

Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Methods
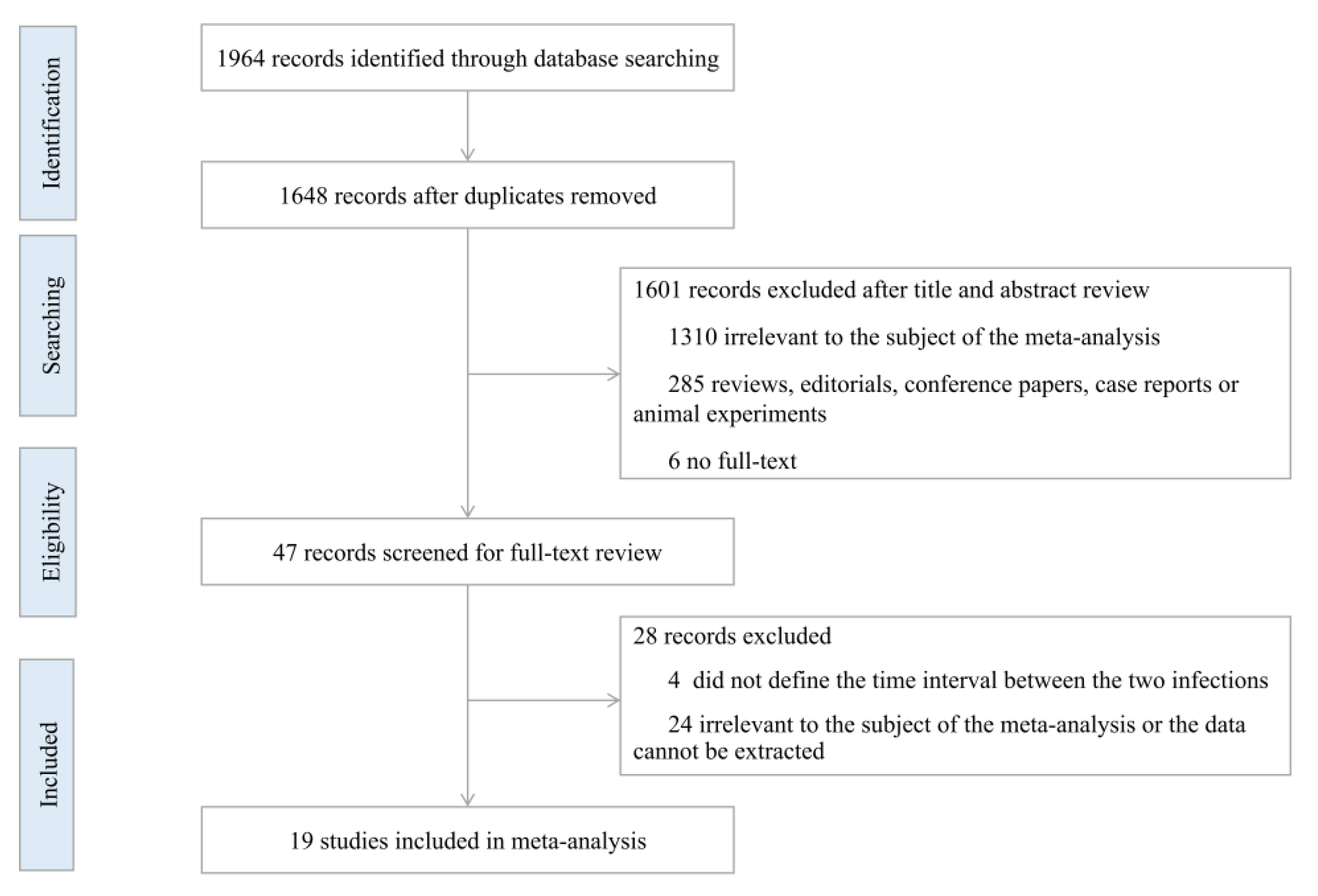
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction
2.3. Quality Assessment and Risk of Bias
2.4. Data Synthesis and Statistical Analysis
3. Results
3.1. Basic Characteristics
3.2. Pooled Prevalence (PP) of Severity and Outcomes of SARS-CoV-2 Reinfection
3.3. Pooled Prevalence (PP) of Symptoms among Symptomatic SARS-CoV-2 Reinfection Cases
3.4. Comparison of Severity and Outcomes of SARS-CoV-2 Reinfection and Primary Infection
3.5. Quality Evaluation and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| RBD | receptor binding domain |
| RT-PCR | reverse transcription–polymerase chain reaction |
| UK | United Kingdom |
| ICU | intensive care unit |
| WHO | World Health Organization |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PP | pooled prevalence |
| OR | odds ratio |
| CI | confidence interval |
| HR | hazard ratio |
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 9 February 2023).
