
An Intensive Longitudinal Assessment Approach to Surveilling Trajectories of Burnout over the First Year of the COVID Pandemic

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Transparency and Openness
2.2. Overview
2.3. Participants and Recruitment
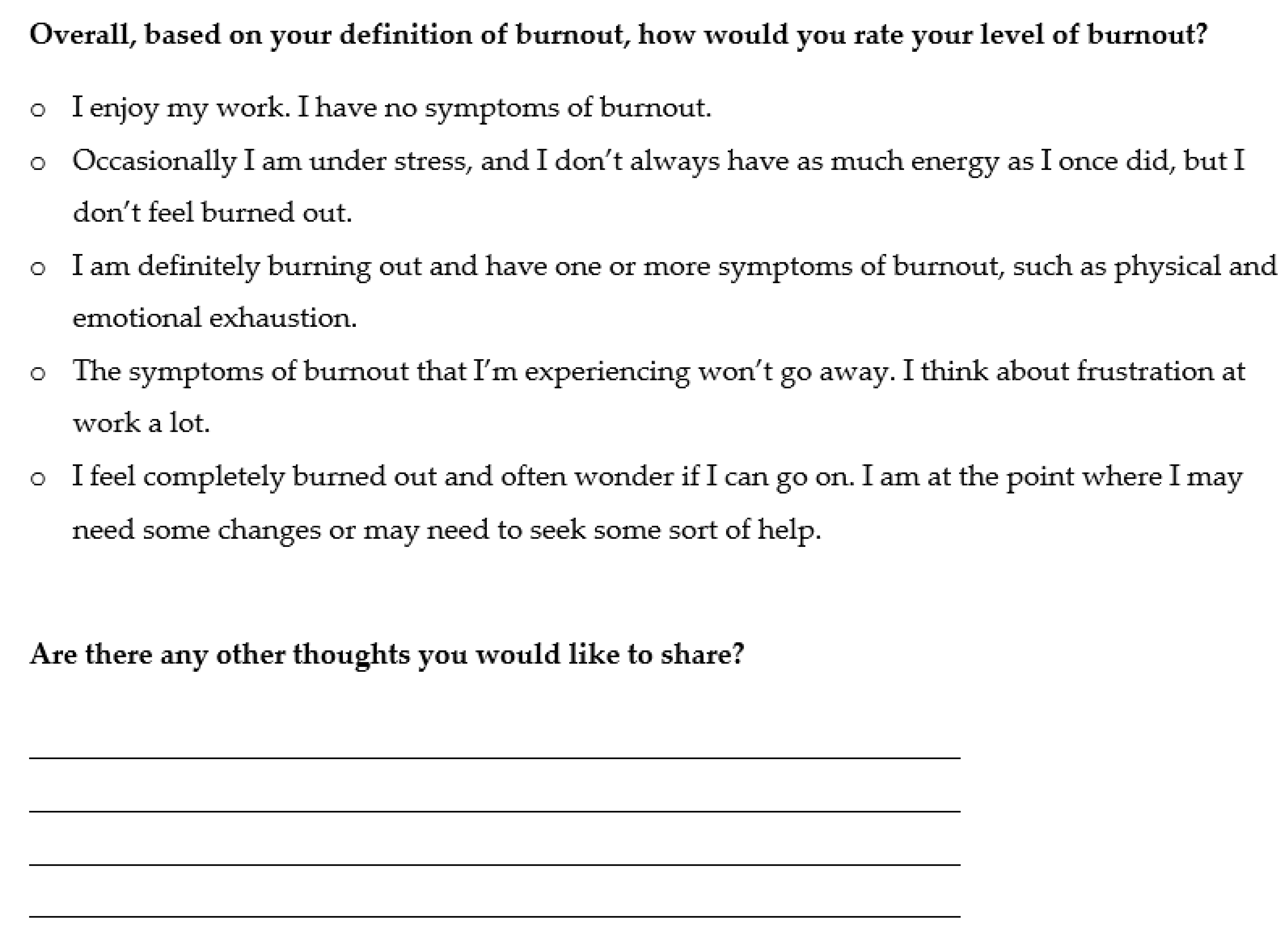
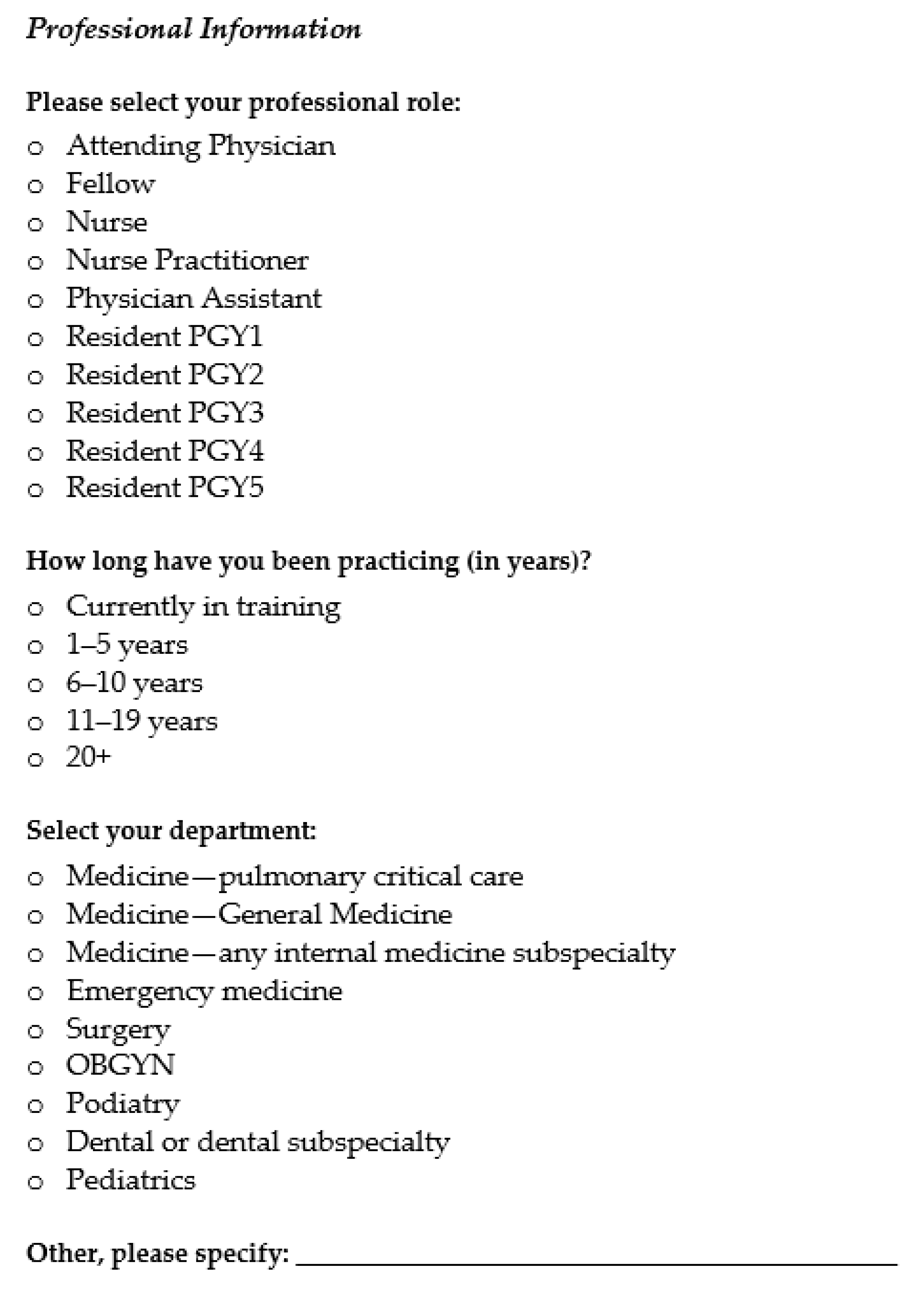
2.4. Survey Measures
2.5. Data Analysis
3. Results
3.1. Response Rate and Personal and Professional Correlates of Response
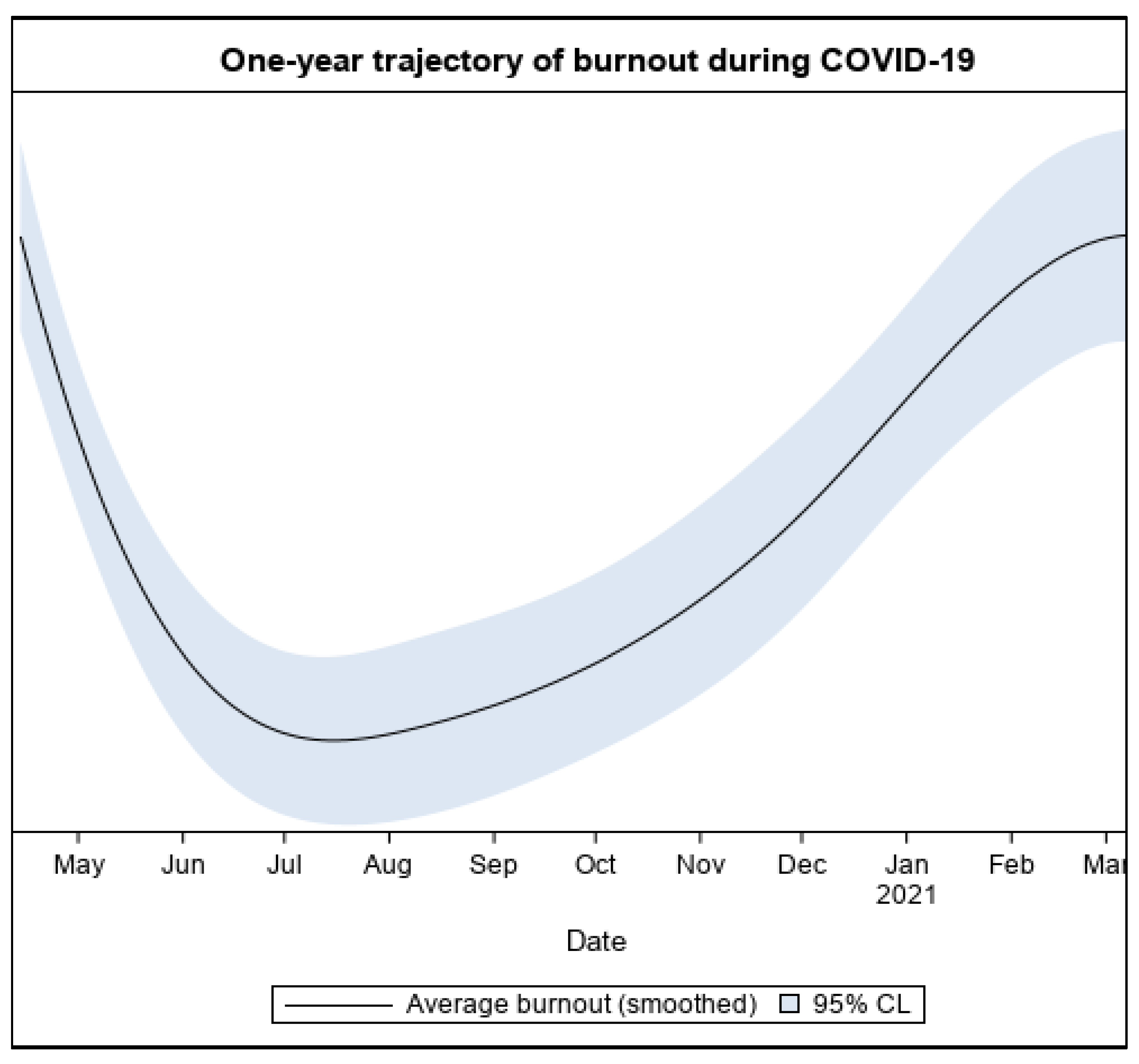
3.2. Initial and Subsequent Burnout Rates
3.3. Caseload and Burnout
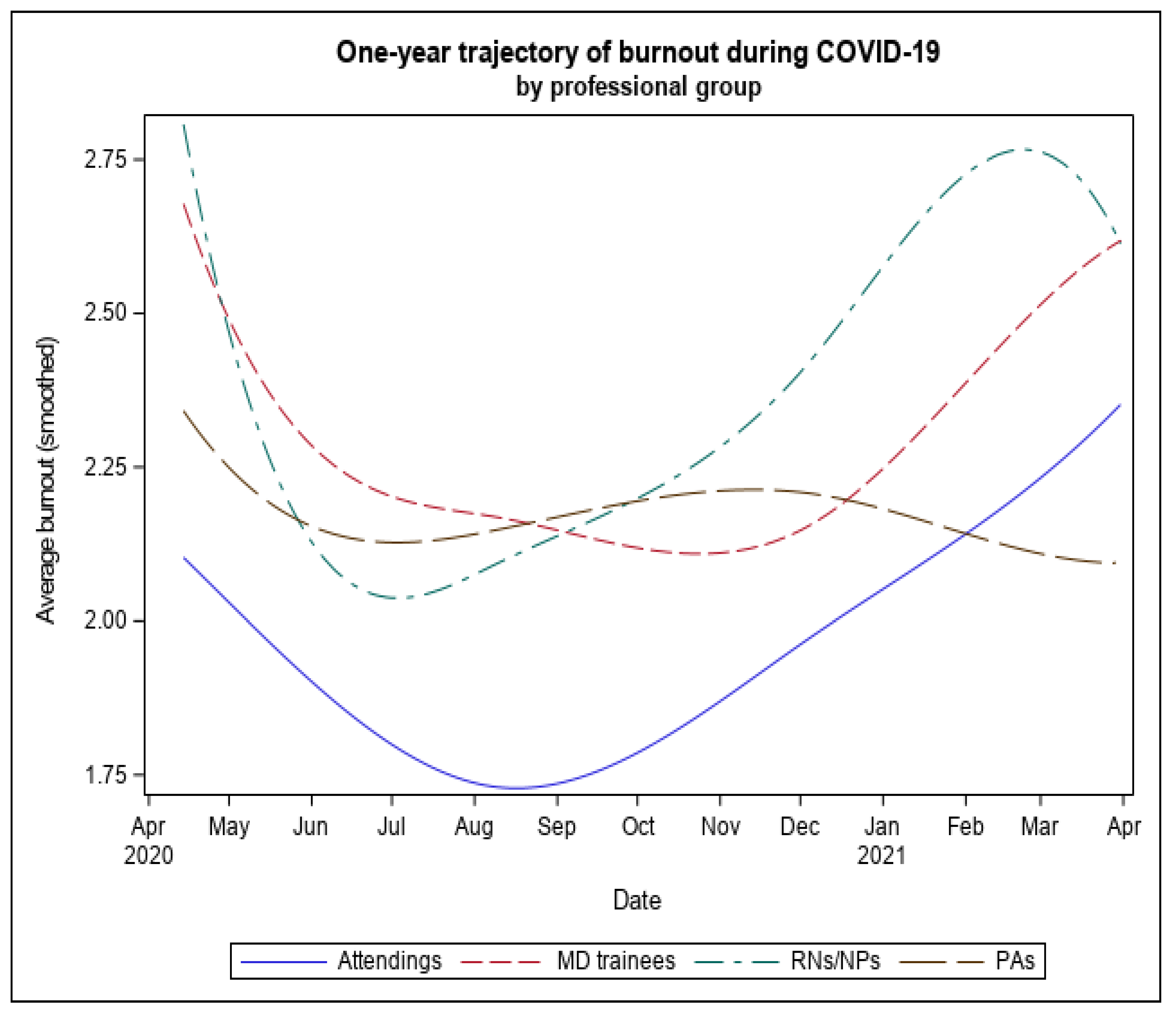
3.4. Professional Role Differences in Burnout
3.5. Participants’ Personal and Professional Resources and Burnout
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A





References
- Norful, A.A.; Rosenfeld, A.; Schroeder, K.; Travers, J.; Aliyu, S. Primary drivers and psychological manifestations of stress in frontline healthcare workforce during the initial COVID-19 outbreak in the United States. Gen. Hosp. Psychiatry 2021, 69, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shirom, A.; Nirel, N.; Vinokur, A.D. Work hours and caseload as predictors of physician burnout: The Mediating Effects by Perceived Workload and by Autonomy. Appl. Psychol. 2010, 59, 539–565. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Burnout. In Stress and Quality of Working Life: Current Perspectives in Occupational Health, 37th ed.; Information Age Publishing: Greenwich, CT, USA, 2006; pp. 42–49. [Google Scholar]
- Cimiotti, J.P.; Aiken, L.H.; Sloane, D.M.; Wu, E.S. Nurse staffing, burnout, and health care-associated infection. Am. J. Infect. Control 2012, 40, 486–490. [Google Scholar] [PubMed]
- Tawfik, D.S.; Profit, J.; Morgenthaler, T.I.; Satele, D.V.; Sinsky, C.A.; Dyrbye, L.N.; Tutty, M.A.; West, C.P.; Shanafelt, T.D. Physician Burnout, Well-being, and Work Unit Safety Grades in Relationship to Reported Medical Errors. Mayo Clin. Proc. 2018, 93, 1571–1580. [Google Scholar] [CrossRef]
