
Interaction between Occupational and Non-Occupational Arsenic Exposure and Tobacco Smoke on Lung Cancerogenesis: A Systematic Review

 , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of Studies
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
3. Results
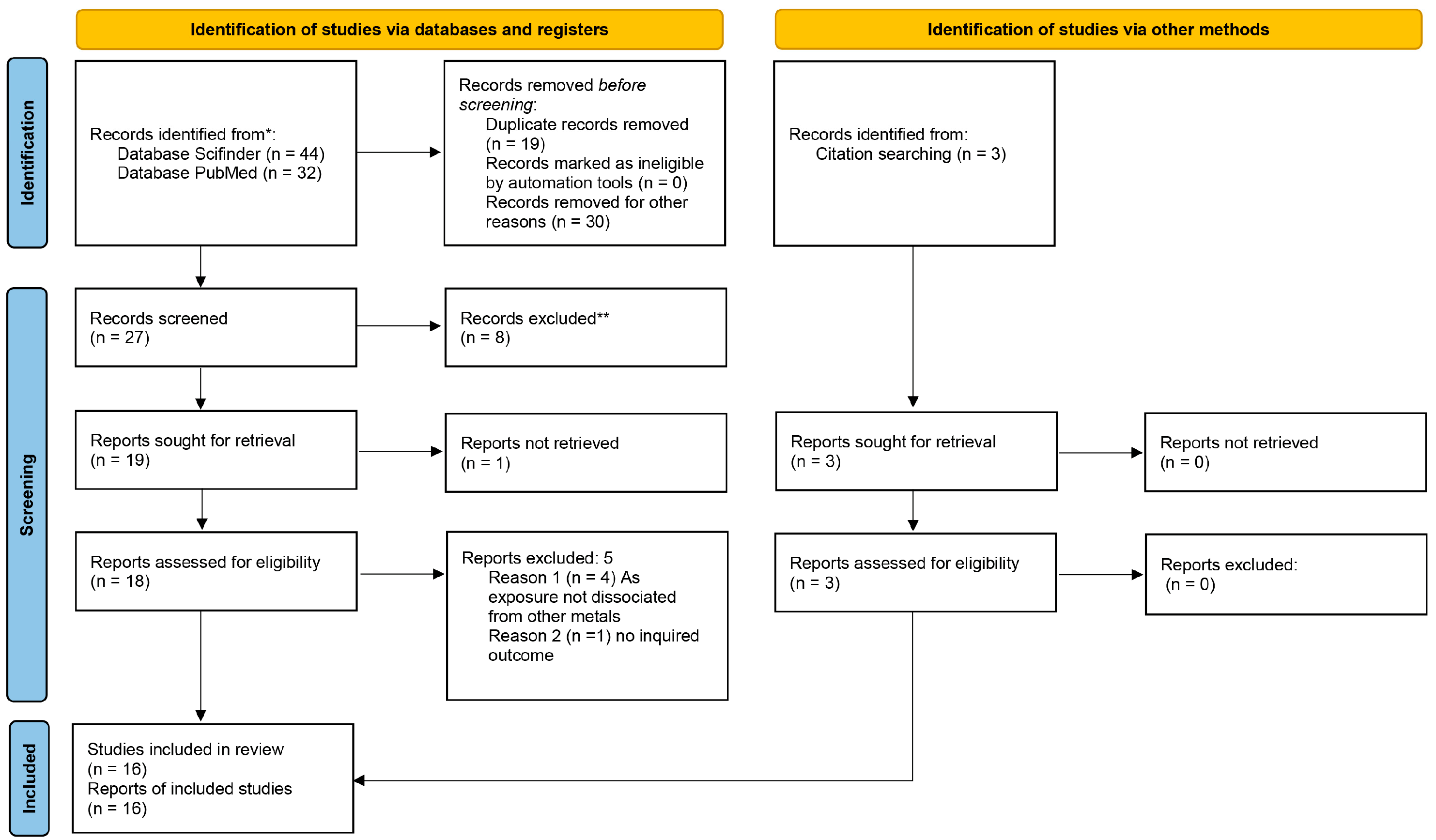
3.1. Study Selection
3.2. Characteristics of the Included Studies

{kind=link}
{kind=link}
| Author (Year) | Study Design | Subjects | Country | Age (Years) | Exposed Study Period | Data Collection | NOS * |
|---|---|---|---|---|---|---|---|
| Su Z. et al., 2022 [30] | Cohort | M/W (1215/405) | Taiwan | ≥40 | 1992–2019 | Baseline questionnaire and face to face interview | 9 |
| Fan Y. et al., 2016 [44] | Prospective occupational-based cohort | M/W (8696/599) | China | 40–59; 60–69; >70 | 1992–2001 | Personal interview | 5 |
| Steinmaus C.M. et al., 2015 [29] | Case-control | M/W (637/298) Cases: 301 Controls: 634 | Chile | Case: 65.9 ± 10.2 Control: 66.3 ± 11.3 | 2007–2009 | Standardized study questionnaire and government agencies, research studies | 6 |
| D’Ippoliti D. et al., 2015 [42] | Population-based | M/W (82,169/83,440) | Italy | ≤35; 36–64; >65 | 1990–2010 | Population registries | 4 |
| Steinmaus C.M. et al., 2014 [35] | Case-control | M/W (257/123) Cases: 92 Controls: 288 | Chile | 25–65 | 2007–2010 | Face to face interview and questionnaire | 8 |
| Steinmaus C.M. et al., 2013 [36] | Case-control | M/W (601/271) Cases: 306 Controls: 640 | Chile | 30–39; 40–49; 50–59; 60–69; 70+ | 1958–1970 | Standardized questionnaire | 8 |
| Hsu L. et al., 2013 [31] | Cohort | M/W (1231/1216) | Taiwan | 30–49; 50–59; 60–69; ≥70 | 1985–1989 | Interviewed at homewith a structured questionnaire | 5 |
| Ferreccio C. et al., 2013 [37] | Case-control | M/W (646/300) Cases: 306 Controls: 640 | Chile | 30–39; 40–49; 50–59; 60–69; 70+ | 2007–2010 | Standardized study questionnaire and government agencies, research studies | 6 |
| Dauphiné D.C. et al., 2013 [38] | Case-control | M/W (237/318) Cases: 196 Controls: 359 | Nevada and California (USA) | Case: mean 70.2 ± 10 Control: mean 69.0 ± 8.6 | 2002–2005 | Standardized study questionnaire by telephone | 8 |
