
Exploratory Study on Central Sensitization and Bioelectrical Activity of the Selected Masticatory Muscles in Subjects with Myopia

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.2.1. Assessment of the Bioelectrical Muscle Activity
- The anterior part of the temporalis muscle (TA);
- The superficial part of the masseter muscle (MM);
- The middle part of the sternocleidomastoid muscle belly (SCM);
- The anterior belly of the digastric muscle (DA).
- At rest (10 s);
- During maximal voluntary clenching in the intercuspal position (as hard as possible; 3 × 3 s, 2 s rest between);
- During maximal voluntary clenching on dental rollers (as hard as possible; 3 × 3 s, 2 s rest between);
- During maximal mouth opening (as wide as possible; 3 × 3 s, 2 s rest between).
2.2.2. Ophthalmological Examination
2.2.3. Assessment of the Central Sensitization Inventory
2.2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
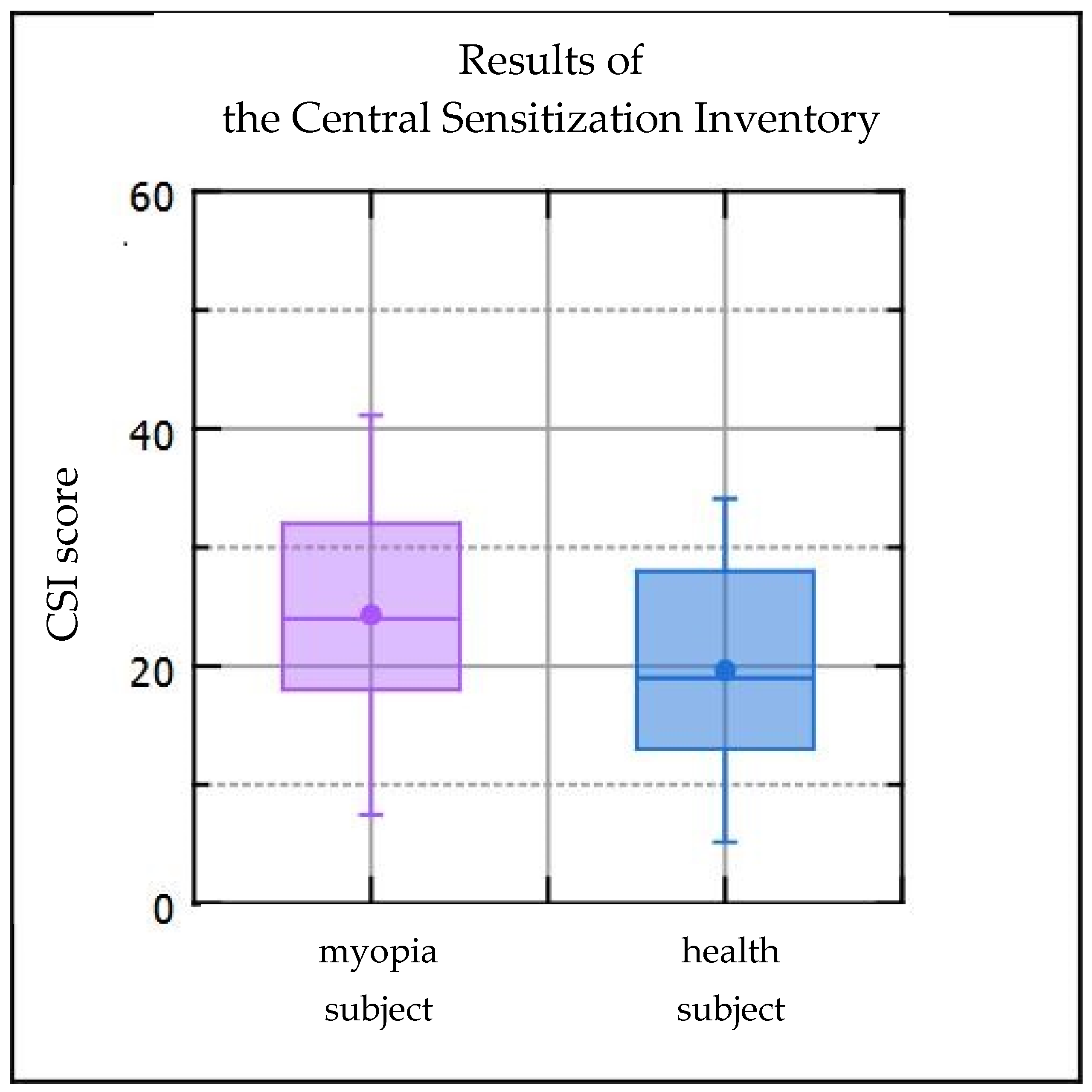
- Subjects with myopia have an increased score in the central sensitization inventory.
