assessment of sarcopenia. Clin. Interv. Aging 2020, 15, 567. [Google Scholar] [CrossRef]
- Drey, M.; Ferrari, U.; Schraml, M.; Kemmler, W.; Schoene, D.; Franke, A.; Freiberger, E.; Kob, R.; Sieber, C. German version of SARC-F: Translation, adaption, and validation. J. Am. Med. Dir. Assoc. 2020, 21, 747–751.e741. [Google Scholar] [CrossRef]
- Gasparik, A.; Demián, M.; Pascanu, I. Romanian Translation and Validation of the SARC-F Questionnaire. Acta Endocrinol. 2020, 16, 216. [Google Scholar] [CrossRef]
- Gade, J.; Beck, A.M.; Rønholt, F.; Andersen, H.E.; Munk, T.; Vinther, A. Validation of the Danish SARC-F in hospitalized, geriatric medical patients. J. Nutr. Health Aging 2020, 24, 1120–1127. [Google Scholar] [CrossRef]
- Tsekoura, M.; Billis, E.; Tsepis, E.; Lampropoulou, S.; Beaudart, C.; Bruyere, O.; Yilmaz, O.; Bahat, G.; Gliatis, J. Cross-cultural adaptation and validation of the Greek Version of the SARC-F for evaluating sarcopenia in Greek older adults. J. Musculoskelet. Neuronal Interact. 2020, 20, 505. [Google Scholar]
- Wu, T.-Y.; Liaw, C.-K.; Chen, F.-C.; Kuo, K.-L.; Chie, W.-C.; Yang, R.-S. Sarcopenia screened with SARC-F questionnaire is associated with quality of life and 4-year mortality. J. Am. Med. Dir. Assoc. 2016, 17, 1129–1135. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Ida, S.; Kaneko, R.; Murata, K. SARC-F for screening of sarcopenia among older adults: A meta-analysis of screening test accuracy. J. Am. Med. Dir. Assoc. 2018, 19, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Voelker, S.N.; Michalopoulos, N.; Maier, A.B.; Reijnierse, E.M. Reliability and concurrent validity of the SARC-F and its modified versions: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2021, 22, 1864–1876. e1816. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.-L.; Ding, L.-Y.; Xu, Q.; Zhu, S.-Q.; Xu, X.-Y.; Hua, H.-X.; Chen, L.; Xu, H. Screening accuracy of SARC-F for sarcopenia in the elderly: A diagnostic meta-analysis. J. Nutr. Health Aging 2021, 25, 172–182. [Google Scholar] [CrossRef]
- Kera, T.; Kawai, H.; Hirano, H.; Kojima, M.; Watanabe, Y.; Motokawa, K.; Fujiwara, Y.; Osuka, Y.; Kojima, N.; Kim, H. Limitations of SARC-F in the diagnosis of sarcopenia in community-dwelling older adults. Arch. Gerontol. Geriatr. 2020, 87, 103959. [Google Scholar] [CrossRef]
