
A Quantitative Study on Employees’ Experiences of a Support Model for Systematic Work Environment Management in Swedish Municipalities



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
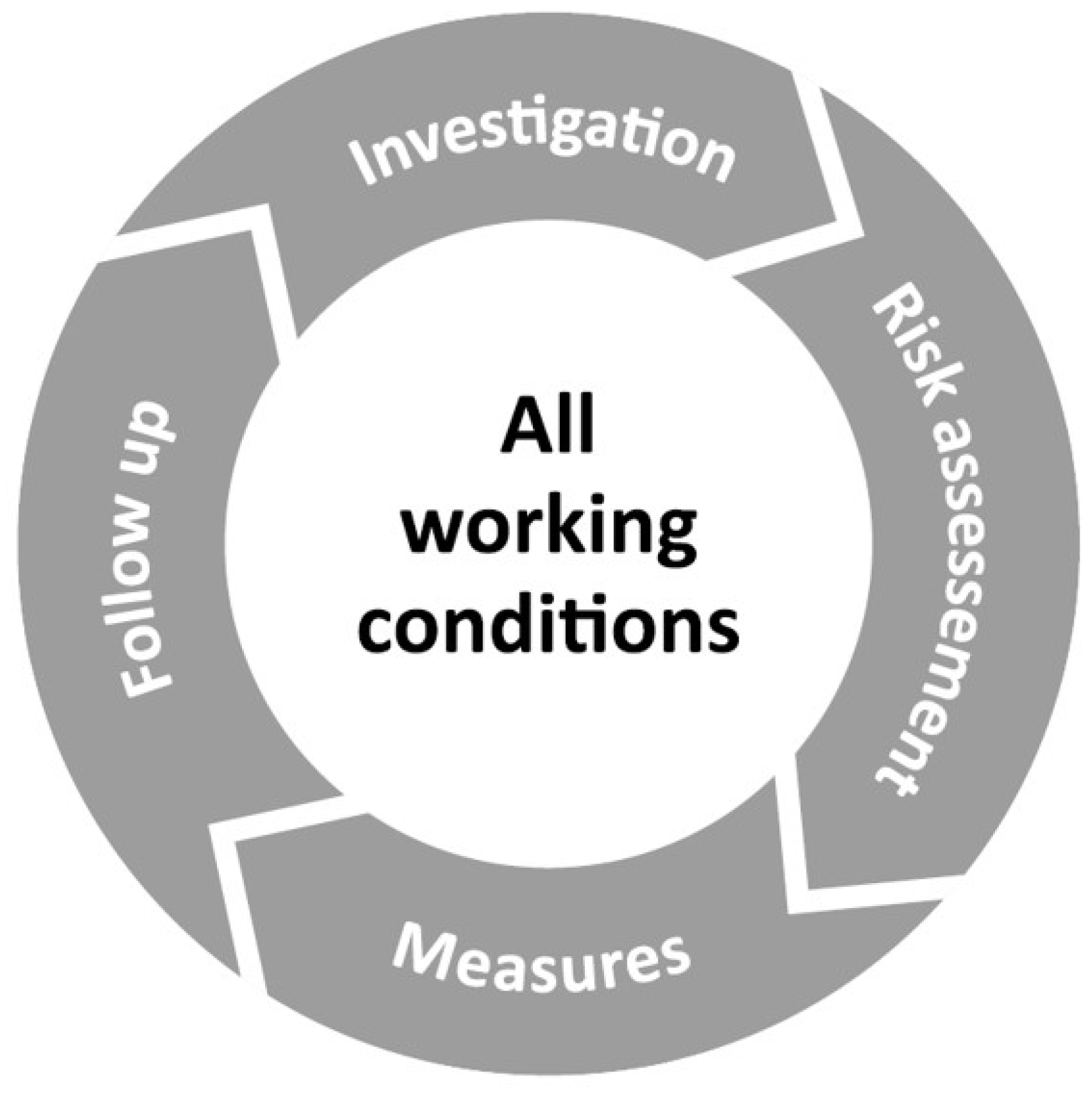
2.2. Stamina Model
2.3. Measures
2.3.1. Human Resource Index
2.3.2. Perceived Productivity
2.3.3. Organizational (Relational) Justice
2.3.4. Short-Term Recovery during Sleep
2.4. Data Analysis
3. Results
3.1. Participants

{kind=link}
{kind=link}
| Baseline (T1) | Time Point 2 (T2) | Time Point 3 (T3) | Time Point 4 (T4) | |
|---|---|---|---|---|
| Data collection | Spring 2017 | Autumn 2017 | Spring 2018 | Autumn 2018 |
| Days after T1 (mean) | - | 228 days | 357 days | 550 days |
| No. of participants (all municipals) | 1191 | 1005 | 558 | 329 |
| No. of free-text answers in total | 5 036 | 3688 | 1999 | 1863 |
3.2. Work Situation Categorisation, Attitude, and Perceived Influence
3.3. HRI, Perceived Productivity, Short-Term Recovery, and Relational Justice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Step 1. Introduction
- Your first answer—A thought or perception;
- Your second answer;
- Your third answer;
- Your fourth answer;
- Etc.