- Xuechun, M.; Linghang, W. Research progress in the reinfection of novel coronavirus. Chin. Med. J. 2022, 102, 3229–3232. [Google Scholar] [CrossRef]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.W. Omicron Variant (B.1.1.529): Infectivity, Vaccine Breakthrough, and Antibody Resistance. J. Chem. Inf. Model. 2022, 62, 412–422. [Google Scholar] [CrossRef]
- Chen, J.; Wei, G.W. Omicron BA.2 (B.1.1.529.2): High Potential for Becoming the Next Dominant Variant. J. Phys. Chem. Lett. 2022, 13, 3840–3849. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Investigative Criteria for Suspected Cases of SARS-CoV-2 Reinfection (ICR). Available online: https://stacks.cdc.gov/view/cdc/96072 (accessed on 30 December 2022).
- To, K.K.; Hung, I.F.; Ip, J.D.; Chu, A.W.; Chan, W.M.; Tam, A.R.; Fong, C.H.; Yuan, S.; Tsoi, H.W.; Ng, A.C.; et al. Coronavirus Disease 2019 (COVID-19) Re-infection by a Phylogenetically Distinct Severe Acute Respiratory Syndrome Coronavirus 2 Strain Confirmed by Whole Genome Sequencing. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e2946–e2951. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Acuti Martellucci, C.; Baccolini, V.; De Vito, C.; Renzi, E.; Villari, P.; Manzoli, L. Risk of reinfection and disease after SARS-CoV-2 primary infection: Meta-analysis. Eur. J. Clin. Investig. 2022, 52, e13845. [Google Scholar] [CrossRef] [PubMed]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat. Med. 2022, 28, 2398–2405. [Google Scholar] [CrossRef]
- Mensah, A.A.; Lacy, J.; Stowe, J.; Seghezzo, G.; Sachdeva, R.; Simmons, R.; Bukasa, A.; O’Boyle, S.; Andrews, N.; Ramsay, M.; et al. Disease severity during SARS-COV-2 reinfection: A nationwide study. J. Infect. 2022, 84, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Medić, S.; Anastassopoulou, C.; Lozanov-Crvenković, Z.; Vuković, V.; Dragnić, N.; Petrović, V.; Ristić, M.; Pustahija, T.; Gojković, Z.; Tsakris, A.; et al. Risk and severity of SARS-CoV-2 reinfections during 2020-2022 in Vojvodina, Serbia: A population-level observational study. Lancet Reg. Health. Eur. 2022, 20, 100453. [Google Scholar] [CrossRef]
- Chunxiao, L.; Bo, W.; Jun, L.; Liming, L. Progress in research of etiology and epidemiology of 2019-nCoV Omicron variant. Chin. J. Epidemiol. 2022, 43, 1691–1698. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clin. Res. Ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Bertollini, R. Severity of SARS-CoV-2 Reinfections as Compared with Primary Infections. N. Engl. J. Med. 2021, 385, 2487–2489. [Google Scholar] [CrossRef]
- Alhaddad, F.; Abdulkareem, A.; Alsharrah, D.; Alkandari, A.; Bin-Hasan, S.; Al-Ahmad, M.; Al Hashemi, H.; Alghounaim, M. Incidence of SARS-CoV-2 reinfection in a paediatric cohort in Kuwait. BMJ Open 2022, 12, e056371. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, J.N.; Campbell, L.; Rabatsky-Her, T.; Leung, V.; Parikh, S. Repeat positive SARS-CoV-2 RNA testing in nursing home residents during the initial 9 months of the COVID-19 pandemic: An observational retrospective analysis. Lancet Reg. Health Am. 2021, 3, 100054. [Google Scholar] [CrossRef]
- Arslan, Y.; Akgul, F.; Sevim, B.; Varol, Z.S.; Tekin, S. Re-infection in COVID-19: Do we exaggerate our worries? Eur. J. Clin. Investig. 2022, 52, e13767. [Google Scholar] [CrossRef] [PubMed]
