
Machine Learning Models to Predict the Risk of Rapidly Progressive Kidney Disease and the Need for Nephrology Referral in Adult Patients with Type 2 Diabetes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Data Extraction
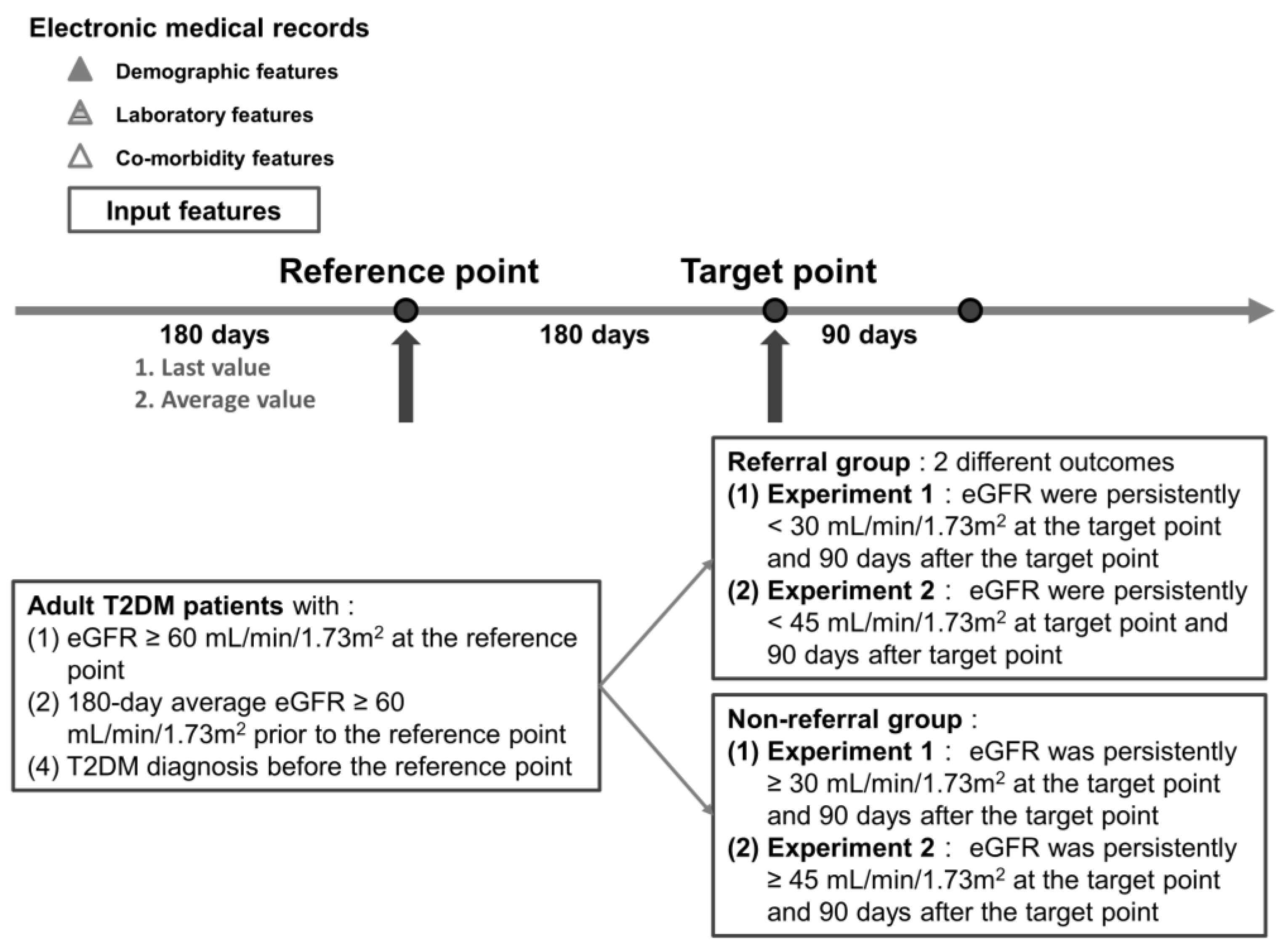
2.3. Study Design and Label Definition
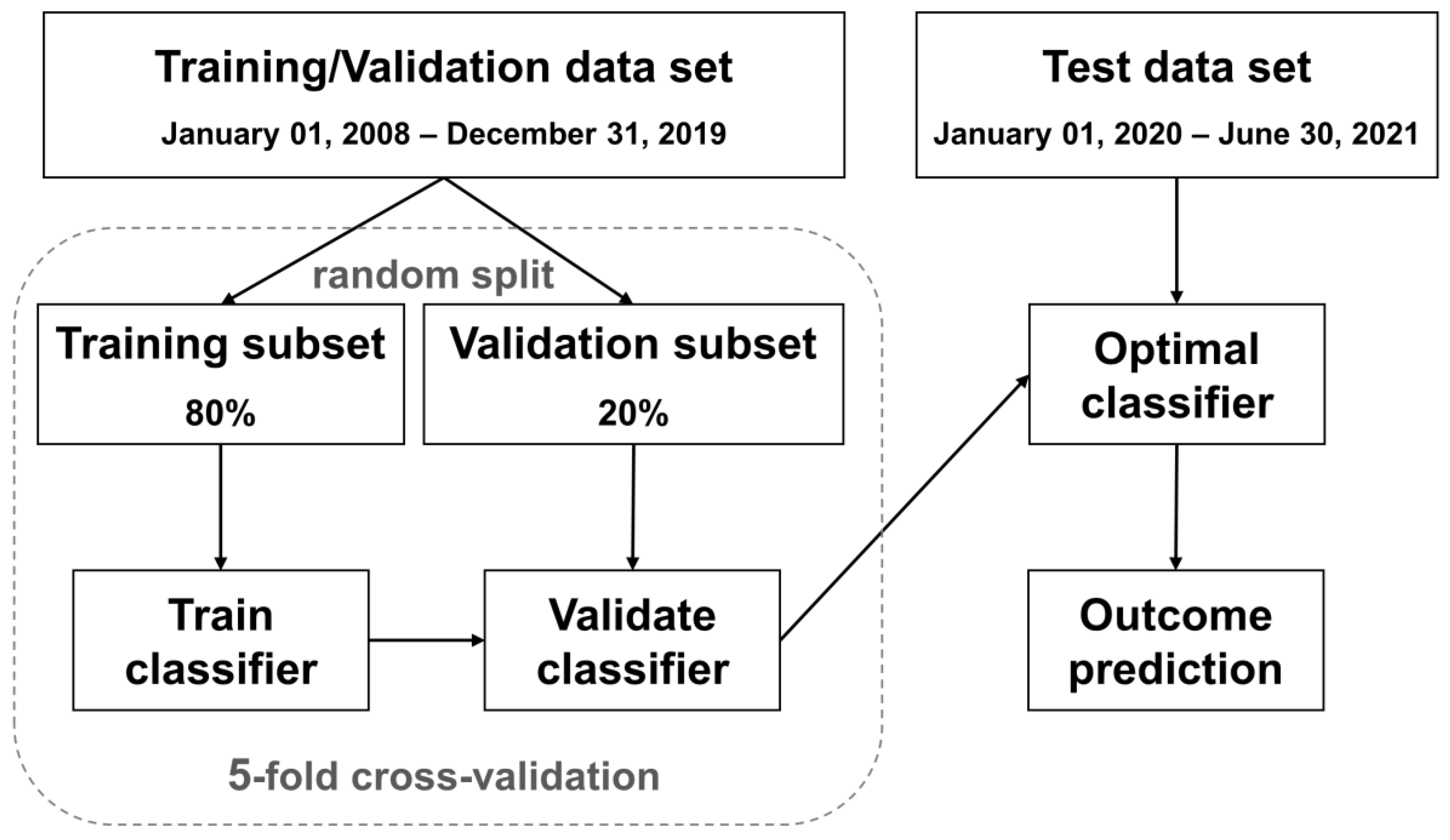
2.4. Data Preprocessing and Machine Learning Models
3. Results
3.1. Experiment 1: Predict Rapidly Progressive Kidney Disease and Nephrology Referral When the eGFR Was Persistently Lower than 30 mL/min/1.73 m2
3.2. Experiment 2: Predict Rapidly Progressive Kidney Disease and Nephrology Referral When the eGFR Was Persistently Lower than 45 mL/min/1.73 m2
3.3. Additional Experiment with Loose Inclusion and Labeling Criteria for Both Experiments 1 and 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | Data Sets | Accuracy | Referral Group (n = 1314) | Non-Referral Group (n = 10,328) | AUROC | ||
|---|---|---|---|---|---|---|---|
| Recall | Precision | Recall | Precision | ||||
| Original | Validation | 0.88 ± 0.01 | 0.80 ± 0.01 | 0.48 ± 0.02 | 0.89 ± 0.01 | 0.97 ± 0.00 | 0.92 ± 0.01 |
| Test | 0.88 ± 0.01 | 0.84 ± 0.01 | 0.53 ± 0.01 | 0.89 ± 0.00 | 0.97 ± 0.00 | 0.92 ± 0.00 | |
| Downsample | Validation | 0.86 ± 0.01 | 0.81 ± 0.02 | 0.43 ± 0.01 | 0.86 ± 0.01 | 0.97 ± 0.00 | 0.91 ± 0.01 |
| Test | 0.87 ± 0.01 | 0.82 ± 0.01 | 0.46 ± 0.01 | 0.88 ± 0.01 | 0.98 ± 0.00 | 0.90 ± 0.01 | |
| SMOTE | Validation | 0.92 ± 0.00 | 0.68 ± 0.01 | 0.62 ± 0.01 | 0.95 ± 0.00 | 0.96 ± 0.00 | 0.92 ± 0.01 |
| Test | 0.88 ± 0.01 | 0.74 ± 0.01 | 0.49 ± 0.02 | 0.90 ± 0.01 | 0.96 ± 0.00 | 0.87 ± 0.00 | |
| Tomek Links | Validation | 0.88 ± 0.00 | 0.81 ± 0.02 | 0.47 ± 0.01 | 0.88 ± 0.00 | 0.97 ± 0.00 | 0.92 ± 0.01 |
| Test | 0.86 ± 0.01 | 0.81 ± 0.01 | 0.43 ± 0.02 | 0.86 ± 0.01 | 0.97 ± 0.00 | 0.90 ± 0.00 | |
Appendix B
| Overall (n = 19,892) | Referral Group (n = 648) | Non-Referral Group (n = 19,244) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Number | Percentage | Number | Percentage | Number | Percentage | ||
| Age | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Sex | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Weight | 2310 | 11.61% | 37 | 5.71% | 2273 | 11.81% | <0.001 |
| Height | 3381 | 17.00% | 63 | 9.72% | 3318 | 17.24% | <0.001 |
| Hypertension | 0 | 0% | 0 | 0% | 0 | 0% | - |
| CAD | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Stroke | 0 | 0% | 0 | 0% | 0 | 0% | - |
| PAD | 0 | 0% | 0 | 0% | 0 | 0% | - |
| CHF | 0 | 0% | 0 | 0% | 0 | 0% | - |
| AKI | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Liver cirrhosis | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Cancer | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Bacteremia | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Shock | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Peritonitis | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Ascites | 0 | 0% | 0 | 0% | 0 | 0% | - |
| EV bleeding | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Creatinine | 0 | 0% | 0 | 0% | 0 | 0% | - |
| BUN | 3612 | 18.16% | 23 | 3.55% | 3589 | 18.65% | <0.001 |
| Fasting glucose | 6520 | 32.78% | 128 | 19.75% | 6392 | 33.22% | <0.001 |
| Random glucose | 5240 | 26.34% | 74 | 11.42% | 5166 | 26.84% | <0.001 |