| Chen C. et al., 2010 [32] | Cohort | M/W (3481/3407) | Taiwan | ≤50; 50–54.9; 55–59.9; ≥60 | 1991–2002 | Home interview with a questionnaire | 7 |
| Paul S. et al., 2013 [41] | Cross-sectional | 2005–2006 88 M, unexposed 83 W, unexposed 94 M, exposed 95, W exposed 2010–2011 87 M, unexposed 83 W, unexposed 85 M, exposed 91 W, exposed | India | 2005–2006 34.76 ± 9.52 unexposed 34.62 ± 12.93 exposed 2010–2011 39.05 ± 9.08 unexposed 38.65 ± 13.09 exposed | 2005–2010 | Expert physician screening | 4 |
| Marano K.M. et al., 2012 [43] | Review of epidemiological data | Cigarette smokers, n = 991 Smokeless tobacco (SLT) consumers, n = 90 Non-consumers of tobacco n = 3385 | USA | ≥20 | 2003–2008 | Database (NHANES: National Health and Nutrition Examination Survey) | 2 |
| Wadhwa S.K. et al., 2011 [39] | Case–control | Exposed subjects 98 M, referents without cancer 52 M, with lung cancer Non-exposed subjects 95 M, referents without cancer 55 M, with lung cancer | Pakistan | median 47 (range 35–65) | 2007–2009 | Face to face interview and medical database | 4 |
| Olsson A.C. et al., 2011 [33] | Multicenter case-control | M/W (4054/1260) Cases: 2624 Controls:2690 M/W exposed (91/5) Exposed cases: 60 Exposed controls:36 | Czech Republic, Hungary, Poland, Romania, Russia and Slovakia | <45; 45 to 49; 50 to 54; 55 to 59; 60 to 64; 65 to 69; 70 to 74; 75+ | 1998–2002 | Face to face interview and questionnaire | 7 |
| ’t Mannetje A. et al., 2014 [34] | Multicenter case-control | M/W (4492/1464) Cases: 2852 Controls: 3104 Exposed cases: 70 Exposed controls:43 | Romania, Hungary, Poland, Russia, Slovakia, Czech Republic and UK | 25–45; 45–55; 55–65; 65 or older | 1998–2003 | Face to face interview and questionnaire | 7 |
| Melak D. et al., 2014 [40] | Case-control | Cases: 94 Controls: 347 | Chile | >25 | 2007–2010 | Face to face interview, questionnaire and medical database | 8 |
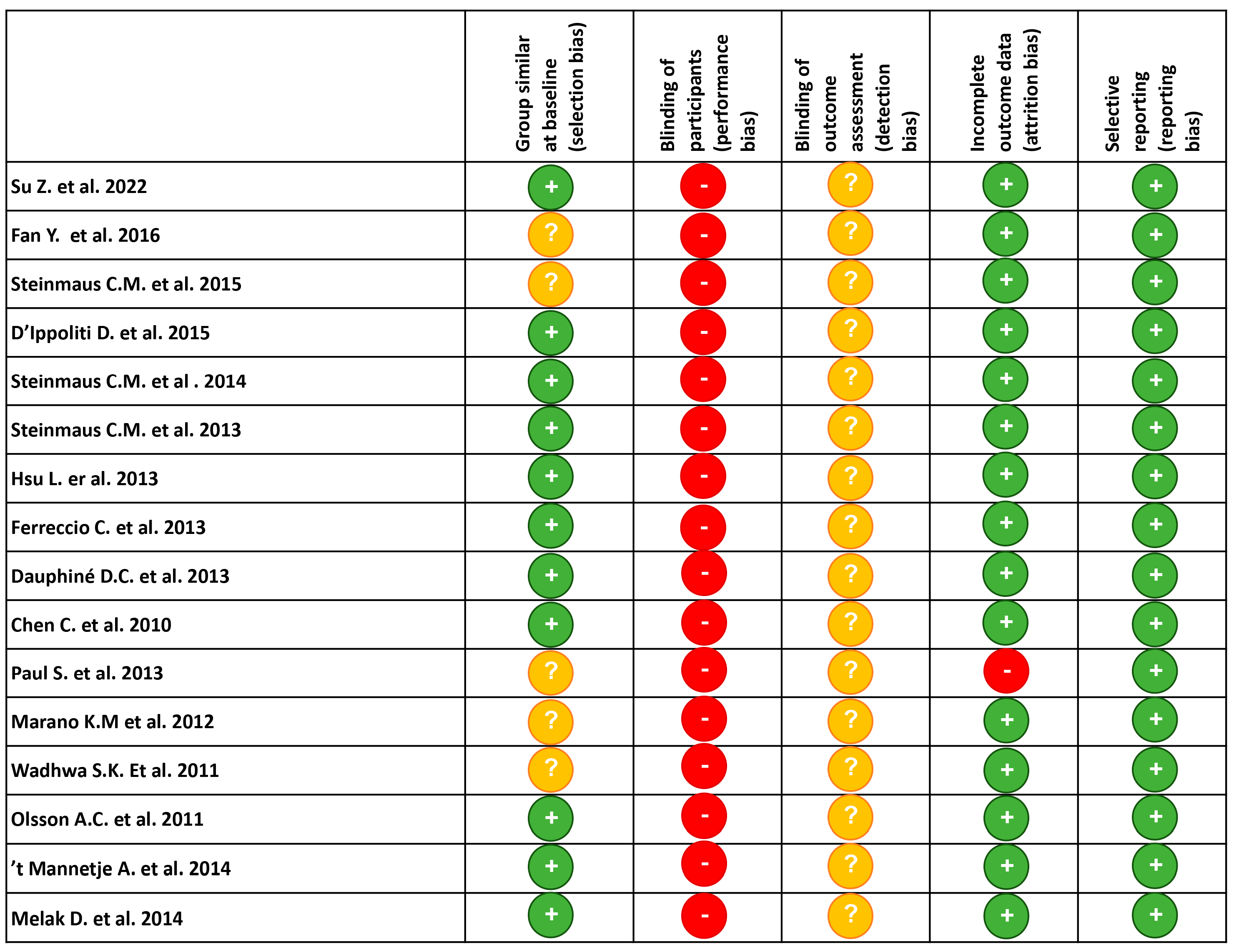
3.3. Risk of Bias in Included Studies
3.4. Arsenic–Smoking Interaction
3.5. Outcome Measures
4. Discussion
4.1. Summary of Findings