- Brouqui, P.; Colson, P.; Melenotte, C.; Houhamdi, L.; Bedotto, M.; Devaux, C.; Gautret, P.; Million, M.; Parola, P.; Stoupan, D.; et al. COVID-19 re-infection. Eur. J. Clin. Investig. 2021, 51, e13537. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Aguilar-Company, J.; Salazar, R.; Bower, M.; Sita-Lumsden, A.; Plaja, A.; Lee, A.J.X.; Bertuzzi, A.; Tondini, C.; Diamantis, N.; et al. Natural immunity to SARS-CoV-2 and breakthrough infections in vaccinated and unvaccinated patients with cancer. Br. J. Cancer 2022, 127, 1787–1792. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Acuti Martellucci, C.; Soldato, G.; Carota, R.; Fazii, P.; Caponetti, A.; Manzoli, L. Rate of reinfections after SARS-CoV-2 primary infection in the population of an Italian province: A cohort study. J. Public Health (Oxf. Engl.) 2022, 44, e475–e478. [Google Scholar] [CrossRef] [PubMed]
- Gazit, S.; Shlezinger, R.; Perez, G.; Lotan, R.; Peretz, A.; Ben-Tov, A.; Herzel, E.; Alapi, H.; Cohen, D.; Muhsen, K.; et al. The Incidence of SARS-CoV-2 Reinfection in Persons With Naturally Acquired Immunity With and Without Subsequent Receipt of a Single Dose of BNT162b2 Vaccine: A Retrospective Cohort Study. Ann. Intern. Med. 2022, 175, 674–681. [Google Scholar] [CrossRef]
- Kim, P.; Gordon, S.M.; Sheehan, M.M.; Rothberg, M.B. Duration of Severe Acute Respiratory Syndrome Coronavirus 2 Natural Immunity and Protection Against the Delta Variant: A Retrospective Cohort Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e185–e190. [Google Scholar] [CrossRef]
- Malhotra, S.; Mani, K.; Lodha, R.; Bakhshi, S.; Mathur, V.P.; Gupta, P.; Kedia, S.; Sankar, J.; Kumar, P.; Kumar, A.; et al. SARS-CoV-2 Reinfection Rate and Estimated Effectiveness of the Inactivated Whole Virion Vaccine BBV152 Against Reinfection Among Health Care Workers in New Delhi, India. JAMA Netw. Open 2022, 5, e2142210. [Google Scholar] [CrossRef] [PubMed]
- Mensah, A.A.; Campbell, H.; Stowe, J.; Seghezzo, G.; Simmons, R.; Lacy, J.; Bukasa, A.; O’Boyle, S.; Ramsay, M.E.; Brown, K.; et al. Risk of SARS-CoV-2 reinfections in children: A prospective national surveillance study between January, 2020, and July, 2021, in England. Lancet Child Adolesc. Health 2022, 6, 384–392. [Google Scholar] [CrossRef]
- Pilz, S.; Chakeri, A.; Ioannidis, J.P.; Richter, L.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Allerberger, F. SARS-CoV-2 re-infection risk in Austria. Eur. J. Clin. Investig. 2021, 51, e13520. [Google Scholar] [CrossRef]
- Sheehan, M.M.; Reddy, A.J.; Rothberg, M.B. Reinfection Rates Among Patients Who Previously Tested Positive for Coronavirus Disease 2019: A Retrospective Cohort Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, 1882–1886. [Google Scholar] [CrossRef] [PubMed]
- Spicer, K.B.; Glick, C.; Cavanaugh, A.M.; Thoroughman, D. Protective Immunity after Natural Infection with Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2)—Kentucky, USA, 2020. Int. J. Infect. Dis. 2022, 114, 21–28. [Google Scholar] [CrossRef]
- Ünsal, O.; Yazıcı, O.; Özdemir, N.; Çubukçu, E.; Ocak, B.; Üner, A.; Özet, A. Clinical and laboratory outcomes of the solid cancer patients reinfected with SARS-CoV-2. Future Oncol. (Lond. Engl. ) 2022, 18, 533–541. [Google Scholar] [CrossRef]
- Vitale, J.; Mumoli, N.; Clerici, P.; De Paschale, M.; Evangelista, I.; Cei, M.; Mazzone, A. Assessment of SARS-CoV-2 Reinfection 1 Year After Primary Infection in a Population in Lombardy, Italy. JAMA Intern. Med. 2021, 181, 1407–1408. [Google Scholar] [CrossRef]
