

Acute Mountain Sickness and the Risk of Subsequent Psychiatric Disorders—A Nationwide Cohort Study in Taiwan
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset Sources
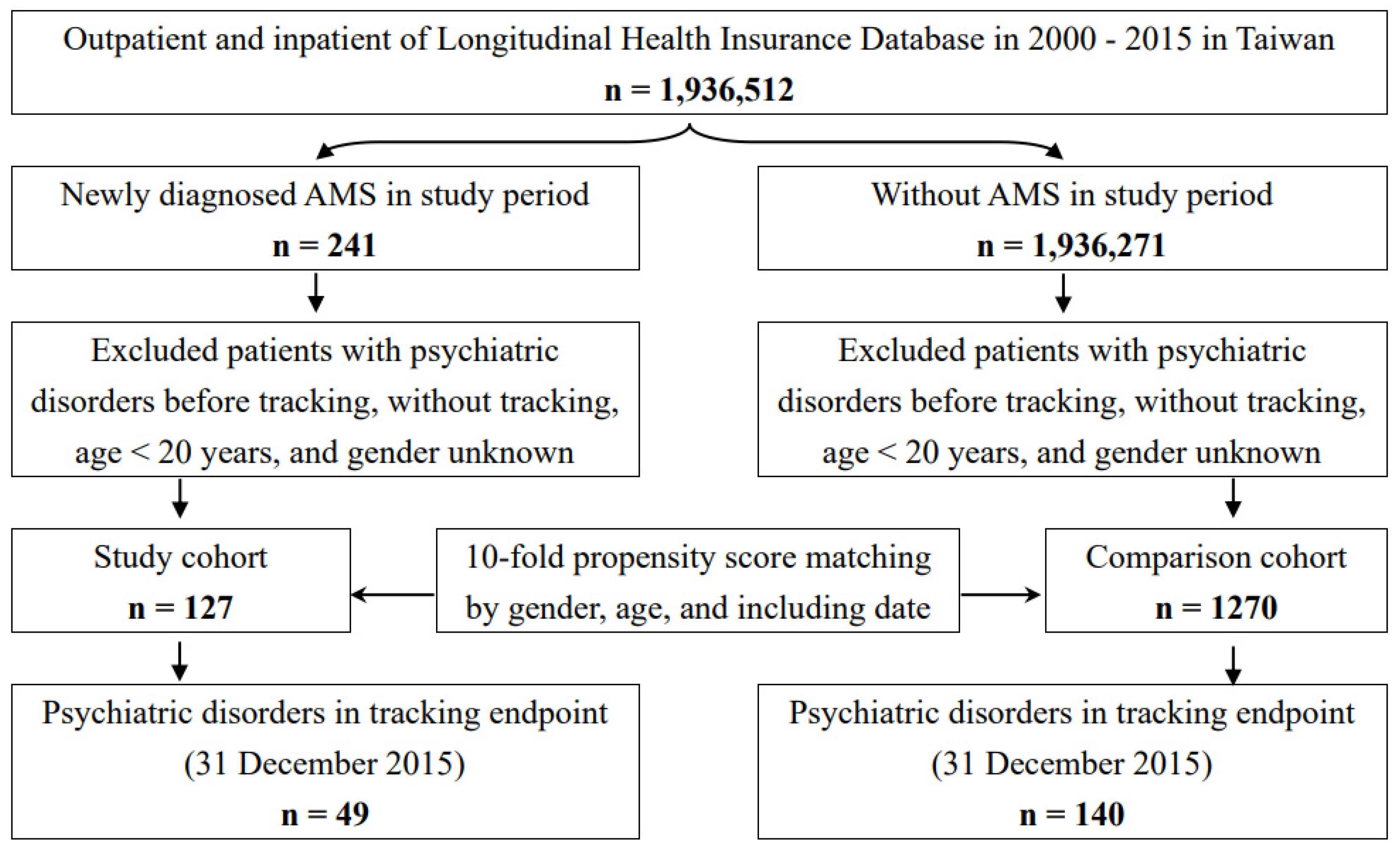
2.2. Study Design and Patient Selection
2.3. Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Study Cohort Characteristics
3.2. Kaplan–Meier Curves for the Cumulative Survival of Psychiatric Disorders
3.3. Sub-Distribution Hazard Ratio Analysis of Psychiatric Disorders in the AMS Group
3.4. Subgroup Analysis of Psychiatric Disorders in the AMS Group and the Control Group
3.5. Sensitivity Analysis and Types of Psychiatric Disorders
3.6. Years from AMS to the Development of Psychiatric Disorders
3.7. AMS and the Risk of Single or Multiple Psychiatric Diagnoses
4. Discussion
4.1. Strengths of This Study
4.2. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gudbjartsson, T.; Sigurdsson, E.; Gottfredsson, M.; Bjornsson, O.M.; Gudmundsson, G. High altitude illness and related diseases—A review. Laeknabladid 2019, 105, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Meier, D.; Collet, T.H.; Locatelli, I.; Cornuz, J.; Kayser, B.; Simel, D.L.; Sartori, C. Does This Patient Have Acute Mountain Sickness? The Rational Clinical Examination Systematic Review. JAMA 2017, 318, 1810–1819. [Google Scholar] [CrossRef]
- Boos, C.J.; Bass, M.; O’Hara, J.P.; Vincent, E.; Mellor, A.; Sevier, L.; Abdul-Razakq, H.; Cooke, M.; Barlow, M.; Woods, D.R. The relationship between anxiety and acute mountain sickness. PLoS ONE 2018, 13, e0197147. [Google Scholar] [CrossRef] [PubMed]
- Hüfner, K.; Sperner-Unterweger, B.; Brugger, H. Going to Altitude with a Preexisting Psychiatric Condition. High Alt. Med. Biol. 2019, 20, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Hüfner, K.; Caramazza, F.; Pircher Nöckler, E.R.; Stawinoga, A.E.; Fusar-Poli, P.; Bhandari, S.S.; Basnyat, B.; Brodmann Maeder, M.; Strapazzon, G.; Tomazin, I.; et al. Association of Pre-existing Mental Health Conditions with Acute Mountain Sickness at Everest Base Camp. High Alt. Med. Biol. 2022, 23, 338–344. [Google Scholar] [CrossRef]
- Roberts, M.J. Acute mountain sickness -- experience on the roof of Africa expedition and military implications. J. R. Army Med. Corps 1994, 140, 49–51. [Google Scholar] [CrossRef]
- Hazlerigg, A.; Woods, D.R.; Mellor, A.J. Incidence of acute mountain sickness in UK Military Personnel on Mount Kenya. J. R. Army Med. Corps 2016, 162, 465–469. [Google Scholar] [CrossRef]
- Chen, H.C.; Lin, W.L.; Wu, J.Y.; Wang, S.H.; Chiu, T.F.; Weng, Y.M.; Hsu, T.Y.; Wu, M.H. Change in oxygen saturation does not predict acute mountain sickness on Jade Mountain. Wilderness Environ. Med. 2012, 23, 122–127. [Google Scholar] [CrossRef]