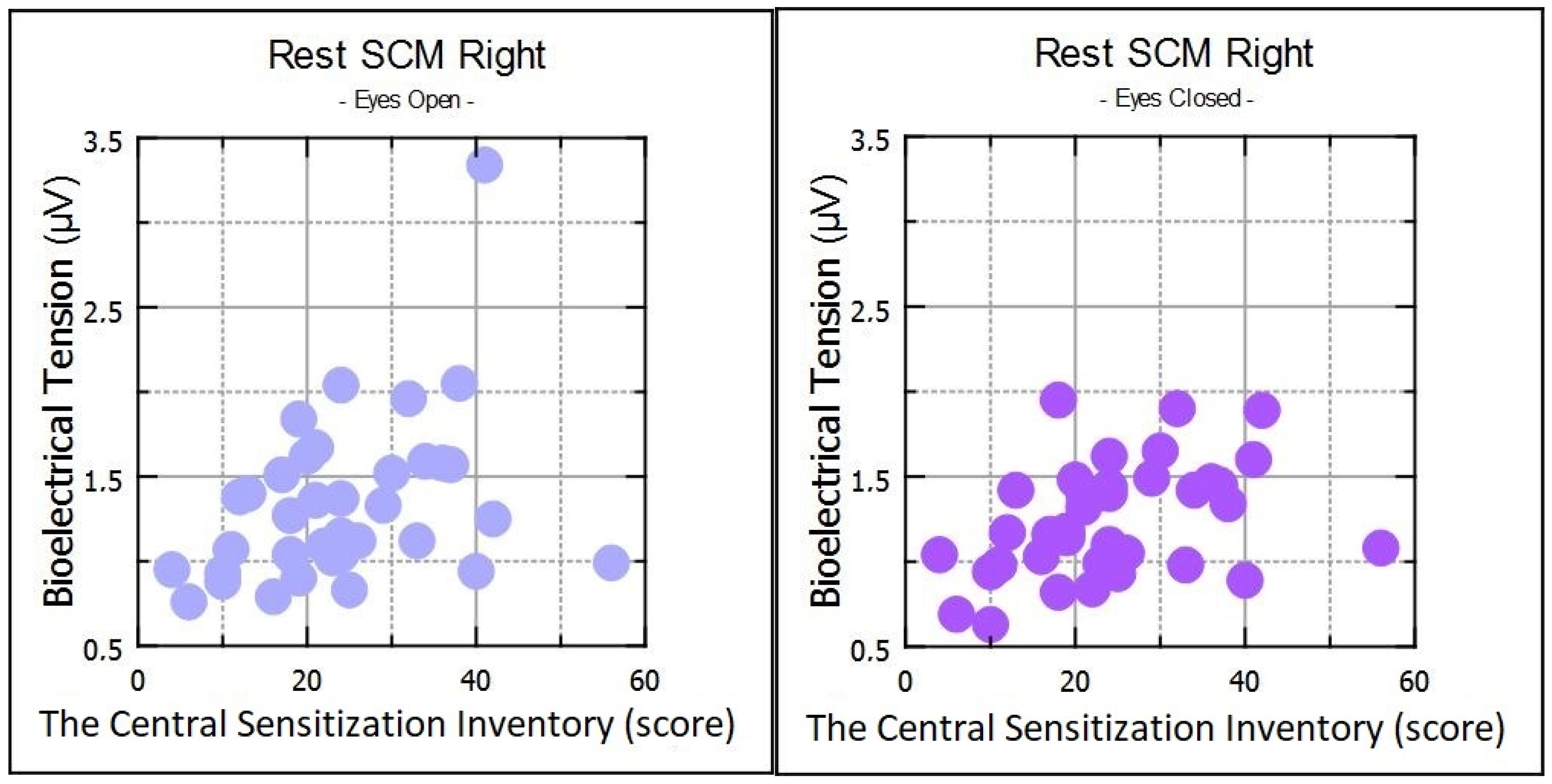
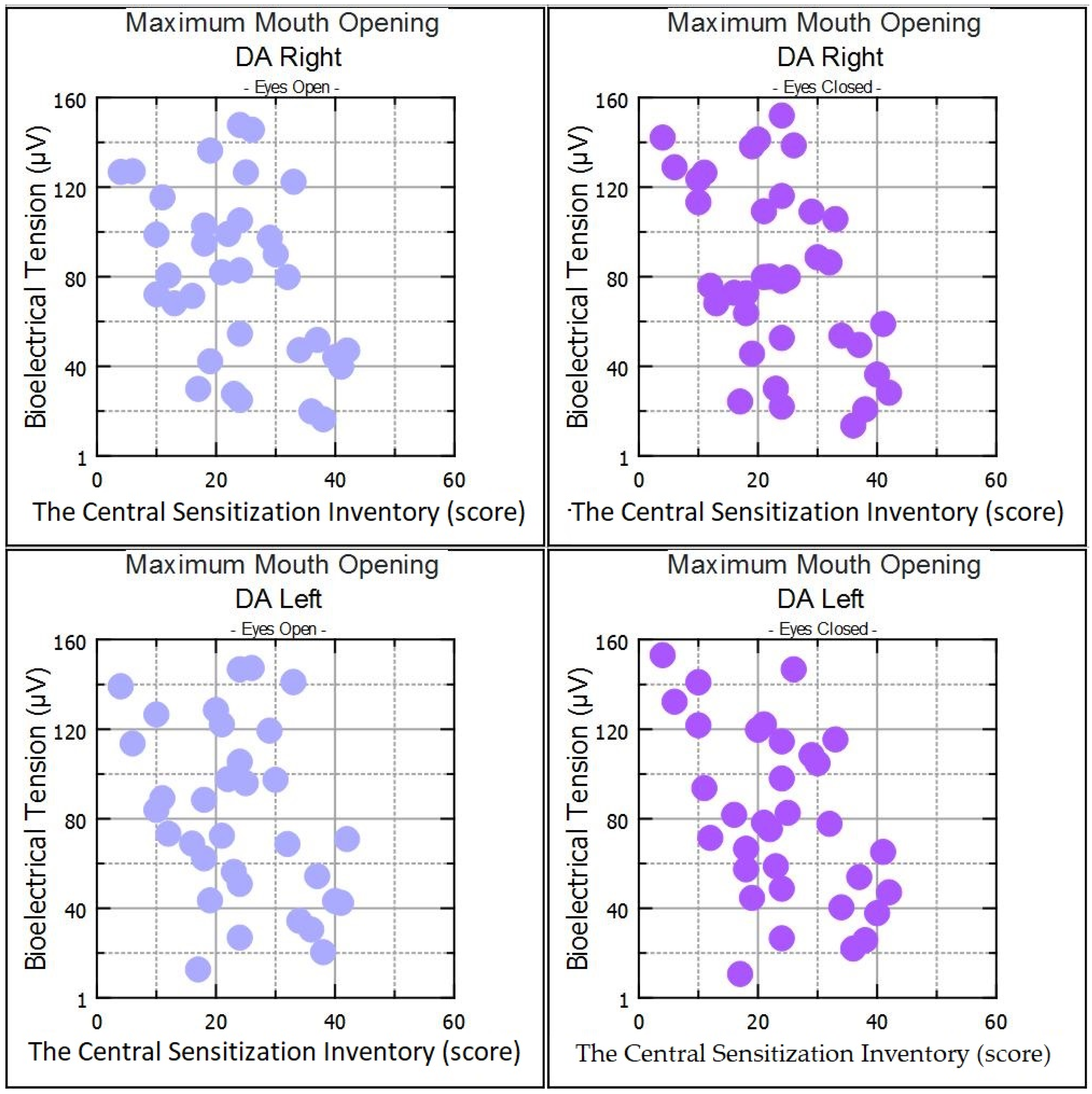
- The increase in the central sensitization inventory score is connected with the changes in the electromyographic activity of the masticatory and neck muscles.