- Yuguero, O.; Companys, M.; Guzmán, M.; Maciel, R.; Llobet, C.; López, A.; Olles, R.; Pujol, V.; Ruiz, M.J.; Saura, M.; et al. Epidemiological and clinical characteristics of SARS-CoV-2 reinfections in a Spanish region. SAGE Open Med. 2022, 10, 20503121221108556. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, R.A.; Qamar, M.A.; Gilani, J.A.; Irfan, O.; Waqar, U.; Sajid, M.I.; Mahmood, S.F. The mystery of COVID-19 reinfections: A global systematic review and meta-analysis. Ann. Med. Surg. 2021, 72, 103130. [Google Scholar] [CrossRef]
- Muralidar, S.; Ambi, S.V.; Sekaran, S.; Krishnan, U.M. The emergence of COVID-19 as a global pandemic: Understanding the epidemiology, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie 2020, 179, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zhu, K.; Liu, X.; Zhuang, C.; Huang, X.; Huang, Y.; Yao, X.; Quan, J.; Lin, H.; Huang, S.; et al. The Protection of Naturally Acquired Antibodies Against Subsequent SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis. Emerg. Microbes Infect. 2022, 11, 793–803. [Google Scholar] [CrossRef]
- Hammerman, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Peretz, A.; Netzer, D.; Yaron, S.; Arbel, R. Effectiveness of the BNT162b2 Vaccine after Recovery from COVID-19. N. Engl. J. Med. 2022, 386, 1221–1229. [Google Scholar] [CrossRef]
- Chivese, T.; Matizanadzo, J.T.; Musa, O.A.H.; Hindy, G.; Furuya-Kanamori, L.; Islam, N.; Al-Shebly, R.; Shalaby, R.; Habibullah, M.; Al-Marwani, T.A.; et al. The prevalence of adaptive immunity to COVID-19 and reinfection after recovery—A comprehensive systematic review and meta-analysis. Pathog. Glob. Health 2022, 116, 269–281. [Google Scholar] [CrossRef]
- Guedes, A.R.; Oliveira, M.S.; Tavares, B.M.; Luna-Muschi, A.; Lazari, C.D.S.; Montal, A.C.; de Faria, E.; Maia, F.L.; Barboza, A.D.S.; Leme, M.D.; et al. Reinfection rate in a cohort of healthcare workers over 2 years of the COVID-19 pandemic. Sci. Rep. 2023, 13, 712. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Hasan, M.R.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Al-Kanaani, Z.; Al-Kuwari, E.; et al. Protective Effect of Previous SARS-CoV-2 Infection against Omicron BA.4 and BA.5 Subvariants. N. Engl. J. Med. 2022, 387, 1620–1622. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Sharma, K.; Shaw, D.; Bhargava, A.; Negi, S.S. Mosaic Recombination Inflicted Various SARS-CoV-2 Lineages to Emerge into Novel Virus Variants: A Review Update. Indian J. Clin. Biochem. 2022. [Google Scholar] [CrossRef] [PubMed]
- GISAID. Genomic Epidemiology of SARS-CoV-2 with Subsampling Focused Globally over the Past 6 Months. Available online: https://gisaid.org/phylodynamics/global/nextstrain/ (accessed on 3 January 2023).
- Wong, C. Subvariant ‘soup’ may drive wave. New Sci. 2022, 256, 11. [Google Scholar] [CrossRef]
- World Health Organization. TAG-VE Statement on Omicron Sublineages BQ.1 and XBB. Available online: https://www.who.int/news/item/27-10-2022-tag-ve-statement-on-omicron-sublineages-bq.1-and-xbb (accessed on 3 January 2023).


{kind=link}
| Infection Status | Reinfection | Primary Infection | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Consequences | Data Source | Patients n/N | PP (%) | 95%CI (%) | p Value | I2 (%) | Data Source | Patients n/N | PP (%) | 95%CI (%) | p Value | I2 (%) |
| Severity of illness | ||||||||||||
| Asymptomatic infection | 2, 5, 7, 8, 10, 11, 15, 18 | 1326/4786 | 41.77 | 19.23–64.31 | <0.05 | 99.7 | 13, 18, 20 | 237,198/655,381 | 19.61 | −3.70–42.92 | >0.05 | 100 |