- Five studies have identified a synergism between arsenic dose and cigarette smoking in the induction of lung carcinoma [30,32,36,37,39]. In particular, Su et al. [30] found a sub-multiplicative interaction and Ferreccio et al. [37] referred to a “greater than additive effects”, while the others defined a synergistic interaction.
- Synergism with smoking significantly changed the lung cancer risk when exposed to higher versus lower concentrations of arsenic.
- Some studies did not have complete quantitative characterization of exposure [34]. Conversely, Ferreccio et al. [37] asserted that “his study took place in an area with a history of high concentrations of arsenic in drinking water and good data on past exposure”. Moreover, detailed tobacco consumption was sometimes missing; for example, D’ippoliti et al. [42] reported indirect data on cigarette sales in different municipalities as an indicator of smoking status.
4.2. Strengths and Limitations of This Systematic Review
4.3. Interaction between Arsenic and Tobacco Smoke and Determination of Estimate Effect Values
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuivenhoven, M.; Mason, K. StatPearls. In Arsenic Toxicity; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Howard, G. Arsenic, Drinking-water and Health Risk Substitution in Arsenic Mitigation: A Discussion Paper. Available online: http://www.who.int/mediacentre/factsheets/fs372/en/ (accessed on 2 December 2022).
- Mandal, B.K.; Suzuki, K.T. Arsenic round the world: A review. Talanta 2002, 58, 201–235. [Google Scholar] [CrossRef] [PubMed]
- IARC monographs on the evaluation of carcinogenic risks to humans. Arsenic, metals, fibres and dusts. In A Review of Human Carcinogens; International Agency for Research on Cancer: Lyon, France, 2012. [Google Scholar]
- EUR-Lex. Directive. (EU) 2019/983 of the European Parliament and of the Council of 5 June 2019 Amending Directive 2004/37/EC on the Protection of Workers from the Risks Related to Exposure to Carcinogens or Mutagens at Work; European Union: Luxembourg, 2019. [Google Scholar]
- NIOSH. Arsine. Available online: https://www.cdc.gov/niosh/idlh/7784421.html#print (accessed on 12 February 2022).