| HbA1c | 4845 | 24.36% | 83 | 12.81% | 4762 | 24.75% | <0.001 |
| HGB | 9557 | 48.04% | 348 | 53.70% | 9209 | 47.85% | 0.003 |
| HCT | 8704 | 43.76% | 205 | 31.64% | 8499 | 44.16% | <0.001 |
| Albumin | 11,362 | 57.12% | 204 | 31.48% | 11,158 | 57.98% | <0.001 |
| AST | 4667 | 23.46% | 118 | 18.21% | 4549 | 23.64% | 0.001 |
| ALT | 1866 | 9.38% | 96 | 14.81% | 1770 | 9.20% | <0.001 |
| CPK | 12,846 | 64.58% | 261 | 40.28% | 12,585 | 65.40% | <0.001 |
| hsCRP | 10,935 | 54.97% | 251 | 38.73% | 10,684 | 55.52% | <0.001 |
| K | 2886 | 14.51% | 7 | 1.08% | 2879 | 14.96% | <0.001 |
| RBC | 7353 | 36.96% | 168 | 25.93% | 7185 | 37.34% | <0.001 |
| WBC | 1764 | 8.87% | 35 | 5.40% | 1729 | 8.98% | 0.002 |
| Bil-T | 8844 | 44.46% | 286 | 44.14% | 8558 | 44.47% | 0.866 |
| Uric acid | 12,835 | 64.52% | 289 | 44.60% | 12,546 | 65.19% | <0.001 |
| CHO | 7093 | 35.66% | 165 | 25.46% | 6928 | 36.00% | <0.001 |
| LDL | 7233 | 36.36% | 129 | 19.91% | 7104 | 36.92% | <0.001 |
| TG | 6863 | 34.50% | 159 | 24.54% | 6704 | 34.84% | <0.001 |
| UPCR | 16,736 | 84.13% | 295 | 45.52% | 16,441 | 85.43% | <0.001 |
| UACR | 11,665 | 58.64% | 258 | 39.81% | 11,407 | 59.28% | <0.001 |
| Overall (n = 16,145) | Referral Group (n = 986) | Non-Referral Group (n = 15,159) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Number | Percentage | Number | Percentage | Number | Percentage | ||
| Age | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Sex | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Weight | 1898 | 11.76% | 73 | 7.40% | 1825 | 12.04% | <0.001 |
| Height | 2694 | 16.69% | 123 | 12.47% | 2571 | 16.96% | <0.001 |
| Hypertension | 0 | 0% | 0 | 0% | 0 | 0% | - |
| CAD | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Stroke | 0 | 0% | 0 | 0% | 0 | 0% | - |
| PAD | 0 | 0% | 0 | 0% | 0 | 0% | - |
| CHF | 0 | 0% | 0 | 0% | 0 | 0% | - |
| AKI | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Liver cirrhosis | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Cancer | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Bacteremia | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Shock | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Peritonitis | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Ascites | 0 | 0% | 0 | 0% | 0 | 0% | - |
| EV bleeding | 0 | 0% | 0 | 0% | 0 | 0% | - |
| Creatinine | 0 | 0% | 0 | 0% | 0 | 0% | - |
| BUN | 3312 | 20.51% | 92 | 9.33% | 3220 | 21.24% | <0.001 |
| Fasting glucose | 5103 | 31.61% | 225 | 22.82% | 4878 | 32.18% | <0.001 |
| Random glucose | 4408 | 27.30% | 129 | 13.08% | 4279 | 28.23% | <0.001 |
| HbA1c | 3781 | 23.42% | 135 | 13.69% | 3646 | 24.05% | <0.001 |
| HGB | 7723 | 47.84% | 554 | 56.19% | 7169 | 47.29% | <0.001 |
| HCT | 7207 | 44.64% | 369 | 37.42% | 6838 | 45.11% | <0.001 |
| Albumin | 9668 | 59.88% | 421 | 42.70% | 9247 | 61.00% | <0.001 |
| AST | 3879 | 24.03% | 199 | 20.18% | 3680 | 24.28% | 0.004 |
| ALT | 1330 | 8.24% | 127 | 12.88% | 1203 | 7.94% | <0.001 |
| CPK | 10,836 | 67.12% | 466 | 47.26% | 10,370 | 68.41% | <0.001 |
| hsCRP | 9211 | 57.05% | 424 | 43.00% | 8787 | 57.97% | <0.001 |
| K | 2663 | 16.49% | 48 | 4.87% | 2615 | 17.25% | <0.001 |
| RBC | 6195 | 38.37% | 297 | 30.12% | 5898 | 38.91% | <0.001 |
| WBC | 1545 | 9.57% | 65 | 6.59% | 1480 | 9.76% | 0.001 |
