
The Effectiveness of Workplace Musculoskeletal Injury Risk Factor Screening Tools for Reducing Injury: A Systematic Review

 , , , ,
, , , ,
Abstract
:1. Introduction
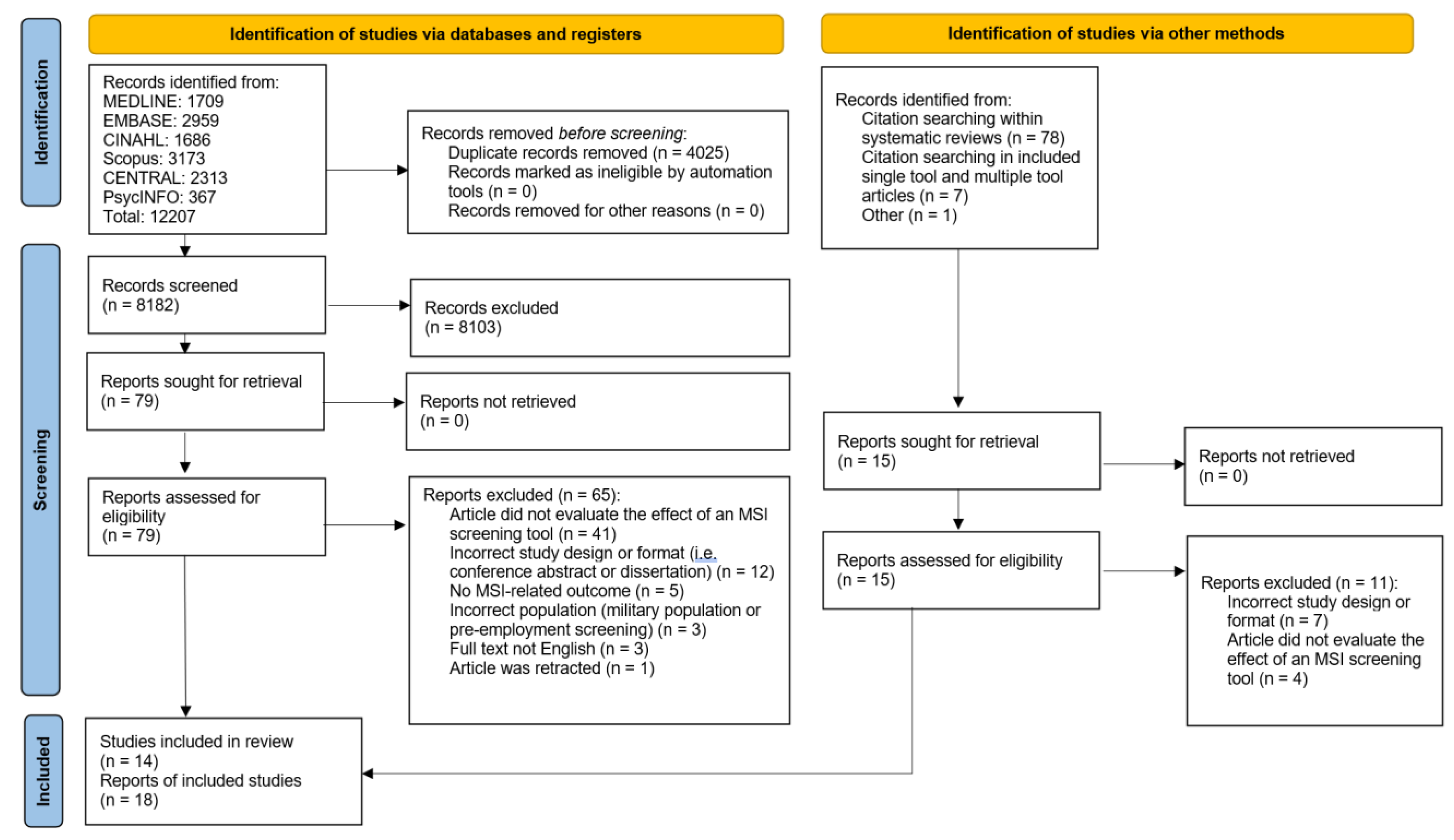
2. Materials and Methods
3. Results
3.1. Characteristics of Single-Tool Articles
3.2. Characteristics of Multiple-Tool Articles
3.3. Synthesis of Included Study Results
3.4. Effects on Musculoskeletal Discomfort
3.5. Effects on Work Absence
3.6. Effects on Health Resource Utilization
3.7. Effects on Workplace Behaviour
3.8. Effects on Workplace-Associated MSI
3.9. Effects on Claims Costs
3.10. Effects on Self-Rated Health Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Briggs, A.M.; Woolf, A.D.; Dreinhöfer, K.; Homb, N.; Hoy, D.G.; Kopansky-Giles, D.; Åkesson, K.; March, L. Reducing the Global Burden of Musculoskeletal Conditions. Bull. World Health Organ. 2018, 96, 366–368. [Google Scholar] [CrossRef]
- Briggs, A.M.; Jordan, J.E.; Kopansky-Giles, D.; Sharma, S.; March, L.; Schneider, C.H.; Mishrra, S.; Young, J.J.; Slater, H. The Need for Adaptable Global Guidance in Health Systems Strengthening for Musculoskeletal Health: A Qualitative Study of International Key Informants. Glob. Health Res. Policy 2021, 6, 24. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and Treatment of Low Back Pain: Evidence, Challenges, and Promising Directions. The Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- World Health Organization; International Labour Organization. WHO/ILO Joint Estimates of the Work-Related Burden of Disease and Injury, 2000–2016: Global Monitoring Report; World Health Organization; International Labour Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Wilhelmus Johannes Andreas, G.; Johanssons, E. Observational Methods for Assessing Ergonomic Risks for Work-Related Musculoskeletal Disorders. A Scoping Review. Rev. Cienc. Salud 2018, 16, 8–38. [Google Scholar] [CrossRef]