- United States Environmental Protection Agency. Technical Fact Sheet: Final Rule for Arsenic in Drinking Water; EPA 815-F-00-016; United States Environmental Protection Agency: Washington, DC, USA, 2001. [Google Scholar]
- Monteiro De Oliveira, E.C.; Caixeta, E.S.; Santos, V.S.V.; Pereira, B.B. Arsenic exposure from groundwater: Environmental contamination, human health effects, and sustainable solutions. J. Toxicol. Environ. Health B Crit. Rev. 2021, 24, 119–135. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.S.; Chatterjee, D.; Das, N.; Giri, A.K. Substantial Evidences Indicate That Inorganic Arsenic Is a Genotoxic Carcinogen: A Review. Toxicol. Res. 2018, 34, 311–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, H.F.; Ho, S.C.; Yang, C.Y. Lung cancer mortality reduction after installation of tap-water supply system in an arseniasis-endemic area in Southwestern Taiwan. Lung Cancer 2004, 46, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Eisler, R. Arsenic hazards to humans, plants, and animals from gold mining. Rev. Environ. Contam. Toxicol. 2004, 180, 133–165. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.R.; Atkin, P.; Holroyd, C.; Lutman, E.; Batlle, J.V.; Wakeford, R.; Walker, P. Lung cancer mortality at a UK tin smelter. Occup. Med. 2007, 57, 238–245. [Google Scholar] [CrossRef] [Green Version]
- Molin, M.; Ulven, S.M.; Meltzer, H.M.; Alexander, J. Arsenic in the human food chain, biotransformation and toxicology—Review focusing on seafood arsenic. J. Trace Elem. Med. Biol. 2015, 31, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Bagryantseva, O.V.; Khotimchenko, S.A. Risks associated with the consumption of inorganic and organic arsenic. Vopr Pitan 2021, 90, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.S.; Beyer, L.A.; Zu, K. Considerations in deriving quantitative cancer criteria for inorganic arsenic exposure via inhalation. Environ. Int. 2015, 74, 258–273. [Google Scholar] [CrossRef]
- Bozack, A.K.; Saxena, R.; Gamble, M.V. Nutritional Influences on One-Carbon Metabolism: Effects on Arsenic Methylation and Toxicity. Annu. Rev. Nutr. 2018, 38, 401–429. [Google Scholar] [CrossRef]
- Chen, C.L.; Hsu, L.I.; Chiou, H.Y.; Hsueh, Y.M.; Chen, S.Y.; Wu, M.M.; Chen, C.J.; Group, B.D.S. Ingested arsenic, cigarette smoking, and lung cancer risk: A follow-up study in arseniasis-endemic areas in Taiwan. JAMA 2004, 292, 2984–2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC monographs on the evaluation of carcinogenic risks to humans. Personal habits and indoor combustions. In A Review of Human Carcinogens; International Agency for Research on Cancer: Lyon, France, 2012. [Google Scholar]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertz-Picciotto, I.; Smith, A.H.; Holtzman, D.; Lipsett, M.; Alexeeff, G. Synergism between occupational arsenic exposure and smoking in the induction of lung cancer. Epidemiology 1992, 3, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.A. Could removing arsenic from tobacco smoke significantly reduce smoker risks of lung cancer? Risk Anal. 2009, 29, 3–17. [Google Scholar] [CrossRef]
- Wei, S.; Zhang, H.; Tao, S. A review of arsenic exposure and lung cancer. Toxicol. Res. 2019, 8, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Alberg, A.J.; Shopland, D.R.; Cummings, K.M. The 2014 Surgeon General’s report: Commemorating the 50th Anniversary of the 1964 Report of the Advisory Committee to the US Surgeon General and updating the evidence on the health consequences of cigarette smoking. Am. J. Epidemiol. 2014, 179, 403–412. [Google Scholar] [CrossRef] [Green Version]
- Folesani, G.; Galetti, M.; Ranzieri, S.; Petronini, P.G.; La Monica, S.; Corradi, M.; Cavallo, D. Interaction between occupational radon exposure and tobacco smoke: A systematic review. Expert Rev. Respir. Med. 2022, 16, 787–800. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 22 October 2022).
- Montazeri, Z.; Nyiraneza, C.; El-Katerji, H.; Little, J. Waterpipe smoking and cancer: Systematic review and meta-analysis. Tob. Control 2017, 26, 92–97. [Google Scholar] [CrossRef]
