
Piloting a Home Visual Support Intervention with Families of Autistic Children and Children with Related Needs Aged 0–12


Abstract
:1. Introduction
2. Methods
2.1. Research Question
2.2. Participants and Procedures
2.3. Visual Supports Intervention Model for the Current Study
- Families are equal partners;
- Support should be provided to enable families to make visual supports resources independently;
- Assessment and planning processes are multi-disciplinary, including health and education staff, dynamic, parent focussed, and developmentally and functionally relevant;
- Support is ‘time friendly’ with long-term access to visual supports for professionals and parents;
- Family friendly information and signposting is provided;
- Flexibility of access to professional support is provided to include intensive start-up options, drop-in sessions, peer support, home support, parent training, coaching, and modelling;
- Professional training and awareness raising around visual supports are included;
- There is consistency across settings with ‘symbol sets’ and templates of commonly used resources.
2.4. Staff Providing the Intervention and Intervention Delivery
- Prior to Visit 1: Parent completed the pre-questionnaire and assessments. These were subsequently collected on Visit 1. Support to complete these was offered;
- Visit 1: Parent assessment was completed to identify priorities relevant to child’s stage and family targets. Between visits, staff collected visual supports resource pack for the family and prepared ‘how to’ guides. Staff could make individualised resources if required. A local ‘Boardmaker in Libraries’ programme [15] was also available to families to attend ‘drop-ins’ or to make their own resources. Families were made aware of this, although use and experience of this external maintenance mechanism was not evaluated in this study;