- Beliveau, P.J.H.; Johnston, H.; Van Eerd, D.; Fischer, S.L. Musculoskeletal Disorder Risk Assessment Tool Use: A Canadian Perspective. Appl. Ergon. 2022, 102, 103740. [Google Scholar] [CrossRef] [PubMed]
- Kee, D. Systematic Comparison of OWAS, RULA, and REBA Based on a Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 595. [Google Scholar] [PubMed]
- Rimando, C.R.D.; Batay, C.M.L.; Canita, V.E.S.; Dela Cruz, A.M.C.; Egos, G.A.D.; Ladisla, N.K.E.; Panlilio, J.K.S.; Ramos, A.M.P.; Tayo, P.A.B.; Villamor, Z.M.F.; et al. Validity and Reliability of the Modified RULA (MRULA) among Public and Private Office Workers. In Proceedings of the Journal of Physics: Conference Series, Xi’an, China, 18–19 October 2020; Institute of Physics Publishing: Bristol, UK, 2020; Volume 1529, p. 32056. [Google Scholar]
- Speklé, E.M.; Hoozemans, M.J.; Blatter, B.M.; Heinrich, J.; van der Beek, A.J.; Knol, D.L.; Bongers, P.M.; van Dieën, J.H. Effectiveness of a Questionnaire Based Intervention Programme on the Prevalence of Arm, Shoulder and Neck Symptoms, Risk Factors and Sick Leave in Computer Workers: A Cluster Randomised Controlled Trial in an Occupational Setting. BMC Musculoskelet. Disord. 2010, 11, 99. [Google Scholar] [CrossRef]
- Colombini, D.; Occhipinti, E. Scientific Basis of the OCRA Method for Risk Assessment of Biomechanical Overload of Upper Limb, as Preferred Method in ISO Standards on Biomechanical Risk Factors. Scand. J. Work Environ. Health 2018, 44, 436–438. [Google Scholar] [CrossRef]
- Armstrong, T.J.; Burdorf, A.; Descatha, A.; Farioli, A.; Graf, M.; Horie, S.; Marras, W.S.; Potvin, J.R.; Rempel, D.; Spatari, G.; et al. Scientific Basis of ISO Standards on Biomechanical Risk Factors. Scand. J. Work Environ. Health 2018, 44, 323–329. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar]
- WorkSafeBC. Available online: https://www.worksafebc.com/en/law-policy/occupational-health-safety/searchable-ohs-regulation/ohs-regulation/part-04-general-conditions#SectionNumber:4.46 (accessed on 15 March 2022).