| Bil-T | 7282 | 45.10% | 404 | 40.97% | 6878 | 45.37% | 0.007 |
| Uric acid | 10,478 | 64.90% | 533 | 54.06% | 9945 | 65.60% | <0.001 |
| CHO | 5465 | 33.85% | 248 | 25.15% | 5217 | 34.42% | <0.001 |
| LDL | 5734 | 35.52% | 188 | 19.07% | 5546 | 36.59% | <0.001 |
| TG | 5309 | 32.88% | 250 | 25.35% | 5059 | 33.37% | <0.001 |
| UPCR | 14,034 | 86.92% | 509 | 51.62% | 13,525 | 89.22% | <0.001 |
| UACR | 9340 | 57.85% | 419 | 42.49% | 8921 | 58.85% | <0.001 |
References
- Kianmehr, H.; Zhang, P.; Luo, J.; Guo, J.; Pavkov, M.E.; Bullard, K.M.; Gregg, E.W.; Ospina, N.S.; Fonseca, V.; Shi, L.; et al. Potential Gains in Life Expectancy Associated With Achieving Treatment Goals in US Adults With Type 2 Diabetes. JAMA Netw. Open 2022, 5, e227705. [Google Scholar] [CrossRef]
- Loukine, L.; Waters, C.; Choi, B.C.; Ellison, J. Impact of diabetes mellitus on life expectancy and health-adjusted life expectancy in Canada. Popul. Health Metr. 2012, 10, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao Kondapally Seshasai, S.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [PubMed] [Green Version]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; De Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. 2013, 24, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregg, E.W.; Li, Y.; Wang, J.; Rios Burrows, N.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in diabetes-related complications in the United States, 1990–2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Castelao, A.; Soler, M.J.; Górriz Teruel, J.L.; Navarro-González, J.F.; Fernandez-Fernandez, B.; de Alvaro Moreno, F.; Ortiz, A. Optimizing the timing of nephrology referral for patients with diabetic kidney disease. Clin. Kidney J. 2021, 14, 5–8. [Google Scholar] [CrossRef]
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022. [Google Scholar]
- Lai, T.-S.; Hsu, C.-C.; Lin, M.-H.; Wu, V.-C.; Chen, Y.-M. Trends in the incidence and prevalence of end-stage kidney disease requiring dialysis in Taiwan: 2010–2018. J. Formos. Med. Assoc. 2022, 121, S5–S11. [Google Scholar] [CrossRef]
- Smart, N.A.; Dieberg, G.; Ladhani, M.; Titus, T. Early referral to specialist nephrology services for preventing the progression to end-stage kidney disease. Cochrane Database Syst. Rev. 2014, 6, CD007333. [Google Scholar] [CrossRef]
- Porrini, E.; Ruggenenti, P.; Mogensen, C.E.; Barlovic, D.P.; Praga, M.; Cruzado, J.M.; Hojs, R.; Abbate, M.; de Vries, A.P.; on behalf of the ERA-EDTA diabesity working group. Non-proteinuric pathways in loss of renal function in patients with type 2 diabetes. Lancet Diabetes Endocrinol. 2015, 3, 382–391. [Google Scholar] [CrossRef]
- Kritmetapak, K.; Anutrakulchai, S.; Pongchaiyakul, C.; Puapairoj, A. Clinical and pathological characteristics of non-diabetic renal disease in type 2 diabetes patients. Clin. Kidney J. 2018, 11, 342–347. [Google Scholar] [CrossRef]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Q.; Zhang, H.; Deng, T.; Tang, S.; Yuan, X.; Tang, W.; Xie, Y.; Ge, H.; Wang, X.; Zhou, Q. Role of artificial intelligence in kidney disease. Int. J. Med. Sci. 2020, 17, 970–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belur Nagaraj, S.; Pena, M.J.; Ju, W.; Heerspink, H.L.; Consortium, B.D. Machine-learning-based early prediction of end-stage renal disease in patients with diabetic kidney disease using clinical trials data. Diabetes Obes. Metab. 2020, 22, 2479–2486. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Wang, Q.; Ke, Y.; Zhang, W.; Hong, Q.; Liu, C.; Liu, X.; Yang, J.; Xi, Y.; Shi, J. Prediction of 3-year risk of diabetic kidney disease using machine learning based on electronic medical records. J. Transl. Med. 2022, 20, 143. [Google Scholar] [CrossRef]