- Visit 2: The professional brought agreed visual supports and provided guidance on using them (written guides, modelling, coaching, and verbal guidance). Families had the opportunity to ask questions, and in partnership, adjustments were made to the plan. If necessary, further assessment of need could be completed, and more visual supports identified;
- Visits 3–5: Parents used visual supports and provided feedback. Staff offered further consultation and brought additional visual supports if needed. On completion, staff provided a summary of visual supports implemented and guidance shared, which the family can share with school or use as a reminder;
- After the final visit: Parents were given the post questionnaires/assessments at the end of the final visit. These were collected by a team member at a suitable time within a week of the last visit.
2.5. Measures
2.5.1. Outcomes Model
2.5.2. Parent Assessment Tool
2.5.3. The Quality of Life in Autism Questionnaire (QoLA)
2.5.4. Parent Questionnaire
2.6. Data Analysis
2.7. Qualitative Data Collection
2.8. Qualitative Data Analysis
3. Results
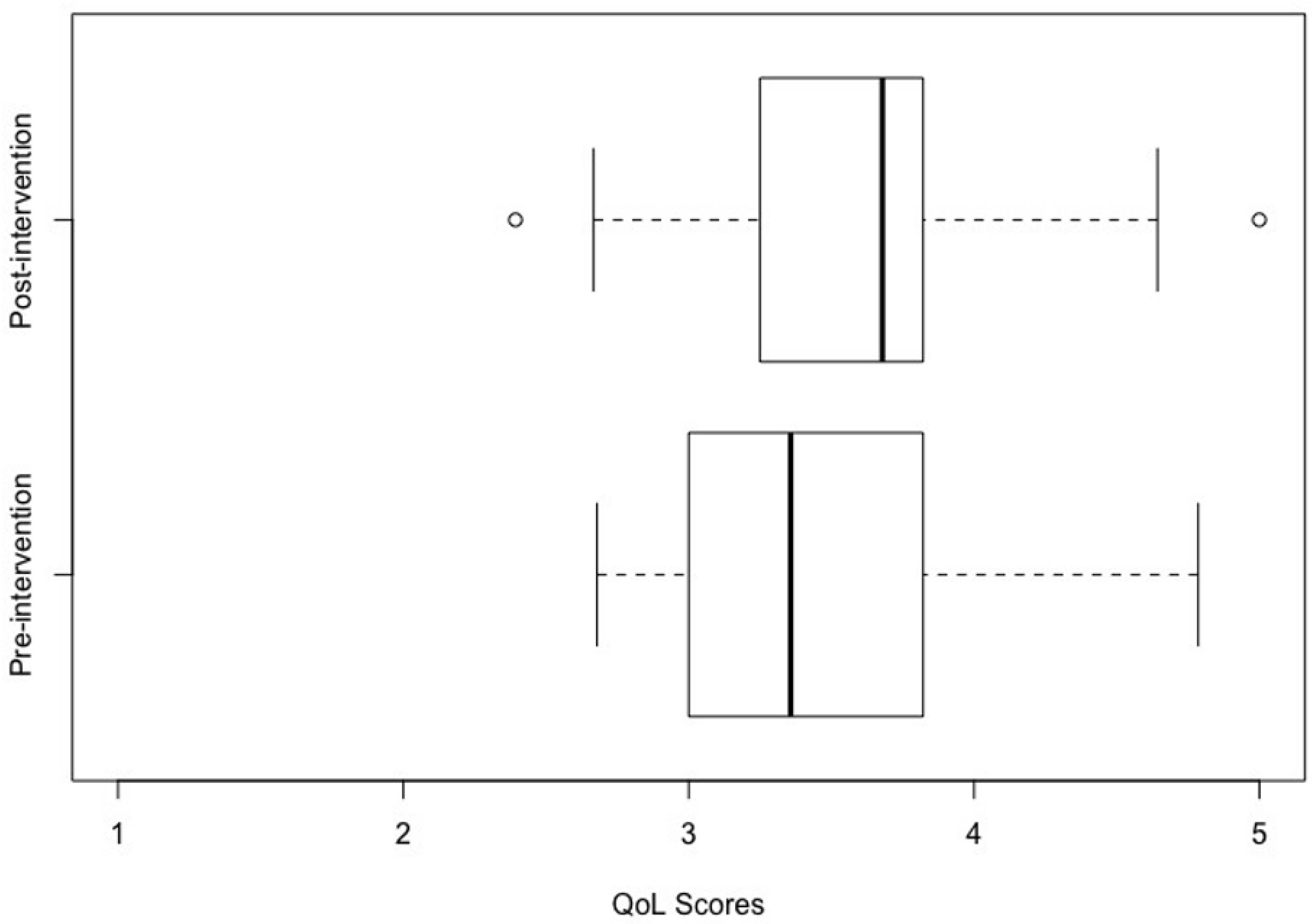
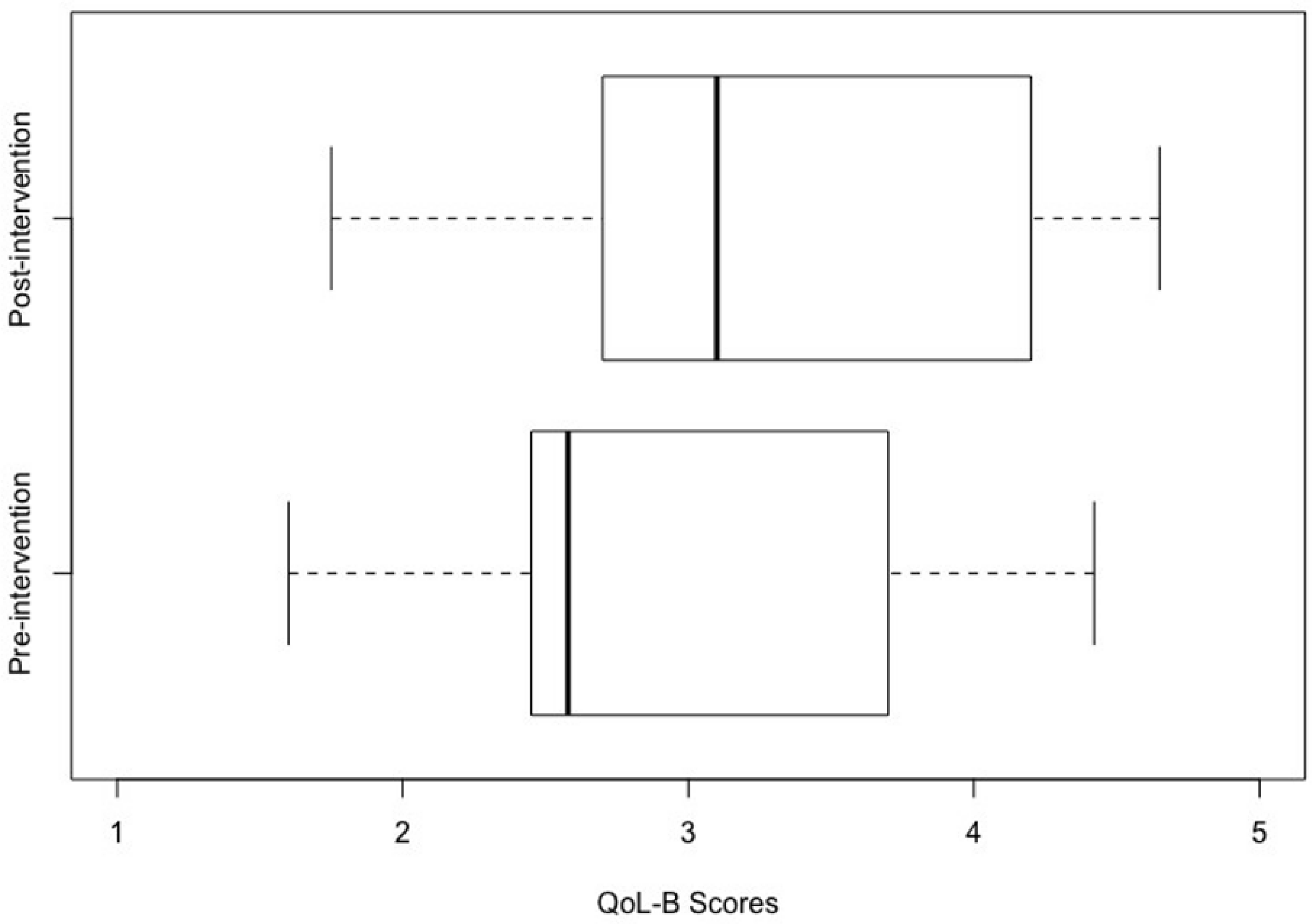
3.1. Pre-Post Intervention Changes
3.2. Parent Questionnaire
3.3. Qualitative Findings
“I have never been offered visuals by the school for use at home. Only since the [staff] came to visit did I really get it.”
“What I liked was the way they came back, so that we were able to tailor it to our current circumstances and then follow it up.”
“We did parent groups… the experience of someone coming into your own home was quite different”
“It was different from other experiences of Visual Supports.”
“It was better for them (staff) to actually see things (at home), it gave it all context. There are real benefits to them coming to the home.”