- Steinmaus, C.; Castriota, F.; Ferreccio, C.; Smith, A.H.; Yuan, Y.; Liaw, J.; Acevedo, J.; Pérez, L.; Meza, R.; Calcagno, S.; et al. Obesity and excess weight in early adulthood and high risks of arsenic-related cancer in later life. Environ. Res. 2015, 142, 594–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Z.; Wei, M.N.; Jia, X.H.; Fan, Y.G.; Zhao, F.H.; Zhou, Q.H.; Taylor, P.R.; Qiao, Y.L. Arsenic, tobacco use, and lung cancer: An occupational cohort with 27 follow-up years. Environ. Res. 2022, 206, 112611. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.I.; Chen, G.S.; Lee, C.H.; Yang, T.Y.; Chen, Y.H.; Wang, Y.H.; Hsueh, Y.M.; Chiou, H.Y.; Wu, M.M.; Chen, C.J. Use of arsenic-induced palmoplantar hyperkeratosis and skin cancers to predict risk of subsequent internal malignancy. Am. J. Epidemiol. 2013, 177, 202–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.L.; Chiou, H.Y.; Hsu, L.I.; Hsueh, Y.M.; Wu, M.M.; Chen, C.J. Ingested arsenic, characteristics of well water consumption and risk of different histological types of lung cancer in northeastern Taiwan. Environ. Res. 2010, 110, 455–462. [Google Scholar] [CrossRef]
- Olsson, A.C.; Gustavsson, P.; Zaridze, D.; Mukeriya, A.; Szeszenia-Dabrowska, N.; Rudnai, P.; Lissowska, J.; Fabianova, E.; Mates, D.; Bencko, V.; et al. Lung cancer risk attributable to occupational exposures in a multicenter case-control study in Central and Eastern Europe. J. Occup. Environ. Med. 2011, 53, 1262–1267. [Google Scholar] [CrossRef]
- ‘t Mannetje, A.; Bencko, V.; Brennan, P.; Zaridze, D.; Szeszenia-Dabrowska, N.; Rudnai, P.; Lissowska, J.; Fabiánová, E.; Cassidy, A.; Mates, D.; et al. Occupational exposure to metal compounds and lung cancer. Results from a multi-center case-control study in Central/Eastern Europe and UK. Cancer Causes Control 2011, 22, 1669–1680. [Google Scholar] [CrossRef]
- Steinmaus, C.; Ferreccio, C.; Yuan, Y.; Acevedo, J.; González, F.; Perez, L.; Cortés, S.; Balmes, J.R.; Liaw, J.; Smith, A.H. Elevated lung cancer in younger adults and low concentrations of arsenic in water. Am. J. Epidemiol. 2014, 180, 1082–1087. [Google Scholar] [CrossRef] [Green Version]
- Steinmaus, C.M.; Ferreccio, C.; Romo, J.A.; Yuan, Y.; Cortes, S.; Marshall, G.; Moore, L.E.; Balmes, J.R.; Liaw, J.; Golden, T.; et al. Drinking water arsenic in northern chile: High cancer risks 40 years after exposure cessation. Cancer Epidemiol. Biomark. Prev. 2013, 22, 623–630. [Google Scholar] [CrossRef] [Green Version]
- Ferreccio, C.; Yuan, Y.; Calle, J.; Benítez, H.; Parra, R.L.; Acevedo, J.; Smith, A.H.; Liaw, J.; Steinmaus, C. Arsenic, tobacco smoke, and occupation: Associations of multiple agents with lung and bladder cancer. Epidemiology 2013, 24, 898–905. [Google Scholar] [CrossRef]
- Dauphiné, D.C.; Smith, A.H.; Yuan, Y.; Balmes, J.R.; Bates, M.N.; Steinmaus, C. Case-control study of arsenic in drinking water and lung cancer in California and Nevada. Int. J. Environ. Res. Public Health 2013, 10, 3310–3324. [Google Scholar] [CrossRef] [Green Version]
- Wadhwa, S.K.; Kazi, T.G.; Kolachi, N.F.; Afridi, H.I.; Khan, S.; Chandio, A.A.; Shah, A.Q.; Kandhro, G.A.; Nasreen, S. Case-control study of male cancer patients exposed to arsenic-contaminated drinking water and tobacco smoke with relation to non-exposed cancer patients. Hum. Exp. Toxicol. 2011, 30, 2013–2022. [Google Scholar] [CrossRef]
- Melak, D.; Ferreccio, C.; Kalman, D.; Parra, R.; Acevedo, J.; Pérez, L.; Cortés, S.; Smith, A.H.; Yuan, Y.; Liaw, J.; et al. Arsenic methylation and lung and bladder cancer in a case-control study in northern Chile. Toxicol. Appl. Pharmacol. 2014, 274, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Paul, S.; Das, N.; Bhattacharjee, P.; Banerjee, M.; Das, J.K.; Sarma, N.; Sarkar, A.; Bandyopadhyay, A.K.; Sau, T.J.; Basu, S.; et al. Arsenic-induced toxicity and carcinogenicity: A two-wave cross-sectional study in arsenicosis individuals in West Bengal, India. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 156–162. [Google Scholar] [CrossRef] [PubMed]
- D’Ippoliti, D.; Santelli, E.; De Sario, M.; Scortichini, M.; Davoli, M.; Michelozzi, P. Arsenic in Drinking Water and Mortality for Cancer and Chronic Diseases in Central Italy, 1990–2010. PLoS ONE 2015, 10, e0138182. [Google Scholar] [CrossRef] [PubMed]
- Marano, K.M.; Naufal, Z.S.; Kathman, S.J.; Bodnar, J.A.; Borgerding, M.F.; Wilson, C.L. Arsenic exposure and tobacco consumption: Biomarkers and risk assessment. Regul. Toxicol. Pharmacol. 2012, 64, 225–232. [Google Scholar] [CrossRef]
- Fan, Y.; Jiang, Y.; Hu, P.; Chang, R.; Yao, S.; Wang, B.; Li, X.; Zhou, Q.; Qiao, Y. Modification of association between prior lung disease and lung cancer by inhaled arsenic: A prospective occupational-based cohort study in Yunnan, China. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 464–470. [Google Scholar] [CrossRef]
