
13-Type HPV DNA Test versus 5-Type HPV mRNA Test in Triage of Women Aged 25–33 Years with Minor Cytological Abnormalities–6 Years of Follow-Up

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
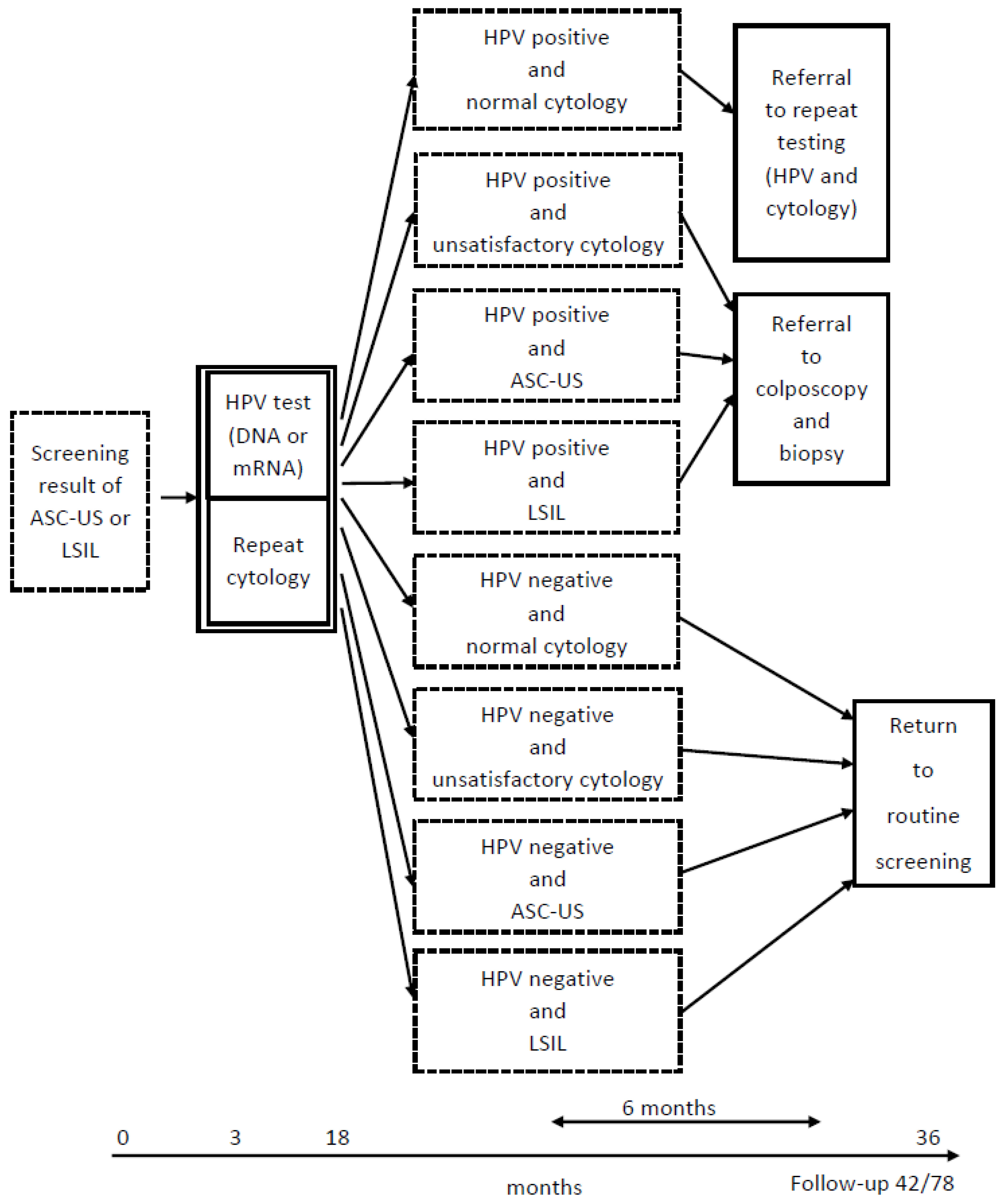
2.2. Study Sample and Screening Algorithm
2.3. HPV Testing
2.4. Outcomes and Follow-Up
2.5. Statistical Analyses
3. Results
4. Discussion
4.1. HPV Positivity Rates at Triage
4.2. Referral Rates for Colposcopy and Biopsy and Repeat Testing after Triage
4.3. CIN3+ Detection Rate
4.4. HPV Types Included in the Test
4.5. Overmanagement and Overtreatment
4.6. Strengths
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jansen, E.E.L.; Zielonke, N.; Gini, A.; Anttila, A.; Segnan, N.; Vokó, Z.; Ivanuš, U.; McKee, M.; de Koning, H.J.; de Kok, I.M.C.M.; et al. Effect of organised cervical cancer screening on cervical cancer mortality in Europe: A systematic review. Eur. J. Cancer 2020, 127, 207–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koliopoulos, G.; Nyaga, V.N.; Santesso, N.; Bryant, A.; Martin-Hirsch, P.P.; Mustafa, R.A.; Schünemann, H.; Paraskevaidis, E.; Arbyn, M. Cytology versus HPV testing for cervical cancer screening in the general population. Cochrane Database Syst. Rev. 2017, 8, CD008587. [Google Scholar] [CrossRef] [PubMed]
- Polman, N.; Snijders, P.; Kenter, G.; Berkhof, J.; Meijer, C. HPV-based cervical screening: Rationale, expectations and future perspectives of the new Dutch screening programme. Prev. Med. 2018, 119, 108–117. [Google Scholar] [CrossRef] [PubMed]
- England, P.H. Cervical Screening: Programme Overview. 2021. Available online: https://www.gov.uk/guidance/cervical-screening-programme-overview (accessed on 5 December 2022).