- Step 2. How would you describe your current work situation?
- Step 3. Evaluation
- 1. You wrote: [STRESS]
- What attitude do you have to this that you wrote?
- Negative—Positive.
- To what extent can you influence what you have written?
- Not at all—Completely.
- How important is this for you?
- Not at all important—Very important.
- Results and goal fulfilment;
- External circumstances and the outside world;
- Implementation and follow-up;
- Work environment and health;
- Roles and tasks;
- Skills and learning;
- Demands and feedback;
- Time use and working methods;
- Communication and collaboration;
- Other.
- Step 4. Research questions
References
- Väänänen, A.; Toivanen, M. The Challenge of Tied Autonomy for Traditional Work Stress Models. Work Stress 2018, 32, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Work-Related Diseases|Safety and Health at Work EU-OSHA. Available online: https://osha.europa.eu/en/themes/work-related-diseases (accessed on 13 February 2023).
- Försäkringskassan [Swedish Social Insurance Agency]. Sjukfrånvaro i Psykiatriska Diagnoser: En Registerstudie av Sveriges Arbetande Befolkning i åldern 20–69 år [Sick Leave due to Mental Disorders: A Register Based Study of the Working Population 20–69 Years in Sweden. Social Insurance Report 2020:8]; Swedish Social Insurance Agency: Stockholm, Sweden, 2020. [Google Scholar]
- Statens Beredning för Medicinsk Utvärdering (SBU); [Swedish Council on Health Technology Assessment]. Arbetsmiljöns Betydelse för Symtom på Depression Och Utmattningssyndrom. En Systematisk Litteraturöversikt. [The Importance of the Work Environment for Symptoms of Depression and Fatigue Syndrome. A Systematic Literature Review]; Swedish Council on Health Technology Assessment: Stockholm, Sweden, 2014; p. 461. [Google Scholar]
- Kivimäki, M.; Nyberg, S.T.; Pentti, J.; Madsen, I.E.H.; Hanson, L.L.M.; Rugulies, R.; Vahtera, J.; Coggon, D. IPD-Work consortium Individual and Combined Effects of Job Strain Components on Subsequent Morbidity and Mortality. Epidemiology 2019, 30, e27–e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madsen, I.E.H.; Nyberg, S.T.; Hanson, L.L.M.; Ferrie, J.E.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Job Strain as a Risk Factor for Clinical Depression: Systematic Review and Meta-Analysis with Additional Individual Participant Data. Psychol. Med. 2017, 47, 1342–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Council Directive. Council Directive 89/391/EEC of 12 June 1989 on the Introduction of Measures to Encourage Improvements in the Safety and Health of Workers at Work. Off. J. Eur. Communities 1989, 183, 1–11, Directive 89/391/EEC. [Google Scholar]
- Arbetsmiljöverket [Swedish Work Environment Authority]. Provision AFS 2001:1: Systematiskt Arbetsmiljöarbete. [Systematic Work Environment Management]; Swedish Work Environment Authority: Stockholm, Sweden, 2001; Volume 1. [Google Scholar]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can Work Make You Mentally Ill? A Systematic Meta-Review of Work-Related Risk Factors for Common Mental Health Problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Van Eerd, D.; Cole, D.; Irvin, E.; Mahood, Q.; Keown, K.; Theberge, N.; Village, J.; St. Vincent, M.; Cullen, K. Process and Implementation of Participatory Ergonomic Interventions: A Systematic Review. Ergonomics 2010, 53, 1153–1166. [Google Scholar] [CrossRef]