- Navasumrit, P.; Chaisatra, K.; Promvijit, J.; Parnlob, V.; Waraprasit, S.; Chompoobut, C.; Binh, T.T.; Hai, D.N.; Bao, N.D.; Hai, N.K.; et al. Exposure to arsenic in utero is associated with various types of DNA damage and micronuclei in newborns: A birth cohort study. Environ. Health 2019, 18, 51. [Google Scholar] [CrossRef] [Green Version]
- Roh, T.; Steinmaus, C.; Marshall, G.; Ferreccio, C.; Liaw, J.; Smith, A.H. Age at Exposure to Arsenic in Water and Mortality 30–40 Years After Exposure Cessation. Am. J. Epidemiol. 2018, 187, 2297–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, T.; Zhang, H.; Chen, B.; Tao, S. Association between lung cancer risk and inorganic arsenic concentration in drinking water: A dose-response meta-analysis. Toxicol. Res. 2018, 7, 1257–1266. [Google Scholar] [CrossRef] [Green Version]
- Lamm, S.H.; Boroje, I.J.; Ferdosi, H.; Ahn, J. A review of low-dose arsenic risks and human cancers. Toxicology 2021, 456, 152768. [Google Scholar] [CrossRef]
- Gianicolo, E.A.L.; Mangia, C.; Cervino, M.; Bruni, A.; Portaluri, M.; Comba, P.; Pirastu, R.; Biggeri, A.; Vigotti, M.; Blettner, M. Long-term effect of arsenic exposure: Results from an occupational cohort study. Am. J. Ind. Med. 2019, 62, 145–155. [Google Scholar] [CrossRef]
- Keil, A.P.; Richardson, D.B. Reassessing the Link between Airborne Arsenic Exposure among Anaconda Copper Smelter Workers and Multiple Causes of Death Using the Parametric g-Formula. Environ. Health Perspect. 2017, 125, 608–614. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, M.G.; McDonald, J.C.; Cherry, N.M. Lung cancer and exposure to arsenic in rural Bangladesh. Occup. Environ. Med. 2008, 65, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Ferreccio, C.; González, C.; Milosavjlevic, V.; Marshall, G.; Sancha, A.M.; Smith, A.H. Lung cancer and arsenic concentrations in drinking water in Chile. Epidemiology 2000, 11, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Frost, G. The latency period of mesothelioma among a cohort of British asbestos workers (1978–2005). Br. J. Cancer 2013, 109, 1965–1973. [Google Scholar] [CrossRef] [Green Version]
- Marshall, G.; Ferreccio, C.; Yuan, Y.; Bates, M.N.; Steinmaus, C.; Selvin, S.; Liaw, J.; Smith, A.H. Fifty-year study of lung and bladder cancer mortality in Chile related to arsenic in drinking water. J. Natl. Cancer Inst. 2007, 99, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinmaus, C.; Balmes, J.R. Government laboratory worker with lung cancer: Comparing risks from beryllium, asbestos, and tobacco smoke. Environ. Health Perspect. 2000, 108, 1003–1006. [Google Scholar] [CrossRef]
- Gibb, H.; Haver, C.; Gaylor, D.; Ramasamy, S.; Lee, J.S.; Lobdell, D.; Wade, T.; Chen, C.; White, P.; Sams, R. Utility of recent studies to assess the National Research Council 2001 estimates of cancer risk from ingested arsenic. Environ. Health Perspect. 2011, 119, 284–290. [Google Scholar] [CrossRef] [Green Version]


| Author (Year) | Type of Exposure | Smoking Status | Estimate Effect Type | Estimate Effect Value | Type of Interaction | ||
|---|---|---|---|---|---|---|---|
| Su Z. et al., 2022 [30] | Occupational: tin miners (Chinese Yunnan tin corporation) | Never smoker Current smoker | ERR | Mean cumulative arsenic exposure: 83.6 mg/m3 | Sub-multiplicative | ||
| Cumulative arseinc exposure < 3 mg/m3 * | |||||||
| 0.0033 (95% CI: 0.0014–0.0045) | |||||||
| Cumulative arseinc exposure ≥ 3 mg/m3 * | |||||||
| 0.0056 (95% CI: 0.0035–0.0073) | |||||||
| * Adjusted for smoking | |||||||
| Fan Y. et al., 2016 [44] | Occupational: tin miners | Never smokers Former smoker Current smoker | HR | Cumulative arsenic exposure between 0 and 17,435 mg/m3 | Not reported | ||
| 1.00 | Never smokers * | ||||||
| 1.31 (95% CI: 0.77–2.24) | Former smokers * | ||||||
| 1.53 (95% CI: 0.95–2.44) | Current smokers * | ||||||
| * adjusted for all prior lung diseases and different carcinogenic compounds exposure | |||||||
| Steinmaus C.M. et al., 2015 [29] | Non-occupational: arsenic drinking water | Never smokers Ever smokers Heavier smokers (smoking > 20 cigs/day) | OR | LOW BMI, Unadjusted | Not reported | ||
| 1.00 | [<100 μg/L] | ||||||
| 1.24 (95% CI: 0.84–1.82) | [100–800 μg/L] | ||||||
| 2.47 (95% CI: 1.75–3.49) | [>800 μg/L] | ||||||
| LOW BMI, Adjusted * | |||||||
| 1.00 | [<100 μg/L] | ||||||
| 1.17 (95% CI: 0.79–1.73) | [100–800 μg/L] | ||||||
| 2.31 (95% CI: 1.63–3.29) | [>800 μg/L] | ||||||
| HIGH BMI, Unadjusted | |||||||
| 1.00 | [<100 μg/L] | ||||||
| 1.52 (95% CI: 0.56–4.15) | [100–800 μg/L] | ||||||
| 5.83 (95% CI: 1.73–19.64) | [>800 μg/L] | ||||||