- Dewa, C.S.; Loong, D.; Bonato, S.; Trojanowski, L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: A systematic review. BMJ Open 2017, 7, e015141. [Google Scholar] [CrossRef] [PubMed]
- Halbesleben, J.R.B.; Rathert, C. Linking physician burnout and patient outcomes: Exploring the dyadic relationship between physicians and patients. Health Care Manag. Rev. 2008, 33, 29–39. [Google Scholar]
- National Academies of Sciences, Engineering, Medicine. Taking Action against Clinician Burnout: A Systems Approach to Professional Well-Being; The National Academies Press: Washington, DC, USA, 2019. [Google Scholar]
- Salyers, M.P.; Bonfils, K.A.; Luther, L.; Firmin, R.L.; White, D.A.; Adams, E.L.; Rollins, A.L. The Relationship Between Professional Burnout and Quality and Safety in Healthcare: A Meta-Analysis. J. Gen. Intern. Med. 2017, 32, 475–482. [Google Scholar]
- Welp, A.; Meier, L.L.; Manser, T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Front. Psychol. 2015, 5, 1573. [Google Scholar]
- De Paiva, L.C.; Gomes Canário, A.C.; Corsino de Paiva China, E.L.; Gonçalves, A.K. Burnout syndrome in health-care professionals in a university hospital. Clinics 2017, 72, 305–309. [Google Scholar]
- Shanafelt, T.D.; Mungo, M.; Schmitgen, J.; Storz, K.A.; Reeves, D.; Hayes, S.N.; Sloan, J.A.; Swensen, S.J.; Buskirk, S.J. Longitudinal Study Evaluating the Association Between Physician Burnout and Changes in Professional Work Effort. Mayo Clin. Proc. 2016, 9, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Willard-Grace, R.; Knox, M.; Huang, B.; Hammer, H.; Kivlahan, C.; Grumbach, K. Burnout and health care workforce turnover. Ann. Fam. Med. 2019, 17, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Mealer, M.; Burnham, E.L.; Goode, C.J.; Rothbaum, B.; Moss, M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress. Anxiety 2009, 26, 1118–1126. [Google Scholar] [PubMed]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General US Population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar]
- Abhiram, K.; Tan, B.Y.; Tan, M.; Tan, L.; Sia, C.-H.; Chua, Y.X.; Lim, L.J.; Suppiah, C.M.; Sim, K.; Chan, Y.H.; et al. The Effect of COVID-19 Endemicity on the Mental Health of Health Workers. J. Am. Med. Dir. Assoc. 2022, 23, 405–413.e3. [Google Scholar] [CrossRef]
- Miotto, K.; Sanford, J.; Brymer, M.J.; Bursch, B.; Pynoos, R.S. Implementing an Emotional Support and Mental Health Response Plan for Healthcare Workers During the COVID-19 Pandemic. Psychol. Trauma Theory Res. Pr. Policy 2020, 12, 165–167. [Google Scholar] [CrossRef]
- Ehrlich, H.; McKenney, M.; Elkbuli, A. Protecting our healthcare workers during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 1527–1528. [Google Scholar] [CrossRef]
- Institute for Healthcare Improvement. A Guide to Promoting Health Care Workforce Well-Being During and After the COVID-19 Pandemic; Institute for Healthcare Improvement: Boston, MA, USA, 2020; Available online: www.ihi.org (accessed on 16 February 2022).
- Esmaeilzadeh, P.; Mirzaei, T. Using electronic health records to mitigate workplace burnout among clinicians during the COVID-19 pandemic: Field study in Iran. JMIR Med. Inform. 2021, 9, e28497. [Google Scholar]
- Wu, Y.; Wang, J.; Luo, C.; Hu, S.; Lin, X.; Anderson, A.E.; Bruera, E.; Yang, X.; Wei, S.; Qian, Y. A Comparison of Burnout Frequency Among Oncology Physicians and Nurses Working on the Frontline and Usual Wards During the COVID-19 Epidemic in Wuhan, China. J. Pain Symptom Manag. 2020, 60, e60–e65. [Google Scholar] [CrossRef]