- Yi, Y.; Baek, J.Y.; Lee, E.; Jung, H.-W.; Jang, I.-Y. A Comparative Study of High-Frequency Bioelectrical Impedance Analysis and Dual-Energy X-ray Absorptiometry for Estimating Body Composition. Life 2022, 12, 994. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean ± SD | ||||
|---|---|---|---|---|
| All (n = 312) | Male (n = 112) | Female (n = 200) | p-Value | |
| Age, years | 72.63 ± 7.81 | 73.07 ± 7.31 | 72.39 ± 8.09 | 0.458 |
| Body Height, cm | 153.65 ± 8.22 | 159.99 ± 8.26 | 150.10 ± 5.67 | <0.001 |
| Body Mass, kg | 63.70 ± 12.67 | 69.29 ± 11.61 | 60.52 ± 12.18 | <0.001 |
| BMI, kg/m2 | 26.88 ± 4.65 | 27.08 ± 4.64 | 26.76 ± 4.65 | 0.566 |
| SARC-F score, pts | 1.75 ± 1.88 | 1.43 ± 1.68 | 1.92 ± 1.95 | 0.915 |
| SARC-F ≥ 4 pts, n (%) # | 56 (17.9) | 14 (12.5) | 42 (21.0) | 0.061 |
| Physical Fitness | ||||
| Chair Stand Test, n | 10.86 ± 3.22 | 11.08 ± 3.34 | 10.74 ± 3.15 | 0.365 |
| Arm Curl Test, n | 12.56 ± 3.83 | 13.19 ± 4.07 | 12.22 ± 3.66 | 0.031 |
| CSAR, cm * | 4.00 (11) | 6.00 (11) | 3.00 (11) | 0.284 |
| BST, cm * | −19.00 (21) | −23.00 (18) | −17.00 (23) | <0.001 |
| FUG, seg | 8.08 ± 2.67 | 7.43 ± 2.06 | 8.44 ± 2.89 | <0.001 |
| 6MWT, m | 407.29 ± 108.43 | 450.76 ± 125.58 | 382.95 ± 88.99 | <0.001 |
| FAB score, pts | 12.44 ± 3.66 | 13.29 ± 3.07 | 11.97 ± 3.88 | 0.002 |
| Male (n = 112) | Female (n = 200) | ||||||
|---|---|---|---|---|---|---|---|
| Symptoms | None | Some | A Lot, or Unable | None | Some | A Lot, or Unable | p-Value |
| 1. Lack of strength, n (%) | 79 (70.5) | 20 (17.9) | 13 (11.6) | 133 (66.5) | 48 (24.0) | 19 (9.5) | 0.808 |
| 2. Assistance in walking, n (%) | 93 (83.0) | 18 (16.1) | 1 (0.9) | 156 (78.0) | 37 (18.5) | 7 (3.5) | 0.175 |
| 3. Difficulty rising from a chair, n (%) | 84 (75.0) | 26 (23.2) | 2 (1.8) | 142 (71.0) | 55 (27.5) | 3 (1.5) | 0.521 |
| 4. Difficulty climbing stairs, n (%) | 63 (56.3) | 41 (36.6) | 8 (7.1) | 115 (57.5) | 71 (35.5) | 14 (7.0) | 0.851 |
| 5. Falls, n (%) | 73 (65.2) | 39 (34.8) | 0 (0.0) | 150 (75.0) | 50 (25.0) | 0 (0.0) | 0.124 |
| SARC-F (Score) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Male (n = 112) | Female (n = 200) | |||||||