| Symptomatic infection | 2, 3, 4, 5, 10, 11, 12, 18 | 1519/4190 | 51.83 | 23.90–79.76 | <0.05 | 99.7 | 13 | 1638/1917 | 85.45 | 83.87–87.03 | <0.05 | – |
| Mild illness | 7, 9 | 13,687/13,821 | 65.65 | −1.12–132.41 | >0.05 | 98.4 | 12 | 237,243/251,104 | 94.48 | 94.39–94.57 | <0.05 | – |
| Severe illness | 7, 9, 14 | 116/15,125 | 0.58 | 0.031–1.14 | <0.05 | 83.3 | 12 | 13,735/251,104 | 5.47 | 5.38–5.56 | <0.05 | – |
| Critical illness | 9, 14 | 6/15,096 | 0.04 | 0.009–0.078 | <0.05 | - | 12 | 126/251,104 | 0.05 | 0.041–0.059 | <0.05 | – |
| Outcomes | ||||||||||||
| Hospitalization | 1, 2, 3, 4, 5, 6, 7, 8, 9, 12, 13, 16, 17, 18, 19 | 1764/29,692 | 15.48 | 11.98–18.97 | <0.05 | 99 | 12, 18, 21, 24 | 33,124/325,982 | 9.51 | 2.7116.31 | <0.05 | 99.9 |
| Admission to ICU | 2, 5, 15, 16, 19 | 30/2869 | 3.58 | 0.39–6.77 | <0.05 | 86.3 | 21, 24 | 1620/59,803 | 1.48 | −1.02–3.98 | >0.05 | 99.6 |
| Death | 1, 2, 4, 5, 6, 8, 9, 12, 14, 15, 16, 17 | 453/33,501 | 2.96 | 1.25–4.67 | <0.05 | 97.7 | 1, 13, 17, 20, 21, 22, 23 | 5999/800,417 | 8.58 | 6.78–10.38 | <0.05 | 99.9 |
| Need for mechanical ventilation | 5, 18 | 3/74 | 3.79 | −0.55–8.14 | >0.05 | 0 | - | - | - | - | - | - |
| Symptoms | Data Source | Patients n/N | PP (%) | 95%CI (%) | p Value | I2 (%) |
|---|---|---|---|---|---|---|
| Fever | 3, 7, 18 | 28/78 | 35.46 | 24.92–46.00 | <0.05 | 0 |
| Cough | 3, 7, 18 | 22/78 | 28.04 | 18.09–37.99 | <0.05 | 0 |
| Shortness of breath | 3, 7 | 16/60 | 25.4 | −5.52–56.33 | >0.05 | 88.9 |
| Fatigue | 3, 18 | 12/49 | 24.33 | 12.33–36.32 | <0.05 | 0 |
| Diarrhea | 3, 7 | 4/60 | 12.90 | 1.10–24.70 | <0.05 | - |
| Nausea/vomiting | 3, 18 | 6/49 | 12.19 | 3.03–21.35 | <0.05 | 0 |
| Myalgia | 3, 7 | 6/60 | 8.52 | −3.66–20.70 | >0.05 | 65.7 |
| Headache | 3, 7 | 6/60 | 8.52 | −3.66–20.70 | >0.05 | 65.7 |
| Sore throat | 3, 7 | 5/60 | 7.93 | 1.11–14.74 | <0.05 | 0 |
| Consequences | Data Source | Reinfection n/N | Primary Infection n/N | OR | 95%CI (%) | p Value | I2 (%) |
|---|---|---|---|---|---|---|---|
| Severity of illness | |||||||
| Asymptomatic infection | 10, 15 | 1060/4030 | 236,093/640,306 | 0.34 | 0.013–8.65 | >0.05 | 99.5 |
| Symptomatic infection | 14 | 94/1917 | 1638/1917 | 0.01 | 0.007–0.011 | <0.05 | - |
| Mild illness | 9 | 13,678/13,792 | 237,243/251,104 | 7.01 | 5.83–8.44 | <0.05 | - |
| Severe illness | 9 | 108/13,792 | 13,735/251,104 | 0.14 | 0.11–0.16 | <0.05 | - |
| Critical illness | 9 | 6/13,792 | 126/251,104 | 0.87 | 0.38–1.97 | >0.05 | - |
| Outcomes | |||||||
| Hospitalization | 9, 13, 16, 19 | 193/14,237 | 33,124/325,982 | 0.95 | 0.23–3.92 | >0.05 | 97.4 |
| Admission to ICU | 16, 19 | 21/440 | 1620/59,803 | 14.11 | 0.068–2909.82 | >0.05 | 97.5 |
| Death | 1, 12, 15, 16, 17 | 30/2971 | 5162/792,331 | 0.89 | 0.36–2.23 | >0.05 | 67.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, J.; Ma, Y.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 3335. https://doi.org/10.3390/ijerph20043335
Deng J, Ma Y, Liu Q, Du M, Liu M, Liu J. Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(4):3335. https://doi.org/10.3390/ijerph20043335
Chicago/Turabian StyleDeng, Jie, Yirui Ma, Qiao Liu, Min Du, Min Liu, and Jue Liu. 2023. "Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 4: 3335. https://doi.org/10.3390/ijerph20043335
APA StyleDeng, J., Ma, Y., Liu, Q., Du, M., Liu, M., & Liu, J. (2023). Severity and Outcomes of SARS-CoV-2 Reinfection Compared with Primary Infection: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 20(4), 3335. https://doi.org/10.3390/ijerph20043335