- The effect of central sensitization on masticatory muscle activity in myopic subjects requires further studies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woolf, C.J.; Ma, Q. Nociceptors—Noxious Stimulus Detectors. Neuron 2007, 55, 353–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, S.A.; Herr, M.J. Physiology, Nociception. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Latremoliere, A.; Woolf, C.J. Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, K.C.; Volcheck, M.M. Central Sensitization Syndrome and the Initial Evaluation of a Patient with Fibromyalgia: A Review. Rambam Maimonides Med. J. 2015, 6, e0020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Zolnoun, D.A.; Francisco, E.M.; Holden, J.K.; Dennis, R.G.; Tommerdahl, M. Altered Central Sensitization in Subgroups of Women With Vulvodynia. Clin. J. Pain 2011, 27, 755–763. [Google Scholar] [CrossRef]
- Woolf, C.J. Evidence for a central component of post-injury pain hypersensitivity. Nature 1983, 306, 686–688. [Google Scholar] [CrossRef]
- Sturge, W.A. The Phenomena of Angina Pectoris, and their Bearing Upon the Theory of Counter-Irritation. Brain 1883, 5, 492–510. [Google Scholar] [CrossRef] [Green Version]
- Terminology | International Association for the Study of Pain. Available online: https://www.iasp-pain.org/resources/terminology/ (accessed on 1 March 2023).
- Woolf, C.J.; Salter, M.W. Neuronal Plasticity: Increasing the Gain in Pain. Science 2000, 288, 1765–1769. [Google Scholar] [CrossRef]
- Bittencourt, J.V.; de Melo Magalhães Amaral, A.C.; Rodrigues, P.V.; Corrêa, L.A.; Silva, B.M.; Reis, F.J.J.; Nogueira, L.A.C. Diagnostic accuracy of the clinical indicators to identify central sensitization pain in patients with musculoskeletal pain. Arch. Physiother. 2021, 11, 2. [Google Scholar] [CrossRef]
- Turczyn, P.; Kosińska, B.; Janikowska-Hołoweńko, D.; Malec-Milewska, M.; Marszalec, N.; Maleszka, P.; Tarnacka, B. Translation and cross-cultural adaptation of the Polish Central Sensitization Inventory. Rheumatology 2019, 57, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Foster, P.J.; Jiang, Y. Epidemiology of myopia. Eye 2014, 28, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Medical Advisory Secretariat Phakic Intraocular Lenses for the Treatment of Refractive Errors: An Evidence-Based Analysis. Ont. Health Technol. Assess. Ser. 2009, 9, 1–120.
- Baird, P.N.; Saw, S.-M.; Lanca, C.; Guggenheim, J.A.; Smith, E.L., III; Zhou, X.; Matsui, K.-O.; Wu, P.-C.; Sankaridurg, P.; Chia, A.; et al. Myopia. Nat. Rev. Dis. Primers 2020, 6, 99. [Google Scholar] [CrossRef]
- Lens, A.; Nemeth, S.C.; Ledford, J.K. Ocular Anatomy and Physiology, 2nd ed.; SLACK: Thorofare, NJ, USA, 2008; ISBN 978-1-55642-792-3. [Google Scholar]
- Grosvenor, T.P. Primary Care Optometry, 5th ed.; Butterworth-Heinemann/Elsevier: St. Louis, MO, USA, 2007; ISBN 978-0-7506-7575-8. [Google Scholar]
- Flitcroft, D.I.; He, M.; Jonas, J.B.; Jong, M.; Naidoo, K.; Ohno-Matsui, K.; Rahi, J.; Resnikoff, S.; Vitale, S.; Yannuzzi, L. IMI–Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investig. Opthalmology Vis. Sci. 2019, 60, M20–M30. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.; Tkatchenko, A.V. A Review of Current Concepts of the Etiology and Treatment of Myopia. Eye Contact Lens Sci. Clin. Pract. 2018, 44, 231–247. [Google Scholar] [CrossRef] [PubMed]
- Marchili, N.; Ortu, E.; Pietropaoli, D.; Cattaneo, R.; Monaco, A. Dental Occlusion and Ophthalmology: A Literature Review. Open Dent. J. 2016, 10, 460–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monaco, A.; Cattaneo, R.; Spadaro, A.; Giannoni, M.; Di Martino, S.; Gatto, R. Visual input effect on EMG activity of masticatory and postural muscles in healthy and in myopic children. Eur. J. Paediatr. Dent. 2006, 7, 18–22. [Google Scholar] [PubMed]