| Functional Fitness Tests | B | p | OR | 95% CI | B | p | OR | 95% CI |
| 30-s chair stand test, n | −0.244 | 0.014 | 0.784 | 0.645–0.953 | −0.105 | 0.081 | 0.900 | 0.800–1.013 |
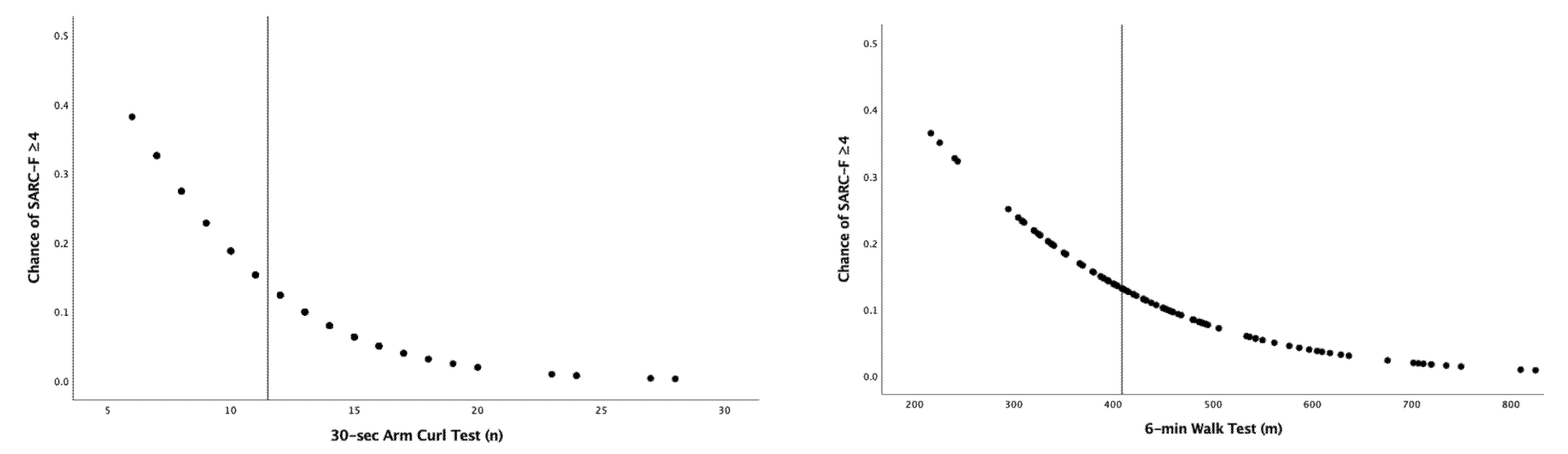
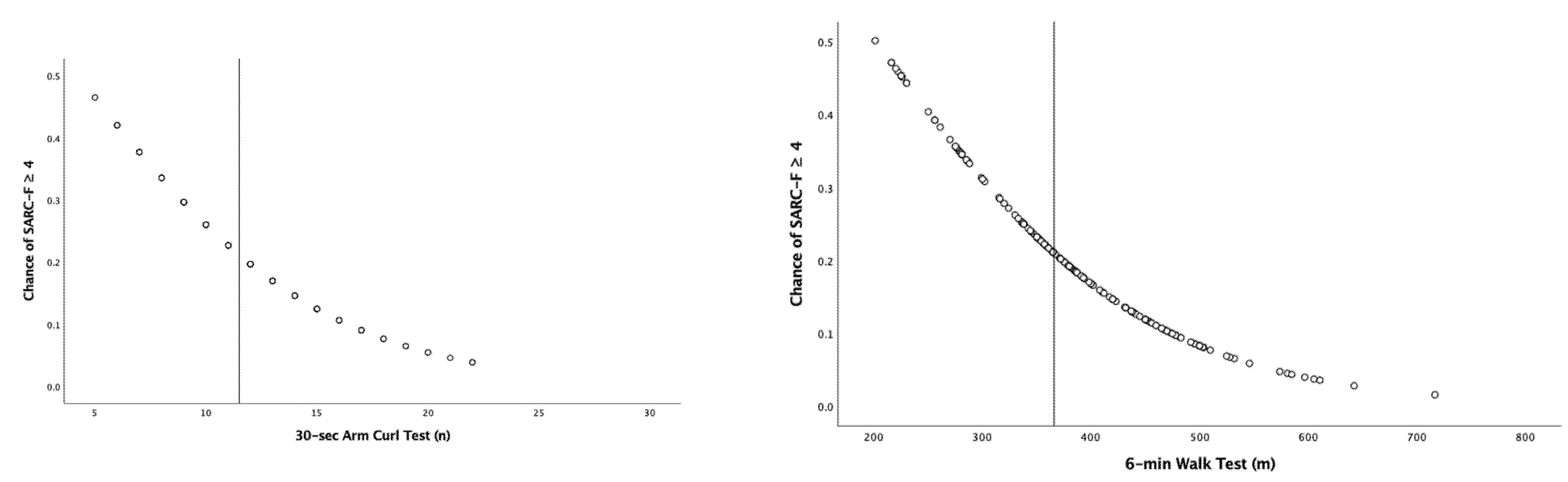
| 30-s arm curl test, n | −0.246 | 0.012 | 0.782 | 0.646–0.947 | −0.187 | 0.001 | 0.829 | 0.742–0.926 |
| Chair sit-and-reach test, cm | −0.051 | 0.028 | 0.950 | 0.907–0.994 | −0.007 | 0.624 | 0.993 | 0.964–1.022 |
| Back scratch test, cm | −0.036 | 0.126 | 0.964 | 0.961–1.010 | −0.031 | 0.026 | 0.969 | 0.943–0.996 |
| Foot up-and-go test, seg | 0.161 | 0.182 | 1.174 | 0.928–1.486 | 0.125 | 0.024 | 1.133 | 1.016–1.263 |
| 6-min walk test, m | −0.007 | 0.032 | 0.993 | 0.987–0.999 | −0.008 | 0.001 | 0.992 | 0.988–0.997 |
| Fullerton Advanced Balance, n | −0.084 | 0.305 | 0.919 | 0.783–1.079 | −0.095 | 0.026 | 0.910 | 0.837–0.989 |
| Difficulty in Lifting and Carrying 4.5 kg | ||||||||
| Male (n = 112) | Female (n = 200) | |||||||
| Predictor | β | p | OR | 95% CI | β | p | OR | 95% CI |
| 30-s chair stand test, n | −0.070 | 0.276 | 0.932 | 0.822–1.058 | 0.013 | 0.784 | 1.013 | 0.923–1.112 |
| 30-s arm curl test, n | −0.087 | 0.128 | 0.917 | 0.820–1.025 | −0.030 | 0.476 | 0.971 | 0.895–1.053 |
| Chair sit-and-reach test, cm | 0.002 | 0.908 | 1.002 | 0.966–1.040 | −0.015 | 0.257 | 0.985 | 0.960–1.011 |
| Back scratch test, cm | 0.001 | 0.925 | 1.001 | 0.975–1.028 | 0.022 | 0.046 | 1.022 | 1.000–1.044 |
| 8-foot up-and-go test, seg | 0.039 | 0.689 | 1.040 | 0.857–1.262 | −0.023 | 0.669 | 0.978 | 0.882–1.084 |
| 6-min walk test, m | −0.002 | 0.195 | 0.998 | 0.994–1.001 | −0.001 | 0.441 | 0.999 | 0.995–1.002 |
| Fullerton Advanced Balance Scale, n | −0.069 | 0.291 | 0.934 | 0.822–1.061 | 0.046 | 0.258 | 1.047 | 0.967–1.132 |
| Difficulty in Walking Across a Room | ||||||||
| Male (n = 112) | Female (n = 200) | |||||||
| Predictor | β | p | OR | 95% CI | β | p | OR | 95% CI |
| 30-s chair stand test, n | 0.008 | 0.911 | 1.008 | 0.870–1.169 | -0.037 | 0.504 | 0.964 | 0.864–1.074 |
| 30-s arm curl test, n | −0.066 | 0.336 | 0.936 | 0.819–1.070 | −0.025 | 0.593 | 0.975 | 0.889–1.070 |