- Wang, S.H.; Chen, Y.C.; Kao, W.F.; Lin, Y.J.; Chen, J.C.; Chiu, T.F.; Hsu, T.Y.; Chen, H.C.; Liu, S.W. Epidemiology of acute mountain sickness on Jade Mountain, Taiwan: An annual prospective observational study. High Alt. Med. Biol. 2010, 11, 43–49. [Google Scholar] [CrossRef]
- Kao, W.F.; Kuo, C.C.; Hsu, T.F.; Chang, H.; Sung, Y.Y.; Yen, D.H.; Wu, J.K.; Lee, C.H. Acute mountain sickness in Jade Mountain climbers of Taiwan. Aviat. Space Environ. Med. 2002, 73, 359–362. [Google Scholar]
- Wang, S.H.; Hsu, T.Y.; Kuan, J.T.; Chen, J.C.; Kao, W.F.; Chiu, T.F.; Chen, Y.C.; Chen, H.C. Medical problems requiring mountain rescues from 1985 to 2007 in Yu-Shan National Park, Taiwan. High Alt. Med. Biol. 2009, 10, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.W.; Lin, Y.C.; Chiu, Y.H.; Weng, Y.M.; Li, W.C.; Lin, Y.J.; Wang, S.H.; Hsu, T.Y.; Huang, K.F.; Chiu, T.F. Incidence and risk factors associated with acute mountain sickness in children trekking on Jade Mountain, Taiwan. J. Travel Med. 2016, 23, tav008. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.D.; Vincent, A.L. High Altitude Cerebral Edema. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Dong, J.Q.; Zhang, J.H.; Qin, J.; Li, Q.N.; Huang, W.; Gao, X.B.; Yu, J.; Chen, G.Z.; Tang, X.G.; Huang, L. Anxiety correlates with somatic symptoms and sleep status at high altitudes. Physiol. Behav. 2013, 112–113, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Hüfner, K.; Brugger, H.; Kuster, E.; Dünsser, F.; Stawinoga, A.E.; Turner, R.; Tomazin, I.; Sperner-Unterweger, B. Isolated psychosis during exposure to very high and extreme altitude—Characterisation of a new medical entity. Psychol. Med. 2018, 48, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Bian, S.Z.; Jin, J.; Dong, J.Q.; Li, Q.N.; Yu, J.; Tang, C.F.; Yu, S.Y.; Zhao, X.H.; Qin, J.; Huang, L. A higher baseline somatization score at sea level as an independent predictor of acute mountain sickness. Physiol. Behav. 2016, 167, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Ho Chan, W.S. Taiwan’s healthcare report 2010. EPMA J. 2010, 1, 563–585. [Google Scholar] [CrossRef] [PubMed]
- Wan, F.J.; Chien, W.C.; Chung, C.H.; Yang, Y.J.; Tzeng, N.S. Association between traumatic spinal cord injury and affective and other psychiatric disorders-A nationwide cohort study and effects of rehabilitation therapies. J. Affect. Disord. 2020, 265, 381–388. [Google Scholar] [CrossRef]