- Afulani, P.A.; Gyamerah, A.O.; Nutor, J.J.; Laar, A.; Aborigo, R.A.; Malechi, H.; Sterling, M.; Awoonor-Williams, J.K. Inadequate preparedness for response to COVID-19 is associated with stress and burnout among healthcare workers in Ghana. PLoS ONE 2021, 16, e0250294. [Google Scholar]
- Azoulay, E.; De Waele, J.; Ferrer, R.; Staudinger, T.; Borkowska, M.; Povoa, P.; Iliopoulou, K.; Artigas, A.; Schaller, S.J.; Hari, M.S.; et al. Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann. Intensiv. Care 2020, 10, 110. [Google Scholar] [CrossRef]
- Denning, M.; Goh, E.T.; Tan, B.; Kanneganti, A.; Almonte, M.; Scott, A.; Martin, G.; Clarke, J.; Sounderajah, V.; Markar, S.; et al. Determinants of burnout and other aspects of psychological well-being in healthcare workers during the COVID-19 pandemic: A multinational cross-sectional study. PLoS ONE 2021, 16, e0238666. [Google Scholar]
- Dimitriu, M.; Pantea-Stoian, A.; Smaranda, A.C.; Nica, A.A.; Carap, A.C.; Constantin, V.D.; Davitoiu, A.M.; Cirstoveanu, C.; Bacalbasa, N.; Bratu, O.G.; et al. Burnout syndrome in Romanian medical residents in time of the COVID-19 pandemic. Med. Hypotheses 2020, 144, 109972. [Google Scholar] [CrossRef]
- Petrikov, S.; Kholmogorova, A.B.; Suroegina, A.Y.; Mikita, O.Y.; Roy, A.P.; Rakhmanina, A.A. Professional burnout, symptoms of emotional distress and disstress among healthcare workers during the COVID-19 epidemic. Couns. Psychol. Psychother. 2020, 28, 8–45. [Google Scholar] [CrossRef]
- Bryant, R.A. Acute Stress Disorder as a Predictor of Posttraumatic Stress Disorder: A Systematic Review. J. Clin. Psychiatry 2011, 72, 233. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.E.; Stone, A.A. The Analysis of Real-Time Momentary Data: A Practical Guide. In The Science and Theory of Real-Time Data Capture; Oxford University Press: Oxford, UK, 2007; pp. 76–113. [Google Scholar]