“I had bought Visual Supports online (before) but wasn’t really using it. The [staff] helped me use it effectively.”
“They asked really good questions, they could really help… made us realise that it doesn’t need to be like this.”
“The [staff] workers never said you’re doing it wrong. It was so comforting to have strangers tell you that you are doing great.”
“We came up with the ideas together.”
“The [staff] team really listened and I found it encouraging. It pushed me more to help my child.”
“They answered all my questions.”
“Crucially, I got to choose.”
“The amount of support was just right.”
“I was very anxious but this experience was so personal and focussed on my own needs, that was nice.”
“Teaching us about it individually is much better than teaching in a group. It is individualised and personalised.”
“I liked how personal it was.”
“Groups are not about your child but [the project] was about our child.”
“Time for specific advice for me rather than in a group is so much more valuable.”
“He didn’t have symbolic understanding, so it was tailored to his needs… It was set up for him as an individual and the progression to symbols was explained.”
“[My child made the] choice of what to focus on and symbol selection.”
“My daughter has made her own visuals.”
“The sooner you have access to expertise and from as young an age as possible, the better.”
“If this had been introduced to me 2 years ago, I would have needed much more support.”
“Eventually we will get better but we need lots of input.”
“Follow ups are crucial at key times (e.g., phone calls at times of transition).”
“I didn’t realise the scope of [visual supports] before. A lot more info would be useful to parents.”
“Visuals helped immediately–it was like, really? That’s all it takes?”
“The [visual supports] has helped, it’s so much more than just timetables.”