| Chair sit-and-reach test, cm | 0.005 | 0.815 | 1.005 | 0.961–1.052 | −0.025 | 0.098 | 0.975 | 0.947–1.005 |
| Back scratch test, cm | −0.024 | 0.215 | 0.977 | 0.941–1.014 | 0.015 | 0.218 | 1.015 | 0.991–1.039 |
| 8-foot up-and-go test, seg | −0.015 | 0.904 | 0.985 | 0.772–1.257 | 0.012 | 0.837 | 1.012 | 0.903–1.134 |
| 6-min walk test, m | 0.001 | 0.956 | 1.000 | 0.996–1.004 | 0.001 | 0.730 | 1.001 | 0.997–1.004 |
| Fullerton Advanced Balance Scale, n | −0.036 | 0.645 | 0.965 | 0.828–1.124 | 0.033 | 0.467 | 1.034 | 0.945–1.131 |
| Difficulty in Transferring from a Chair or Bed | ||||||||
| Male (n = 112) | Female (n = 200) | |||||||
| Predictor | β | p | OR | 95% CI | β | p | OR | 95% CI |
| 30 s chair stand test, n | −0.031 | 0.635 | 0.696 | 0.851–1.103 | −0.098 | 0.065 | 0.907 | 0.817–1.006 |
| 30 s arm curl test, n | −0.012 | 0.819 | 0.988 | 0.887–1.099 | −0.101 | 0.027 | 0.904 | 0.827–0.989 |
| Chair sit-and-reach test, cm | 0.007 | 0.728 | 1.007 | 0.968–1.047 | −0.022 | 0.109 | 0.978 | 0.952–1.005 |
| Back scratch test, cm | −0.016 | 0.299 | 0.984 | 0.955–1.014 | 0.018 | 0.103 | 1.018 | 0.996–1.041 |
| 8-foot up-and-go test, seg | −0.090 | 0.435 | 0.914 | 0.729–1.146 | 0.013 | 0.808 | 1.013 | 0.913–1.125 |
| 6-min walk test, m | −0.001 | 0.655 | 0.999 | 0.996–1.003 | −0.001 | 0.672 | 0.999 | 0.996–1.003 |
| Fullerton Advanced Balance Scale, n | 0.086 | 0.297 | 1.090 | 0927–1.280 | 0.049 | 0.245 | 1.050 | 0.967–1.141 |
| Difficulty in Climbing a Flight of 10 Stairs | ||||||||
| Male (n = 112) | Female (n = 200) | |||||||
| Predictor | β | p | OR | 95% CI | β | p | OR | 95% CI |
| 30-s chair stand test, n | −0.023 | 0.962 | 0.977 | 0.873–1.094 | −0.036 | 0.428 | 0.964 | 0.881–1.055 |
| 30-s arm curl test, n | −0.050 | 0.301 | 0.951 | 0.864–1.046 | −0.003 | 0.929 | 0.997 | 0.923–1.076 |
| Chair sit-and-reach test, cm | −0.014 | 0.414 | 0.986 | 0.953–1.020 | 0.007 | 0.581 | 1.007 | 0.983–1.032 |
| Back scratch test, cm | 0.002 | 0.841 | 1.002 | 0.978–1.027 | 0.018 | 0.091 | 1.018 | 0.997–1.039 |
| 8-foot up-and-go test, seg | 0.005 | 0.957 | 1.005 | 0.838–1.205 | 0.005 | 0.917 | 1.005 | 0.912–1.107 |
| 6-min walk test, m | −0.001 | 0.394 | 0.999 | 0.996–1.002 | 0.001 | 0.868 | 1.000 | 0.997–1.003 |