| HIGH BMI, Adjusted * | |||||||
| 1.00 | [<100 μg/L] | ||||||
| 1.48 (95% CI: 0.53–4.14) | [100–800 μg/L] | ||||||
| 6.98 (95% CI: 1.84–26.56) | [>800 μg/L] | ||||||
| * Adjusted for age, sex and smoking | |||||||
| D’Ippoliti D. et al., 2015 [42] | Non-occupational: arsenic drinking water | Not directly determined (used tobacco sales from municipal level assumption) | HR | Arsenic (10–20 μg/L) * | Not reported (dose response relationship) | ||
| 1.27 (95% CI: 1.18–1.38) | Natural causes, males | ||||||
| 1.47 (95% CI: 1.17–1.86) | Tracheas, bronchus and lung, males | ||||||
| 1.14 (95% CI: 1.05–1.24) | Natural causes, females | ||||||
| 1.80 (95% CI: 1.23–2.66) | Tracheas, bronchus and lung, females | ||||||
| Cumulative Arsenic dose (CAI; 204.9–804.0 μg) * | |||||||
| 1.59 (95% CI: 1.45–1.74) | Natural causes, males | ||||||
| 2.03 (95% CI: 1.48–2.79) | Tracheas, bronchus and lung, males | ||||||
| 1.45 (95% CI: 1.32–1.58) | Natural causes, females | ||||||
| 1.66 (95% CI: 0.93–2.95) | Tracheas, bronchus and lung, females | ||||||
| * Adjusted for age, calendar period, socio economic level, occupation in the ceramic industry, smoking sales and radon exposure | |||||||
| Steinmaus C.M. et al., 2014 [35] | Non-occupational: arsenic drinking water | Never smokers Ever smokers Smoker > 10 cigs/day | OR | Unadjusted | Not reported | ||
| 1.00 | [<10 μg/L] | ||||||
| 1.46 (90% CI: 0.88–2.43) | [10–59.9 μg/L] | ||||||
| 1.90 (90% CI: 1.16–3.13) | [>59.9 μg/L] | ||||||
| Adjusted * | |||||||
| 1.00 | [<10 μg/L] | ||||||
| 1.43 (90% CI: 0.82–2.52) | [10–59.9 μg/L] | ||||||
| 2.01 (90% CI: 1.14–3.52) | [>59.9 μg/L] | ||||||
| * Adjusted for age, sex and smoking behavior | |||||||
| Steinmaus C.M. et al., 2013 [36] | Non-occupational: arsenic drinking water | Never smoker Ever smoker | OR | Adjusted for smoking | Synergistic | ||
| 1.00 | [<11 μg/L] | ||||||
| 1.27 (95% CI: 0.81–1.98) | [11–90 μg/L] | ||||||
| 2.00 (95% CI: 1.24–3.24) | [91–335 μg/L] | ||||||
| 4.32 (95% CI: 2.60–7.17) | [>335 μg/L] | ||||||
| Hsu L. et al., 2013 [31] | Non-occupational: arsenic drinking water | Non-smokers Smokers | HR | Non-smokers * | Not reported | ||
| 1.00 | Group 1 (no arsenical skin lesions) | ||||||
| 0.24 (95% CI: 0.03–1.79) | Group 2 (hyperpigmentation only) | ||||||
| 0.58 (95% CI: 0.08–4.26) | Group 3 (hyperkeratosis with or without hyperpigmentation) | ||||||
| 3.24 (95% CI: 1.54–6.80) | Group 4 (skin cancer without hyperkeratosis) | ||||||
| 2.22 (95% CI: 0.76–6.48) | Group 5 (skin cancer and hyperkeratosis) | ||||||
| Smokers * | |||||||
| 2.20 (95% CI: 1.05–4.63) | Group 1 (no arsenical skin lesions) | ||||||
| 1.69 (95% CI: 0.46–6.20) | Group 2 (hyperpigmentation only) | ||||||
| 12.34 (95% CI: 4.79–31.75) | Group 3 (hyperkeratosis with or without hyperpigmentation) | ||||||
| 12.04 (95% CI: 5.12–28.31) | Group 4 (skin cancer without hyperkeratosis) | ||||||
| 23.54 (95% CI: 9.39–59.00) | Group 5 (skin cancer and hyperkeratosis) | ||||||
| * Hazard ratios were adjusted for age, sex, body mass index, educational level and cumulative arsenic exposure | |||||||
| Ferreccio C. et al., 2013 [37] | Non-occupational: arsenic drinking water | Never smokers Ever smoker Heavier smokers (smoking > 10 cigs/day) | OR | Never smoker * | Greater than additive | ||
| 1.00 | [0–34 μg/L] | ||||||
| 0.87 (95% CI: 0.42–1.81) | [35–260 μg/L] | ||||||
| 1.67 (95% CI: 0.78–3.56) | [>260 μg/L] | ||||||
| Smoked > 10 cigs/day * | |||||||
| 4.36 (95% CI: 2.12–8.99) | [0–34 μg/L] | ||||||
| 6.94 (95% CI: 3.48–13.83) | [35–260 μg/L] | ||||||
| 20.80 (95% CI: 9.03–47.91) | [>260 μg/L] | ||||||
| * Adjusted for age, sex, socioeconomic status, and second-hand tobacco smoke exposure. | |||||||
| Dauphiné D.C. et al., 2013 [38] | Non-occupational: arsenic drinking water | Never smoker Ever smoker | OR | All subjects | Not reported | ||
| 1.00 | [≤10 μg/L] | ||||||
| 0.84 (95% CI:0.40–1.79) | [11–84 μg/L] | ||||||
| 1.39 (95% CI: 0.55–3.53) | [>85 µg/L] | ||||||
| Smokers | |||||||
| 1.00 | [≤10 μg/L] | ||||||
| 0.66 (95% CI:0.30–1.44) | [11–84 μg/L] | ||||||
| 1.61 (95% CI: 0.59–4.38) | [>85 µg/L] | ||||||
| Chen C. e al., 2010 [32] | Non-occupational: arsenic drinking water | Never smokers Current smokers (<25 cigs/day) Current smokers (≥25 cigs/day) | RR | Never smokers | Synergistic for squamous and small cell lung cancer | ||
| 1.00 | [<10 µg/L] | ||||||
| 1.22 (95% CI: 0.64–2.32) | [10–99.9 µg/L] | ||||||
| 1.32 (95% CI: 0.64–2.74) | [≥100 µg/L] | ||||||