- National Cervical Screening Program: Guidelines for the Management of Screen-Detected Abnormalities, Screening in Specific Populations and Investigation of Abnormal Vaginal Bleeding. Available online: https://wiki.cancer.org.au/australiawiki/images/a/ad/National_Cervical_Screening_Program_guidelines_long-form_PDF.pdf (accessed on 5 December 2022).
- WHO. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, 2nd ed.; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- von Karsa, L.; Arbyn, M.; De Vuyst, H.; Dillner, J.; Dillner, L.; Franceschi, S.; Patnick, J.; Ronco, G.; Segnan, N.; Suonio, E.; et al. European guidelines for quality assurance in cervical cancer screening. Summary of the supplements on HPV screening and vaccination. Papillomavirus Res. 2015, 1, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Institution, T.P.H. Turkey Cancer Control Programme. 2016. Available online: https://www.iccp-portal.org/system/files/plans/Turkiye_Kanser_Kontrol_Program_English.pdf (accessed on 5 December 2022).
- Socialstyrelsen. Senaste Versionen av HSLF-FS 2019:14 Socialstyrelsens Föreskrifter Och Allmänna Råd om Villkor för Avgiftsfri Screening. 2021. Available online: https://www.socialstyrelsen.se/kunskapsstod-och-regler/regler-och-riktlinjer/foreskrifter-och-allmanna-rad/konsoliderade-foreskrifter/201914-om-villkor-for-avgiftsfri-screening/ (accessed on 5 December 2022).
- Norway, C.R.O. HPV I Primærscreening. Cancer Registry of Norway. Available online: https://www.kreftregisteret.no/en/screening/cervix/Helsepersonell/screeningstrategi-og-nasjonale-retningslinjer/hpv-i-primarscreening/ (accessed on 5 December 2022).
- Norway, T.C.R.O. Primary HPV Test—Now also for Women Under 34. 2023. Available online: https://www.kreftregisteret.no/screening/livmorhalsprogrammet/hpv/ (accessed on 5 December 2022).