- Engelen, L.; Chau, J.Y.; Burks-Young, S.; Bauman, A. Application of ecological momentary assessment in workplace health evaluation. Health Promot. J. Aust. 2016, 27, 259–263. [Google Scholar]
- Chor, W.P.D.; Ng, W.M.; Cheng, L.; Situ, W.; Chong, J.W.; Ng, L.Y.A.; Mok, P.L.; Yau, Y.W.; Lin, Z. Burnout amongst emergency healthcare workers during the COVID-19 pandemic: A multi-center study. Am. J. Emerg. Med. 2021, 46, 700–702. [Google Scholar]
- HaGani, N.; Yagil, D.; Cohen, M. Burnout among oncologists and oncology nurses: A systematic review and meta-analysis. Health Psychol. 2022, 41, 53–64. [Google Scholar] [CrossRef]
- Lanners, M.S. Are Teachers More Affected by Burnout than Physicians, Nurses and Other Professionals? A Systematic Review of the Literature; Advances in Intelligent Systems and Computing; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; Volume 957, pp. 147–155. [Google Scholar] [CrossRef]
- Velando-Soriano, A.; Ortega-Campos, E.; Gómez-Urquiza, J.L.; Ramírez-Baena, L.; De La Fuente, E.I.; Cañadas-De La Fuente, G.A. Impact of social support in preventing burnout syndrome in nurses: A systematic review. Jpn. J. Nurs. Sci. 2020, 17, e12269. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.; Zhao, S.; Gao, X.; An, Z.; Wang, S.; Li, H.; Li, Y.; Gao, L.; Lu, L.; Dong, Z. General self-efficacy modifies the effect of stress on burnout in nurses with different personality types. BMC Health Serv. Res. 2018, 18, 667. [Google Scholar] [CrossRef]
- Tan, K.-L.; Yeap, P.F. The impact of work engagement and meaningful work to alleviate job burnout among social workers in New Zealand. Manag. Decis. 2022, 60, 3042–3065. [Google Scholar] [CrossRef]
- Cotel, A.; Golu, F.; Pantea Stoian, A.; Dimitriu, M.; Socea, B.; Cirstoveanu, C.; Davitoiu, A.; Alexe, F.J.; Oprea, B. Predictors of Burnout in Healthcare Workers during the COVID-19 Pandemic. Healthcare 2021, 9, 304. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 45120, 867–872. [Google Scholar]