“The Nursery was always supportive in using visuals but it was really timetable based. I found using these difficult as home is different than school. However now I understand that it’s about so much more than timetables. I have a much broader understanding.”
“One morning my child got up and set the timetable himself.”
“We wanted our son to be more independent and the [visual supports] has helped.”
“It can help behaviour but also encourages independence.”
“I do believe it has helped keep his behaviour more consistent at home.”
“I want to share my story to inspire others.”
“It felt good to know that other families were experiencing the same thing.”
“I’m thinking creatively now and I have ideas for tackling other issues.”
“It has helped me tackle hard things.”
“We became more consistent with words we used and the order we did things, his speech has really improved.”
“It’s not been magical but it helps.”
“Visual support is great but is does have its limitations.”
“If you are busy it’s not always practical.”
“Not everything worked but I have ideas of other ways and places to use visual supports.”
3.4. Summary of the Qualitative Analysis
4. Discussion
4.1. Limitations
4.2. Implications for Practice
- Home visits can be used as an effective way of providing brief interventions focussed on visual supports;
- Parents can take positives, even when things do not work—so several symbols and methods should be tried;
- Professionals should listen to families and their needs and set appropriate expectations about the level of input and likely benefits of visual supports;
- Professionals should offer visual support as early as possible, and help parents find it, understand it, and use it;
- Parents report positively when they have access to a range of resources relevant to a range of developmental levels;
- Parents should be involved in the assessment process and selecting the symbols used from an early stage;
- It is helpful when staff model how to use visual supports in context (i.e., at home);
- Individualisation and tailoring are viewed positively by parents, particularly around the child’s individual developmental level;
- Follow up visits are needed with parents with the chance to review and adapt, and maintenance options for symbols and other technology are helpful, though these should not be too complex;
- Enhanced knowledge and skills to assess needs and implement visual supports are a core practice for specialist educational professionals and some allied health professionals (for example occupational therapists and speech and language therapists). Such professionals would be well placed to apply home visual support interventions.
4.3. Implications for Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scottish Intercollegiate Guidelines Network (SIGN). Assessment, Diagnosis and Interventions for Autism Spectrum Disorders; SIGN 145; SIGN: Edinburgh, UK, 2016. [Google Scholar]
- Wong, C.; Odom, S.L.; Hume, K.A.; Cox, A.W.; Fettig, A.; Kucharczyk, S.; Plavnick, J.B.; Fleury, V.P.; Schultz, T.R. Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. J. Autism Dev. Disord. 2015, 45, 1951–1966. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, M.; Baxter, J.; Grayson, Z.; Johnston, L.; O’Hare, A. Visual supports at home and in the community for individuals with autism spectrum disorders: A scoping review. Autism 2020, 24, 447–469. [Google Scholar] [CrossRef] [PubMed]
- Oono, I.P.; Honey, E.J.; McConachie, H. Parent-mediated early intervention for young children with autism spectrum disorders (ASD). Evid.-Based Child Health Cochrane Rev. J. 2013, 8, 2380–2479. [Google Scholar] [CrossRef]
- Mesibov, G.; Howley, M.; Naftel, S. Accessing the Curriculum for Learners with Autism Spectrum Disorders: Using the TEACCH Programme to Help Inclusion; Routledge: London, UK, 2015. [Google Scholar]