- Veritas Health Innovation Covidence Systematic Review Software. Available online: https://www.covidence.org/ (accessed on 28 January 2022).
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, P.; Jutai, J.W.; Strong, G.; Russell-Minda, E. Age-Related Macular Degeneration and Low-Vision Rehabilitation: A Systematic Review. Can. J. Ophthalmol. 2008, 43, 180–187. [Google Scholar] [CrossRef]
- Slavin, R.E. Best Evidence Synthesis: An Intelligent Alternative to Meta-Analysis. J. Clin. Epidemiol. 1995, 48, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without Meta-Analysis (SWiM) in Systematic Reviews: Reporting Guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- Boon, M.H.; Thomson, H. The Effect Direction Plot Revisited: Application of the 2019 Cochrane Handbook Guidance on Alternative Synthesis Methods. Res. Synth. Methods 2021, 12, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.A.; Amick III, B.C.; Dennerlein, J.T.; Brewer, S.; Catli, S.; Williams, R.; Serra, C.; Gerr, F.; Irvin, E.; Mahood, Q.; et al. Systematic Review of the Role of Occupational Health and Safety Interventions in the Prevention of Upper Extremity Musculoskeletal Symptoms, Signs, Disorders, Injuries, Claims and Lost Time. J. Occup. Rehabil. 2010, 20, 127–162. [Google Scholar] [CrossRef]
- Frost, P.; Haahr, J.P.; Andersen, J.H. Reduction of Pain-Related Disability in Working Populations: A Randomized Intervention Study of the Effects of an Educational Booklet Addressing Psychosocial Risk Factors and Screening Workplaces for Physical Health Hazards. Spine 2007, 32, 1949–1954. [Google Scholar] [CrossRef]
- Ho, W.Y.; Sung, C.Y.Y.; Yu, Q.H.; Chan, C.C.H. Effectiveness of Computerized Risk Assessment System on Enhancing Workers’ Occupational Health and Attitudes towards Occupational Health. Work 2014, 48, 471–484. [Google Scholar] [CrossRef]
- Ketola, R.; Toivonen, R.; Häkkänen, M.; Luukkonen, R.; Takala, E.P.; Viikari-Juntura, E. Effects of Ergonomic Intervention in Work with Video Display Units. Scand. J. Work Environ. Health 2002, 28, 18–24. [Google Scholar] [CrossRef]
- Speklé, E.M.; Heinrich, J.; Hoozemans, M.J.; Blatter, B.M.; Van Der Beek, A.J.; Van Dieën, J.H.; Van Tulder, M.W. The Cost-Effectiveness of the RSI Quickscan Intervention Programme for Computer Workers: Results of an Economic Evaluation alongside a Randomised Controlled Trial. BMC Musculoskelet. Disord. 2010, 11, 259. [Google Scholar] [CrossRef]
- Carrivick, P.J.W.; Lee, A.H.; Yau, K.K.W. Consultative Team to Assess Manual Handling and Reduce the Risk of Occupational Injury. Occup. Environ. Med. 2001, 58, 339–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrivick, P.J.W.; Lee, A.H.; Yau, K.K.W. Effectiveness of a Participatory Workplace Risk Assessment Team in Reducing the Risk and Severity of Musculoskeletal Injury. J. Occup. Health 2002, 44, 221–225. [Google Scholar] [CrossRef]