- Yeh, T.C.; Chien, W.C.; Chung, C.H.; Liang, C.S.; Chang, H.A.; Kao, Y.C.; Yeh, H.W.; Yang, Y.J.; Tzeng, N.S. Psychiatric Disorders After Traumatic Brain Injury: A Nationwide Population-Based Cohort Study and the Effects of Rehabilitation Therapies. Arch. Phys. Med. Rehabil. 2020, 101, 822–831. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- de Groot, V.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. How to measure comorbidity. a critical review of available methods. J. Clin. Epidemiol. 2003, 56, 221–229. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, R.I.; Feinstein, A.R. The problem of “protopathic bias” in case-control studies. Am. J. Med. 1980, 68, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Usui, C.; Inoue, Y.; Kimura, M.; Kirino, E.; Nagaoka, S.; Abe, M.; Nagata, T.; Arai, H. Irreversible subcortical dementia following high altitude illness. High Alt. Med. Biol. 2004, 5, 77–81. [Google Scholar] [CrossRef]
- Nicolas, M.; Thullier-Lestienne, F.; Bouquet, C.; Gardette, B.; Gortan, C.; Joulia, F.; Bonnon, M.; Richalet, J.P.; Therme, P.; Abraini, J.H. An anxiety, personality and altitude symptomatology study during a 31-day period of hypoxia in a hypobaric chamber (experiment ‘Everest-Comex 1997’). J. Environ. Psychol. 1999, 19, 407–414. [Google Scholar] [CrossRef]
- Bian, S.Z.; Zhang, J.H.; Gao, X.B.; Li, M.; Yu, J.; Liu, X.; Dong, J.Q.; Chen, G.Z.; Huang, L. Risk factors for high-altitude headache upon acute high-altitude exposure at 3700 m in young Chinese men: A cohort study. J. Headache Pain 2013, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, O.O. The Lake Louise Acute Mountain Sickness Score: Still a Headache. High Alt. Med. Biol. 2021, 22, 351–352. [Google Scholar] [CrossRef]
- Jackson, A.; Cavanagh, J.; Scott, J. A systematic review of manic and depressive prodromes. J. Affect. Disord. 2003, 74, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashem, F.H.; Assiri, A.S.; Shatoor, A.S.; Elrefaey, H.M.; Alessa, R.M.; Alkhateeb, M.A. Increased systemic low-grade inflammation in high altitude native rats mediated by adrenergic receptors. Saudi Med. J. 2014, 35, 538–546. [Google Scholar] [CrossRef]
- Park, J.Y.; Hwang, T.K.; Park, H.K.; Ahn, R.S. Differences in cardiovascular and hypothalamic-pituitary-adrenal axis functions between high-altitude visitors and natives during a trek on the Annapurna circuit. Neuroendocrinology 2014, 99, 130–138. [Google Scholar] [CrossRef]
- Prioux-Guyonneau, M.; Mocaër-Cretet, E.; Redjimi-Hafsi, F.; Jacquot, C. Changes in brain 5-hydroxytryptamine metabolism induced by hypobaric hypoxia. Gen. Pharmacol. 1982, 13, 251–254. [Google Scholar] [CrossRef]
- Feddersen, B.; Ausserer, H.; Neupane, P.; Thanbichler, F.; Depaulis, A.; Waanders, R.; Noachtar, S. Right temporal cerebral dysfunction heralds symptoms of acute mountain sickness. J. Neurol. 2007, 254, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Hackett, P.H.; Roach, R.C. High altitude cerebral edema. High Alt. Med. Biol. 2004, 5, 136–146. [Google Scholar] [CrossRef]
