
Impact of the Frequency and Type of Procedures Performed in Nuclear Medicine Units on the Expected Radiological Hazard

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Thermoluminescent Detectors (TLD)
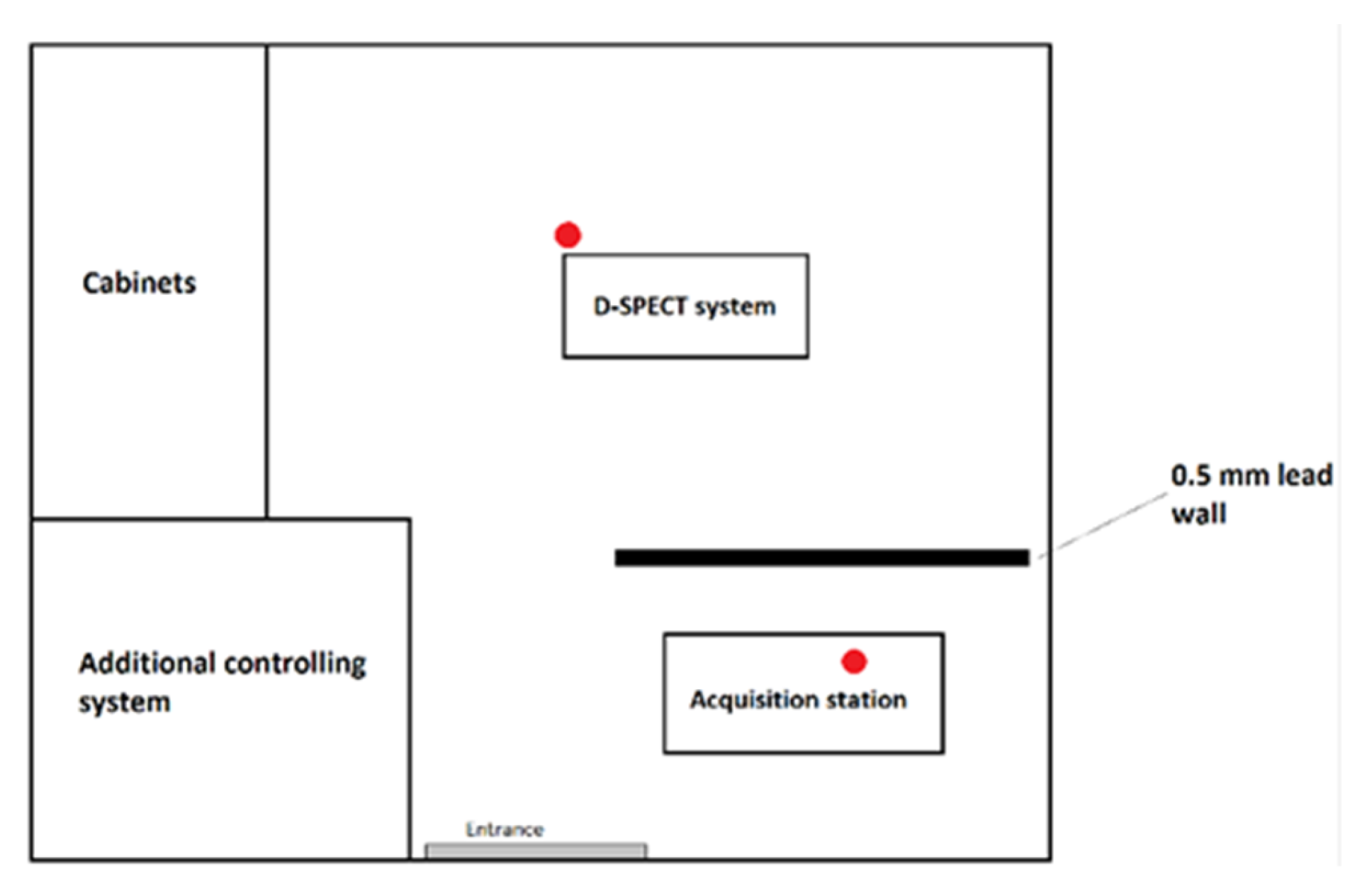
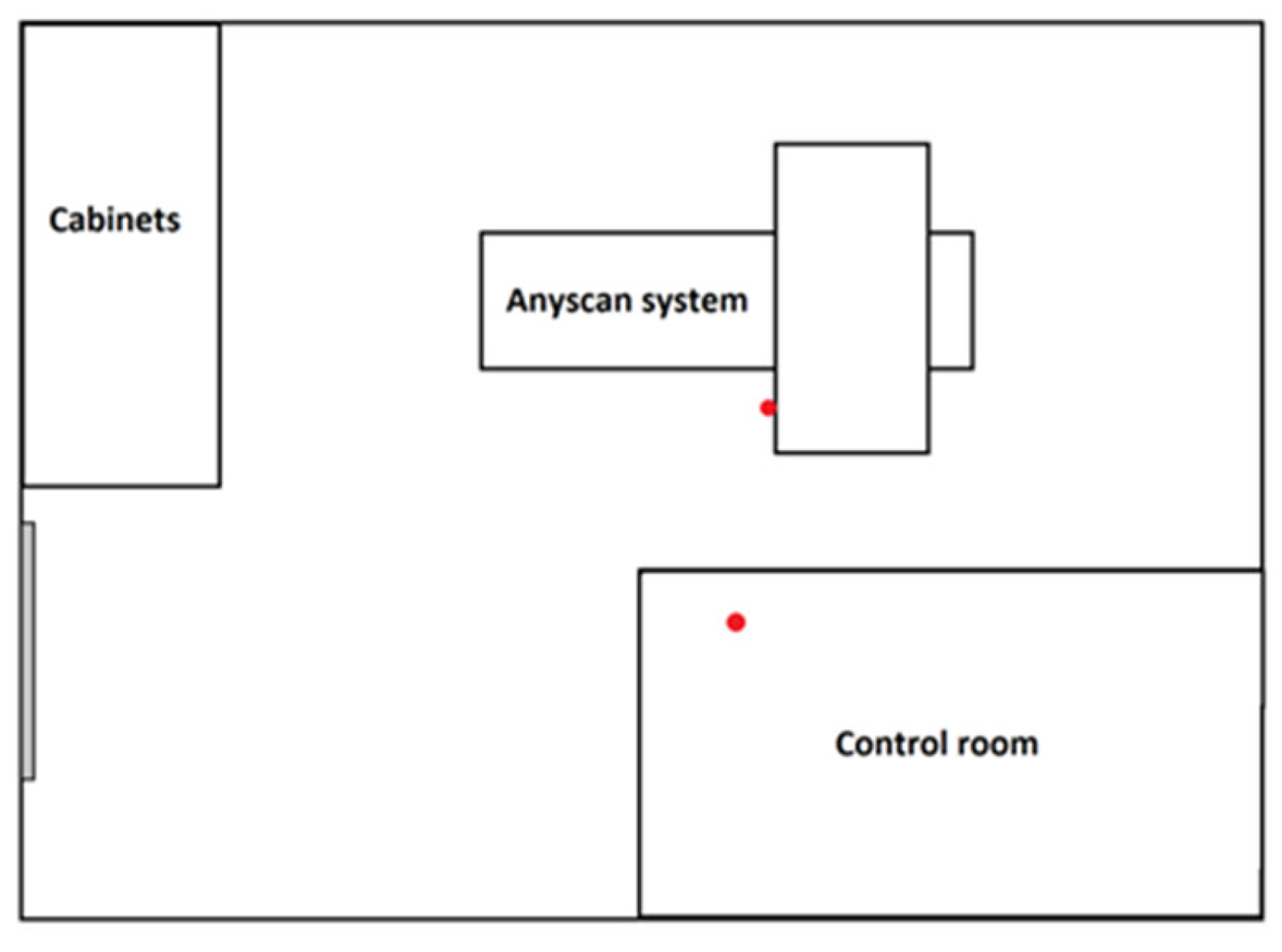
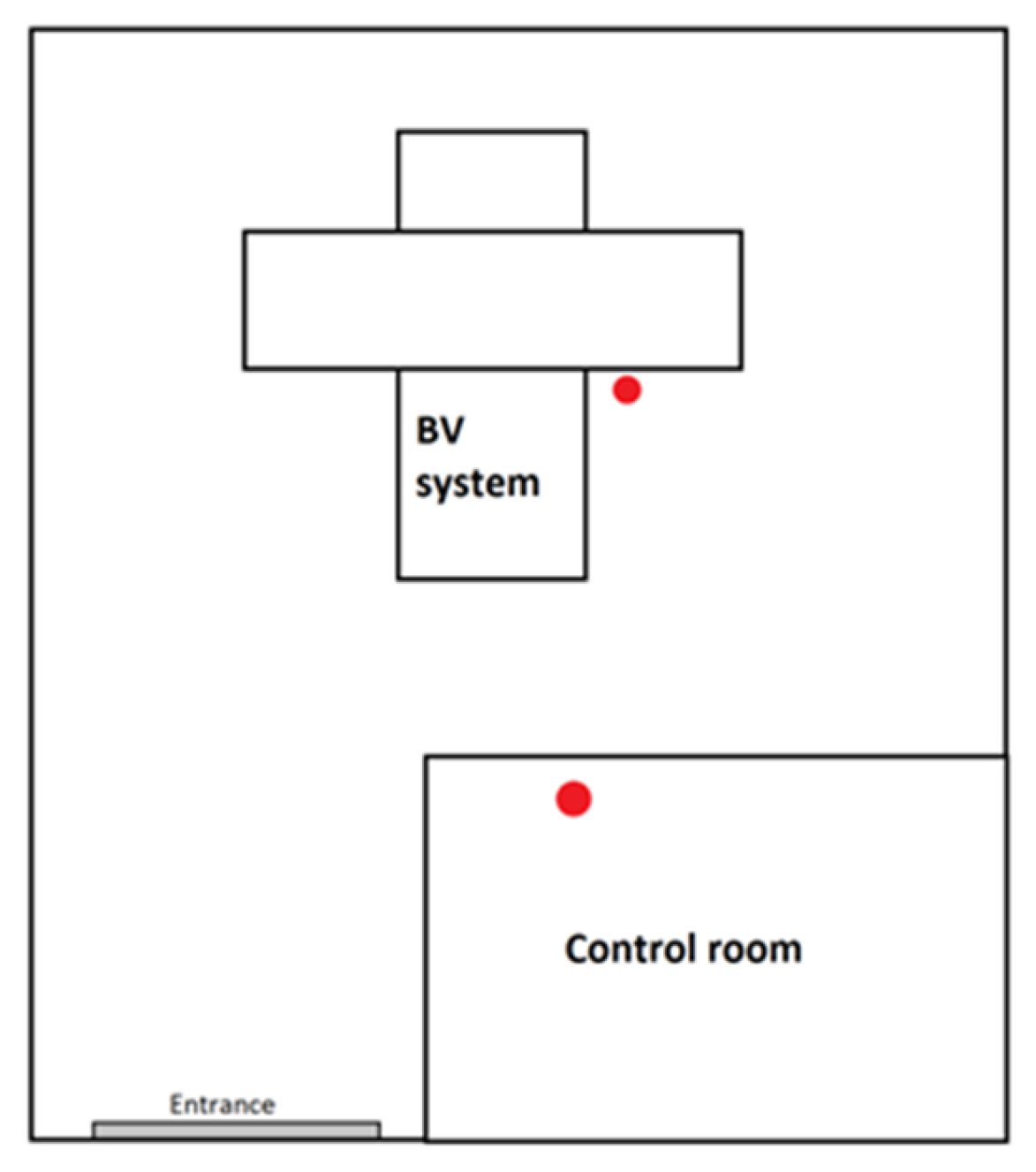
2.2. Equipment
- double-head gamma camera AnyScan SC SPECT/CT, produced by Mediso;
- double-head gamma camera BrightView XCT SPECT/CT, produced by Philips;
- cardiac CZT gamma camera D-SPECT, produced by Spectrum Dynamics Medical.