- Carrivick, P.J.W.; Lee, A.H.; Yau, K.K.W. Effectiveness of a Workplace Risk Assessment Team in Reducing the Rate, Cost, and Duration of Occupational Injury. J. Occup. Environ. Med. 2002, 44, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Carrivick, P.J.W.; Lee, A.H.; Yau, K.K.W.; Stevenson, M.R. Evaluating the Effectiveness of a Participatory Ergonomics Approach in Reducing the Risk and Severity of Injuries from Manual Handling. Ergonomics 2005, 48, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.S.; Chan, E.P.-S. The Effect of Individual Job Coaching and Use of Health Threat in a Job-Specific Occupational Health Education Program on Prevention of Work-Related Musculoskeletal Back Injury. J. Occup. Environ. Med. 2009, 51, 1413–1421. [Google Scholar] [CrossRef]
- Craib, K.J.P.; Hackett, G.; Back, C.; Cvitkovich, Y.; Yassi, A. Injury Rates, Predictors of Workplace Injuries, and Results of an Intervention Program among Community Health Workers: Populations at Risk across the Lifespan: Empirical Studies. Public Health Nurs. 2007, 24, 121–131. [Google Scholar] [CrossRef]
- Johnson, K.A.; Ruppe, J. A Job Safety Program for Construction Workers Designed to Reduce the Potential for Occupational Injury Using Tool Box Training Sessions and Computer-Assisted Biofeedback Stress Management Techniques. Int. J. Occup. Saf. Ergon. 2002, 8, 321–329. [Google Scholar] [CrossRef]
- Laing, A.C.; Frazer, M.B.; Cole, D.C.; Kerr, M.S.; Wells, R.P.; Norman, R.W. Study of the Effectiveness of a Participatory Ergonomics Intervention in Reducing Worker Pain Severity through Physical Exposure Pathways. Ergonomics 2005, 48, 150–170. [Google Scholar] [CrossRef]
- Laing, A.C.; Cole, D.C.; Theberge, N.; Wells, R.P.; Kerr, M.S.; Frazer, M.B. Effectiveness of a Participatory Ergonomics Intervention in Improving Communication and Psychosocial Exposures. Ergonomics 2007, 50, 1092–1109. [Google Scholar] [CrossRef]
- Melhorn, J.M.; Wilkinson, L.; Riggs, J.D. Management of Musculoskeletal Pain in the Workplace. J. Occup. Environ. Med. 2001, 43, 83–93. [Google Scholar] [CrossRef]
- Oude Hengel, K.M.; Blatter, B.M.; van der Molen, H.F.; Bongers, P.M.; van der Beek, A.J. The Effectiveness of a Construction Worksite Prevention Program on Work Ability, Health, and Sick Leave: Results from a Cluster Randomized Controlled Trial. Scand. J. Work Environ. Health 2013, 39, 456–467. [Google Scholar] [CrossRef]
- Porru, S.; Calza, S.; Arici, C. Prevention of Occupational Injuries: Evidence for Effective Good Practices in Foundries. J. Safety Res. 2017, 60, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Rautiainen, R.H.; Lange, J.L.; Hodne, C.J.; Schneiders, S.; Donham, K.J. Injuries in the Iowa Certified Safe Farm Study. J. Agric. Saf. Health 2004, 10, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Gross, D.P.; Armijo-Olivo, S.; Shaw, W.S.; Williams-Whitt, K.; Shaw, N.T.; Hartvigsen, J.; Qin, Z.; Ha, C.; Woodhouse, L.J.; Steenstra, I.A. Clinical Decision Support Tools for Selecting Interventions for Patients with Disabling Musculoskeletal Disorders: A Scoping Review. J. Occup. Rehabil. 2016, 26, 286–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Evidence Level | Minimum Study Quality according to Downs & Black (D&B) Rating | Minimum Study Quantity | Consistency |
|---|---|---|---|
| Strong | High (D&B score band of good or better) | 3 or more studies | Agreement of effect direction in 3 high quality studies. For ≥3 studies, at least 75% of high- and medium-quality studies agree in effect direction |