- Gorin, A.; Stone, A.A. Recall biases and cognitive errors in retrospective self-reports: A call for momentary assessments. Handb. Health Psychol. 2001, 23, 405–413. [Google Scholar]
- Testoni, I.; Brondolo, E.; Ronconi, L.; Petrini, F.; Navalesi, P.; Antonellini, M.; Biancalani, G.; Crupi, R.; Capozza, D. Burnout following moral injury and dehumanization: A study of distress among Italian medical staff during the first COVID-19 pandemic period. Psychol. TraumaTheory Res. Pr. Policy 2022. [Google Scholar] [CrossRef]
- Bandura, A. Guide for constructing self-efficacy scales. In Self-Efficacy Beliefs of Adolescents, 5th ed.; IAP: Greenwich, CT, USA, 2006; pp. 307–337. [Google Scholar]
- Cheraghi, F.; Hassani, P.; Yaghmaei, F.; Alavi-Majed, H. Developing a valid and reliable self-efficacy in clinical performance scale. Int. Nurs. Rev. 2009, 56, 214–221. [Google Scholar] [CrossRef]
- Dolan, E.D.; Mohr, D.; Lempa, M.; Joos, S.; Fihn, S.D.; Nelson, K.M.; Helfrich, C.D. Using a Single Item to Measure Burnout in Primary Care Staff: A Psychometric Evaluation. J. Gen. Intern. Med. 2015, 30, 582–587. [Google Scholar] [PubMed]
- Helfrich, C.D.; Simonetti, J.A.; Clinton, W.L.; Wood, G.B.; Taylor, L.; Schectman, G.; Stark, R.; Rubenstein, L.V.; Fihn, S.D.; Nelson, K.M. The Association of Team-Specific Workload and Staffing with Odds of Burnout Among VA Primary Care Team Members. J. Gen. Intern. Med. 2017, 32, 760–766. [Google Scholar]
- Linzer, M.; Manwell, L.B.; Williams, E.S.; Bobula, J.A.; Brown, R.L.; Varkey, A.B.; Man, B.; McMurray, J.E.; Maguire, A.; Horner-Ibler, B.; et al. Improving Patient Care Annals of Internal Medicine Working Conditions in Primary Care: Physician Reactions and Care Quality. Ann. Intern. Med. 2009, 151, 28–36. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19581644 (accessed on 8 January 2021).