- Zieliński, G.; Matysik-Woźniak, A.; Rapa, M.; Baszczowski, M.; Ginszt, M.; Zawadka, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. The Influence of Visual Input on Electromyographic Patterns of Masticatory and Cervical Spine Muscles in Subjects with Myopia. J. Clin. Med. 2021, 10, 5376. [Google Scholar] [CrossRef] [PubMed]
- Zieliński, G.; Wójcicki, M.; Rapa, M.; Matysik-Woźniak, A.; Baszczowski, M.; Ginszt, M.; Litko-Rola, M.; Szkutnik, J.; Różyło-Kalinowska, I.; Rejdak, R.; et al. Masticatory Muscle Thickness and Activity Correlates to Eyeball Length, Intraocular Pressure, Retinal and Choroidal Thickness in Healthy Women versus Women with Myopia. J. Pers. Med. 2022, 12, 626. [Google Scholar] [CrossRef]
- Zieliński, G.; Filipiak, Z.; Ginszt, M.; Matysik-Woźniak, A.; Rejdak, R.; Gawda, P. The Organ of Vision and the Stomatognathic System—Review of Association Studies and Evidence-Based Discussion. Brain Sci. 2022, 12, 14. [Google Scholar] [CrossRef]
- Zieliński, G.; Matysik-Woźniak, A.; Baszczowski, M.; Rapa, M.; Ginszt, M.; Zawadka, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. Effects of visual input on changes in the bioelectrical activity of the cervical and masticatory muscles in myopic subjects. Sci. Rep. 2022, 12, 9435. [Google Scholar] [CrossRef]
- Ilhan, N.; Ilhan, O.; Tuzcu, E.A.; Daglioglu, M.C.; Coskun, M.; Parlakfikirer, N.; Keskin, U. Is There a Relationship Between Pathologic Myopia and Dry Eye Syndrome? Cornea 2014, 33, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Kalangara, J.P.; Galor, A.; Levitt, R.C.; Felix, E.R.; Alegret, R.; Sarantopoulos, C.D. Burning Eye Syndrome: Do Neuropathic Pain Mechanisms Underlie Chronic Dry Eye? Pain Med. Off. J. Am. Acad. Pain Med. 2016, 17, 746–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis, M.N.; Lluch, E.; Nijs, J.; Struyf, F.; Kangasperko, M. The role of central sensitization in shoulder pain: A systematic literature review. Semin. Arthritis Rheum. 2015, 44, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, L. Central and peripheral sensitization in tension-type headache. Curr. Pain Headache Rep. 2003, 7, 460–465. [Google Scholar] [CrossRef]
- Monaco, A.; Cattaneo, R.; Marci, M.C.; Pietropaoli, D.; Ortu, E. Central Sensitization-Based Classification for Temporomandibular Disorders: A Pathogenetic Hypothesis. Pain Res. Manag. 2017, 2017, 5957076. [Google Scholar] [CrossRef] [Green Version]
- Osiewicz, M.A.; Lobbezoo, F.; Loster, B.W.; Wilkosz, M.; Naeije, M.; Ohrbach, R. Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD)—The Polish version of a dual-axis system for the diagnosis of TMD. RDC/TMD Form. J. Stomatol. 2013, 66, 576–649. [Google Scholar] [CrossRef]
- Zieliński, G.; Baszczowski, M.; Ginszt, M.; Rapa, M.; Matysik-Woźniak, A.; Szkutnik, J.; Rejdak, R.; Gawda, P. Analysis of changes in electromyographic masticatory muscle activity in relation to the selected correction of refractive error. Ann. Agric. Environ. Med. 2022. [Google Scholar] [CrossRef]
- Wieczorek, A.; Loster, J.; Loster, B.; Sierpińska, T.; Gołębiewska, M. Correlation between activity and asymmetry indices and skeletal classes in symptomatic-free young adults. J. Stomatol. 2013, 66, 750–760. [Google Scholar] [CrossRef]
- Wieczorek, A.; Loster, J.; Loster, B.W. Relationship between Occlusal Force Distribution and the Activity of Masseter and Anterior Temporalis Muscles in Asymptomatic Young Adults. BioMed Res. Int. 2012, 2013, e354017. [Google Scholar] [CrossRef] [Green Version]