- Nielsen, K.; Randall, R.; Holten, A.-L.; González, E. Conducting Organizational-Level Occupational Health Interventions: What Works? Work Stress 2010, 24, 234–259. [Google Scholar] [CrossRef]
- Fox, K.E.; Johnson, S.T.; Berkman, L.F.; Sianoja, M.; Soh, Y.; Kubzansky, L.D.; Kelly, E.L. Organisational-and Group-Level Workplace Interventions and Their Effect on Multiple Domains of Worker Well-Being: A Systematic Review. Work Stress 2022, 36, 30–59. [Google Scholar] [CrossRef]
- Fransson, E.I.; Nyberg, S.T.; Heikkilä, K.; Alfredsson, L.; Bacquer, D.D.; Batty, G.D.; Bonenfant, S.; Casini, A.; Clays, E.; Goldberg, M.; et al. Comparison of Alternative Versions of the Job Demand-Control Scales in 17 European Cohort Studies: The IPD-Work Consortium. BMC Public Health 2012, 12, 62. [Google Scholar] [CrossRef] [Green Version]
- Karasek, R.A. Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Johnson, J.V.; Hall, E.M. Job Strain, Work Place Social Support, and Cardiovascular Disease: A Cross-Sectional Study of a Random Sample of the Swedish Working Population. Am. J. Public Health 1988, 78, 1336–1342. [Google Scholar] [CrossRef] [Green Version]
- Theorell, T.; Hammarström, A.; Aronsson, G.; Träskman Bendz, L.; Grape, T.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Hall, C. A Systematic Review Including Meta-Analysis of Work Environment and Depressive Symptoms. BMC Public Health 2015, 15, 738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theorell, T.; De Manzano, Ö.; Lennartsson, A.-K.; Pedersen, N.L.; Ullén, F. Self-Reported Psychological Demands, Skill Discretion and Decision Authority at Work: A Twin Study. Scand. J. Public Health 2016, 44, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An Instrument for Internationally Comparative Assessments of Psychosocial Job Characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef]
- De Jonge, J.; Kompier, M.A.J. A Critical Examination of the Demand-Control-Support Model from a Work Psychological Perspective. Int. J. Stress Manag. 1997, 4, 235–258. [Google Scholar] [CrossRef]
- Rugulies, R.; Martin, M.H.T.; Garde, A.H.; Persson, R.; Albertsen, K. Deadlines at Work and Sleep Quality. Cross-Sectional and Longitudinal Findings among Danish Knowledge Workers. Am. J. Ind. Med. 2012, 55, 260–269. [Google Scholar] [CrossRef]
- Väänänen, A.; Kumpulainen, R.; Kevin, M.V.; Ala-Mursula, L.; Kouvonen, A.; Kivimäki, M.; Toivanen, M.; Linna, A.; Vahtera, J. Work-Family Characteristics as Determinants of Sickness Absence: A Large-Scale Cohort Study of Three Occupational Grades. J. Occup. Health Psychol. 2008, 13, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.F.; Svendsen, P.A.; Nielsen, K.; Brinkmann, S.; Rugulies, R.; Madsen, I.E.H. Influence at Work Is a Key Factor for Mental Health—But What Do Contemporary Employees in Knowledge and Relational Work Mean by “Influence at Work”? Int. J. Qual. Stud. Health Well-Being 2022, 17, 2054513. [Google Scholar] [CrossRef]
- Dyne, L.V.; Ang, S.; Botero, I.C. Conceptualizing Employee Silence and Employee Voice as Multidimensional Constructs*. J. Manag. Stud. 2003, 40, 1359–1392. [Google Scholar] [CrossRef]
- Wheelan, S.A. Creating Effective Teams. A Guide for Members and Leaders, 4th ed.; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2013; ISBN 978-1-4833-4612-0. [Google Scholar]
- Wheelan, S.A.; Kesselring, J. Link Between Faculty Group: Development and Elementary Student Performance on Standardized Tests. J. Educ. Res. 2005, 98, 323–330. [Google Scholar] [CrossRef]