2.3. Selected Nuclear Medicine Procedures
- Myocardial perfusion scintigraphy—the reference activity was 800 MBq per injection but due to using CZT gamma camera, while performing the presented study, it was possible to reduce injected radioactivity by 50% in relation to the reference value [26]. Study duration: 5–12 min [27]. Data obtained from 158 patients (105 women, 53 men) were taken into account. In this group, 76 rest and 82 stress myocardial perfusion scintigraphy procedures were performed. The average administered radioactivity was 396 ± 74 MBq.
- Bone scintigraphy—the reference activity was 740 MBq. Study duration of the delayed phase: 20 min [27]. The analyzed data consist of 24 patients (14 women and 10 men). The average administered radioactivity was 722 ± 103 MBq.
- Renal scintigraphy—in the case of the presented work performed in dynamic protocol. The reference radioactivity ranged from 70 to 200 MBq. Study duration: 20–30 min [27]. Data obtained from nine patients (six with use of 131I and three with 99mTc) were taken into account.
- Parathyroid glands scintigraphy—acquisition was carried out with two different radiotracers: 99mTcO4 and 99mTc-MIBI. The reference radioactivity for thyroid study was 80 MBq for the test with 99mTcO4 and 500–740 MBq for imaging with 99mTc-MIBI. For imaging with 99mTc-MIBI, imaging was performed twice—20 min and 120 min after injection. Duration of each part of the study: 15 min [27]. The analyzed data consist of five patients.
- Thyroid scintigraphy—typically performed using two isotopes: 131I or 99mTc which depended on clinical indications. In the case of 131I the reference, the activity was 7.4 MBq, while for 99mTc, it was 80 MBq. Study duration for each studies: 15–30 min [27]. The analyzed data consist of five patients.
3. Results
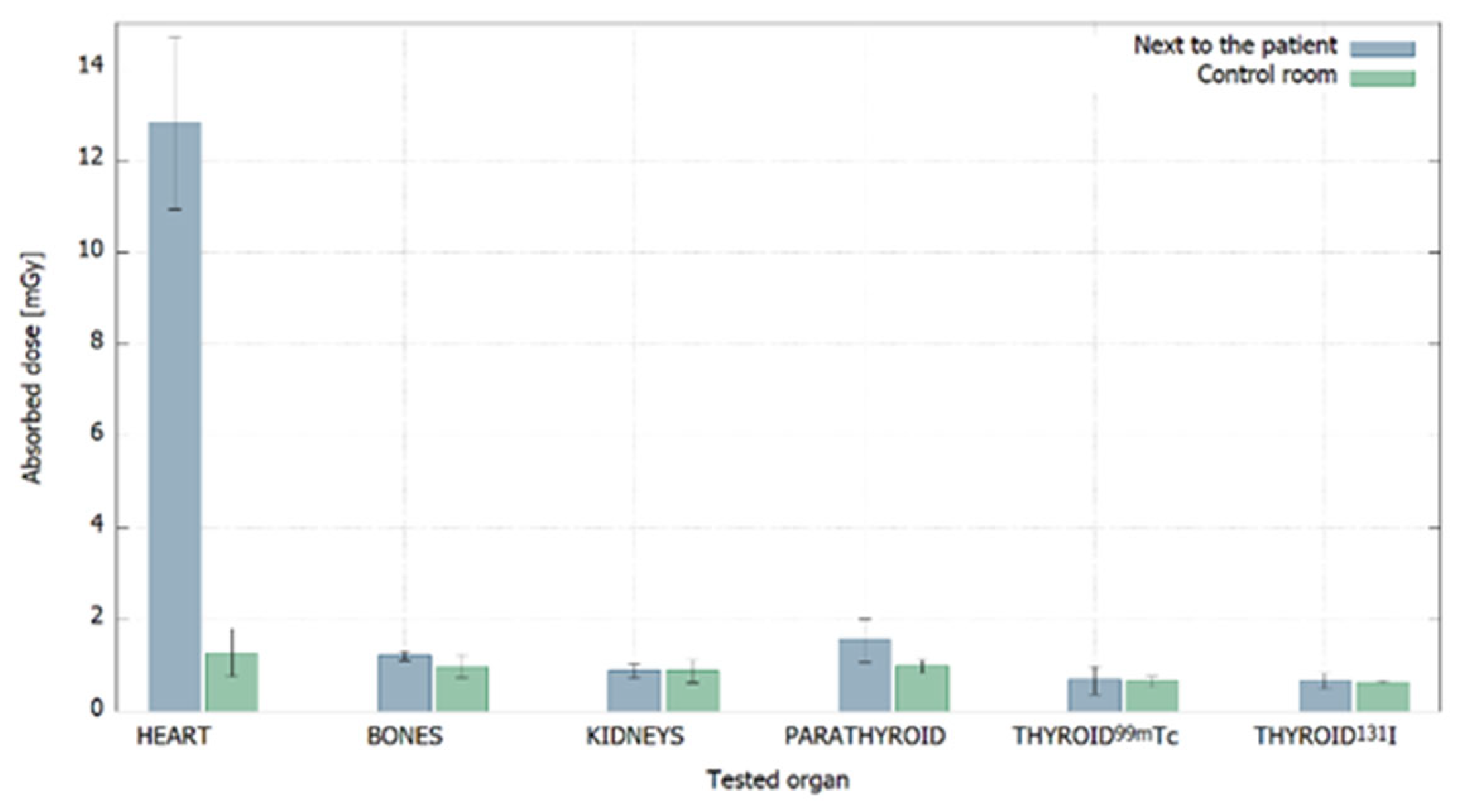
3.1. Absorbed Doses
3.2. Comparison with Dose Limits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nuclear Medicine. Available online: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/nuclear-medicine (accessed on 5 July 2020).