- Peck, D.F.; Robertson, A.; Zeffert, S. Psychological sequelae of mountain accidents: A preliminary study. J. Psychosom. Res. 1996, 41, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Roth, W.T.; Gomolla, A.; Meuret, A.E.; Alpers, G.W.; Handke, E.M.; Wilhelm, F.H. High altitudes, anxiety, and panic attacks: Is there a relationship? Depress Anxiety 2002, 16, 51–58. [Google Scholar] [CrossRef]
- Rybnikova, E.A.; Zenko, M.Y.; Barysheva, V.S.; Vetrovoy, O. Acclimatization to Middle Attitude Hypoxia Masks the Symptoms of Experimental Posttraumatic Stress Disorder, but Does Not Affect Its Pathogenetic Mechanisms. Bull. Exp. Biol. Med. 2020, 168, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, N.S.; Chung, C.H.; Lin, F.H.; Chiang, C.P.; Yeh, C.B.; Huang, S.Y.; Lu, R.B.; Chang, H.A.; Kao, Y.C.; Yeh, H.W.; et al. Anti-herpetic Medications and Reduced Risk of Dementia in Patients with Herpes Simplex Virus Infections-a Nationwide, Population-Based Cohort Study in Taiwan. Neurotherapeutics 2018, 15, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Hsu, R.J.; Lin, C.Y.; Chang, F.W.; Huang, C.F.; Chuang, H.C.; Liu, J.M. The association between scabies and myasthenia gravis: A nationwide population-based cohort study. J. Clin. Neurosci. 2017, 45, 115–120. [Google Scholar] [CrossRef]
- Lin, C.Y.; Chang, F.W.; Yang, J.J.; Chang, C.H.; Yeh, C.L.; Lei, W.T.; Huang, C.F.; Liu, J.M.; Hsu, R.J. Increased risk of bipolar disorder in patients with scabies: A nationwide population-based matched-cohort study. Psychiatry Res. 2017, 257, 14–20. [Google Scholar] [CrossRef]
- Tzeng, N.S.; Chang, H.A.; Chung, C.H.; Kao, Y.C.; Chang, C.C.; Yeh, H.W.; Chiang, W.S.; Chou, Y.C.; Chang, S.Y.; Chien, W.C. Increased Risk of Psychiatric Disorders in Allergic Diseases: A Nationwide, Population-Based, Cohort Study. Front. Psychiatry 2018, 9, 133. [Google Scholar] [CrossRef]
- Tzeng, N.S.; Chung, C.H.; Yeh, C.B.; Huang, R.Y.; Yuh, D.Y.; Huang, S.Y.; Lu, R.B.; Chang, H.A.; Kao, Y.C.; Chiang, W.S.; et al. Are Chronic Periodontitis and Gingivitis Associated with Dementia? A Nationwide, Retrospective, Matched-Cohort Study in Taiwan. Neuroepidemiology 2016, 47, 82–93. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Acute Mountain Sickness | 993.2 |
|---|---|
| High altitude periodic breathing | 327.22 |
| Acute mountain sickness only | 993.2 only |
| High altitude cerebral edema | 993.2 + 348.5 (within 1 month after index date) |
| High altitude pulmonary edema | 993.2 + 518.4 (within 1 month after index date) |
| Psychiatric disorders | |
| Dementia | 290.0, 290.10–290.13, 290.20–290.21, 290.3, 290.41–290.43, 290.8–290.9, 331.0 |