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; de Sanjosé, S. Cervical Human Papillomavirus Prevalence in 5 Continents: Meta-Analysis of 1 Million Women with Normal Cytological Findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef] [Green Version]
- Moscicki, A.-B.; Ma, Y.; Wibbelsman, C.; Powers, A.; Darragh, T.M.; Farhat, S.; Shaber, R.; Shiboski, S. Risks for Cervical Intraepithelial Neoplasia 3 Among Adolescents and Young Women with Abnormal Cytology. Obstet. Gynecol. 2008, 112, 1335–1342. [Google Scholar] [CrossRef] [Green Version]
- Moscicki, A.-B.; Ma, Y.; Wibbelsman, C.J.; Darragh, T.M.; Powers, A.; Farhat, S.; Shiboski, S. Rate of and Risks for Regression of Cervical Intraepithelial Neoplasia 2 in Adolescents and Young Women. Obstet. Gynecol. 2010, 116, 1373–1380. [Google Scholar] [CrossRef] [Green Version]
- Molden, T.; Kraus, I.; Karlsen, F.; Skomedal, H.; Hagmar, B. Human papillomavirus E6/E7 mRNA expression in women younger than 30 years of age. Gynecol. Oncol. 2006, 100, 95–100. [Google Scholar] [CrossRef]
- Ho, G.Y.; Bierman, R.; Beardsley, L.; Chang, C.J.; Burk, R.D. Natural History of Cervicovaginal Papillomavirus Infection in Young Women. N. Engl. J. Med. 1998, 338, 423–428. [Google Scholar] [CrossRef]
- Boardman, L.A.; Robison, K. Screening adolescents and young women. In Obstetrics and Gynecology Clinics of North America; W.B. Saunders Ltd.: Philadelphia, PE, USA, 2013; pp. 257–268. [Google Scholar]
- Engesæter, B.L.G.; Skare, G.B.; Tropé, A. Årsrapport 2021—Screeningaktivitet og Resultater fra Livmorhalsprogrammet; Cancer Registry of Norway: Oslo, Norway, 2021. [Google Scholar]
- Baldauf, J.J.; Ritter, J. Comparison of the risks of cytologic surveillance of women with atypical cells or low-grade abnormalities on cervical smear: Review of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 1998, 76, 193–199. [Google Scholar] [CrossRef]
- Stefani, C.; A Liverani, C.; Bianco, V.; Penna, C.; Guarnieri, T.; Comparetto, C.; Monti, E.; Valente, I.; Pieralli, A.L.; Fiaschi, C.; et al. Spontaneous regression of low-grade cervical intraepithelial lesions is positively improved by topical bovine colostrum preparations (GINEDIE®). A multicentre, observational, Italian pilot study. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 728–733. [Google Scholar] [PubMed]
- St-Martin, G.; Thamsborg, L.H.; Andersen, B.; Christensen, J.; Ejersbo, D.; Jochumsen, K.; Johansen, T.; Larsen, L.G.; Waldstrøm, M.; Lynge, E. Management of low-grade cervical cytology in young women. Cohort study from Denmark. Acta Oncol. 2020, 60, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Katki, H.A.; Schiffman, M.; Castle, P.E.; Fetterman, B.; Poitras, N.E.; Lorey, T.; Cheung, L.; Raine-Bennett, T.R.; Gage, J.C.; Kinney, W.K. Benchmarking CIN 3+ Risk as the Basis for Incorporating HPV and Pap Cotesting into Cervical Screening and Management Guidelines. J. Low. Genit. Tract Dis. 2013, 17, S28–S35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tjalma, W.A.; Fiander, A.; Reich, O.; Powell, N.; Nowakowski, A.; Kirschner, B.; Koiss, R.; O’Leary, J.; Joura, E.A.; Rosenlund, M.; et al. Differences in human papillomavirus type distribution in high-grade cervical intraepithelial neoplasia and invasive cervical cancer in Europe. Int. J. Cancer 2012, 132, 854–867. [Google Scholar] [CrossRef]
- Sørbye, S.W.; Fismen, S.; Gutteberg, T.J.; Mortensen, E.S.; Skjeldestad, F.E. HPV mRNA Is More Specific than HPV DNA in Triage of Women with Minor Cervical Lesions. PLoS ONE 2014, 9, e112934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayar, R.; Wilbur, D.C. The Pap Test and Bethesda 2014. “The reports of my demise have been greatly exaggerated”. (after a quotation from Mark Twain). Acta. Cytol. 2015, 59, 121–132. [Google Scholar] [CrossRef]
- WHO. Comprehensive Cervical Cancer Control: A guide to essential practice. In Comprehensive Cervical Cancer Control: A Guide to Essential Practice; WHO: Geneva, Swrizterland, 2006. [Google Scholar]
- QIAGEN. Digene Specimen Transport Medium. 2023. Available online: https://www.qiagen.com/de/products/diagnostics-and-clinical-research/sexual-reproductive-health/cervical-cancer-screening/digene-specimen-transport-medium (accessed on 5 December 2022).