- Rutherford, M.; Maciver, D.; Johnston, L.; Prior, S.; Forsyth, K. Development of a Pathway for Multidisciplinary Neurodevelopmental Assessment and Diagnosis in Children and Young People. Children 2021, 8, 1033. [Google Scholar] [CrossRef] [PubMed]
- Maciver, D.; Hunter, C.; Johnston, L.; Forsyth, K. Using Stakeholder Involvement, Expert Knowledge and Naturalistic Implementation to Co-Design a Complex Intervention to Support Children’s Inclusion and Participation in Schools: The CIRCLE Framework. Children 2021, 8, 217. [Google Scholar] [CrossRef]
- Maciver, D.; Rutherford, M.; Johnston, L.; Curnow, E.; Boilson, M.; Murray, M. An interdisciplinary nationwide complex intervention for lifespan neurodevelopmental service development: Underpinning principles and realist programme theory. Front. Rehabil. Sci. 2022, 3, 596. [Google Scholar] [CrossRef]
- Steinbrenner, J.R.; Hume, K.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Brock, M.E.; Savage, M.N. Evidence-Based Practices for Children, Youth, and Young Adults with Autism; The University of North Carolina: Chapel Hill, NC, USA, 2020. [Google Scholar]
- Wellington, W.; Stackhouse, J. Using visual support for language and learning in children with SLCN: A training programme for teachers and teaching assistants. Child Lang. Teach. Ther. 2011, 27, 183–201. [Google Scholar] [CrossRef]
- Baxter, J.; Rutherford, M.; Holmes, S. The Visual Support Project (visual supports P): An authority-wide training, accreditation and practical resource for education settings supporting inclusive practice. J. Commun. Matters 2015, 29, 9–13. [Google Scholar]
- Rutherford, M.; Burns, M.; Gray, D.; Bremner, L.; Clegg, S.; Russell, L.; Macdonaldm, H.; O’Hare, A. Improving Efficiency and Quality of the Children’s ASD Diagnostic Pathway: Lessons Learned from Practice. J. Autism Dev. Disord. 2018, 48, 1579–1595. [Google Scholar] [CrossRef] [Green Version]
- Prizant, B.M.; Wetherby, A.M.; Rubin, E.; Laurent, A.C. The SCERTS Model: A transactional, family-centered approach to enhancing communication and socioemotional abilities of children with autism spectrum disorder. Infants Young Child. 2003, 16, 296–316. [Google Scholar] [CrossRef] [Green Version]
- NHS Education for Scotland. The NHS Education for Scotland Autism Training Framework, Optimising Outcomes: A Framework for All Staff Working with People with Autism Spectrum Disorders, Their Families and Carers. 2014. Available online: http://www.knowledge.scot.nhs.uk/media/12392691/sct0117216030-3%20asd%20training%20framework%20cov_final.pdf (accessed on 21 February 2018).
- Tutin, J. IT learning sessions at Leeds Library and Information Service. Libr. Inf. Res. 2013, 37, 29–36. [Google Scholar] [CrossRef]
- McConachie, H.; Parr, J.R.; Glod, M.; Hanratty, J.; Livingstone, N.; Oono, I.P.; Robalino, S.; Baird, G.; Beresford, B.; Charman, T.; et al. Systematic review of tools to measure outcomes for young children with autism spectrum disorder. Health Technol. Assess. 2015, 19, 1–538. [Google Scholar] [CrossRef] [Green Version]
- Leadbitter, K.; Aldred, C.; McConachie, H.; Le Couteur, A.; Kapadia, D.; Charman, T.; Macdonald, W.; Salomone, E.; Emsley, R. The autism family experience questionnaire (AFEQ): An ecologically-valid, parent-nominated measure of family experience, quality of life and prioritised outcomes for early intervention. J. Autism Dev. Disord. 2018, 48, 1052–1062. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.; Dumas, G.; Frazier, T.; Salomone, A.; Taylor, J.L. Autism spectrum disorder. Nat. Rev. Dis. Prim. 2020, 6, 1–23. [Google Scholar] [CrossRef]
- Moss, P.; Mandy, W.; Howlin, P. Child and adult factors related to quality of life in adults with autism. J. Autism Dev. Disord. 2017, 47, 1830–1837. [Google Scholar] [CrossRef] [Green Version]