| Current smokers (<25 cigs/day) | |||||||
| 2.14 (95% CI: 0.79–5.79) | [<10 µg/L] | ||||||
| 1.52 (95% CI: 0.56–4.15) | [10–99.9 µg/L] | ||||||
| 5.30 (95% CI: 2.19–12.8) | [≥100 µg/L] | ||||||
| Current smokers (≥25 cigs/day) | |||||||
| 4.08 (95% CI: 1.83–9.10) | [<10 µg/L] | ||||||
| 4.19 (95% CI: 1.92–9.14) | [10–99.9 µg/L] | ||||||
| 8.17 (95% CI: 3.74–17.9) | [≥100 µg/L] | ||||||
| Paul S. et al., 2013 [41] | Non-occupational: arsenic drinking water | 2005–2006 63 M, unexposed 34 W, unexposed 57 M, exposed 31 W, exposed 2010–2011 69 M, unexposed 39 W, unexposed 53 M, exposed 33 W, exposed | Lung cancer death (number) | 2010–2011 * | Not reported | ||
| 1 individual among the unexposed died due to natural cause | |||||||
| 3 males, exposed | |||||||
| 0 female, exposed | |||||||
| * tobacco consumption were matched between unexposed and exposed subjects | |||||||
| Marano K.M et al., 2012 [43] | Occupational and non-occupational | Cigarette smokers Smokeless tobacco (SLT) consumers Non-consumers of tobacco | Geometric mean of urine arsenic (μg/g creatinine) | 39.1 for lung cancer Vs | Not reported | ||
| 7.98 (95% CI: 7.08–9.00) | Cigarette smokers * | ||||||
| 6.14 (95% CI: 4.86–7.74) | SLT consumers * | ||||||
| 9.56 (95% CI: 8.92–10.27) | Non-consumers of tobacco * | ||||||
| * without lung cancer | |||||||
| Wadhwa S.K. et al., 2011 [39] | Non-occupational: water, food and fish; locally made cigarette | 100% smokers | OR | Arsenic concentrations 3–15 fold higher than the permissible level (< 10 µg/L) 3.05 (95% CI: 1.26–7.36) (for lung cancer mortality among exposed lung cancer patients as compared to non-exposed lung cancer patients) | Synergistic | ||
| Olsson A.C. et al., 2011 [33] | Occupational: different kinds of industries, e.g., wood work and painting | Never smoker Former smoker Current smoker | OR | Arsenic < 50% TLV (2011) = low; 50–150% TLV (2011) = medium; >150% TLV (2011) = high Adjusted for smoking (tobacco pack years) Men: 1.92 (95% CI: 1.15–3.20) Women: 1.05 (95% CI: 0.11–9.89) | Not reported | ||
| ’t Mannetje A. et al., 2014 [34] | Occupational: agriculture, miners and different kinds of industries | Never smokers Ex-smokers Ever smokers | OR | Arsenic concentration values not reported (low, medium and high exposure). Adjusted * 1.65 (95% CI: 1.05–2.58) * adjusted for age, center, sex, tobacco consumption and for other occupational exposures including metals | Not reported | ||
| Melak D. et al., 2014 [40] | Non-occupational: arsenic drinking water | Never smokers Smokers | OR | Water arsenic < 200 µg/L | Not reported | ||
| Crude | Adjusted * | ||||||
| 1.00 | 1.00 | %MMA < 12.5% | |||||
| 2.65 (95% CI: 1.18–5.94) | 2.48 (95% CI: 1.08–5.68) | %MMA ≥ 12.5% | |||||
| Water arsenic ≥ 200 µg/L | |||||||
| Crude | Adjusted * | ||||||
| 3.05 (95% CI: 1.56–5.95) | 3.16 (95% CI: 1.59–6.32) | %MMA < 12.5% | |||||
| 6.94 (95% CI:3.39–14.22) | 6.81 (95% CI:3.24–14.31) | %MMA ≥ 12.5% | |||||
| * Odds ratios adjusted for age, gender and smoking | |||||||
| %MMA = % monomethylarsenic in urine; the cut-off value of 12.5% divided the upper from the two lower tertiles | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Folesani, G.; Galetti, M.; Petronini, P.G.; Mozzoni, P.; La Monica, S.; Cavallo, D.; Corradi, M. Interaction between Occupational and Non-Occupational Arsenic Exposure and Tobacco Smoke on Lung Cancerogenesis: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4167. https://doi.org/10.3390/ijerph20054167
Folesani G, Galetti M, Petronini PG, Mozzoni P, La Monica S, Cavallo D, Corradi M. Interaction between Occupational and Non-Occupational Arsenic Exposure and Tobacco Smoke on Lung Cancerogenesis: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(5):4167. https://doi.org/10.3390/ijerph20054167
Chicago/Turabian StyleFolesani, Giuseppina, Maricla Galetti, Pier Giorgio Petronini, Paola Mozzoni, Silvia La Monica, Delia Cavallo, and Massimo Corradi. 2023. "Interaction between Occupational and Non-Occupational Arsenic Exposure and Tobacco Smoke on Lung Cancerogenesis: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 5: 4167. https://doi.org/10.3390/ijerph20054167
APA StyleFolesani, G., Galetti, M., Petronini, P. G., Mozzoni, P., La Monica, S., Cavallo, D., & Corradi, M. (2023). Interaction between Occupational and Non-Occupational Arsenic Exposure and Tobacco Smoke on Lung Cancerogenesis: A Systematic Review. International Journal of Environmental Research and Public Health, 20(5), 4167. https://doi.org/10.3390/ijerph20054167