| Anxiety disorders | 300 |
| Depressive disorders | 296.2–296.3, 300.4, 311 |
| Bipolar disorders | 296.0, 296.4–296.8 |
| Sleep disorders | 307.4, 780.5 |
| Posttraumatic stress disorder/acute stress disorder | 308, 309.81 |
| Psychotic disorders | 295, 297–298 |
| Schizophrenia | 295 except 295.4 |
| Schizophreniform disorder | 295.4 |
| Other psychotic disorders | 297–298 |
| Substance-related disorders | 291–292, 303.0, 303.9, 304–305 |
| Alcohol use disorder | 291, 303.0, 303.9, 305.0 |
| Illicit drug use disorder | 292, 304–305 except 305.0 |
| AMS | With (n = 127) | Without (n = 1270) | p | ||
|---|---|---|---|---|---|
| Variables | n | % | n | % | |
| Total | 127 | 9.09 | 1270 | 90.91 | |
| Gender | 0.999 | ||||
| Male | 90 | 70.87 | 900 | 70.87 | |
| Female | 37 | 29.13 | 370 | 29.13 | |
| Age (years) | 51.85 ± 17.82 | 51.30 ± 18.11 | 0.748 | ||
| Age groups (yrs) | 0.999 | ||||
| 20–49 | 48 | 37.80 | 480 | 37.80 | |
| 50–64 | 45 | 35.43 | 450 | 35.43 | |
| ≥65 | 34 | 26.77 | 340 | 26.77 | |
| Insured premium (NT$) | 0.111 | ||||
| <18,000 | 123 | 96.85 | 1240 | 97.64 | |
| 18,000–34,999 | 2 | 1.57 | 26 | 2.05 | |
| ≥35,000 | 2 | 1.57 | 4 | 0.31 | |
| CCI_R | 0.41 ± 1.07 | 0.70 ± 1.67 | 0.055 | ||
| CCI_R groups | 0.116 | ||||
| 0 | 99 | 77.95 | 887 | 69.84 | |
| 1 | 15 | 11.81 | 192 | 15.12 | |
| 2 | 9 | 7.09 | 72 | 5.67 | |
| 3 | 2 | 1.57 | 64 | 5.04 | |
| ≥4 | 2 | 1.57 | 55 | 4.33 | |
| Season | 0.999 | ||||
| Spring (Mar–May) | 19 | 14.96 | 190 | 14.96 | |
| Summer (Jun–Aug) | 42 | 33.07 | 420 | 33.07 | |
| Autumn (Sep–Nov) | 43 | 33.86 | 430 | 33.86 | |
| Winter (Dec–Feb) | 23 | 18.11 | 230 | 18.11 | |
| Location | 0.283 | ||||
| Northern Taiwan | 59 | 46.46 | 477 | 37.56 | |
| Middle Taiwan | 34 | 26.77 | 385 | 30.31 | |
| Southern Taiwan | 26 | 20.47 | 334 | 26.30 | |
| Eastern Taiwan | 8 | 6.30 | 69 | 5.43 | |
| Outlets islands | 0 | 0.00 | 5 | 0.39 | |
| Urbanization level | 0.094 | ||||
| 1 (The highest) | 37 | 29.13 | 436 | 34.33 | |
| 2 | 64 | 50.39 | 515 | 40.55 | |
| 3 | 6 | 4.72 | 119 | 9.37 | |
| 4 (The lowest) | 20 | 15.75 | 200 | 15.75 | |
| Level of care | <0.001 | ||||
| Hospital center | 56 | 44.09 | 364 | 28.66 | |
| Regional hospital | 47 | 37.01 | 392 | 30.87 | |
| Local hospital | 24 | 18.90 | 514 | 40.47 | |
| Competing Risk in the Model | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Crude sHR | 95% CI | 95% CI | p | Adjusted sHR | 95% CI | 95% CI | p |
| AMS (reference: without AMS) | 9.999 | 7.123 | 14.036 | <0.001 | 10.384 | 7.267 | 14.838 | <0.001 |
| Male (reference: female) | 1.212 | 0.883 | 1.665 | 0.234 | 1.386 | 0.998 | 1.924 | 0.051 |
| Age 50–64 (reference: age 20–49) | 1.846 | 0.584 | 2.226 | 0.378 | 1.791 | 0.520 | 2.202 | 0.273 |