- Huang, G.-M.; Huang, K.-Y.; Lee, T.-Y.; Weng, J.T.-Y. An interpretable rule-based diagnostic classification of diabetic nephropathy among type 2 diabetes patients. BMC Bioinform. 2015, 16, S5. [Google Scholar] [CrossRef] [Green Version]
- Makino, M.; Yoshimoto, R.; Ono, M.; Itoko, T.; Katsuki, T.; Koseki, A.; Kudo, M.; Haida, K.; Kuroda, J.; Yanagiya, R. Artificial intelligence predicts the progression of diabetic kidney disease using big data machine learning. Sci. Rep. 2019, 9, 11862. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Romero, V.; Bergstrom, R.F.; Decker, B.S.; Lahu, G.; Vakilynejad, M.; Bies, R.R. Prediction of nephropathy in type 2 diabetes: An analysis of the ACCORD trial applying machine learning techniques. Clin. Transl. Sci. 2019, 12, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Association, A.D. 11. Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes-2021. Diabetes Care 2020, 44, S151–S167. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Pinier, C.; Gatault, P.; Francois, M.; Barbet, C.; Longuet, H.; Rabot, N.; Noble, J.; Bailly, E.; Buchler, M.; Sautenet, B. Renal function at the time of nephrology referral but not dialysis initiation as a risk for death in patients with diabetes mellitus. Clin. Kidney J. 2018, 11, 762–768. [Google Scholar] [CrossRef]
- Emmanuel, T.; Maupong, T.; Mpoeleng, D.; Semong, T.; Mphago, B.; Tabona, O. A survey on missing data in machine learning. J. Big Data 2021, 8, 140. [Google Scholar] [CrossRef] [PubMed]
- Soley-Bori, M. Dealing with missing data: Key assumptions and methods for applied analysis. Boston Univ. 2013, 4, 1–19. [Google Scholar]
- Chauhan, N.K.; Singh, K. Performance assessment of machine learning classifiers using selective feature approaches for cervical cancer detection. Wirel. Pers. Commun. 2022, 124, 2335–2366. [Google Scholar] [CrossRef]
- Kumari, V.A.; Chitra, R. Classification of diabetes disease using support vector machine. Int. J. Eng. Res. Appl. 2013, 3, 1797–1801. [Google Scholar]
- Neamțu, B.M.; Visa, G.; Maniu, I.; Ognean, M.L.; Pérez-Elvira, R.; Dragomir, A.; Agudo, M.; Șofariu, C.R.; Gheonea, M.; Pitic, A. A decision-tree approach to assist in forecasting the outcomes of the neonatal brain injury. Int. J. Environ. Res. Public Health 2021, 18, 4807. [Google Scholar] [CrossRef]
- Prusty, S.; Patnaik, S.; Dash, S.K. SKCV: Stratified K-fold cross-validation on ML classifiers for predicting cervical cancer. Front. Nanotechnol. 2022, 4, 972421. [Google Scholar] [CrossRef]
- Yang, T.; Zhang, L.; Yi, L.; Feng, H.; Li, S.; Chen, H.; Zhu, J.; Zhao, J.; Zeng, Y.; Liu, H. Ensemble Learning Models Based on Noninvasive Features for Type 2 Diabetes Screening: Model Development and Validation. JMIR Med. Inform. 2020, 8, e15431. [Google Scholar] [CrossRef]