- Schafer, J.L.; Yucel, R.M. Computational strategies for multivariate linear mixed-effects models with missing values. J. Comput. Graph. Stat. 2002, 11, 437–457. [Google Scholar]
- Shanafelt, T.D.; Hasan, O.; Dyrbye, L.N.; Sinsky, C.; Satele, D.; Sloan, J.; West, C.P. Changes in Burnout and Satisfaction With Work-Life Balance in Physicians and the General US Working Population Between 2011 and 2014. In Mayo Clinical Proceedings; Elsevier: Amsterdam, The Netherlands, 2016; Volume 90, pp. 1600–1613. [Google Scholar] [CrossRef]
- Vandenbroeck, S.; Van Gerven, E.; De Witte, H.; Vanhaecht, K.; Godderis, L. Burnout in Belgian physicians and nurses. Occup. Med. 2017, 67, 546–554. [Google Scholar]
- Surgeon General of the United States. Addressing Health Worker Burnout. 2022. Available online: https://www.hhs.gov/sites/default/files/health-worker-wellbeing-advisory.pdf (accessed on 26 July 2022).
- Taylor, M.J.; McNicholas, C.; Nicolay, C.; Darzi, A.; Bell, D.; Reed, J.E. Systematic review of the application of the plan-do-study-act method to improve quality in healthcare. BMJ Qual. Saf. 2014, 23, 290–298. [Google Scholar] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Grace, M.K.; VanHeuvelen, J.S. Occupational variation in burnout among medical staff: Evidence for the stress of higher status. Soc. Sci. Med. 2019, 232, 199–208. [Google Scholar] [CrossRef]
- Kelley, M.M.; Zadvinskis, I.M.; Miller, P.S.; Monturo, C.; Norful, A.A.; O’Mathúna, D.; Roberts, H.; Smith, J.; Tucker, S.; Zellefrow, C.; et al. United States nurses’ experiences during the COVID-19 pandemic: A grounded theory. J. Clin. Nurs. 2021, 31, 2167–2180. [Google Scholar] [PubMed]
- Schroeder, K.; Norful, A.A.; Travers, J.; Aliyu, S. Nursing perspectives on care delivery during the early stages of the COVID-19 pandemic: A qualitative study. Int. J. Nurs. Stud. Adv. 2020, 2, 100006. [Google Scholar] [CrossRef] [PubMed]
- Dewey, C.; Hingle, S.; Goelz, E.; Linzer, M. Supporting Clinicians During the COVID-19 Pandemic. Ann. Intern. Med. 2020, 172, 752–753. [Google Scholar] [CrossRef] [PubMed]
- Ben-Porat, A.; Itzhaky, H. Burnout among trauma social workers: The contribution of personal and environmental resources. J. Soc. Work. 2015, 15, 606–620. [Google Scholar]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Methods 2002, 7, 147–177. [Google Scholar]
- King, K.M.; Littlefield, A.K.; McCabe, C.J.; Mills, K.L.; Flournoy, J.; Chassin, L. Longitudinal modeling in developmental neuroimaging research: Common challenges, and solutions from developmental psychology. Dev. Cogn. Neurosci. 2018, 33, 54–72. [Google Scholar] [CrossRef]
- NYC Health Department. COVID-19: Data on Vaccines-NYC Health. Available online: https://www.nyc.gov/site/doh/covid/covid-19-data-vaccines.page#trends (accessed on 10 August 2022).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Full Sample | Attending Physicians | Residents and Fellows | Nurses and Nurse Practitioners | Physician Assistants |
|---|---|---|---|---|---|
| n, % of total who received the survey invitation | 398 (19.7%) of the 2023 who received the survey invitation | 86 (23.1%) of 373 Attending Physicians who received the survey invitation | 61 (22.8%) of 267 Residents and Fellows who received the survey invitation (Residents: n = 57/251; Fellows: n = 4/16) | 209 [17.8%) of 1177 Nurses and Nurse Practitioners who received the survey invitation (Nurse: n = 199/1144; Nurse Practitioner: n = 10/33) | 42 (20.4%) of 206 Physician Assistants who received the survey invitation |