| Age ≥ 65 (reference: age 20–49) | 1.915 | 0.616 | 2.359 | 0.659 | 1.805 | 0.541 | 2.297 | 0.283 |
| Insured premium (NT$) 18,000–34,999 (reference: Insured premium < 18,000) | 3.218 | 0.798 | 12.976 | 0.100 | 3.262 | 0.750 | 14.192 | 0.115 |
| Insured premium (NT$) ≥ 35,000 (reference: Insured premium < 18,000) | 0.378 | 0.094 | 1.522 | 0.171 | 0.403 | 0.099 | 1.634 | 0.203 |
| CCI = 1 (reference: CCI = 0) | 1.020 | 0.715 | 1.456 | 0.912 | 0.953 | 0.659 | 1.379 | 0.799 |
| CCI = 2 (reference: CCI = 0) | 1.118 | 0.683 | 1.830 | 0.657 | 1.328 | 0.790 | 2.233 | 0.284 |
| CCI = 3 (reference: CCI = 0) | 0.991 | 0.565 | 1.737 | 0.974 | 1.084 | 0.604 | 1.944 | 0.787 |
| CCI ≥ 4 (reference: CCI = 0) | 0.814 | 0.470 | 1.410 | 0.463 | 0.994 | 0.650 | 2.050 | 0.625 |
| Season Summer (reference: spring) | 1.512 | 1.004 | 2.279 | 0.048 | 1.509 | 0.993 | 2.294 | 0.054 |
| Season Autumn (reference: spring) | 1.194 | 0.767 | 1.858 | 0.433 | 1.310 | 0.835 | 2.054 | 0.240 |
| Season Winter (reference: spring) | 1.245 | 0.797 | 1.946 | 0.335 | 1.163 | 0.736 | 1.835 | 0.518 |
| Urbanization level | ||||||||
| 1 (The highest) | 1.150 | 0.768 | 1.721 | 0.498 | 1.091 | 0.693 | 1.719 | 0.706 |
| 2 | 1.146 | 0.663 | 1.980 | 0.625 | 1.049 | 0.585 | 1.879 | 0.873 |
| 3 | 0.802 | 0.565 | 1.140 | 0.220 | 0.809 | 0.580 | 0.170 | 0.260 |
| 4 (The lowest) | Reference | Reference | ||||||
| Medical center (reference: Local hospital) | 1.800 | 1.228 | 2.639 | 0.003 | 1.698 | 1.092 | 2.639 | 0.019 |
| Regional hospital (reference: Local hospital) | 1.387 | 0.974 | 1.974 | 0.070 | 1.168 | 0.785 | 1.739 | 0.443 |
| AMS | No competing Risk in the Model | Competing Risk in the Model | ||||||
|---|---|---|---|---|---|---|---|---|
| Stratified | Adjusted HR | 95% CI | 95% CI | p | Adjusted sHR | 95% CI | 95% CI | p |
| Total | 10.609 | 7.424 | 15.159 | <0.001 | 10.384 | 7.267 | 14.838 | <0.001 |
| Gender | ||||||||
| Male | 10.855 | 7.596 | 15.510 | <0.001 | 10.625 | 7.435 | 15.182 | <0.001 |
| Female | 10.182 | 7.125 | 14.549 | <0.001 | 9.966 | 6.975 | 14.241 | <0.001 |
| Age groups (years) | ||||||||
| 20–49 | 10.057 | 7.038 | 14.370 | <0.001 | 9.844 | 6.889 | 14.066 | <0.001 |
| 50–64 | 10.283 | 7.196 | 14.692 | <0.001 | 10.064 | 7.043 | 14.381 | <0.001 |
| ≥65 | 11.180 | 7.823 | 15.974 | <0.001 | 10.942 | 7.658 | 15.636 | <0.001 |
| Insured premium (NT$) | ||||||||
| <18,000 | 10.296 | 7.205 | 14.711 | <0.001 | 10.077 | 7.052 | 14.400 | <0.001 |
| 18,000–34,999 | 55.592 | 38.902 | 79.434 | <0.001 | 54.413 | 38.079 | 77.752 | <0.001 |
| ≥35,000 | 6.551 | 4.584 | 9.360 | <0.001 | 6.412 | 4.487 | 9.162 | <0.001 |
| CCI_R groups | ||||||||
| 0 | 12.043 | 8.428 | 17.208 | <0.001 | 11.788 | 8.249 | 16.844 | <0.001 |