- de Oliveira, G.P.; Fonseca, A.; Rodrigues, P.C. Diabetes diagnosis based on hard and soft voting classifiers combining statistical learning models. Braz. J. Biom. 2022, 40, 415–427. [Google Scholar] [CrossRef]
- Kumari, S.; Kumar, D.; Mittal, M. An ensemble approach for classification and prediction of diabetes mellitus using soft voting classifier. Int. J. Cogn. Comput. Eng. 2021, 2, 40–46. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Lundberg, S.M.; Erion, G.G.; Lee, S.-I. Consistent individualized feature attribution for tree ensembles. arXiv 2018, arXiv:1802.03888. [Google Scholar]
- Tseng, P.-Y.; Chen, Y.-T.; Wang, C.-H.; Chiu, K.-M.; Peng, Y.-S.; Hsu, S.-P.; Chen, K.-L.; Yang, C.-Y.; Lee, O.K.-S. Prediction of the development of acute kidney injury following cardiac surgery by machine learning. Crit. Care 2020, 24, 478. [Google Scholar] [CrossRef] [PubMed]
- Tomek, I. Two Modifications of CNN. IEEE Trans. Syst. Man Cybern 1976, SMC-6, 769–772. [Google Scholar]
- Barros, T.M.; Souza Neto, P.A.; Silva, I.; Guedes, L.A. Predictive models for imbalanced data: A school dropout perspective. Educ. Sci. 2019, 9, 275. [Google Scholar] [CrossRef]
- He, H.; Garcia, E.A. Learning from Imbalanced Data. IEEE Trans. Knowl. Data Eng. 2009, 21, 1263–1284. [Google Scholar]






| Overall (n = 19,892) | Referral Group (n = 648) | Non-Referral Group (n = 19,244) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Age (years) | 64.21 | (55.85–72.55) | 68.75 | (59.92–76.80) | 64.04 | (55.70–72.30) | <0.001 |
| Male sex | 11,765 | (59.14%) | 391 | (60.34%) | 11,374 | (59.10%) | 0.529 |
| Weight (kg) | 66.50 | (58.0–76.0) | 66.0 | (59.0–75.0) | 66.5 | (58.0–76.0) | 0.904 |
| Height (cm) | 162.0 | (155.5–168.0) | 161.50 | (155.9–168.0) | 162.00 | (155.5–168.0) | 0.188 |
| Hypertension | 10,273 | (51.64%) | 464 | (71.60%) | 9809 | (50.97%) | <0.001 |
| CAD | 3196 | (16.07%) | 139 | (21.45%) | 3057 | (15.89%) | <0.001 |
| Stroke | 2962 | (14.89%) | 133 | (20.52%) | 2829 | (14.70%) | <0.001 |
| PAD | 351 | (1.76%) | 36 | (5.56%) | 315 | (1.64%) | <0.001 |
| CHF | 1147 | (5.77%) | 94 | (14.51%) | 1053 | (5.47%) | <0.001 |
| AKI | 454 | (2.28%) | 103 | (15.9%) | 351 | (1.82%) | <0.001 |
| Liver cirrhosis | 966 | (4.86%) | 42 | (6.48%) | 924 | (4.80%) | 0.050 |
| Cancer | 5480 | (27.55%) | 138 | (21.30%) | 5342 | (27.76%) | <0.001 |
| Bacteremia | 644 | (3.24%) | 39 | (6.02%) | 605 | (3.14%) | <0.001 |
| Shock | 289 | (1.45%) | 15 | (2.31%) | 274 | (1.42%) | 0.060 |
| Peritonitis | 282 | (1.42%) | 8 | (1.23%) | 274 | (1.42%) | 0.689 |
| Ascites | 167 | (0.84%) | 10 | (1.54%) | 157 | (0.82%) | 0.046 |
| EV bleeding | 44 | (0.22%) | 1 | (0.15%) | 43 | (0.22%) | 0.713 |
| Creatinine (mg/dl) | 0.89 | (0.72–1.10) | 1.75 | (1.48–2.05) | 0.88 | (0.71–1.07) | <0.001 |
| BUN (mg/dl) | 16.0 | (13.0–21.0) | 28.0 | (22.0–35.0) | 16.0 | (12.5–20.0) | <0.001 |
| Fasting glucose (mg/dl) | 123.0 | (105.0–147.0) | 123.0 | (103.0–161.0) | 123.0 | (105.0–146.0) | <0.001 |
| Random glucose (mg/dl) | 136.0 | (111.0–180.0) | 143.0 | (113.0–197.0) | 135.5 | (111.0–180.0) | 0.019 |
| HbA1c (%) | 6.8 | (6.2–7.7) | 7.1 | (6.3–8.0) | 6.8 | (6.2–6.7) | <0.001 |
| HGB (g/dL) | 13.3 | (11.8–14.6) | 11.4 | (10.0–12.8) | 13.4 | (11.9–14.7) | <0.001 |
| HCT (%) | 39.29 | (34.80–43.00) | 34.50 | (30.33–38.50) | 39.45 | (35.10–43.10) | <0.001 |