- Eapen, V.; Črnčec, R.; Walter, A.; Tay, K.P. Conceptualisation and development of a quality of life measure for parents of children with autism spectrum disorder. Autism Res. Treat. 2014, 2014, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Vasilopoulou, E.; Nisbet, J. The quality of life of parents of children with autism spectrum disorder: A systematic review. Res. Autism Spectr. Disord. 2016, 23, 36–49. [Google Scholar] [CrossRef]
- Tavernor, L.; Barron, E.; Rodgers, J.; McConachie, H. Finding out what matters: Validity of quality of life measurement in young people with ASD. Child 2013, 39, 592–601. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. Pract. 2016, 6, 100. [Google Scholar] [CrossRef] [Green Version]
- Donato, C.; Shane, H.C.; Bronwyn, H. Exploring the feasibility of the visual language in autism program for children in an early intervention group setting: Views of parents, educators, and health professionals. Dev. Nuerorehabilitation 2014, 17, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Machalicek, W.; Didden, R.; Lang, R.; Green, V.; Lequia, J.; Sigafoos, J.; O’Reilly, M.F. Families of children with autism spectrum disorders: Intervention and family supports. In Autism and Child Psychopathology Series: Handbook of Early Intervention for Autism Spectrum Disorders; Tarbox, J., Dixon, D.R., Sturmey, P., Matson, J.L., Eds.; Springer: New York, NY, USA, 2014; pp. 511–532. [Google Scholar]
- Arthur-Kelly, M.; Sigafoos, J.; Green, V.; Mathisen, B.; Arthur-Kelly, R. Issues in the use of visual supports to promote communication in individuals with autism spectrum disorder. Disabil. Rehabil. 2009, 31, 1474–1486. [Google Scholar] [CrossRef] [PubMed]
- Foster-Cohen, S.; Mirfin-Veitch, B. Evidence for the effectiveness of visual supports in helping children with disabilities access the mainstream primary school curriculum. J. Res. Spec. Educ. Needs 2015, 17, 77–155. [Google Scholar] [CrossRef]
- Knight, V.; Sartini, E.; Spriggs, A.D. Evaluating visual activity schedules as evidence-based practice for individuals with autism spectrum disorders. J. Autism Dev. Disord. 2015, 45, 157–178. [Google Scholar] [CrossRef] [PubMed]
- Walker, V.L.; Snell, M.E. Effects of augmentative and alternative communication on challenging behavior: A meta-analysis. Augment. Altern. Commun. 2013, 29, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Meadan, H.; Angell, M.E.; Stoner, J.B.; Daczewitz, M.E. Parent-implemented social-pragmatic communication intervention: A pilot study. Focus Autism Other Dev. Disabil. 2014, 29, 95–110. [Google Scholar] [CrossRef]
- DeThorne, L.S.; Searsmith, K. Autism and Neurodiversity: Addressing Concerns and Offering Implications for the School-Based Speech-Language Pathologist. Perspect. ASHA Spec. Interest Groups 2021, 6, 184–190. [Google Scholar] [CrossRef]
- Benevides, T.W.; Shore, S.M.; Andresen, M.L.; Caplan, R.; Cook, B.; Gassner, D.L.; Erves, J.M.; Hazlewood, T.M.; King, M.C.; Morgan, L.; et al. Interventions to address health outcomes among autistic adults: A systematic review. Autism 2020, 24, 1345–1359. [Google Scholar] [CrossRef]
- Sussman, F.; Lewis, R.B. More Than Words: A Guide to Helping Parents Promote Communication and Social Skills in Children with Autism Spectrum Disorder; Hanen Centre: Toronto, AN, Canada, 1999. [Google Scholar]
- Banda, D.R.; Grimmett, D. Enhancing social and transition behaviors of persons with autism through activity schedules: A review. Educ. Train. Dev. Disabil. 2008, 43, 324–333. [Google Scholar]
- Lequia, J.; Machalicek, W.; Rispoli, M.J. Effects of activity schedules on challenging behaviour exhibited in children with autism spectrum disorders: A systematic review. Res. Autism Spectr. Disord. 2012, 6, 480–492. [Google Scholar] [CrossRef]