| 1 | 6.729 | 4.709 | 9.615 | <0.001 | 6.587 | 4.609 | 9.412 | <0.001 |
| 2 | 18.686 | 13.076 | 26.701 | <0.001 | 18.290 | 12.800 | 26.135 | <0.001 |
| 3 | 19.960 | 13.968 | 28.521 | <0.001 | 19.537 | 13.673 | 27.917 | <0.001 |
| ≥4 | 7.257 | 5.079 | 10.370 | <0.001 | 7.104 | 4.971 | 10.150 | <0.001 |
| Season | ||||||||
| Spring | 6.886 | 4.818 | 9.839 | <0.001 | 6.740 | 4.717 | 9.630 | <0.001 |
| Summer | 15.289 | 10.699 | 21.846 | <0.001 | 14.965 | 10.473 | 21.383 | <0.001 |
| Autumn | 12.662 | 8.861 | 18.092 | <0.001 | 12.393 | 8.673 | 17.709 | <0.001 |
| Winter | 7.265 | 5.084 | 10.381 | <0.001 | 7.111 | 4.976 | 10.161 | <0.001 |
| Urbanization level | ||||||||
| 1 (The highest) | 13.753 | 9.624 | 19.652 | <0.001 | 13.462 | 9.421 | 19.236 | <0.001 |
| 2 | 13.398 | 9.376 | 19.144 | <0.001 | 13.114 | 9.178 | 18.739 | <0.001 |
| 3 | 5.195 | 3.636 | 7.424 | <0.001 | 5.085 | 3.559 | 7.266 | <0.001 |
| 4 (The lowest) | 5.624 | 3.936 | 8.036 | <0.001 | 5.505 | 3.852 | 7.866 | <0.001 |
| Level of care | ||||||||
| Medical center | 28.888 | 20.215 | 41.277 | <0.001 | 28.275 | 19.788 | 40.403 | <0.001 |
| Regional hospital | 10.378 | 7.262 | 14.828 | <0.001 | 10.158 | 7.109 | 14.514 | <0.001 |
| Local hospital | 5.124 | 3.586 | 7.322 | <0.001 | 5.016 | 3.510 | 7.167 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-H.; Chien, W.-C.; Chung, C.-H.; Her, Y.-N.; Yao, C.-Y.; Lee, B.-L.; Li, F.-L.; Wan, F.-J.; Tzeng, N.-S. Acute Mountain Sickness and the Risk of Subsequent Psychiatric Disorders—A Nationwide Cohort Study in Taiwan. Int. J. Environ. Res. Public Health 2023, 20, 2868. https://doi.org/10.3390/ijerph20042868
Wang Y-H, Chien W-C, Chung C-H, Her Y-N, Yao C-Y, Lee B-L, Li F-L, Wan F-J, Tzeng N-S. Acute Mountain Sickness and the Risk of Subsequent Psychiatric Disorders—A Nationwide Cohort Study in Taiwan. International Journal of Environmental Research and Public Health. 2023; 20(4):2868. https://doi.org/10.3390/ijerph20042868
Chicago/Turabian StyleWang, Ya-Hsuan, Wu-Chien Chien, Chi-Hsiang Chung, Yu-Ning Her, Chia-Yi Yao, Biing-Luen Lee, Fang-Ling Li, Fang-Jung Wan, and Nian-Sheng Tzeng. 2023. "Acute Mountain Sickness and the Risk of Subsequent Psychiatric Disorders—A Nationwide Cohort Study in Taiwan" International Journal of Environmental Research and Public Health 20, no. 4: 2868. https://doi.org/10.3390/ijerph20042868
APA StyleWang, Y. -H., Chien, W. -C., Chung, C. -H., Her, Y. -N., Yao, C. -Y., Lee, B. -L., Li, F. -L., Wan, F. -J., & Tzeng, N. -S. (2023). Acute Mountain Sickness and the Risk of Subsequent Psychiatric Disorders—A Nationwide Cohort Study in Taiwan. International Journal of Environmental Research and Public Health, 20(4), 2868. https://doi.org/10.3390/ijerph20042868