- PreTect, T.M. 2023. Available online: https://www.pretect.no/products/pretecttm (accessed on 5 December 2022).
- QIAGEN. Digene HC2 HPV DNA Test. 2023. Available online: https://www.qiagen.com/us/products/diagnostics-and-clinical-research/sexual-reproductive-health/cervical-cancer-screening/digene-hc2-hpv-dna-test (accessed on 5 December 2022).
- PreTect. PRETECT HPV-PROOFER. 2023. Available online: https://www.pretect.no/products/pretecthpvproofermoreinformation (accessed on 5 December 2022).
- PreTect. NASBA—NUCLEIC ACID SEQUENCE BASED AMPLIFICATION. 2023. Available online: https://www.pretect.no/nasba (accessed on 5 December 2022).
- Arbyn, M.; Martin-Hirsch, P.; Buntinx, F.; Van Ranst, M.; Paraskevaidis, E.; Dillner, J. Triage of women with equivocal or low-grade cervical cytology results: A meta-analysis of the HPV test positivity rate. J. Cell Mol. Med. 2009, 13, 648–659. [Google Scholar] [CrossRef] [Green Version]
- Reinholdt, K.J.K.E.; Dehlendorff, C.; Munk, C.; Kjær, S.K.; Thomsen, L.T. Triage of low-grade squamous intraepithelial lesions using human papillomavirus messenger ribonucleic acid tests—A prospective population-based register study. Acta Obstet. Gynecol.Scand. 2019, 17, e0275858. [Google Scholar] [CrossRef]
- Westre, B.; Giske, A.; Guttormsen, H.; Sørbye, S.; Skjeldestad, F.E. 5-type HPV mRNA versus 14-type HPV DNA test: Test performance, over-diagnosis and overtreatment in triage of women with minor cervical lesions. BMC Clin. Pathol. 2016, 16, 9. [Google Scholar] [CrossRef] [Green Version]
- Thomsen, L.T.; Dehlendorff, C.; Junge, J.; Waldstrom, M.; Schledermann, D.; Frederiksen, K.; Kjaer, S.K. Human papillomavirus mRNA and DNA testing in women with atypical squamous cells of undetermined significance: A prospective cohort study. Int. J. Cancer 2016, 139, 1839–1850. [Google Scholar] [CrossRef] [Green Version]
- Katki, H.A.; Schiffman, M.; Castle, P.; Fetterman, B.; Poitras, N.; Lorey, T.; Cheung, L.; Raine-Bennett, T.; Gage, J.; Kinney, W. Five-year risks of CIN 3+ and cervical cancer among women who test Pap-negative but are HPV-positive. J. Low Genit. Tract. Dis. 2013, 17 (Suppl. S1), S56–S63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egemen, D.; Cheung, L.; Chen, X.; Demarco, M.; Perkins, R.; Kinney, W.; Poitras, N.; Befano, B.; Locke, A.; Guido, R.; et al. Risk Estimates Supporting the 2019 ASCCP Risk-Based Management Consensus Guidelines. J. Low Genit. Tract. Dis. 2020, 24, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.; Sorbye, S.; Kristiansen, I.; Burger, E.A. Using novel biomarkers to triage young adult women with minor cervical lesions: A cost-effectiveness analysis. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 474–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundstrom, K.; Dillner, J. How many Human Papillomavirus types do we need to screen for? J. Infect. Dis. 2020, 22, 1510–1511. [Google Scholar] [CrossRef]
- Norway, C.R.O. Cervical Cancer Screening Programme. 2021. Available online: https://www.kreftregisteret.no/en/screening/cervix/org/ (accessed on 5 December 2022).