| Albumin (g/dL) | 4.10 | (3.60–4.40) | 3.80 | (3.40–4.10) | 4.10 | (3.60–4.40) | <0.001 |
| AST (U/L) | 25.0 | (19.0–36.0) | 23.3 | (17.0–33.0) | 25.0 | (19.0–36.0) | <0.001 |
| ALT (U/L) | 24.0 | (17.0–37.0) | 20.0 | (13.0–28.0) | 24.0 | (17.0–37.0) | <0.001 |
| CPK (U/L) | 87.0 | (54.0–144.0) | 88.0 | (54.3–165.8) | 87.0 | (53.6–143.0) | 0.1415 |
| hsCRP (mg/dl) | 0.66 | (0.15–3.80) | 1.29 | (0.23–4.69) | 0.64 | (0.15–3.77) | <0.001 |
| K (mEq/L) | 4.10 | (3.80–4.40) | 4.30 | (3.90–4.61) | 4.10 | (3.80–4.40) | <0.001 |
| RBC (×106/μL) | 4.32 | (3.83–4.78) | 3.81 | (3.28–4.32) | 4.33 | (3.85–4.79) | <0.001 |
| WBC (/μL) | 7320 | (5808–9350) | 7310 | (5800–9350) | 7510 | (6015–9376) | 0.282 |
| Bil-T (mg/dl) | 0.60 | (0.40–0.80) | 0.50 | (0.30–0.70) | 0.60 | (0.40–0.80) | <0.001 |
| Uric acid (mg/dl) | 5.9 | (4.9–7.9) | 6.8 | (5.4–8.2) | 5.9 | (4.9–7.0) | <0.001 |
| CHO (mg/dl) | 163.0 | (140.0–190.9) | 160.0 | (130.0–191.8) | 163.0 | (140.0–190.0) | 0.568 |
| LDL (mg/dl) | 93.0 | (74.0–117.0) | 93.0 | (74.0–115.0) | 93.0 | (74.0–117.0) | 0.9311 |
| TG (mg/dl) | 122.0 | (86.0–174.0) | 139.0 | (98.5–201.3) | 121.0 | (86.0–173.0) | <0.001 |
| UPCR (mg/g) | 140.0 | (79.5–380.0) | 1180.0 | (317.5–3318.0) | 120.0 | (71.0–270.0) | <0.001 |
| UACR (mg/g) | 16.1 | (6.9–61.8) | 696.9 | (118.5–2106.0) | 14.9 | (6.7–51.3) | <0.001 |
| Models | Data Sets | Accuracy | Referral Group (n = 648) | Non-Referral Group (n = 19,244) | AUROC | ||
|---|---|---|---|---|---|---|---|
| Recall | Precision | Recall | Precision | ||||
| XGB | Validation | 0.96 ± 0.01 | 0.87 ± 0.04 | 0.42 ± 0.02 | 0.96 ± 0.00 | 1.00 ± 0.00 | 0.97 ± 0.01 |
| Test | 0.95 ± 0.00 | 0.80 ± 0.02 | 0.37 ± 0.01 | 0.95 ± 0.00 | 0.99 ± 0.00 | 0.96 ± 0.00 | |
| LR | Validation | 0.94 ± 0.00 | 0.91 ± 0.03 | 0.34 ± 0.02 | 0.94 ± 0.01 | 1.00 ± 0.00 | 0.97 ± 0.01 |
| Test | 0.93 ± 0.00 | 0.87 ± 0.01 | 0.30 ± 0.01 | 0.93 ± 0.00 | 1.00 ± 0.00 | 0.97 ± 0.00 | |
| RF | Validation | 0.91 ± 0.01 | 0.91 ± 0.02 | 0.26 ± 0.02 | 0.91 ± 0.01 | 1.00 ± 0.00 | 0.97 ± 0.01 |
| Test | 0.91 ± 0.00 | 0.91 ± 0.01 | 0.26 ± 0.00 | 0.91 ± 0.00 | 1.00 ± 0.00 | 0.96 ± 0.00 | |
| Voting | Validation | 0.95 ± 0.00 | 0.91 ± 0.03 | 0.37 ± 0.02 | 0.95 ± 0.00 | 1.00 ± 0.00 | 0.98 ± 0.01 |
| Test | 0.94 ± 0.00 | 0.86 ± 0.01 | 0.33 ± 0.01 | 0.94 ± 0.00 | 1.00 ± 0.00 | 0.97 ± 0.00 | |
| Overall (n = 16,145) | Referral Group (n = 986) | Non-Referral Group (n = 15,159) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Age (years) | 63.88 | (55.62–72.05) | 69.84 | (61.79–78.05) | 62.46 | (54.37–70.13) | <0.001 |
| Male sex | 9425 | (58.38%) | 563 | (57.10%) | 8862 | (58.46%) | 0.401 |
| Weight (kg) | 66.3 | (58.0–75.9) | 64.5 | (57.0–73.1) | 67.0 | (58.3–76.5) | <0.001 |
| Height (cm) | 162.0 | (155.5–168.0) | 161.0 | (154.0–166.7) | 162.1 | (156.0–168.5) | <0.001 |
| Hypertension | 8066 | (49.96%) | 662 | (67.14%) | 7404 | (48.84%) | <0.001 |
| CAD | 2565 | (15.89%) | 207 | (20.99%) | 2358 | (15.56%) | <0.001 |
| Stroke | 2256 | (13.97%) | 202 | (20.49%) | 2054 | (13.55%) | <0.001 |
| PAD | 248 | (1.54%) | 32 | (3.25%) | 216 | (1.42%) | <0.001 |
| CHF | 786 | (4.87%) | 132 | (13.39%) | 654 | (4.31%) | <0.001 |
| AKI | 165 | (1.02%) | 79 | (8.01%) | 86 | (0.57%) | <0.001 |