- Wieczorek, A.; Loster, J.E. Activity of the masticatory muscles and occlusal contacts in young adults with and without orthodontic treatment. BMC Oral Health 2015, 15, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L.; Kassoff, A.; Bresnick, G.H.; Bailey, I. New Visual Acuity Charts for Clinical Research. Am. J. Ophthalmol. 1982, 94, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The Development and Psychometric Validation of the Central Sensitization Inventory (CSI). Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing Clinically Significant Values for Identifying Central Sensitivity Syndromes in an Outpatient Chronic Pain Sample. J. Pain Off. J. Am. Pain Soc. 2013, 14, 438–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosińska, B.; Tarnacka, B.; Turczyn, P.; Gromadzka, G.; Malec-Milewska, M.; Janikowska-Hołowenko, D.; Neblett, R. Psychometric validation of the Polish version of the Central Sensitization Inventory in subjects with chronic spinal pain. BMC Neurol. 2021, 21, 483. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 0-203-77158-3. [Google Scholar]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef]
- Suzuki, K.; Haruyama, Y.; Kobashi, G.; Sairenchi, T.; Uchiyama, K.; Yamaguchi, S.; Hirata, K. Central Sensitization in Neurological, Psychiatric, and Pain Disorders: A Multicenter Case-Controlled Study. Pain Res. Manag. 2021, 2021, 6656917. [Google Scholar] [CrossRef]
- Ciavarella, D.; Palazzo, A.; De Lillo, A.; Russo, L.L.; Paduano, S.; Laino, L.; Chimenti, C.; Frezza, F.; Muzio, L.L. Influence of vision on masticatory muscles function: Surface electromyographic evaluation. Ann. Di Stomatol. 2014, 5, 61–65. [Google Scholar] [CrossRef]
- Somisetty, S.; M Das, J. Neuroanatomy, Vestibulo-Ocular Reflex. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Stack, B.; Sims, A.B. The Relationship between Posture and Equilibrium and the Auriculotemporal Nerve in Patients with Disturbed Gait and Balance. Cranio J. Craniomandib. Pract. 2009, 27, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Mense, S. Algesic agents exciting muscle nociceptors. Exp. Brain Res. 2009, 196, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Burnstock, G. Physiology and Pathophysiology of Purinergic Neurotransmission. Physiol. Rev. 2007, 87, 659–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zorena, K.; Gładysiak, A.; Ślęzak, D. Early Intervention and Nonpharmacological Therapy of Myopia in Young Adults. J. Ophthalmol. 2018, 2018, 4680603. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.M.; Hysi, P.G.; Yonova-Doing, E.; Mahroo, O.A.; Snieder, H.; Hammond, C.J. Phenotypic and genotypic correlation between myopia and intelligence. Sci. Rep. 2017, 7, 45977. [Google Scholar] [CrossRef] [Green Version]
- Shahidi, B.; Haight, A.; Maluf, K. Differential effects of mental concentration and acute psychosocial stress on cervical muscle activity and posture. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2013, 23, 1082–1089. [Google Scholar] [CrossRef] [Green Version]
- Szeto, G.P.Y.; Straker, L.M.; O’Sullivan, P.B. A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work—2: Neck and shoulder kinematics. Man. Ther. 2005, 10, 281–291. [Google Scholar] [CrossRef]
- Edmondston, S.J.; Sharp, M.; Symes, A.; Alhabib, N.; Allison, G.T. Changes in mechanical load and extensor muscle activity in the cervico-thoracic spine induced by sitting posture modification. Ergonomics 2011, 54, 179–186. [Google Scholar] [CrossRef]
- Edwards, M.J.M.; Hazi, A.; Crewther, S.G. Acute Psychosocial Stress Induces a Myopic Shift in Undergraduate Students. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2841. [Google Scholar]
- Li, Q.; Yang, J.; He, Y.; Wang, T.; Zhong, L.; Zhu, Z.; Wang, T.; Ling, S. Investigation of the psychological health of first-year high school students with myopia in Guangzhou. Brain Behav. 2020, 10, e01594. [Google Scholar] [CrossRef]
- Zhang, H.; Gao, H.; Zhu, Y.; Zhu, Y.; Dang, W.; Wei, R.; Yan, H. Relationship Between Myopia and Other Risk Factors With Anxiety and Depression Among Chinese University Freshmen During the COVID-19 Pandemic. Front. Public Health 2021, 9, 774237. [Google Scholar] [CrossRef] [PubMed]
- Jones-Jordan, L.A.; Sinnott, L.T.; Chu, R.H.; Cotter, S.A.; Kleinstein, R.N.; Manny, R.E.; Mutti, D.O.; Twelker, J.D.; Zadnik, K.; CLEERE Study Group. Myopia Progression as a Function of Sex, Age, and Ethnicity. Investig. Opthalmol. Vis. Sci. 2021, 62, 36. [Google Scholar] [CrossRef] [PubMed]