- Hellman, T.; Molin, F.; Svartengren, M. A Mixed-Method Study of Providing and Implementing a Support Model Focusing on Systematic Work Environment Management. J. Occup. Environ. Med. 2020, 62, e160–e166. [Google Scholar] [CrossRef] [PubMed]
- Hellman, T.; Molin, F.; Svartengren, M. A Qualitative Study on Employees’ Experiences of a Support Model for Systematic Work Environment Management. Int. J. Environ. Res. Public Health 2019, 16, 3551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molin, F.; Hellman, T.; Svartengren, M. Implementing New Working Practices Through a Structured Support Model for Systematic Work Environment Management: A Qualitative Study From Swedish Municipalities. J. Occup. Environ. Med. 2021, 63, e259–e266. [Google Scholar] [CrossRef] [PubMed]
- Arakelian, E.; Paulsson, S.; Molin, F.; Svartengren, M. How Human Resources Index, Relational Justice, and Perceived Productivity Change after Reorganization at a Hospital in Sweden That Uses a Structured Support Model for Systematic Work Environment Management. Int. J. Environ. Res. Public Health 2021, 18, 11611. [Google Scholar] [CrossRef] [PubMed]
- Ndjaboué, R.; Brisson, C.; Vézina, M. Organisational Justice and Mental Health: A Systematic Review of Prospective Studies. Occup. Environ. Med. 2012, 69, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J. A Taxonomy of Organizational Justice Theories. Acad. Manag. Rev. 1987, 12, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, J. Organizational Justice: Yesterday, Today, and Tomorrow. J. Manag. 1990, 16, 399–432. [Google Scholar] [CrossRef]
- Greenberg, J. Organizational Injustice as an Occupational Health Risk. Acad. Manag. Ann. 2010, 4, 205–243. [Google Scholar] [CrossRef]
- Kivimäki, M.; Elovainio, M.; Vahtera, J.; Ferrie, J.E. Organisational Justice and Health of Employees: Prospective Cohort Study. Occup. Environ. Med. 2003, 60, 27–33, discussion 33-34. [Google Scholar] [CrossRef] [Green Version]
- Sonnentag, S.; Fritz, C. The Recovery Experience Questionnaire: Development and Validation of a Measure for Assessing Recuperation and Unwinding from Work. J. Occup. Health Psychol. 2007, 12, 204–221. [Google Scholar] [CrossRef] [Green Version]
- Åkerstedt, T.; Hume, K.; Minors, D.; Waterhouse, J. The Subjective Meaning of Good Sleep, An Intraindividual Approach Using the Karolinska Sleep Diary. Percept. Mot. Skills 1994, 79, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Linton, S.J.; Kecklund, G.; Franklin, K.A.; Leissner, L.C.; Sivertsen, B.; Lindberg, E.; Svensson, A.C.; Hansson, S.O.; Sundin, Ö.; Hetta, J.; et al. The Effect of the Work Environment on Future Sleep Disturbances: A Systematic Review. Sleep Med. Rev. 2015, 23, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Morphy, H.; Dunn, K.M.; Lewis, M.; Boardman, H.F.; Croft, P.R. Epidemiology of Insomnia: A Longitudinal Study in a UK Population. Sleep 2007, 30, 274–280. [Google Scholar] [PubMed] [Green Version]
- Buysse, D.J.; Grunstein, R.; Horne, J.; Lavie, P. Can an Improvement in Sleep Positively Impact on Health? Sleep Med. Rev. 2010, 14, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.; Hagen, S.E.; Sathyanarayanan, S.; Schultz, A.B.; Edington, D.W. Presenteeism: Critical Issues. J. Occup. Environ. Med. 2010, 52, 1055–1067. [Google Scholar] [CrossRef]
- Karlsson, M.L.; Bergström, G.; Björklund, C.; Hagberg, J.; Jensen, I. Measuring Production Loss Due to Health and Work Environment Problems: Construct Validity and Implications. J. Occup. Environ. Med. 2013, 55, 1475–1483. [Google Scholar] [CrossRef]