| Liver cirrhosis | 748 | (4.63%) | 62 | (6.29%) | 686 | (4.53%) | 0.011 |
| Cancer | 4345 | (26.91%) | 279 | (28.30%) | 4066 | (26.82%) | 0.312 |
| Bacteremia | 426 | (2.64%) | 52 | (5.27%) | 374 | (2.47%) | <0.001 |
| Shock | 179 | (1.11%) | 23 | (2.33%) | 156 | (1.03%) | <0.001 |
| Peritonitis | 211 | (1.31%) | 22 | (2.23%) | 189 | (1.25%) | 0.008 |
| Ascites | 114 | (0.71%) | 17 | (1.72%) | 97 | (0.64%) | <0.001 |
| EV bleeding | 37 | (0.23%) | 4 | (0.41%) | 33 | (0.22%) | 0.232 |
| Creatinine (mg/dl) | 0.88 | (0.71–1.07) | 1.14 | (0.94–1.38) | 0.83 | (0.70–0.99) | <0.001 |
| BUN (mg/dl) | 16.0 | (12.3–20.0) | 19.5 | (15.0–25.0) | 15.0 | (12.0–18.5) | <0.001 |
| Fasting glucose (mg/dl) | 123.0 | (106.0–147.0) | 124.0 | (104.6–153.0) | 123.0 | (106.0–146.0) | 0.277 |
| Random glucose (mg/dl) | 136.0 | (111.0–180.6) | 142.0 | (112.0–192.0) | 134.0 | (111.0–177.0) | <0.001 |
| HbA1c (%) | 6.8 | (6.2–7.7) | 6.9 | (6.2–7.8) | 6.8 | (6.3–7.7) | 0.632 |
| HGB (g/dL) | 13.4 | (11.9–14.6) | 12.1 | (10.7–13.5) | 13.6 | (12.2–14.8) | <0.001 |
| HCT (%) | 39.20 | (34.70–42.90) | 35.90 | (31.60–40.00) | 40.00 | (35.90–43.45) | <0.001 |
| Albumin (g/dL) | 4.10 | (3.55–4.40) | 3.90 | (3.37–4.20) | 4.10 | (3.65–4.40) | <0.001 |
| AST (U/L) | 25.0 | (19.0–37.0) | 25.0 | (19.0–39.0) | 25.0 | (19.0–36.0) | 0.017 |
| ALT (U/L) | 24.0 | (17.0–37.0) | 21.0 | (15.0–34.0) | 25.0 | (17.0–38.0) | <0.001 |
| CPK (U/L) | 86.0 | (52.0–141.0) | 79.7 | (47.0–138.0) | 89.0 | (55.0–142.0) | <0.001 |
| hsCRP (mg/dl) | 0.65 | (0.15–3.74) | 1.28 | (0.26–5.46) | 0.51 | (0.12–3.16) | <0.001 |
| K (mEq/L) | 4.10 | (3.80–4.40) | 4.20 | (3.81–4.50) | 4.10 | (3.80–4.40) | <0.001 |
| RBC (×106/μL) | 4.31 | (3.82–4.77) | 3.94 | (3.46–4.44) | 4.41 | (3.96–4.84) | <0.001 |
| WBC (/μL) | 7250 | (5760–9260) | 7300 | (5700–9307) | 7240 | (5780–9250) | 0.797 |
| Bil-T (mg/dl) | 0.60 | (0.40–0.80) | 0.54 | (0.40–0.80) | 0.60 | (0.40–0.80) | <0.001 |
| Uric acid (mg/dl) | 5.9 | (4.9–7.1) | 6.4 | (5.2–7.6) | 5.8 | (4.8–6.9) | <0.001 |
| CHO (mg/dl) | 163.0 | (140.0–190.0) | 157.0 | (133.0–185.0) | 165.0 | (142.0–192.0) | <0.001 |
| LDL (mg/dl) | 93.0 | (74.0–116.0) | 90.0 | (70.0–113.0) | 94.0 | (75.0–117.0) | <0.001 |
| TG (mg/dl) | 121.0 | (86.0–174.0) | 124.0 | (88.0–179.0) | 120.0 | (85.0–172.0) | 0.003 |
| UPCR (mg/g) | 141.0 | (80.0–370.0) | 200.0 | (98.8–572.3) | 115.0 | (70.0–240.0) | <0.001 |
| UACR (mg/g) | 15.9 | (6.8–60.5) | 57.7 | (14.7–334.5) | 12.6 | (6.2–38.1) | <0.001 |
| Models | Data Sets | Accuracy | Referral Group (n = 986) | Non-Referral Group (n = 15,159) | AUROC | ||
|---|---|---|---|---|---|---|---|
| Recall | Precision | Recall | Precision | ||||
| XGB | Validation | 0.93 ± 0.01 | 0.84 ± 0.03 | 0.44 ± 0.02 | 0.93 ± 0.01 | 0.99 ± 0.00 | 0.95 ± 0.01 |
| Test | 0.92 ± 0.00 | 0.84 ± 0.01 | 0.42 ± 0.01 | 0.93 ± 0.00 | 0.99 ± 0.00 | 0.93 ± 0.01 | |
| LR | Validation | 0.90 ± 0.01 | 0.88 ± 0.04 | 0.37 ± 0.02 | 0.90 ± 0.01 | 0.99 ± 0.00 | 0.95 ± 0.01 |
| Test | 0.90 ± 0.00 | 0.87 ± 0.03 | 0.35 ± 0.01 | 0.90 ± 0.00 | 0.99 ± 0.00 | 0.94 ± 0.01 | |
| RF | Validation | 0.89 ± 0.01 | 0.89 ± 0.03 | 0.33 ± 0.01 | 0.89 ± 0.00 | 0.99 ± 0.00 | 0.95 ± 0.01 |
| Test | 0.88 ± 0.00 | 0.86 ± 0.03 | 0.32 ± 0.01 | 0.88 ± 0.00 | 0.99 ± 0.00 | 0.93 ± 0.00 | |