- Committee on State of the Science of Nuclear Medicine; Nuclear and Radiation Studies Board; Board on Health Sciences Policy; Division on Earth and Life Studies; National Research Council. Advancing Nuclear Medicine Through Innovation; National Academies Press: Washington, DC, USA, 2007; p. 1. [Google Scholar]
- Bevelacqua, J.J. Skin contaminations, internal intakes and ALARA. Radiat. Prot. Manag. 2004, 21, 11–16. [Google Scholar]
- Miller, D.; Schauer, D. The ALARA principle in medical imaging. AAPM Newsl. 2015, 40, 38–40. [Google Scholar]
- Huda, W. Radiation Risk: What is to Be Done? Am. J. Roentgenol. 2015, 204, 124–127. [Google Scholar] [CrossRef]
- Biran, T.; Malchi, J.S.; Marciano, R.; Chisin, R. Measurements of occupational exposure for a technologist performing 18F FDG PET scans. Health Phys. 2004, 87, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Soret, M.; Maisonobej, A.; Payen, S.; Gaubert, A.; Brunel, S.; Rozemblum, L.; Hubert, E.; Kas, A. Radiation dose of nuclear medicine technicians performing PET/MR. J. Radiol. Prot. 2020, 40, 861–866. [Google Scholar] [CrossRef] [PubMed]
- ICRP. ICRP Publication 60: 1990 Recommendations of the International Commission on Radiological Protection; Elsevier Health Sciences: Amsterdam, The Netherlands, 1991. [Google Scholar]
- Ustawa z Dnia 13 Czerwca 2019 r. o Zmianie Ustawy. Prawo Atomowe. DzU z 2019 r., poz. 1593. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20190001593 (accessed on 15 July 2020). (In Polish)
- Obwieszczenie Marszalka Sejmu Rzeczypospolitej Polskiej z 11 Wrzesnia 2019r. w Sprawie Ogłoszenia Jednolitego Tekstu Ustawy—Prawo Atomowe. DzU 2019 r., poz 1792. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20190001792 (accessed on 15 July 2020). (In Polish)
- Council Directive 2013/59/EUROATOM of 05 December 2013 Laying Down Basic Safety Standards for the Protection of the Health of Workers and the General Laying Down Basic Safety Standards for the Protection of the Health of Workers and the General. Available online: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A31996L0029 (accessed on 21 August 2020).