- Lohela-Karlsson, M.; Hagberg, J.; Bergström, G. Production Loss among Employees Perceiving Work Environment Problems. Int. Arch. Occup. Environ. Health 2015, 88, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Svartengren, M.; Hellman, T. Study Protocol of an Effect and Process Evaluation of the Stamina Model; a Structured and Time-Effective Approach through Methods for an Inclusive and Active Working Life. BMC Public Health 2018, 18, 1070. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Evans, R.E.; Hawkins, J.; Littlecott, H.; Melendez-Torres, G.J.; Bonell, C.; Murphy, S. From Complex Social Interventions to Interventions in Complex Social Systems: Future Directions and Unresolved Questions for Intervention Development and Evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef] [Green Version]
- Molin, F.; Hellman, T.; Svartengren, M. First-Line Managers’ Experiences of Working with a Structured Support Model for Systematic Work Environment Management. Int. J. Environ. Res. Public Health 2020, 17, 3884. [Google Scholar] [CrossRef]
- Molin, F.; Paulsson, S.Å.; Hellman, T.; Svartengren, M. Can the Human Resources Index (HRI) Be Used as a Process Feedback Measurement in a Structured Support Model for Systematic Work Environment Management? Int. J. Environ. Res. Public Health 2021, 18, 6509. [Google Scholar] [CrossRef]
- Josephson, M.; Vingård, E. Zest for Work? Assessment of Enthusiasm and Satisfaction with the Present Work Situation and Health—A 1.5-Year Follow-up Study. Work 2007, 29, 225–231. [Google Scholar] [PubMed]
- Aboagye, E.; Jensen, I.; Bergström, G.; Hagberg, J.; Axén, I.; Lohela-Karlsson, M. Validity and Test–Retest Reliability of an at-Work Production Loss Instrument. Occup. Med. 2016, 66, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elovainio, M.; Heponiemi, T.; Sinervo, T.; Magnavita, N. Organizational Justice and Health; Review of Evidence. G. Ital. Med. Lav. Ergon. 2010, 32, B5–B9. [Google Scholar] [PubMed]
- Stoetzer, U.; Bergman, P.; Aborg, C.; Johansson, G.; Ahlberg, G.; Parmsund, M.; Svartengren, M. Organizational Factors Related to Low Levels of Sickness Absence in a Representative Set of Swedish Companies. Work 2014, 47, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Stoetzer, U.; Åborg, C.; Johansson, G.; Svartengren, M. Organization, Relational Justice and Absenteeism. Work 2014, 47, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A Systematic Review Including Meta-Analysis of Work Environment and Burnout Symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lallukka, T.; Haaramo, P.; Rahkonen, O.; Sivertsen, B. Joint Associations of Sleep Duration and Insomnia Symptoms with Subsequent Sickness Absence: The Helsinki Health Study. Scand. J. Public Health 2013, 41, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Nordin, M.; Åkerstedt, T.; Nordin, S. Psychometric Evaluation and Normative Data for the Karolinska Sleep Questionnaire. Sleep Biol. Rhythm. 2013, 11, 216–226. [Google Scholar] [CrossRef]
- Weiner, B.J. A Theory of Organizational Readiness for Change. Implement. Sci. 2009, 4, 67. [Google Scholar] [CrossRef] [Green Version]
- Cedstrand, E.; Augustsson, H.; Alderling, M.; Sánchez Martinez, N.; Bodin, T.; Nyberg, A.; Johansson, G. Effects of a Co-Created Occupational Health Intervention on Stress and Psychosocial Working Conditions within the Construction Industry: A Controlled Trial. Front. Public Health 2022, 10, 973890. [Google Scholar] [CrossRef] [PubMed]