| Voting | Validation | 0.91 ± 0.00 | 0.88 ± 0.02 | 0.40 ± 0.01 | 0.91 ± 0.01 | 0.99 ± 0.00 | 0.95 ± 0.01 |
| Test | 0.91 ± 0.00 | 0.87 ± 0.02 | 0.39 ± 0.01 | 0.91 ± 0.00 | 0.99 ± 0.00 | 0.94 ± 0.00 | |
| Loose Inclusion and Labeling Criteria Compared with Experiment 1 | |||||||
|---|---|---|---|---|---|---|---|
| Models | Data Sets | Accuracy | Referral Group (n = 2541) | Non-Referral Group (n = 19,244) | AUROC | ||
| Recall | Precision | Recall | Precision | ||||
| XGB | Validation | 0.87 ± 0.00 | 0.78 ± 0.02 | 0.46 ± 0.01 | 0.88 ± 0.01 | 0.97 ± 0.00 | 0.92 ± 0.00 |
| Test | 0.87 ± 0.00 | 0.80 ± 0.01 | 0.47 ± 0.00 | 0.88 ± 0.00 | 0.97 ± 0.00 | 0.92 ± 0.00 | |
| LR | Validation | 0.85 ± 0.01 | 0.81 ± 0.01 | 0.42 ± 0.01 | 0.85 ± 0.01 | 0.97 ± 0.00 | 0.91 ± 0.01 |
| Test | 0.84 ± 0.00 | 0.80 ± 0.01 | 0.41 ± 0.00 | 0.85 ± 0.00 | 0.97 ± 0.00 | 0.90 ± 0.00 | |
| RF | Validation | 0.83 ± 0.00 | 0.83 ± 0.03 | 0.40 ± 0.01 | 0.83 ± 0.01 | 0.97 ± 0.00 | 0.92 ± 0.01 |
| Test | 0.84 ± 0.00 | 0.84 ± 0.01 | 0.41 ± 0.01 | 0.84 ± 0.00 | 0.98 ± 0.00 | 0.92 ± 0.00 | |
| Loose Inclusion and Labeling Criteria Compared with Experiment 2 | |||||||
| Models | Data Sets | Accuracy | Referral Group (n = 3836) | Non-Referral Group (n = 15,159) | AUROC | ||
| Recall | Precision | Recall | Precision | ||||
| XGB | Validation | 0.84 ± 0.01 | 0.81 ± 0.01 | 0.58 ± 0.01 | 0.85 ± 0.00 | 0.95 ± 0.00 | 0.91 ± 0.00 |
| Test | 0.84 ± 0.00 | 0.79 ± 0.00 | 0.57 ± 0.01 | 0.85 ± 0.00 | 0.94 ± 0.00 | 0.90 ± 0.00 | |
| LR | Validation | 0.83 ± 0.00 | 0.81 ± 0.01 | 0.55 ± 0.01 | 0.83 ± 0.00 | 0.95 ± 0.00 | 0.90 ± 0.01 |
| Test | 0.83 ± 0.00 | 0.82 ± 0.00 | 0.55 ± 0.00 | 0.83 ± 0.00 | 0.95 ± 0.00 | 0.89 ± 0.00 | |
| RF | Validation | 0.82 ± 0.01 | 0.83 ± 0.01 | 0.53 ± 0.01 | 0.81 ± 0.01 | 0.95 ± 0.00 | 0.90 ± 0.01 |
| Test | 0.82 ± 0.00 | 0.81 ± 0.01 | 0.54 ± 0.01 | 0.83 ± 0.00 | 0.95 ± 0.00 | 0.89 ± 0.00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-T.; Pai, K.-C.; Chen, L.-C.; Lin, S.-H.; Wu, M.-J. Machine Learning Models to Predict the Risk of Rapidly Progressive Kidney Disease and the Need for Nephrology Referral in Adult Patients with Type 2 Diabetes. Int. J. Environ. Res. Public Health 2023, 20, 3396. https://doi.org/10.3390/ijerph20043396
Hsu C-T, Pai K-C, Chen L-C, Lin S-H, Wu M-J. Machine Learning Models to Predict the Risk of Rapidly Progressive Kidney Disease and the Need for Nephrology Referral in Adult Patients with Type 2 Diabetes. International Journal of Environmental Research and Public Health. 2023; 20(4):3396. https://doi.org/10.3390/ijerph20043396
Chicago/Turabian StyleHsu, Chia-Tien, Kai-Chih Pai, Lun-Chi Chen, Shau-Hung Lin, and Ming-Ju Wu. 2023. "Machine Learning Models to Predict the Risk of Rapidly Progressive Kidney Disease and the Need for Nephrology Referral in Adult Patients with Type 2 Diabetes" International Journal of Environmental Research and Public Health 20, no. 4: 3396. https://doi.org/10.3390/ijerph20043396
APA StyleHsu, C. -T., Pai, K. -C., Chen, L. -C., Lin, S. -H., & Wu, M. -J. (2023). Machine Learning Models to Predict the Risk of Rapidly Progressive Kidney Disease and the Need for Nephrology Referral in Adult Patients with Type 2 Diabetes. International Journal of Environmental Research and Public Health, 20(4), 3396. https://doi.org/10.3390/ijerph20043396