- Bjørge, T.; Skare, G.; Bjørge, L.; Tropé, A.; Lönnberg, S. Adverse Pregnancy Outcomes After Treatment for Cervical Intraepithelial Neoplasia. Obstet. Gynecol. 2016, 128, 1265–1273. [Google Scholar] [CrossRef]
- Castle, P.E.; Schiffman, M.; Wheeler, C.; Solomon, D. Evidence for frequent regression of cervical intraepithelial neoplasia-grade 2. Obstet. Gynecol. 2009, 113, 18–25. [Google Scholar] [CrossRef] [Green Version]
- McCredie, M.R.; Sharples, K.; Paul, C.; Baranyai, J.; Medley, G.; Jones, R.; Skegg, D. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: A retrospective cohort study. Lancet Oncol. 2008, 9, 425–434. [Google Scholar] [CrossRef]
- Ronco, G.; Giorgi-Rossi, P.; Carozzi, F.; Confortini, M.; Palma, P.D.; Del Mistro, A.; Ghiringhello, B.; Girlando, S.; Gillio-Tos, A.; De Marco, L.; et al. New Technologies for Cervical Cancer screening Working. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: A randomised controlled trial. Lancet Oncol. 2010, 11, 249–257. [Google Scholar] [CrossRef]


{kind=link}
| HPV DNA n = 2556 (%) | HPV mRNA n = 1559 (%) | p-Value | ||
|---|---|---|---|---|
| Age (years) | 25–29 | 60.4 | 59.9 | 0.771 |
| 30–33 | 39.6 | 40.1 | ||
| Screening result | ASC-US | 65.9 | 68.8 | 0.06 |
| LSIL | 34.1 | 31.2 | ||
| Most recent cytology result before screening | No Previous Test | 35.5 | 36.0 | 0.603 |
| Unsatisfactory | 3.0 | 3.5 | ||
| Normal | 61.5 | 60.5 | ||
| Triage Results | HPV DNA n = 2556 (%) | HPV mRNA n = 1559 (%) | |
|---|---|---|---|
| HPV | Cytology | ||
| Positive | Normal | 713 (27.9%) | 79 (5.1%) |
| Unsatisfactory | 32 (1.3%) | 3 (0.2%) | |
| ASC-US | 285 (11.2%) | 131 (8.4%) | |
| LSIL | 320 (12.5%) | 151 (9.7%) | |
| Total | 1350 (52.8%)* | 364 (23.3%) * | |
| Negative | Normal | 1042 (40.8%) | 852 (54.7%) |
| Unsatisfactory | 43 (1.7%) | 26 (1.7%) | |
| ASC-US | 93 (3.6%) | 206 (13.2%) | |
| LSIL | 28 (1.1%) | 111 (7.1%) | |
| Total | 1206 (47.2%) * | 1195 (76.7%) * | |
| SAR Group after Triage | Status | 42 Months Post-Screening | p-Value | 78 Months Post-Screening | p-Value | ||
|---|---|---|---|---|---|---|---|
| HPV DNA | HPV mRNA | HPV DNA | HPV mRNA | ||||
| SAR Referral for Colposcopy and Biopsy | n = 637 (%) | n = 285 (%) | n = 637 (%) | n = 285 (%) | |||
| Did not attend | 7 (1.1) | 1 (0.4) | 7 (1.1) | 1 (0.4) | |||
| Incomplete follow-up | 292 (45.8) | 113 (39.6) | 135 (21.2) | 45 (15.8) | |||
| Returned to routine screening | 86 (13.5) | 38 (13.3) | 229 (35.9) | 99 (34.7) | |||