- ICRU. ICRU Report 39: Determination of dose equivalents resulting from external radiation sources. J. Int. Comm. Radiat. Units Meas. 1985, os20, 3–6. [Google Scholar] [CrossRef]
- ICRP. ICRP Publication 103: The 2007 Recommendations of the International Commission on Radiological Protection; Elsevier Health Sciences: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Ho, W.Y.; Wong, K.K.; Leung, Y.L.; Cheng, K.C.; Ho, F.T.H. Radiation doses to staff in a nuclear medicine department. J. HK Coll Radiol. 2002, 5, 24–28. [Google Scholar]
- Nassef, M.H.; Kinsara, A.A. Occupational radiation dose for medical workers at a university hospital. J. Taibah Univ. Sci. 2017, 11, 1259–1266. [Google Scholar] [CrossRef] [Green Version]
- Valuckas, K.P.; Atkočius, V.; Samerdokienė, V. Occupational exposure of medical radiation workers in Lithuania 1991–2003. Acta Med. Litu. 2007, 14, 155–159. [Google Scholar]
- Mettler, F.A.; Mahesh, M.; Bhargavan-Chatfield, M.; Chambers, C.E.; Elee, J.G.; Frush, D.P.; Miller, D.L.; Royal, H.D.; Milano, M.T.; Spelic, D.C.; et al. Patient exposure from radiologic and nuclear medicine procedures in the united states: Procedure volume and effective dose for the period 2006–2016. Radiology 2020, 295, 418–427. [Google Scholar] [CrossRef]
- Bayram, T.; Yilmaz, A.H.; Demir, M.; Sonmez, B. Radiation dose to technologists per nuclear medicine examination and estimation of annual dose. J. Nucl. Med. Technol. 2011, 39, 55–59. [Google Scholar] [CrossRef]
- Kopec, R.; Budzanowski, M.; Budzynska, A.; Czepczynski, R.; Dziuk, M.; Sowinski, J.; Wyszomirska, A. On the relationship between whole body, extremity and eye lens doses for medical staff in the preparation and application of radiopharmaceuticals in nuclear medicine. Radiat. Meas. 2011, 46, 1295–1298. [Google Scholar] [CrossRef]
- Matusiak, K.; Patora, A.; Jung, A. Comparison of MCP-Ns and MCP-N detectors usefulness for beta rays detection. Radiat. Meas. 2017, 102, 10–15. [Google Scholar] [CrossRef]
- Matusiak, K.; Patora, A.; Jung, A. The Influence Of Pre- And Post-Irradiation Annealingon Lif:Mg,Cu,P Stability. Radiat. Prot. Dosim. 2015, 171, 346–350. [Google Scholar] [CrossRef]
- Jung, K.; Matusiak, K. The impact of accidental immersion in selected liquids on the sensitivityand repeatability of MCP-N thermoluminescent detectors. Radiat. Meas. 2021, 141, 106525. [Google Scholar] [CrossRef]
- Bilski, P. Response of various LiF thermoluminescent detectors to high energy ions—Results of the ICCHIBAN experiment. Nucl. Instrum. Methods Phys. Res. B 2006, 251, 121–126. [Google Scholar] [CrossRef]