- Luong, T.Q.; Shu, Y.-H.; Modjtahedi, B.S.; Fong, D.S.; Choudry, N.; Tanaka, Y.; Nau, C.L. Racial and Ethnic Differences in Myopia Progression in a Large, Diverse Cohort of Pediatric Patients. Investig. Opthalmol. Vis. Sci. 2020, 61, 20. [Google Scholar] [CrossRef] [PubMed]
- Coronado, R.A.; George, S.Z. The Central Sensitization Inventory and Pain Sensitivity Questionnaire: An exploration of construct validity and associations with widespread pain sensitivity among individuals with shoulder pain. Musculoskelet. Sci. Pract. 2018, 36, 61–67. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Myopic Group | Healthy Group | Test | p | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||
| n | 37.00 | 41.00 | ||||||
| Refractive Error (Diopters) | R | −2.50 | −1.50 | - | - | |||
| L | −2.50 | −1.50 | - | - | ||||
| Best Corrected Visual Acuity | R | 1.0 | - | |||||
| L | 1.0 | - | ||||||
| Visual Acuity | R | - | 1.0 | |||||
| L | - | 1.0 | ||||||
| Intraocular Pressure (mmHg) | R | 14.52 | 4.81 | 15.87 | 3.49 | z | −0.98 | 0.33 |
| L | 15.74 | 3.25 | 14.70 | 4.00 | z | 0.65 | 0.52 | |
| Axial Length (mm) | R | 24.38 | 0.63 | 23.59 | 0.63 | z | 3.51 | 0.00 * ES = 0.25 |
| L | 24.38 | 0.66 | 23.59 | 0.62 | z | 3.49 | 0.00 * ES = 0.25 | |
| Sex | F | 24 | 28 | z | 0.31 | 0.75 | ||
| M | 13 | 13 | ||||||
| Age (years) | 22.92 | 1.69 | 23.19 | 1.06 | z | −0.74 | 0.46 | |
| Height (cm) | 172.62 | 9.64 | 171.02 | 8.17 | z | 0.34 | 0.73 | |
| Weight (kg) | 68.19 | 17.33 | 65.50 | 12.04 | z | 0.36 | 0.72 | |
| Body Mass Index | 22.59 | 3.67 | 22.30 | 3.21 | z | 0.00 | 1.00 | |
| Mandibular Range Of Motion (mm) | Abduction Without Pain | 51.16 | 7.34 | 50.86 | 5.44 | t | 0.21 | 0.83 |
| Active Abduction | 51.73 | 7.01 | 52.00 | 5.77 | t | −0.19 | 0.85 | |
| Passive Abduction | 54.05 | 7.03 | 54.24 | 6.15 | t | −0.12 | 0.90 | |
| Mandibular Movement to The Right | 9.16 | 1.86 | 9.17 | 2.67 | z | −0.39 | 0.70 | |
| Mandibular Movement to The Left | 9.81 | 1.98 | 9.88 | 2.46 | z | −0.54 | 0.59 | |
| Protrusion | 8.86 | 2.30 | 8.60 | 2.49 | z | 0.69 | 0.49 | |
| Myopic Subjects | Healthy Subjects | Test | p | 95% IC | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||
| CSI | 24.30 | 11.22 | 19.57 | 9.54 | t | 2.02 | 0.04 * ES = 0.45 | 0.05, 9.41 |
| Myopic Subjects | Healthy Subjects | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | R | t(N-2) | p | 95% IC | Mean | SD | R | t(N-2) | p | 95% IC | ||
| Rest | TA-R | 2.30 | 1.87 | 0.08 | 0.46 | 0.65 | −0.25, 0.39 | 2.50 | 1.92 | 0.05 | 0.31 | 0.76 | −0.26, 0.35 |
| TA-L | 2.36 | 1.34 | 0.21 | 1.26 | 0.22 | −1.22, 0.50 | 2.20 | 1.53 | 0.06 | 0.35 | 0.73 | −0.25, 0.36 | |
| MM- R | 2.36 | 1.56 | 0.12 | 0.70 | 0.49 | −0.21, 0.43 | 2.53 | 1.87 | 0.01 | 0.03 | 0.97 | −0.30, 0.31 | |
| MM-L | 2.42 | 1.65 | −0.06 | −0.37 | 0.72 | −0.38, 0.27 | 2.14 | 0.96 | 0.00 | 0.01 | 0.99 | −0.31, 0.31 | |
| SCM-R | 1.33 | 0.49 | 0.38 | 2.41 | 0.02 * | 0.60, 0.63 | 1.17 | 0.34 | 0.15 | 0.93 | 0.36 | −0.17, 0.44 | |
| SCM-L | 1.47 | 0.51 | 0.07 | 0.42 | 0.68 | −0.26, 0.39 | 1.24 | 0.31 | 0.09 | 0.55 | 0.59 | −0.22, 0.39 | |
| DA-R | 1.92 | 1.09 | 0.15 | 0.90 | 0.37 | −0.18, 0.45 | 1.75 | 0.88 | 0.20 | 1.24 | 0.22 | −0.11, 0.48 | |
| DA-L | 1.93 | 1.14 | −0.07 | −0.39 | 0.70 | −0.39, 0.26 | 1.68 | 0.81 | 0.02 | 0.09 | 0.93 | −0.29, 0.33 | |
| Clenching in the intercuspal position | TA-R | 151.45 | 73.61 | −0.15 | −0.89 | 0.38 | −0.45, 0.18 | 149.95 | 82.19 | 0.13 | 0.80 | 0.43 | −0.19, 0.42 |
| TA-L | 155.35 | 81.38 | −0.08 | −0.49 | 0.63 | 0.39, 025 | 139.57 | 71.21 | 0.04 | 0.22 | 0.83 | −0.27, 0.34 | |
| MM- R | 186.89 | 133.93 | −0.10 | −0.57 | 0.57 | −0.41, 0.23 | 169.12 | 98.21 | 0.04 | 0.25 | 0.80 | −0.27, 0.34 | |
| MM-L | 170.74 | 125.81 | −0.06 | −0.36 | 0.72 | −0.38, 0.27 | 162.76 | 104.02 | 0.08 | 0.51 | 0.61 | −0.23, 0.38 | |