| Fullerton Advanced Balance Scale, n | −0.084 | 0.188 | 0.919 | 0.811–1.042 | 0.029 | 0.439 | 1.029 | 0.957–1.108 |
| Falls in the Past Year | ||||||||
| Male (n = 112) | Female (n = 200) | |||||||
| Predictor | β | p | OR | 95% CI | β | p | OR | 95% CI |
| 30-s chair stand test, n | 0.049 | 0.411 | 1.051 | 0.934–1.182 | 0.061 | 0.230 | 1.063 | 0.962–1.175 |
| 30-s arm curl test, n | −0.043 | 0.399 | 0.958 | 0.867–1.059 | 0.001 | 0.991 | 1.000 | 0.917–1.092 |
| Chair sit-and-reach test, cm | 0.016 | 0.374 | 1.017 | 0.980–1.054 | 0.016 | 0.276 | 1.016 | 0.988–1.044 |
| Back scratch test, cm | −0.012 | 0.371 | 0.988 | 0.962–1.015 | −0.019 | 0.127 | 0.981 | 0.958–1.005 |
| 8-foot up-and-go test, seg | −0.076 | 0.453 | 0.927 | 0.759–1.131 | 0.032 | 0.564 | 1.032 | 0.927–1.149 |
| 6-min walk test, m | 0.001 | 0.786 | 1.000 | 0.996–1.003 | −0.002 | 0.245 | 0.998 | 0.994–1.002 |
| Fullerton Advanced Balance Scale, n | 0.033 | 0.626 | 1.033 | 0.906–1.179 | 0.014 | 0.043 | 0.107 | 0.933–1.103 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lima, A.B.d.; Baptista, F.; Henrinques-Neto, D.; Pinto, A.d.A.; Gouveia, E.R. Symptoms of Sarcopenia and Physical Fitness through the Senior Fitness Test. Int. J. Environ. Res. Public Health 2023, 20, 2711. https://doi.org/10.3390/ijerph20032711
Lima ABd, Baptista F, Henrinques-Neto D, Pinto AdA, Gouveia ER. Symptoms of Sarcopenia and Physical Fitness through the Senior Fitness Test. International Journal of Environmental Research and Public Health. 2023; 20(3):2711. https://doi.org/10.3390/ijerph20032711
Chicago/Turabian StyleLima, Alex Barreto de, Fátima Baptista, Duarte Henrinques-Neto, André de Araújo Pinto, and Elvio Rúbio Gouveia. 2023. "Symptoms of Sarcopenia and Physical Fitness through the Senior Fitness Test" International Journal of Environmental Research and Public Health 20, no. 3: 2711. https://doi.org/10.3390/ijerph20032711
APA StyleLima, A. B. d., Baptista, F., Henrinques-Neto, D., Pinto, A. d. A., & Gouveia, E. R. (2023). Symptoms of Sarcopenia and Physical Fitness through the Senior Fitness Test. International Journal of Environmental Research and Public Health, 20(3), 2711. https://doi.org/10.3390/ijerph20032711