| Sex (n = 398) 1 | |||||
| Men | 121 (30.4) | 49 (57.0) | 32 (52.5) | 26 [12.4) | 14 (33.3) |
| Women | 277 (69.6) | 37 (43.0) | 29 (47.5) | 183 (87.6) | 28 (66.7) |
| Age (n = 388) 1 | |||||
| <34 | 149 (38.4) | 15 [17.9) | 52 (86.7) | 62 (30.5) | 20 (48.8) |
| 35–49 | 157 (40.5) | 42 (50.0) | 8 [13.3) | 91 (44.8) | 16 (39.0) |
| 50–59 | 47 [12.1) | 15 [17.9) | 0 (0) | 30 [14.8) | 2 (4.9) |
| 60+ | 35 (9.0) | 12 [14.3) | 0 (0) | 20 (9.9) | 3 (7.3) |
| Race and Ethnicity (n = 387) 1 | |||||
| White | 145 (37.5) | 43 (51.2) | 22 (36.7) | 62 (30.7) | 18 (43.9) |
| Chinese | 58 [15.0) | 15 [17.9) | 10 [16.7) | 24 [11.9) | 9 (22.0) |
| Black | 40 [10.3) | 2 (2.4) | 3 (5.0) | 34 [16.8) | 1 (2.4) |
| Asian Indian | 36 (9.3) | 13 [15.5) | 8 [13.3) | 13 (6.4) | 2 (4.9) |
| Latinx | 30 (7.8) | 3 (3.6) | 1 [1.7) | 19 (9.4) | 7 [17.1) |
| Other 2 | 78 (20.2) | 8 (9.5) | 16 (26.7) | 50 (24.8) | 4 (9.8) |
| Group | N (%) Reporting Any Burnout | OR, 95% CI 1 |
|---|---|---|
| Sex a (n = 373) | ||
| Men | 33 (29.2) | 0.38 (0.24–0.61) |
| Women | 136 (52.3) | |
| Age b (n = 358) | ||
| <35 years | 77 (54.6) | 4.40 [1.78–10.87) |
| 35–49 years | 63 (44.4) | 2.83 [1.15–6.97) |
| 50–59 years | 13 (30.2) | 1.61 (0.55–4.66) |
| 60 or more years | 7 (21.9) | |
| Professional Role c,d (n = 373) | ||
| Trainees (Residents and Fellows) | 26 (44.83) | 2.16 [1.06–4.42) |
| Nurses and Nurse Practitioners | 109 (55.61) | 3.32 [1.89–5.86) |
| Physician Assistants | 12 (31.58) | 1.22 (0.53–2.84) |
| Attending Physicians | 22 (27.16) | - |
| Department of Medicine e (n = 357) | ||
| Yes | 55 (50.0) | 1.01 (0.99–1.03) |
| No | 106 (42.91) | - |
| Out of Role f (n = 371) | ||
| Yes | 78 (53.06) | 1.75 [1.14–2.68) |
| No | 90 (40.18) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, C.X.; Crupi, R.; August, P.; Sundaram, V.; Norful, A.A.; Schwartz, J.E.; Miele, A.S.; Simons, R.R.; Mikrut, E.E.; Brondolo, E. An Intensive Longitudinal Assessment Approach to Surveilling Trajectories of Burnout over the First Year of the COVID Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 2930. https://doi.org/10.3390/ijerph20042930
Pan CX, Crupi R, August P, Sundaram V, Norful AA, Schwartz JE, Miele AS, Simons RR, Mikrut EE, Brondolo E. An Intensive Longitudinal Assessment Approach to Surveilling Trajectories of Burnout over the First Year of the COVID Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(4):2930. https://doi.org/10.3390/ijerph20042930
Chicago/Turabian StylePan, Cynthia X., Robert Crupi, Phyllis August, Varuna Sundaram, Allison A. Norful, Joseph E. Schwartz, Andrew S. Miele, R. Rhiannon Simons, Emilia E. Mikrut, and Elizabeth Brondolo. 2023. "An Intensive Longitudinal Assessment Approach to Surveilling Trajectories of Burnout over the First Year of the COVID Pandemic" International Journal of Environmental Research and Public Health 20, no. 4: 2930. https://doi.org/10.3390/ijerph20042930
APA StylePan, C. X., Crupi, R., August, P., Sundaram, V., Norful, A. A., Schwartz, J. E., Miele, A. S., Simons, R. R., Mikrut, E. E., & Brondolo, E. (2023). An Intensive Longitudinal Assessment Approach to Surveilling Trajectories of Burnout over the First Year of the COVID Pandemic. International Journal of Environmental Research and Public Health, 20(4), 2930. https://doi.org/10.3390/ijerph20042930