| SCM-R | 14.05 | 11.34 | 0.08 | 0.49 | 0.63 | −0.25, 0,39 | 11.22 | 7.39 | 0.19 | 1.19 | 0.24 | −0.12, 0.47 | |
| SCM-L | 13.82 | 10.41 | 0.18 | 1.08 | 0.29 | −0.15, 0.48 | 13.08 | 12.40 | 0.15 | 0.94 | 0.35 | −0.17, 0.44 | |
| DA-R | 24.08 | 17.15 | 0.24 | 1.46 | 0.15 | 0.09, 0,52 | 20.64 | 12.01 | 0.33 | 2.10 | 0.04 * | 0.03, 0.58 | |
| DA-L | 26.11 | 21.97 | 0.11 | 0.62 | 0.54 | −0.22, 0.42 | 19.83 | 12.16 | 0.21 | 1.31 | 0.20 | −0.10, 0.49 | |
| Clenching on dental cotton rollers | TA-R | 134.69 | 61.21 | −0.05 | −0.28 | 0.78 | −0.37, 0.28 | 140.94 | 79.85 | 0.22 | 1.41 | 0.17 | −0.09, 0.49 |
| TA-L | 137.20 | 68.47 | 0.03 | 0.16 | 0.87 | −0.30, 0.35 | 135.89 | 61.96 | 0.20 | 1.26 | 0.21 | −0.11, 0.49 | |
| MM- R | 191.50 | 107.30 | 0.03 | 0.15 | 0.88 | −0.30, 0.35 | 183.48 | 85.64 | 0.22 | 1.40 | 0.17 | −0.09, 0.49 | |
| MM-L | 179.62 | 107.82 | −0.05 | −0.31 | 0.76 | −0.37, 0.28 | 183.47 | 86.04 | 0.23 | 1.49 | 0.14 | −0.08, 0.50 | |
| SCM-R | 15.21 | 10.95 | 0.23 | 1.38 | 0.18 | −0.10, 0.52 | 13.09 | 7.02 | 0.29 | 1.90 | 0.07 | −0.02, 0.55 | |
| SCM-L | 15.34 | 8.98 | 0.30 | 1.87 | 0.07 | −0.03, 0.57 | 14.95 | 11.35 | 0.28 | 1.82 | 0.08 | −0.03, 0.54 | |
| DA-R | 25.54 | 15.03 | 0.43 | 2.75 | 0.01 * | 0.12, 0.66 | 21.17 | 9.22 | 0.37 | 2.39 | 0.02 * | 0.07, 0.61 | |
| DA-L | 27.54 | 20.12 | 0.21 | 1.28 | 0.21 | −1.12, 0.50 | 21.64 | 9.77 | 0.15 | 0.92 | 0.36 | −0.17, 0.44 | |
| Maximum mouth opening | TA-R | 10.45 | 11.90 | 0.14 | 0.85 | 0.40 | −0.19, 0.44 | 5.90 | 5.09 | −0.14 | −0.91 | 0.37 | −0.43, 0.18 |
| TA-L | 9.25 | 9.08 | 0.19 | 1.12 | 0.27 | −0.14, 0.48 | 6.10 | 5.72 | −0.12 | −0.76 | 0.45 | −0.41, 0.19 | |
| MM- R | 14.87 | 17.88 | 0.15 | 0.90 | 0.37 | −0.18, 0.45 | 9.58 | 11.55 | −0.27 | −1.74 | 0.09 | −0.53, 0.04 | |
| MM-L | 12.64 | 12.69 | 0.13 | 0.77 | 0.45 | −0.20, 0.44 | 8.14 | 6.80 | −0.25 | −1.61 | 0.12 | −0.52, 0.06 | |
| SCM-R | 16.15 | 18.54 | 0.21 | 1.27 | 0.21 | −1.12, 0.50 | 8.61 | 6.52 | −0.12 | −0.75 | 0.46 | −0.41, 0.19 | |
| SCM-L | 17.79 | 23.70 | 0.17 | 0.99 | 0.33 | −0.16, 0.47 | 9.84 | 13.09 | −0.06 | −0.36 | 0.72 | −0.36, 0.25 | |
| DA-R | 84.91 | 41.96 | −0.36 | −2.28 | 0.03 * | −0.61, −0.04 | 60.32 | 38.28 | −0.10 | −0.59 | 0.56 | −0.40, 0.21 | |
| DA-L | 88.43 | 46.72 | −0.35 | −2.21 | 0.03 * | −0.61, −0.03 | 60.71 | 41.81 | −0.02 | −0.10 | 0.92 | −0.33, 0.29 | |
| Myopic Subjects | Healthy Subjects | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | R | t(N-2) | p | 95% IC | Mean | SD | R | t(N-2) | p | 95% IC | ||
| Rest | TA-R | 2.02 | 1.26 | 0.08 | 0.47 | 0.64 | −0.25, 0.39 | 1.96 | 1.29 | 0.13 | 0.82 | 0.41 | −0.19, 0.42 |
| TA-L | 2.22 | 1.54 | 0.05 | 0.27 | 0.79 | −0.28, 0.37 | 1.78 | 1.03 | 0.17 | 1.05 | 0.30 | −0.15, 0.45 | |
| MM- R | 2.23 | 1.37 | 0.14 | 0.80 | 0.43 | −0.19, 0.44 | 2.34 | 1.50 | −0.17 | −1.09 | 0.28 | −0.45, 0.15 | |
| MM-L | 2.33 | 2.01 | 0.02 | 0.14 | 0.89 | −0.31, 0.34 | 2.23 | 1.51 | 0.12 | 0.78 | 0.44 | −0.19, 0.41 | |
| SCM-R | 1.24 | 0.33 | 0.40 | 2.62 | 0.01 * | 0.09, 0.64 | 1.33 | 0.59 | 0.13 | 0.82 | 0.42 | −0.19, 0.42 | |
| SCM-L | 1.42 | 0.46 | 0.27 | 1.68 | 0.10 | −0.06, 0.55 | 1.39 | 0.58 | 0.00 | 0.00 | 1.00 | −0.31, 0.31 | |
| DA-R | 1.70 | 0.73 | −0.28 | −1.70 | 0.10 | −0.55, 0.05 | 1.69 | 0.62 | 0.10 | 0.58 | 0.56 | −0.21, 0.40 | |
| DA-L | 1.72 | 0.76 | −0.33 | −2.01 | 0.05 | −0.59, −0.01 | 1.57 | 0.51 | 0.10 | 0.60 | 0.55 | −0.21, 0.40 | |
| Clenching in the intercuspal position | TA-R | 135.21 | 67.91 | −0.15 | −0.87 | 0.39 | −0.45, 0.18 | 135.73 | 67.68 | 0.10 | 0.61 | 0.54 | −0.21, 0.40 |
| TA-L | 140.55 | 76.46 | −0.06 | −0.38 | 0.70 | −0.38, 0.27 | 131.28 | 63.63 | 0.01 | 0.06 | 0.95 | −0.30, 0.32 | |
| MM- R | 162.55 | 120.38 | −0.11 | −0.63 | 0.53 | −0.42, 0.22 | 143.93 | 89.67 | 0.15 | 0.92 | 0.37 | −0.17, 0.44 | |
| MM-L | 151.62 | 115.81 | −0.06 | −0.35 | 0.73 | −0.38, 0.27 | 139.18 | 85.60 | 0.05 | 0.34 | 0.74 | −0.26, 0.35 | |