- Rutherford, M.; Johnston, L. Rethinking Autism Assessment, Diagnosis, and Intervention Within a Neurodevelopmental Pathway Framework. In Autism Spectrum Disorders-Recent Advances and New Perspectives; IntechOpen: London, UK, 2022; Available online: https://www.intechopen.com/online-first/84848 (accessed on 22 November 2022). [CrossRef]



{kind=link}
{kind=link}
| Resources for Child to Use by Stage | * Social Partners | * Language Partners | * Conversation Partners |
|---|---|---|---|
| Object of reference (e.g., spoon to represent meals) | ✓ | ||
| This is what we are doing ‘Now’ object of reference | ✓ | ||
| Now/next board and objects | ✓ | ||
| Object timetable for part or all of the day | ✓ | ||
| Song signifiers (objects of reference) | ✓ | ||
| Choice board | ✓ | ✓ | ✓ |
| Personal photo book | ✓ | ✓ | ✓ |
| Technology-based (e.g., computer or touch device) | ✓ | ✓ | ✓ |
| Now/next board and symbols | ✓ | ||
| Picture exchange communication system | ✓ | ||
| Sequence chart for daily routines (e.g., toileting) | ✓ | ✓ | |
| Countdown cards (e.g., 3 sleeps until …) | ✓ | ✓ | |
| ‘Help’ card | ✓ | ✓ | |
| ‘Wait’ card | ✓ | ✓ | |
| Song symbol book | ✓ | ✓ | |
| Visual symbol shopping list | ✓ | ✓ | |
| Visual/symbol timetable for part or all of day | ✓ | ✓ | |
| Visual timetable or calendar for the week/month | ✓ | ||
| ‘OK/Not OK’ cards | ✓ | ||
| Emotions (e.g., emotions regulation visual) | ✓ | ||
| Social Stories | ✓ | ||
| Resources for parents/environment at any stage | |||
| Home/school visual diary | |||
| Communication passport | |||
| Environmental visual labelling to show where things are and what goes where (e.g., photo above coat) | |||
| Sand timer to prepare for transitions/learning to wait | |||
| Child Age (Years) | Mean (SD) 6.59 (2.57) | Range 3.64–12.21 |
| Parent Age (Years) | Mean (SD) 36.79 (6.23) | Range 24–48 |
| Child Gender | N | % |
| Male | 20 | 68.97 |
| Female | 9 | 31.03 |
| Number of Siblings | ||
| 1 | 19 | 65.52 |
| More than 1 | 10 | 34.48 |
| Diagnosis of Autism | ||
| Yes | 21 | 72.41 |
| No | 8 | 27.59 |
| Use Visual Supports at home | ||
| Yes | 8 | 27.59 |
| Unsure | 12 | 41.38 |
| No | 8 | 27.59 |
| Missing | 1 | 3.45 |
| Current IEP * | ||
| Yes | 4 | 13.79 |
| Unsure | 6 | 20.69 |
| No | 18 | 62.07 |
| Missing | 1 | 3.45 |
| Measure | t | df | p | 95% CI | Mdiff | Effect Size (Cohen’s d) |
|---|---|---|---|---|---|---|
| A. Quality of life | 3.09 | 28 | 0.005 | [0.067, 0.331] | 0.199 | 0.573 |
| B. Autism specific difficulties | 2.99 | 28 | 0.006 | [0.127, 0.680] | 0.404 | 0.556 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rutherford, M.; Baxter, J.; Johnston, L.; Tyagi, V.; Maciver, D. Piloting a Home Visual Support Intervention with Families of Autistic Children and Children with Related Needs Aged 0–12. Int. J. Environ. Res. Public Health 2023, 20, 4401. https://doi.org/10.3390/ijerph20054401
Rutherford M, Baxter J, Johnston L, Tyagi V, Maciver D. Piloting a Home Visual Support Intervention with Families of Autistic Children and Children with Related Needs Aged 0–12. International Journal of Environmental Research and Public Health. 2023; 20(5):4401. https://doi.org/10.3390/ijerph20054401
Chicago/Turabian StyleRutherford, Marion, Julie Baxter, Lorna Johnston, Vaibhav Tyagi, and Donald Maciver. 2023. "Piloting a Home Visual Support Intervention with Families of Autistic Children and Children with Related Needs Aged 0–12" International Journal of Environmental Research and Public Health 20, no. 5: 4401. https://doi.org/10.3390/ijerph20054401
APA StyleRutherford, M., Baxter, J., Johnston, L., Tyagi, V., & Maciver, D. (2023). Piloting a Home Visual Support Intervention with Families of Autistic Children and Children with Related Needs Aged 0–12. International Journal of Environmental Research and Public Health, 20(5), 4401. https://doi.org/10.3390/ijerph20054401