| Moderate | Medium (D&B score band of fair) | 2 high quality OR 2 medium quality and 1 high quality | Effect directions from 2 high quality studies agree OR effect directions from 2 medium studies and 1 high quality study agree. For ≥3 studies, effect direction agreement in more than 66% of studies |
| Limited | Medium (D&B score band of fair) | 1 high quality OR 2 medium quality OR 1 medium and 1 high quality | Effect directions from 2 medium- or high-quality studies agree. If ≥2 studies, more than 50% of medium and high-quality studies agree |
| Mixed | Medium or high D&B score bands | 2 studies | Effect directions from medium and high-quality studies are contradictory |
| Insufficient | No high quality, only 1 medium quality, any number of low (score band of poor) quality studies | ||
| Single-Tool Studies | Multiple-Tool Studies | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Frost 2007 [21] | Ho 2014 [22] | Ketola 2002 [23] | Speklé 2010 [9,24] (RCT and economic analysis) | Carrivick 2002, 2005 [26,27,28] | Craib 2007 [30] | Porru 2017 [36] | Rautainen 2004 [37] | Oude Hengel 2013 [35] |
| MSI Risk Factor Screening Tool | Danish working environment regulations | DSE RAM System | Ergonomic checklist for VDU work | RSI QuickScan | Manual handling checklist (+ multiple interventions) | Custom-checklist-based screen (+ multiple interventions) | Ad hoc risk assessment checklist (+ multiple interventions) | Certified Safe Farm checklist (+ multiple interventions) | QuickScan questionnaire (+ multiple interventions) |
| Musculoskeletal discomfort |  | |  |  | |||||
| Work absence | | |  | | | | |||
| Health resource utilization | | | |||||||
| Work behavior modification | | ||||||||
| Workplace-associated MSI | |  | | | |||||
| Claims cost | | | |||||||
| Self-rated health status | | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberts, R.; Slade, T.; Voaklander, D.; Straube, S.; Dennett, L.; Cancelliere, C.; Guptill, C.; Miller, L.; Lemay, D.; De Leon, M.; et al. The Effectiveness of Workplace Musculoskeletal Injury Risk Factor Screening Tools for Reducing Injury: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 2762. https://doi.org/10.3390/ijerph20032762
Roberts R, Slade T, Voaklander D, Straube S, Dennett L, Cancelliere C, Guptill C, Miller L, Lemay D, De Leon M, et al. The Effectiveness of Workplace Musculoskeletal Injury Risk Factor Screening Tools for Reducing Injury: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(3):2762. https://doi.org/10.3390/ijerph20032762
Chicago/Turabian StyleRoberts, Richard, Teri Slade, Don Voaklander, Sebastian Straube, Liz Dennett, Carol Cancelliere, Christine Guptill, Linda Miller, Danielle Lemay, Melnard De Leon, and et al. 2023. "The Effectiveness of Workplace Musculoskeletal Injury Risk Factor Screening Tools for Reducing Injury: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 3: 2762. https://doi.org/10.3390/ijerph20032762
APA StyleRoberts, R., Slade, T., Voaklander, D., Straube, S., Dennett, L., Cancelliere, C., Guptill, C., Miller, L., Lemay, D., De Leon, M., & Gross, D. P. (2023). The Effectiveness of Workplace Musculoskeletal Injury Risk Factor Screening Tools for Reducing Injury: A Systematic Review. International Journal of Environmental Research and Public Health, 20(3), 2762. https://doi.org/10.3390/ijerph20032762