| SCM-R | 11.31 | 9.25 | 0.07 | 0.40 | 0.70 | −0.26, 0.39 | 9.38 | 6.26 | 0.18 | 1.12 | 0.27 | −0.14, 0.46 | |
| SCM-L | 11.09 | 7.70 | 0.15 | 0.88 | 0.38 | −0.18, 0.45 | 10.51 | 8.77 | 0.21 | 1.35 | 0.18 | −0.10, 0.49 | |
| DA-R | 20.78 | 13.44 | 0.18 | 1.08 | 0.29 | −0.15, 0.48 | 17.63 | 11.22 | 0.29 | 1.84 | 0.07 | −0.02, 0.55 | |
| DA-L | 22.19 | 18.52 | 0.09 | 0.54 | 0.60 | −0.24, 0.40 | 16.61 | 11.33 | 0.21 | 1.31 | 0.20 | −0.10, 0.49 | |
| Clenching on dental cotton rollers | TA-R | 135.04 | 56.62 | −0.06 | −0.36 | 0.72 | −0.38, 0.27 | 140.88 | 76.42 | 0.17 | 1.10 | 0.28 | −0.15, 0.45 |
| TA-L | 137.40 | 63.16 | −0.06 | −0.36 | 0.72 | −0.38, 0.27 | 136.83 | 62.15 | 0.20 | 1.27 | 0.21 | −0.11, 0.48 | |
| MM- R | 184.33 | 97.21 | 0.06 | 0.38 | 0.71 | −0.27, 0.38 | 173.64 | 85.50 | 0.26 | 1.68 | 0.10 | −0.05, 0.53 | |
| MM-L | 177.26 | 105.41 | 0.02 | 0.09 | 0.93 | −0.31, 0.34 | 174.21 | 82.26 | 0.25 | 1.62 | 0.11 | −0.06, 0.52 | |
| SCM-R | 13.93 | 9.79 | 0.19 | 1.15 | 0.26 | −0.14, 0.48 | 12.38 | 7.26 | 0.39 | 2.67 | 0.01 * | 0.09, 0.62 | |
| SCM-L | 14.48 | 8.75 | 0.18 | 1.11 | 0.27 | −0.15, 0.48 | 14.10 | 10.75 | 0.32 | 2.07 | 0.04 * | 0.01, 0.57 | |
| DA-R | 23.74 | 12.74 | 0.29 | 1.78 | 0.08 | −0.04, 0.56 | 19.28 | 8.46 | 0.36 | 2.35 | 0.02 * | 0.06, 0.60 | |
| DA-L | 25.48 | 20.35 | 0.23 | 1.37 | 0.18 | −0.10, 0.52 | 18.83 | 9.50 | 0.26 | 1.63 | 0.11 | −0.05, 0.53 | |
| Maximum mouth opening | TA-R | 9.28 | 8.19 | 0.08 | 0.50 | 0.62 | −0.25, 0.39 | 5.07 | 3.01 | −0.21 | −1.33 | 0.19 | −0.49, 0.10 |
| TA-L | 8.77 | 7.84 | 0.15 | 0.92 | 0.36 | −0.18, 0.45 | 4.79 | 3.34 | −0.23 | −1.50 | 0.14 | −0.50, 0.08 | |
| MM- R | 13.86 | 16.96 | 0.03 | 0.19 | 0.85 | −0.30, 0.35 | 11.01 | 16.35 | −0.09 | −0.54 | 0.59 | −0.39, 0.22 | |
| MM-L | 12.15 | 10.99 | 0.04 | 0.24 | 0.81 | −0.29, 0.36 | 6.93 | 4.46 | −0.11 | −0.66 | 0.51 | −0.40, 0.20 | |
| SCM-R | 15.64 | 17.91 | 0.07 | 0.42 | 0.68 | −0.26, 0.39 | 8.72 | 8.04 | −0.16 | −0.99 | 0.33 | −0.45, 0.16 | |
| SCM-L | 18.23 | 24.95 | 0.06 | 0.36 | 0.72 | −0.27, 0.38 | 9.63 | 11.19 | −0.07 | −0.42 | 0.68 | −0.37, 0.24 | |
| DA-R | 81.52 | 40.20 | −0.43 | −2.75 | 0.01 * | −0.66, −0.12 | 65.44 | 44.87 | −0.12 | −0.73 | 0.47 | −0.41, 0.19 | |
| DA-L | 88.43 | 46.72 | −0.35 | −2.21 | 0.03 * | −0.61, −0.03 | 60.71 | 41.81 | −0.02 | −0.10 | 0.92 | −0.33, 0.29 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zieliński, G.; Matysik-Woźniak, A.; Baszczowski, M.; Rapa, M.; Ginszt, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. Exploratory Study on Central Sensitization and Bioelectrical Activity of the Selected Masticatory Muscles in Subjects with Myopia. Int. J. Environ. Res. Public Health 2023, 20, 4524. https://doi.org/10.3390/ijerph20054524
Zieliński G, Matysik-Woźniak A, Baszczowski M, Rapa M, Ginszt M, Szkutnik J, Rejdak R, Gawda P. Exploratory Study on Central Sensitization and Bioelectrical Activity of the Selected Masticatory Muscles in Subjects with Myopia. International Journal of Environmental Research and Public Health. 2023; 20(5):4524. https://doi.org/10.3390/ijerph20054524
Chicago/Turabian StyleZieliński, Grzegorz, Anna Matysik-Woźniak, Michał Baszczowski, Maria Rapa, Michał Ginszt, Jacek Szkutnik, Robert Rejdak, and Piotr Gawda. 2023. "Exploratory Study on Central Sensitization and Bioelectrical Activity of the Selected Masticatory Muscles in Subjects with Myopia" International Journal of Environmental Research and Public Health 20, no. 5: 4524. https://doi.org/10.3390/ijerph20054524
APA StyleZieliński, G., Matysik-Woźniak, A., Baszczowski, M., Rapa, M., Ginszt, M., Szkutnik, J., Rejdak, R., & Gawda, P. (2023). Exploratory Study on Central Sensitization and Bioelectrical Activity of the Selected Masticatory Muscles in Subjects with Myopia. International Journal of Environmental Research and Public Health, 20(5), 4524. https://doi.org/10.3390/ijerph20054524