| CIN2 | 50 (7.8) | 46 (16.1) | 53 (8.3) | 48 (16.8) | |||
| CIN3+ | 202 (31.7) | 87 (30.5) | 0.72 | 213 (33.4) | 92 (32.3) | 0.73 | |
| SAR Referral for Repeat Testing (HPV and Cytology) | n = 713 (%) | n = 79 (%) | n = 713 (%) | n = 79 (%) | |||
| Did not attend | 37 (5.2) | 3 (3.8) | 37 (5.2) | 3 (3.8) | |||
| Incomplete follow-up | 376 (52.7) | 45 (57.0) | 181 (25.4) | 17 (21.5) | |||
| Returned to routine screening | 139 (19.5) | 8 (10.1) | 322 (45.2) | 34 (43.0) | |||
| CIN2 | 29 (4.1) | 3 (3.8) | 31 (4.3) | 3 (3.8) | |||
| CIN3+ | 132 (18.5) | 20 (25.3) | 0.145 | 142 (19.9) | 22 (27.8) | 0.099 | |
| SAR Return to Screening | n = 1206 (%) | n = 1195 (%) | n = 1206 (%) | n = 1195 (%) | |||
| Did not attend | 308 (25.5) | 241 (20.2) | 308 (25.5) | 241 (20.2) | |||
| Incomplete follow-up | 799 (66.3) | 819 (68.5) | 560 (46.4) | 511 (42.8) | |||
| Returned to routine screening | 87 (7.2) | 103 (8.6) | 319 (26.5) | 398 (33.3) | |||
| CIN2 | 1 (0.1) | 10 (0.8) | 2 (0.2) | 12 (1.0) | |||
| CIN3+ | 11 (0.9) | 22 (1.8) | 0.05 | 17 (1.4) | 33 (2.8) | 0.02 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rad, A.; Sørbye, S.W.; Brenn, T.; Tiwari, S.; Løchen, M.-L.; Skjeldestad, F.E. 13-Type HPV DNA Test versus 5-Type HPV mRNA Test in Triage of Women Aged 25–33 Years with Minor Cytological Abnormalities–6 Years of Follow-Up. Int. J. Environ. Res. Public Health 2023, 20, 4119. https://doi.org/10.3390/ijerph20054119
Rad A, Sørbye SW, Brenn T, Tiwari S, Løchen M-L, Skjeldestad FE. 13-Type HPV DNA Test versus 5-Type HPV mRNA Test in Triage of Women Aged 25–33 Years with Minor Cytological Abnormalities–6 Years of Follow-Up. International Journal of Environmental Research and Public Health. 2023; 20(5):4119. https://doi.org/10.3390/ijerph20054119
Chicago/Turabian StyleRad, Amir, Sveinung Wergeland Sørbye, Tormod Brenn, Sweta Tiwari, Maja-Lisa Løchen, and Finn Egil Skjeldestad. 2023. "13-Type HPV DNA Test versus 5-Type HPV mRNA Test in Triage of Women Aged 25–33 Years with Minor Cytological Abnormalities–6 Years of Follow-Up" International Journal of Environmental Research and Public Health 20, no. 5: 4119. https://doi.org/10.3390/ijerph20054119
APA StyleRad, A., Sørbye, S. W., Brenn, T., Tiwari, S., Løchen, M. -L., & Skjeldestad, F. E. (2023). 13-Type HPV DNA Test versus 5-Type HPV mRNA Test in Triage of Women Aged 25–33 Years with Minor Cytological Abnormalities–6 Years of Follow-Up. International Journal of Environmental Research and Public Health, 20(5), 4119. https://doi.org/10.3390/ijerph20054119