- Liuzzi, R.; Savino, F.; D’Avino, V.; Pugliese, M.; Cella, L. Evaluation of LiF:Mg,Ti (TLD-100) for Intraoperative Electron Radiation Therapy Quality Assurance. PLoS ONE 2015, 10, e0139287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, A.; Karabin, B.; Matusiak, K. Evaluation of spatial and seasonal dose fluctuations in a Wierzchowska Gorna limestone cave Isotopes. Environ Health Stud. 2013, 49, 180–187. [Google Scholar] [CrossRef]
- Hyafil, F.; Gimelli, A.; Slart, R.; Georgoulias, P.; Rischpler, C.; Lubberink, M.; Sciagra, R.; Bucerius, J.; Agostini, D.; Verberne, H. EANM procedural guidelines for myocardial perfusion scintigraphy using cardiac-centered gamma cameras. Eur. J. Hybrid Imaging 2019, 3, 11. [Google Scholar] [CrossRef] [Green Version]
- Obwieszczenie Ministra Zdrowia z Dnia 22 Grudnia 2014 r. w Sprawie Ogłoszenia Wykazu Wzorcowych Procedur Radiologicznych z Zakresu Medycyny Nuklearnej. DzUrz z 2014 r., poz.82. Available online: https://dziennikmz.mz.gov.pl/legalact/2014/82/ (accessed on 15 July 2020). (In Polish)
- Alkhorayef, M.; Mayhoub, F.H.; Salah, H.; Sulieman, A.; Al-Mohammed, H.I.; Almuwannis, M.; Kappas, C.; Bradley, D.A. Assessment of occupational exposure and radiation risks in nuclear medicine departments. Radiat. Phys. Chem. 2020, 170, 08529. [Google Scholar] [CrossRef]
- Elshami, W.; Erdemir, R.U.; Abuzaid, M.M.; Cavli, B.; Issa, B.; Tekin, H.O. Occupational radiation dose assessment for nuclear medicine workers in Turkey: A comprehensive investigation. J. King Saud Univ. Sci. 2022, 34, 102005. [Google Scholar] [CrossRef]
- Bolus, N.E. Review of Common Occupational Hazards and Safety Concerns for Nuclear Medicine Technologists. J. Nucl. Med. Technol. 2008, 36, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kron, T. Applications of thermoluminescence dosimetry in medicine. Radiat. Prot. Dosim. 1999, 85, 333–340. [Google Scholar] [CrossRef]
- Villoing, D.; Borrego, D.; Preston, D.L.; Alexander, B.H.; Rose, A.; Salasky, M.; Linet, M.S.; Lee, C.; Kitahara, C.M. Trends in Occupational Radiation Doses for U.S. Radiologic Technologists Performing General Radiologic and Nuclear Medicine Procedures, 1980–2015. Radiology 2021, 300, 605–612. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assignment | Average Counts from Group | Dose [mGy] |
|---|---|---|
| Near the Patient | ||
| 13,211 ± 1900 | 12.8 ± 1.8 |
| 1475 ± 97 | 1.21 ± 0.10 |
| 1150 ± 159 | 0.89 ± 0.16 |
| 1816 ± 472 | 1.55 ± 0.47 |
| 941 ± 306 | 0.68 ± 0.30 |
| 927 ± 164 | 0.67 ± 0.16 |
| In the Control Room | ||
| 1541 ± 521 | 1.27 ± 0.52 |
| 1241 ±261 | 0.98 ± 0.26 |
| 1139 ± 252 | 0.88 ± 0.25 |
| 1250 ± 152 | 0.99 ± 0.15 |
| 907 ± 123 | 0.65 ± 0.12 |