| Category | Free-Text Answers Assigned to Each Category * (%) | Positive Attitude within Each Category (%) † | Perceived Influence within Each Category (%) ‡ | ||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 | T3 | p-Value, Difference | T1 | T3 | p-Value, Difference | T1 | T3 | p-Value, Difference | |
| (1) Results and goal fulfilment | 6.4 | 7.6 | p = 0.081 | 66.3 | 68.4 | p = 0.716 | 59.8 | 67.8 | p = 0.114 |
| (2) External circumstances and the outside world | 4.7 | 4.4 | p = 0.603 | 41.6 | 39.8 | p = 0.865 | 28.2 | 28.4 | p = 1.00 |
| (3) Implementation and follow-up | 5.2 | 6.6 | p = 0.027 | 68.1 | 70.5 | p = 0.712 | 65.0 | 68.9 | p = 0.506 |
| (4) Work environment and health | 34.8 | 34.7 | p = 1.00 | 42.7 | 46.5 | p = 0.096 | 40.0 | 43.1 | p = 0.176 |
| (5) Roles and tasks | 10.8 | 10.7 | p = 0.978 | 57.9 | 68.7 | p = 0.008 | 50.0 | 65.0 | p < 0.001 |
| (6) Skills and learning | 9.0 | 8.2 | p = 0.304 | 79.2 | 77.9 | p = 0.825 | 73.2 | 72.4 | p = 0.929 |
| (7) Demands and feedback | 2.3 | 1.5 | p = 0.037 | 43.0 | 34.5 | p = 0.536 | 37.7 | 24.1 | p = 0.249 |
| (8) Time use and working methods | 7.9 | 8.3 | p = 0.701 | 45.0 | 38.2 | p = 0.163 | 45.8 | 41.2 | p = 0.371 |
| (9) Communication and collaboration | 15.8 | 14.7 | p = 0.266 | 67.3 | 70.1 | p = 0.432 | 66.1 | 72.8 | p = 0.042 |
| (10) Other | 3.2 | 3.4 | p = 0.654 | 56.6 | 52.9 | p = 0.717 | 47.2 | 51.5 | p = 0.654 |
| Variable | T1 M (SD) | T2 M (SD) | T3 M (SD) | Difference T1 and T3 | p-Value |
|---|---|---|---|---|---|
| Human Resources Index, HRI | 60.02 (20.93) | 59.76 (22.70) | 60.64 (23.67) | 0.62 | 0.593 † |
| Relational Justice Index, RJI * | 24.77 (4.42) | 24.98 (4.29) | 24.95 (4.40) | 0.18 | 0.416 ‡ |
| Short-term recovery * | 3.74 (1.24) | 3.81 (1.20) | 3.88 (1.25) | 0.14 | 0.253 ‡ |
| Health-related production loss | 3.12 (2.45) | 3.49 (2.85) | 3.30 (2.61) | 0.18 | 0.337 ‡ |
| Work environment related production loss | 3.39 (2.43) | 3.31 (2.49) | 3.58 (2.54) | 0.19 | 0.099 ‡ |
| HRI <= Median n = 596 M(SD) | HRI > Median n = 595 M(SD) | Cohen’s D | |
|---|---|---|---|
| Relational Justice Index | 23.7 (4.78) | 25.8 (3.72) | 0.490 |
| Short-term recovery | 3.46 (1.23) | 4.02 (1.20) | 0.461 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulsson, S.; Hellman, T.; Svartengren, M.; Molin, F. A Quantitative Study on Employees’ Experiences of a Support Model for Systematic Work Environment Management in Swedish Municipalities. Int. J. Environ. Res. Public Health 2023, 20, 4010. https://doi.org/10.3390/ijerph20054010
Paulsson S, Hellman T, Svartengren M, Molin F. A Quantitative Study on Employees’ Experiences of a Support Model for Systematic Work Environment Management in Swedish Municipalities. International Journal of Environmental Research and Public Health. 2023; 20(5):4010. https://doi.org/10.3390/ijerph20054010
Chicago/Turabian StylePaulsson, Sofia, Therese Hellman, Magnus Svartengren, and Fredrik Molin. 2023. "A Quantitative Study on Employees’ Experiences of a Support Model for Systematic Work Environment Management in Swedish Municipalities" International Journal of Environmental Research and Public Health 20, no. 5: 4010. https://doi.org/10.3390/ijerph20054010
APA StylePaulsson, S., Hellman, T., Svartengren, M., & Molin, F. (2023). A Quantitative Study on Employees’ Experiences of a Support Model for Systematic Work Environment Management in Swedish Municipalities. International Journal of Environmental Research and Public Health, 20(5), 4010. https://doi.org/10.3390/ijerph20054010