| 895 ± 30 | 0.64 ± 0.03 |
| Near the Patient | |||
| Dose Limit | Tested Organ | H*(10) [mSv] | Percentage of Dose Limit |
| 1.67 mSv/month | Bone | 1.39 ± 0.11 | 83% |
| Kidneys | 1.02 ± 0.17 | 61% | |
| Thyroid 99mTc | 0.78 ± 0.34 | 47% | |
| Thyroid 131I | 0.77 ± 0.18 | 46% | |
| Parathyroid glands | 1.78 ± 0.52 | 101% | |
| 3.33 mSv/2 months | Heart | 14.7 ± 2.1 | 442% |
| In the Control Room | |||
| Dose Limit | Tested Organ | H*(10) [mSv] | Percentage of Dose Limit |
| 1.67 mSv/month | Bone | 1.13 ± 0.30 | 68% |
| Kidneys | 1.01 ± 0.29 | 61% | |
| Thyroid 99mTc | 0.75 ± 0.13 | 45% | |
| Thyroid 131I | 0.74 ± 0.03 | 44% | |
| Parathyroid glands | 1.14 ± 0.17 | 68% | |
| 3.33 mSv/2months | Heart | 1.47 ± 0.6 | 44% |
| Near the Patient | In Control Room | ||||||
|---|---|---|---|---|---|---|---|
| Tested Organ | Number of Procedures | Share in Total Number of Procedures | H*(10)/Study [mSv] | H*(10) Time Correction [mSv] | H*(10)/Study [mSv] | H*(10) Time Correction [mSv] | Total Dose [mSv] |
| Heart | 158 | 79% | 0.09 | 0.02 | 0.01 | 0.01 | 0.03 |
| Bones | 24 | 12% | 0.06 | 0.01 | 0.05 | 0.04 | 0.05 |
| Kidneys | 5 | 2% | 0.20 | 0.04 | 0.20 | 0.16 | 0.20 |
| 131I Thyroid | 6 | 3% | 0.13 | 0.03 | 0.12 | 0.10 | 0.12 |
| 99mTc Thyroid | 3 | 1% | 0.26 | 0.05 | 0.25 | 0.20 | 0.25 |
| Parathyroid glands | 5 | 2% | 0.36 | 0.07 | 0.23 | 0.18 | 0.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matusiak, K.; Wolna, J.; Jung, A.; Sadowski, L.; Pawlus, J. Impact of the Frequency and Type of Procedures Performed in Nuclear Medicine Units on the Expected Radiological Hazard. Int. J. Environ. Res. Public Health 2023, 20, 5206. https://doi.org/10.3390/ijerph20065206
Matusiak K, Wolna J, Jung A, Sadowski L, Pawlus J. Impact of the Frequency and Type of Procedures Performed in Nuclear Medicine Units on the Expected Radiological Hazard. International Journal of Environmental Research and Public Health. 2023; 20(6):5206. https://doi.org/10.3390/ijerph20065206
Chicago/Turabian StyleMatusiak, Katarzyna, Justyna Wolna, Aleksandra Jung, Leszek Sadowski, and Jolanta Pawlus. 2023. "Impact of the Frequency and Type of Procedures Performed in Nuclear Medicine Units on the Expected Radiological Hazard" International Journal of Environmental Research and Public Health 20, no. 6: 5206. https://doi.org/10.3390/ijerph20065206
APA StyleMatusiak, K., Wolna, J., Jung, A., Sadowski, L., & Pawlus, J. (2023). Impact of the Frequency and Type of Procedures Performed in Nuclear Medicine Units on the Expected Radiological Hazard. International Journal of Environmental Research and Public Health, 20(6), 5206. https://doi.org/10.3390/ijerph20065206